
Abstract
The endothelial activation and stress index (EASIX) can predict endothelial intricacies as well as survival in distinct clinical circumstances. Accordingly, we hypothesize that EASIX may also serve as a predictor for stroke prevalence and mortality outcomes-all-cause mortality (ACM) and cardiovascular mortality (CVM) due to stroke. To validate our hypothesis, we deployed the National Health and Nutrition Examination Survey data. This cohort study employed 1999–2018 NHANES data. To evaluate EASIX effects on stroke risk, weighted logistic regression models were deployed. Meanwhile, we utilized the weighted Cox proportional hazards model for the calculation of hazard ratios (HRs) and 95% confidence intervals (CI) for mortality outcomes. The Kaplan-Meier curves were utilized, seeking the assessment of the interplay between the EASIX and both ACM and CVM among stroke patients. Using restricted cubic spline (RCS) curves, the potential non-linear or linear relations were investigated between the EASIX and both stroke prevalence and mortality outcomes. Subgroup analyses were performed to further assess the interconnection that existed between the EASIX and both stroke presence and its mortality outcomes. Interaction tests between covariates were also performed. Assessment of diagnostic value was done via receiver operating characteristic (ROC) curves. The area under the curve (AUC) was measured to estimate the EASIX predictive values for stroke prevalence and mortality outcomes. Of 43,853 participants, 1674 had a stroke; among them, there were (743/1671, 44.46%) ACM and 225 (13.46%) CVM. After full adjustment, EASIX was positively related to the likelihood of having a stroke (odds ratio [OR] = 1.16, 95% CI: 1.07–1.25). Unlike participants whose EASIX was in the lowest quartile (Q1), those in other quartiles (Q3/Q4) had an increased likelihood of having a stroke (OR = 1.34, 95% CI: 1.04–1.74; OR = 1.54, 95% CI 1.20–1.96, correspondingly). During a median follow-up of 71 months, Cox regression analysis manifested a positive interplay between EASIX and ACM (HR = 1.30, 95% CI: 1.17–1.44) and CVM (HR = 1.29, 95% CI: 1.06–1.58). The results showcased a non-linear interplay between EASIX and stroke presence and mortality outcomes. Additionally, subgroup analysis indicated no significant interactions between EASIX and any categorical covariates for CVM. Nervelessness, significant interaction effects existed between EASIX and the prevalence of stroke in categorical covariates such as hypertension, diabetes, and coronary heart disease (CHD; P < 0.001), as well as between EASIX and ACM in the categorical covariate of gender (P = 0.03). The ROC curves illustrated that the cutoff value of EASIX for stroke incidence and CVM was 0.56, and 0.58 for ACM, with an AUC of 0.663 (95% CI: 0.649–0.677) for stroke prevalence, as well as for ACM with an AUC of 0.620 (95% CI: 0.595–0.649) and for CVM with an AUC of 0.587 (95% CI: 0.549–0.626). The EASIX demonstrated a positive non-linear association with the prevalence and mortality outcomes amongst individuals at the age of 20 years and older who experienced a stroke, as identified in the NHANES dataset. Heightened EASIX scores were significantly related to an escalated risk of both stroke prevalence and mortality outcomes. Collectively, EASIX may be a valuable biomarker for assessing mortality risks in stroke patients and stroke prevalence. Looking forward, implementing EASIX in primary care settings could facilitate the early screening of endothelial function, thereby identifying high-risk patients and guiding appropriate referrals for specialized medical care. This approach can promote patient outcomes and reduce mortality rates among those who have suffered a stroke. Nevertheless, further validation in diverse countries and among various ethnic groups is necessary.
Similar content being viewed by others

Introduction
According to data from the Centers for Disease Control and Prevention (CDC), the self-reported prevalence of stroke among adults aged 18 and older increased by 7.8% between 2011 and 20221. In addition, stroke became the fifth leading cause of death in the United States in 2021 and imposed an economic burden of approximately $56.2 billion on U.S. residents between 2019 and 20201. Despite significant advancements in stroke care as well as secondary prevention, the overall disease burden of stroke remains substantial. This underscores the urgent need for comprehensive interventions—such as public health initiatives, multidisciplinary management, and the exploration of prognostic factors—to predict and mitigate adverse outcomes, enhance patients’ quality of life, and address the escalating challenges posed by stroke.
