
Abstract
Polycystic ovary syndrome (PCOS) is a common endocrine disorder with dysfunctional ovulation affecting female fertility. The purpose of this study was to determine the association between gonadotropin (Gn) duration and in vitro fertilization (IVF) outcomes in PCOS women undergoing GnRH antagonist treatment. Retrospective cohort study at a large private fertility practice. Patients with PCOS undergoing the GnRHantagonist treatment between January 1, 2017, and July 31, 2021 were included. Patients were classified into two groups depending on their Gn duration, ≤ 8 days (n = 501) and >8 days (n = 1326). After propensity score matching (PSM), there were 87 PCOS women with Gn duration ≤ 8 days and 137 PCOS women with Gn duration >8 days in the fresh embryo transfer cycle. The primary outcomes measures included the clinical pregnancy, ongoing pregnancy, early miscarriage and live birth rate between the two groups after fresh embryo transfer. In addition, the embryo quality was also evaluated. There was no significant difference in baseline characteristics between groups. However, the total Gn dosage was lower in PCOS women in the ≤ 8 days group. In addition, the oocytes retrieved and D3 high quality embryos were compared between groups. However, the number of 2PN embryos was decreased in the group with Gn duration ≤ 8 days. The clinical pregnancy and live birth rate were significantly decreased in the ≤ 8 days group in fresh embryo transfer (52.87% vs. % 68.61%, 43.68% vs. 59.12%). After logistic regression, PCOS women with Gn duration ≤ 8 days were associated with poor clinical pregnancy and live birth rate. PCOS women with shorter Gn duration (≤ 8 days) were not associated with impaired embryo outcomes except for 2PN embryos in GnRH antagonist protocol. However, the shorter Gn stimulation was detrimental to clinical pregnancy outcomes in fresh embryo transfer cycle.
Similar content being viewed by others

Introduction
Polycystic ovary syndrome (PCOS), the leading cause of female infertility, is often associated with good ovarian reserve and a robust response with controlled ovarian stimulation(COS)1. Gonadotropin-releasing hormone antagonist(GnRH antagonist) protocol do not seem to compromise pregnancy rates and is associated with lower risk of ovarian hyperstimulation (OHSS) and therefore could be considered as standard treatment in PCOS patients2. To decrease time to pregnancy, fresh embryo transfer can be considered when the risk of OHSS is low in PCOS patients. When optimizing fresh embryo cycle outcomes, both the COS outcomes and the endometrial receptivity should be carefully considered. In addition, compared with traditional COS treatment, personalized ovarian stimulation may optimized IVF outcomes3.
And two potentially modifiable factors related to the COS are total gonadotropin (Gn) dose and the days of Gn duration. Data from fresh IVF-embryo transfer (IVF-ET) cycles demonstrate that prolonged COS is associated with poor clinical outcomes4. However, the proper Gn duration differed between COS response5. Recently study has demonstrated that menstrual cycle length (MCL) was associated with assisted reproductive technology (ART) outcomes in normal responder with regular menstrual cycles6. In patients with different ovarian reserve, the clinical outcomes are not the same with different MCL. It seems that women with polycystic ovary syndrome (PCOS) have a higher likelihood of pregnancy and a lower risk of miscarriage when their menstrual cycles become regular and shorter. However, it is unclear how stimulation duration affect clinical outcomes in PCOS patients as these patients are always with a longer menstruation and with high ovarian reserve.
In 2022, the Chinese Medical Doctor Association (CMDA) promulgated the “Expert Consensus on Standardized Application of gonadotropin-releasing hormone antagonist in Assisted Reproductive Technology”7, which point out several key points to optimize clinical outcomes. It is suggested that an appropriate stimulation length is associated with better oocyte and embryo capacity as well as better endometrial receptivity. Generally, the proper Gn duration may be 8 to 10 days. However, more scientific evidence needed to be determined the appropriate Gn duration based on individualized stimulation protocols and different ovarian response. For PCOS patients, the main treatment goal is to reduce the risk of OHSS. In some patients with good COS parameters, fresh embryo transfer can be considered to shorten the time to live birth. However, the proper cut- off value of Gn duration was not determined in PCOS patients. This study aimed to investigate whether pregnancy outcomes would change in the PCOS patients between different Gn duration and try to figure out the appropriate Gn duration to optimize the fresh embryo transfer.