Multiple pathophysiological processes occur in stroke progression, such as endothelial malfunction, with significance in both stroke onset and progression2. Endothelial dysfunction will cause vascular tone dysregulation, pro-thrombotic state, atherosclerosis, and enhanced inflammatory response2,3,4. Conversely, stroke will aggravate endothelial dysfunction by ischemia-reperfusion injury, inflammatory and immune response, and disruption of the blood-brain barrier (BBB)5,6,7,8. Accordingly, assessing endothelial injury severity may assist in stroke patients’ risk stratification.
Recently, endothelial activation and stress index (EASIX), which incorporates lactic dehydrogenase (LDH), creatinine, and platelets (PLT), has been established and validated to assess endothelial damage degree after allogeneic stem-cell transplantation9. The EASIX correlation has been elucidated with various endothelial activation markers: Chemokine-X-C-ligand 8 (CXCL8), interleukin-18 (IL-18), tumorigenicity-2 suppressor, and insulin-like growth factor-110,11. Moreover, EASIX has been has been demonstrated as a reliable indicator of endothelial dysfunction and mortality risk in various populations, such as those with COVID-19, multiple myeloma, small-cell lung cancer, diffuse large B-cell lymphoma, sepsis, and coronary artery disease12,13,14,15,16,17. Building on this potential, we hypothesize that EASIX may also serve as a predictor for stroke prevalence and mortality outcomes. To date, however, no large-scale studies have explored the relationship between EASIX and both stroke prevalence and mortality outcomes. To address this gap, we aim to utilize data from the National Health and Nutrition Examination Survey (NHANES) to investigate this association. Specifically, the primary objective of this study is to examine the correlation between EASIX levels and stroke prevalence, as well as all-cause mortality (ACM) and cardiovascular mortality (CVM) in stroke patients. We hypothesize that higher EASIX levels will be positively associated with increased stroke prevalence and higher rates of ACM and CVM among stroke patients.
Methods
Data source and study participants
Here, we conducted a continuous cross-sectional analysis utilizing NHANES data spanning ten two-year survey cycles from 1999 to 2018. The NHANES data were collected and curated by the National Center for Health Statistics (NCHS) with the authority of the Centers for Disease Control and Prevention (CDC). The current study employed an intricate, multistage area probability sampling methodology to select a nationally representative sample of non-institutionalized U.S. adults18. The NHANES (https://www.cdc.gov/nchs/nhanes) is a CDC-managed extensive survey designed to produce nationally representative statistics on the U.S. population’s health and nutritional status. The study integrates comprehensive components, including detailed questionnaires, physical evaluations, and laboratory analyses, encompassing a broad spectrum of health indicators and nutritional parameters. These parameters include, but are not limited to, the prevalence of chronic diseases, dietary intake, body mass index (BMI), blood pressure levels, blood biochemical markers, and various lifestyle factors. All participants signed informed consent, ensuring their voluntary contribution to the NHANES survey.
The data collection process of NHANES comprises interviews, physical examinations, and laboratory analyses, thereby providing a wealth of health-related information that serves as a crucial resource for public health research. Each two-year cycle of NHANES data undergoes rigorous quality control and standardization procedures to ensure the data accuracy and comparability. These datasets not only reflect the U.S. population’s health and nutritional status but also facilitate monitoring disease trends, public health policy formulation, and the evaluation of the effectiveness of intervention measures. By leveraging these high-quality data, our study is well-positioned to conduct an in-depth analysis of the interplay between EASIX and stroke incidence and mortality outcomes, thereby ensuring high external validity and practical applicability.
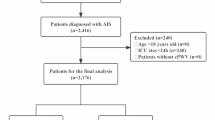
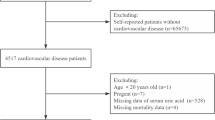
For this analysis, data from 10 consecutive survey cycles, encompassing a total of 101,316 participants, were utilized. All participants signed informed consent, and the NCHS Ethics Review Board authorized the study protocols. Participants with the age of 20 years or older were included (n = 55,081), while those with unavailable stroke data (n = 81) and missing EASIX values (n = 11,147) were excluded. Ultimately, 43,853 participants fulfilled the inclusion criteria and were enrolled, where 1674 participants were diagnosed with stroke. Further, 1671 stroke participants were enrolled to determine the interplay between EASIX and mortality outcomes in stroke participants, except for three participants missing mortality data (Fig. 1).

Study flowchart.