Materials and methods
Study design
This was a retrospective cohort study designed to examine the effect of Gn duration on the IVF outcomes of PCOS patients who underwent a flexible GnRH antagonist protocol during ART. All GnRHantagonist cycles performed at the Reproductive Center of Shenzhen Zhongshan Urology Hospital (now renamed Shenzhen Zhongshan Obstetrics & Gynecology Hospital) from 1st January 2017 to 31st July 2021were assessed. This study was approved by the Institutional Review Board of the Shenzhen Zhongshan Urology Hospital (now renamed Shenzhen Zhongshan Obstetrics & Gynecology Hospital) and owing to the retrospective nature of the study, the requirement for informed consent was waived (SZZSECHU-F-2023026).
Participants
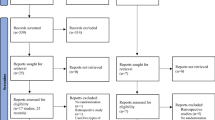
Women with PCOS who completed their first IVF/ICSI cycles were recruited to the control group (Gn >8days) and the study group (Gn ≤ 8 days). For patients who received more than one cycle of COS within this time frame, only the first cycle was considered to prevent repeated inclusion. According to the 2003 Rotterdam consensus8, at least two of the following symptoms were required for women to be diagnosed with PCOS. (1) oligo- and/ or anovulation; (2) ultrasonography appearance of polycystic ovaries; or (3) biochemical and/or clinical indicators of hyperandrogenism. The exclusion criteria included: (1) maternal age>40y; (2) uterine abnormality; (3) abnormal karyotype (chromosome polymorphisms were not excluded). (4)Patients who were undergoing intrauterine insemination (IUI) treatment and then transfer to GnRH antagonist IVF because of multiple follicles growth. Figure 1 depicts the study process.

Patient flow.
Protocols-controlled ovarian stimulation
All PCOS patients underwent COS using a flexible GnRH antagonist protocol. The starting dose of gonadotropin was determined based on physician preference, taking into account of maternal age, BMI, antral follicle count (AFC) and AMH. During COS, FSH doses were adjusted in accordance with the ovarian response. The GnRHantagonist administration was initiated based on a flexible protocol, generally when the leading follicle was 12 mm in size or serum estradiol (E2) exceeded 300pg/mL, whichever occurred first. Once two or more follicles reached a size of 18 mm, either human chorionic gonadotropin (HCG) or dual trigger was administered. Lupron was only administered for final oocyte maturation in situations where more than 15 follicles > 14 mm were present, indicating a higher risk of OHSS. Oocyte retrieval was performed by transvaginal ultrasonography-guided single-lumen needle aspiration 36 h after luteinizing hormone injection. Intracytoplasmic sperm injection (ICSI) was only performed for patients experiencing severe male factor infertility. Fertilization was evaluated 16–18 h after insemination, and embryo morphology was assessed on day 3, taking into account of the number of cells and percentage of fragmentation. Embryo transfer was routinely performed 3 or 5 days after oocyte retrieval. And frozen embryo transfer was used when the patients was diagnosed with a high risk of OHSS or elevated progesterone (>1.3pg/ml). Luteal-phase support was initiated on the day of oocyte retrieval. In instances where Lupron was used for final oocyte maturation, the luteal phase was supported with both estrogen and progesterone.
Outcome measures
The analyses of clinical pregnancy outcomes included PCOS women in the fresh transfer group (Fig. 1), but not the women in the freeze-all group. In this study, clinical pregnancy, ongoing pregnancy, early miscarriage and live birth rate were used as the primary outcome. The secondary outcomes were the rate of moderate to severe OHSS, number of retrieved oocytes, the oocyte matured, fertilized and high-quality embryos. At 4 weeks following ET, ultrasound detection of a gestational sac with or without foetal heart activity indicated the diagnosis of clinical pregnancy. The clinical pregnancy rate was determined by dividing the total number of clinical pregnancies by the sum of ET cycles. The definition of ongoing pregnancy was greater than 12 gestational weeks. The definition of early miscarriage was miscarriage occurred before 12 weeks. The definition of live birth rate was live newborns born after 28 weeks. The ongoing pregnancy rate was determined by dividing the total number of ongoing pregnancies by the sum of ET cycles. The definition of early miscarriage rate was determined by dividing the total number of early miscarriage by the sum of ET cycles. The live birth rate was determined by dividing the total number of live birth by the sum of ET cycles.
Statistical analysis
To determine the cut-off level of stimulation days, we specify the optimal cut-off values by means of the Youden’s index (sensitivity + specificity − 1), which ranges between 0 and 1, with higher values indicating greater diagnostic performance9. When the Youden’s index was the maximum, the specificity and sensitivity were 0.388 and 0.747. Finally, we detected that the proper cut-off level of stimulation days was 8 days. To account for inherent disparities in the baseline characteristics of the two groups, we developed a propensity score matching (PSM). Ten variables were chosen for use in the propensity score estimation, including age, infertility type, BMI, AMH, endometrial thickness, progesterone level on trigger day, the percentage of IVF and ICSI, the type of trigger, as well as type and embryo and number of embryos transferred before IVF/ICSI. PSM was performed using the nearest-neighbor 1:2 (Gn \(\:\le\:\)8 days : Gn \(\:>\)8 days) matching method with a caliper width of 0.1. The mean ± standard deviation (SD) and Student’s t test were used to display and evaluate normally distributed continuous data. The median [25th percentile, 75th percentile] and Mann–Whitney U tests were used to express and assess non-normally distributed continuous data. Categorical data are displayed as n (percentage) and compared with Fisher’s exact test or Pearson’s chi-squared test. In addition to bivariate analyses, multivariable logistic regression was conducted to determine predictors of clinical pregnancy, ongoing pregnancy, early miscarriage or live birth rate with duration of stimulation as the independent variable of interest. All statistical tests were two-sided and statistical significance was set at p < 0.05. Statistical analysis was performed using SPSS statistics 26.0 (IBM Crop., Armonk, NY, USA) and PSM was performed with R version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
The study’s flow chart is summarized in Fig. 1. Specifically, we enrolled 1827 women with PCOS who were candidates for assisted reproductive technology treatment in our clinical centre between January 2017 and July 2021. Based on the criteria outlined in the Methods and Materials, 314 cycles were included. In addition, we used the nearest neighbor random matching method to match 87 women who received the Gn stimulation ≤ 8 days and 137women who received the Gn stimulation>8 days treatment at a 1:2 ratio undergoing fresh embryo transfer. The shortest duration of stimulation was 6 days with the longest being 18 days. The baseline characteristics before PSM and after PSM are presented in Table 1. Post matching analysis showed no significant variations in any baseline characteristics except for basal LH level between the groups (all P > 0.05) (Table 1).
The characteristics of ovarian stimulation are presented in Table 2. The initial Gn dose was higher in Gn ≤ 8 days group (150.00 [112.50, 150.00] vs. (137.25 [112.50, 150.00], P = 0.015). And obviously, the total dose of Gn in the Gn ≤ 8 days group was significantly lower than that in the Gn >8 days group (1200.00 [975.00, 1425.00]) vs.1575.00 [1350.00, 2100.00]], p < 0.001) (Table 2). On trigger day, there was no significance difference in the E2, P4 level,type of trigger or thickness of endometrium between the two groups.
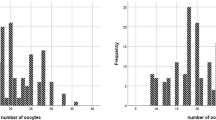
The study and control groups exhibited similar numbers of oocytes retrieved (13.00 [11.00, 16.00] vs. 13.00 [11.00, 17.00], P > 0.05), mature oocytes (12.00 [9.00, 14.00] vs. 13.00 [10.00, 15.00], P > 0.05) and high-quality embryos (6.00 [3.00, 8.00]vs. 6.00 [4.00, 9.00], P > 0.05). However, the number of 2PN embryos was decreased (8.00 [5.00, 10.00]vs9.00 [6.00, 11.00]) in the Gn<8 days group.
There was no significant difference on the stage and number of embryos transferred per cycle between the two groups (Table 3). The clinical pregnancy, and live birth rate was significantly lower in the Gn ≤ 8 days group (52.87% vs. % 68.61%, P = 0.018, 43.68% vs. 59.12%, P = 0.024). However, there was no significant difference in positive pregnancy, ongoing pregnancy rate or early miscarriage rate per embryo transfer between groups. The incidence of OHSS was similar between groups.