Exposure: EASIX
Data on LDH, creatinine, and PLT were collected, thereby calculating the EASIX using the formula outlined previously9: EASIX= [LDH (U/L) × creatinine (mg/dL)] / PLT (109/L).
Outcome: stroke
Within the NHANES, stroke information is collected through participant questionnaires. Stroke was identified relying upon self-reported diagnoses validated by a physician in face-to-face interviews. Specifically, individuals who answered “yes” to “Have you ever been told by a physician or health professional that you had a stroke?” were categorized as having experienced a stroke.
Outcome: ACM and CVM
The mortality outcomes of this study included ACM and CVM, referring to death from any cause and death specifically attributed to cardiovascular diseases, respectively. Importantly, CVM was identified through the International Classification of Diseases-10 coding system. CVM was characterized by cardio- and cerebrovascular diseases under the codes of I00-I09, I11, I13, I20-I5, and I60-I69. Mortality data were acquired through the National Death Index (NDI) and related to NHANES data up to December 31, 2019.
Covariates
Building on established research and biological rationale, we selected a broad set of factors known to impact stroke outcomes. Specifically, we accounted for demographic attributes (age, sex, and race/ethnicity), socioeconomic indicators (marriage status, educational level, and poverty-income ratio), lifestyle and health-associated measures (BMI, smoking habits, alcohol consumption, health insurance coverage, and systolic/diastolic blood pressure [SBP/DBP]), a range of comorbidities (including hypertension, diabetes, hyperglycemia, liver conditions, coronary heart disease [CHD], angina, myocardial infarction, chronic kidney disease [CKD], cancer, and congestive heart failure [CHF]), as well as laboratory parameters (hemoglobin, PLT, estimated glomerular filtration rate (eGFR), total cholesterol, HDL-C, non-HDL-C, LDH, and creatinine). By adjusting for these variables, we aimed to minimize confounding effects and reinforce the reliability of our analysis on the relationship between EASIX and both stroke prevalence and associated mortality outcomes.
Statistical analysis
In our analyses, we accounted for masked variance and applied a weighting methodology19. Given that our study included hematology variables, we chose to use the Mobile Examination Centers (MEC) weights18,20, as the MEC weights were specifically developed to adjust for complex sampling design and non-response biases in data collected through the Mobile Examination Centers, encompassing physical examination components (e.g., blood pressure measurements) and laboratory analyses of biological specimens. For the 1999–2002 cycles, we applied the weight calculation formula of 2/10 × wtmec4 year, while for the 2003–2018 cycles, we used the formula 1/10 × wtmec2 year19,20. Participant characteristics were systematically described and compared on the basis of stroke presence or absence. Non-normally distributed continuous variables are described as median values and interquartile ranges (IQR), while expressing categorical variables as proportions. Baseline attributes between stroke and non-stroke groups were ascertained via chi-square tests for categorical variables while employing t-tests for continuous variables. To investigate the relationship between EASIX (treated either as a continuous variable or categorized into quartiles) and the occurrence of stroke, we utilized weighted multivariable logistic regression. As for mortality outcomes of stroke, multivariable Cox regression analyses were employed. The models were structured as follows: Unadjusted Model 1; Model 2 adjusted for age, gender, and race/ethnicity; and Model 3 further adjusted for smoking status, alcohol consumption, BMI, hypertension, diabetes, hyperlipidemia, CHD, CKD, CHF, SBP, non-HDL-C, and cancer.
Furthermore, Kaplan-Meier survival curves were deployed, aiming at evaluating the association between EASIX and both ACM and CVM among patients who experienced a stroke. To define potential non-linear relations between EASIX (as a continuous variable) and stroke-related mortality outcomes, we utilized restricted cubic splines (RCS) with knots placed at the 5th, 35th, 65th, and 95th percentiles. Subgroup analyses were conducted to further elucidate the interplay between EASIX and stroke prevalence and mortality outcomes. Additionally, interaction tests among covariates were conducted, and the findings were visualized using forest plots. We performed receiver operating characteristic (ROC) curve analyses to determine the optimal cutoff values of EASIX and measured the area under the curve to assess the predictive value of EASIX for stroke prevalence and mortality outcomes. Statistical analyses were conducted through R software version 4.3.2 (http://www.R-project.org), determining statistical significance using a two-tailed P < 0.05.