A binary logistic regression model was also used to assess the association between Gn stimulation days and pregnancy and birth outcomes while adjusting for potential confounders (Table 4). Furthermore, in the crude and adjusted models, the Gn >8 days group was associated with significantly higher clinical pregnancy (OR 1.948, 95%CI (1.121, 3.404), P = 0.018, adjusted OR 2.024, 95%CI (1.153, 3.580), P = 0.015) and live birth rate (OR 1.865,95%CI (1.086, 3.227), P = 0.025, adjusted OR:1.960, 95%CI (1.120, 3.463), P = 0.014). However, the positive pregnancy rate or ongoing pregnancy rate was comparable between groups in the crude or adjusted models.
Discussion
In this retrospective cohort study, we demonstrated that the shorter Gn duration (Gn ≤ 8 days) was associated with decreased clinical pregnancy outcomes in PCOS patients undergoing GnRH antagonist protocol, but the oocyte or embryo capacity was not impacted by the Gn stimulation duration.
Recent evidence demonstrated that longer menstrual cycle length(MCLs) are related to more antral follicular waves and higher ovarian responses10,11,12. Furthermore, MCLs are associated with the number of retrieved oocytes and clinical pregnancy rate in IVF treatment11. According to recent study, clinicians can estimate the range of ovarian stimulation duration by calculating the original length of the follicular phase to obtain more mature oocytes and to optimize clinical outcomes6. Benjamins et found that women with AMH > 8 ng/mL had follicular phases that were longer by 2 days12, PCOS patients are always with a higher AMH and longer menstrual cycle length, thus the shorter ovarian stimulation may be detrimental to IVF success rate.
Previous studies revealed conflicting results when investigating the relationship between the stimulation length and IVF outcomes. Pereira, N. reported that increased odds of live birth in fresh D3 ET undergoing GnRH antagonist treatment with shorter ovarian stimulation (≤ 13d) in patients with normal ovarian reserve13. However, data obtained from Society for Assisted Reproductive Technology(SART) CORS on all fresh donor oocyte GnRH antagonist cycles (n = 1049) between 2014 and 2015 which resulted in a single embryo transferred, and they found out that length of ovarian stimulation does not impact live birth rate in fresh donor oocyte cycles14. Fresh donor oocyte cycles are fundamentally different when compared with fresh autologous cycles, as donors are typically young and without an infertility diagnosis and the effect of COS on the endometrium receptivity is not an influencing factor in the recipients. The results from Purandare discovered the duration of stimulation does not alter the clinical pregnancy rate in ICSI or IVF cycles using the long, antagonist or flare stimulation protocol15. Prior study reported an increased stimulation length for women with PCOS and improved live birth rates, which is consistent with our current study16. The outcome of gonadotrophin OS/IUI cycles found that a shorter follicular phase (≤ 8 days) was associated with a decreased chance of clinical pregnancy17. The lack of consensus is likely due to a lack of standardized cut-off points for ovarian stimulation duration or patients characteristic bias.
COS is utilized in order to increase the number of oocytes retrieved per cycle, thereby increasing the chances of obtaining a high-quality embryo and live birth. In our current study, the PCOS patients with longer ovarian stimulation is always correlated with higher total Gn dosage, but the clinical outcomes were better than the shorter ovarian stimulation group. This may be due to different patients characteristics. PCOS patients were always with higher ovarian response, but the total Gn dosage used was lower than normal or poor responders. In our current study, we found that the embryo capacity is not affected by ovarian stimulation length. Patients with prolonged ovarian stimulation was associated with more total Gn dosage, but not associated with impaired embryo quality. Recent studies reported that higher dosage was not associated with increased aneuploidy rate18,19,20. An analysis of 12,298 trophectoderm biopsies concluded that euploidy rates are not significantly influenced by gonadotropin dosage or duration of ovarian stimulation, regardless of woman’s age20. After stratifying by age, the results from Hong et al.so found that there were no statistically significant differences in the aneuploidy rate in natural and stimulated cycles21. In addition, Barash et al. and Sekhon et al. both reported similar results, that is higher gonadotropin dosage did not affect the rate of aneuploidy after controlling for age18,19. However, a retrospective analysis of embryo aneuploidy in patients undergoing preimplantation genetic testing for aneuploidy (PGT-A) in vitro fertilization (IVF) cycles reported that lower gonadotropin dosage reduces aneuploidy22. An analysis data from 650,637 fresh autologous IVF cycles reported to the SART between 2004 and 2012, they found that excessive FSH doses during ART may be detrimental to oocyte retrieval23.And, they reported that the highest number of oocytes retrieved was in the 1001– 2000 IU FSH group regardless of patient prognosis, age, BMI, ovarian stimulation protocol, and infertility diagnosis. In our current study, the total Gn dosage was below 2000IU, this may explains why in our PCOS patients undergoing fresh IVF-ET cycles, long ovarian stimulation was not correlated with decreased pregnancy rates, as those patients tend to have a low daily Gn dose and the total Gn dose is kept to a minimum dosage.
As the embryo quality was not affected by ovarian stimulation length, we postulated that the endometrial receptivity was impaired in the shorter stimulation group in PCOS patients undergoing GnRH antagonist protocol. In regard to the effect of stimulation length on the endometrium, the data suggest that the ovarian stimulation duration was not associated with endometrium thickness. However, previous study found that longer follicular phase was associated with increased pregnancy outcomes than the shorter group in intrauterine insemination cycles17. This may be due to the small sample size in the shorter Gn group in our present study. And the PCOS patients in the fresh embryo transfer cycle are with good endometrial thickness and morphology in this study. Moreover, it is possible that the effect of shorter ovarian stimulation length on poor clinical outcomes may be partially due to inadequate time for endometrial development and thus detrimental to endometrial receptivity.
Advantages of our study include only the PCOS patients, and all the patients undergoing ovarian stimulation with GnRHantagonist protocols, helping to elucidate the impact of ovarian stimulation length in PCOS patients with GnRHantagonist cycle. It is also important to note that the cut-off chosen for the study cohort was data from the ROC analysis. Given the retrospective nature of the study, we acknowledge some uncertainty in the replication of these findings in a prospective setting. In addition, our findings may not be applicable to normal or poor responders.
Although our retrospective analysis was not designed to address cancellation of fresh embryo cycles in the setting of shorter ovarian stimulation, our findings do highlight that clinical pregnancy outcomes may be affected by shorter ovarian stimulation due to compromised endometrial receptivity. A freeze all strategy may be considered in PCOS patients with shorter Gn duration to optimize clinical outcomes. Thus, the present research should be considered a preliminary effort, and the development of additional evidence requires further by more prospective studies to validate the impact of ovarian stimulation length on IVF-ET outcomes in PCOS women.
Conclusion
In conclusion, our study emphasizes how shorter ovarian stimulation, a potentially modifiable variable, can impact the outcomes of IVF cycles in PCOS patients. Our findings highlight that patients undergoing ovarian stimulation > 8 days achieve better fresh IVF-ET outcomes, with higher clinical pregnancy and live birth rate. We postulated that the shorter ovarian stimulation may lead to inadequate development of the endometrium environment. However, the study’s findings should be taken into consideration for normal or poor responder patients.
Data availability
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
References
Escobar-Morreale, H. F. Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Nat. Rev. Endocrinol. 14 (5), 270–284 (2018).
Costello, M. F. et al. Evidence summaries and recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome: assessment and treatment of infertility. Hum. Reprod. Open. 2019 (1), hoy021 (2019).
Nyboe, A. A. et al. Individualized versus conventional ovarian stimulation for in vitro fertilization: a multicenter, randomized, controlled, assessor-blinded, phase 3 noninferiority trial. Fertil. Steril. 107 (2), 387–396e4 (2017).
Gerber, R. S. et al. Differential impact of controlled ovarian hyperstimulation on live birth rate in fresh versus frozen embryo transfer cycles: a society for assisted reproductive technology clinic outcome system study. Fertil. Steril. 114 (6), 1225–1231 (2020).
Yang, Y. C. et al. The different impact of stimulation duration on oocyte maturation and pregnancy outcome in fresh cycles with GnRH antagonist protocol in poor responders and normal responders. Taiwan. J. Obstet. Gynecol. 58 (4), 471–476 (2019).
Zhao, X. et al. Association between the ratio of ovarian stimulation duration to original follicular phase length and in vitro fertilization outcomes: a novel index to optimise clinical trigger time. Front. Endocrinol. (Lausanne). 13, 862500 (2022).
Expert consensus on standardized application of. gonadotropin-releasing hormone antagonist in assisted reproductive technology. Chin. J. Reprod. Contracept. 42 (2), 109–116 (2022).
Revised consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 19 (1), 41 – 47 (2003).
YOUDEN, W. J. Index for rating diagnostic tests. Cancer 3 (1), 32–35 (1950).
Vassena, R. et al. Menstrual cycle length in reproductive age women is an indicator of oocyte quality and a candidate marker of ovarian reserve. Eur. J. Obstet. Gynecol. Reprod. Biol. 177, 130–134 (2014).
Younis, J. S. et al. Does an association exist between menstrual cycle length within the normal range and ovarian reserve biomarkers during the reproductive years? A systematic review and meta-analysis. Hum. Reprod. Update. 26 (6), 904–928 (2020).
Harris, B. S., Steiner, A. Z. & Jukic, A. M. Ovarian reserve biomarkers and menstrual cycle length in a prospective cohort study. J. Clin. Endocrinol. Metab. 106 (9), e3748–e3759 (2021).
Pereira, N. et al. Increased odds of live birth in fresh in vitro fertilization cycles with shorter ovarian stimulation. Fertil. Steril. 107 (1), 104–109e2 (2017).
Cohen, A. et al. Length of ovarian stimulation does not impact live birth rate in fresh donor oocyte cycles: a SART CORS study. J. Assist. Reprod. Genet. 37 (12), 3033–3038 (2020).
Munch, E. M. et al. High FSH dosing is associated with reduced live birth rate in fresh but not subsequent frozen embryo transfers. Hum. Reprod. 32 (7), 1402–1409 (2017).
Ryan, A. et al. Prolonged gonadotropin stimulation for assisted reproductive technology cycles is associated with decreased pregnancy rates for all women except for women with polycystic ovary syndrome. J. Assist. Reprod. Genet. 31 (7), 837–842 (2014).
Bakkensen, J. B. et al. The effect of follicular phase length on cycle outcomes and endometrial development in gonadotrophin ovarian stimulation/intrauterine insemination cycles. Reprod. Biomed. Online. 40 (3), 362–368 (2020).
Barash, O. O. et al. High gonadotropin dosage does not affect euploidy and pregnancy rates in IVF PGS cycles with single embryo transfer. Hum. Reprod. 32 (11), 2209–2217 (2017).
Sekhon, L. et al. The cumulative dose of gonadotropins used for controlled ovarian stimulation does not influence the odds of embryonic aneuploidy in patients with normal ovarian response. J. Assist. Reprod. Genet. 34 (6), 749–758 (2017).
Irani, M. et al. No effect of ovarian stimulation and oocyte yield on euploidy and live birth rates: an analysis of 12 298 trophectoderm biopsies. Hum. Reprod. 35 (5), 1082–1089 (2020).
Hong, K. H. et al. Embryonic aneuploidy rates are equivalent in natural cycles and gonadotropin-stimulated cycles. Fertil. Steril. 112 (4), 670–676 (2019).
Sachdeva, K. et al. Low gonadotropin dosage reduces aneuploidy in human preimplantation embryos: first clinical study in a UAE population. Genet. Test. Mol. Biomarkers. 22 (10), 630–634 (2018).
Clark, Z. L. et al. FSH dose is negatively correlated with number of oocytes retrieved: analysis of a data set with ~ 650,000 ART cycles that previously identified an inverse relationship between FSH dose and live birth rate. J. Assist. Reprod. Genet. 38 (7), 1787–1797 (2021).
Acknowledgements
We thank all the participants in this study, including the patients and the investigators.
Funding
This work was supported by Natural Science Foundation of Shenzhen (JCYJ20210324123412035) and Basic Research Program of Shenzhen (JCYJ20230807150200001 and JCYJ20220530172814032).
Author information
Authors and Affiliations
Contributions
S.X and SL collected data and developed the manuscript. L.H guided the design and reviewed the manuscript. R.J and TR.Y performed the data collection, and Z.Q.L did the statistical analysis. H.Z.Z and M.M.L guided the design and implementation of the study. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The studies involving human participants were reviewed and approved by The Reproductive Research Ethics Committees (SZZSECHU-F-2023026). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xiao, S., Liu, S., Hong, L. et al. Shorter ovarian stimulation is detrimental to fresh embryo transfer outcomes in PCOS women undergoing GnRH antagonist protocol: a retrospective cohort study. Sci Rep 15, 21002 (2025). https://doi.org/10.1038/s41598-025-06217-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-06217-0