Results
Baseline attributes of the participants
Among the 43,853 enrolled participants, representing over 1.7 billion U.S. individuals, 1,674 had experienced a stroke, corresponding to an estimated 48 million stroke cases in the U.S. Table 1 offers a detailed descriptive analysis distinguishing between participants with and without a stroke. The demographic data reveal a notably higher median age in the stroke group (69 years), unlike the non-stroke group (48 years). Additionally, the stroke group showed a slightly lower percentage of female participants and a diverse ethnic distribution, with significant variations in marital status and educational levels compared to their non-stroke counterparts.
In terms of health indicators, stroke participants had a higher BMI and increased prevalence of smoking and alcohol consumption. The analysis also recorded higher mean SBP/DBP among stroke patients. Comorbid conditions: Hypertension, diabetes, hyperlipidemia, CHD, and other cardiovascular and renal pathologies were markedly more prevalent in the stroke group, highlighting the burden of these comorbidities on stroke risk. Laboratory parameters further supported these findings, with stroke patients displaying lower hemoglobin levels, non-HDL-C, reduced eGFR, and elevated creatinine levels, indicating a poorer overall health status (Table 1). It is important to note that a significant number of patients had missing EASIX values (n = 11,147), which were excluded from the analysis. To assess the potential bias introduced by excluding these individuals, we compared the baseline characteristics of those included in the analysis with those excluded. The detailed statistical results are presented in Supplemental Table S1.
Relationship between the EASIX and the presence of stroke
Table 2 shows a positive interconnection between EASIX and stroke before and after confounder adjustment (odds ratio [ORunadjusted] = 1.53, 95% confidence interval [CI]: 1.43–1.64; ORfull−adjusted = 1.16, 95% CI: 1.07–1.25, correspondingly). Unlike the participants whose EASXI was in the lowest quartile (Q1) group, the likelihood of having a stroke was increased by 54% in the highest quartile group (Q4) (ORfull−adjusted = 1.54, 95% CI: 1.20–1.96, P < 0.001).
Interplay between the EASIX and mortality outcomes in stroke participants
During a median follow-up of 71.00 months (95% CI: 77.48–82.63), a total of 743 deaths were recorded among 1671 stroke patients (44.46%), where 225 (13.46%) participants were dead of cardiovascular diseases. Table 3 shows the baseline characteristics of these stroke patients by EASIX quartiles.
Following the adjustment for all confounders, EASIX was related to a 30% increase in ACM and a 29% increase in CVM among stroke patients (hazard ratio [HRfull−adjusted] = 1.30, 95%CI: 1.17–1.44; HRfull−adjusted = 1.29, 95%CI: 1.06–1.58, correspondingly). Compared to patients whose EASIX was the lowest quartile (Q1) group, those who had the highest EASIX (Q4) showed a significantly increased risk of ACM and CVM (Table 4).
Kaplan-Meier survival curves further corroborated these findings, illustrating that participants in the highest quartile (Q4) of the EASIX displayed significantly elevated mortality rates for both ACM and CVM in comparison to those in the lowest quartile (Q1) (Figs. 2A, B). Altogether, a higher EASIX is consistently related to escalated risks of mortality outcomes in individuals who have experienced a stroke.

Kaplan-Meier plots for (A) ACM and (B) CVM in individuals with stroke.
Nonlinear relationship of the EASIX and prevalence and mortality outcomes of stroke
The RCS plot showcased a nonlinear interplay between the EASIX and stroke prevalence (Fig. 3A, Pnonlinear < 0.001) and ACM (Fig. 3B, Pnonlinear < 0.001) and CVM (Fig. 3C, Pnonlinear = 0.05) among stroke patients. These RCS analyses collectively indicate that the EASIX is a potent predictor not just for stroke but also for mortality outcomes related to any cause and cardiovascular-specific causes. The presence of non-linear relationships in these analyses underscores the complexity of the EASIX’s predictive capacity, suggesting that different EASIX values may have disproportionately high risks. This necessitates careful clinical evaluation and potentially targeted interventions based on EASIX thresholds to mitigate these risks.

RCS analysis with multivariate-adjusted interplays between the EASIX and (A) the prevalence, (B) ACM, and (C) CVM of stroke. The solid red lines correspond to the central estimates, and the red-shaded regions indicate 95% CIs.
Subgroup analysis and interaction test of the EASIX and the prevalence and mortality outcomes of stroke
The outcomes of the subgroup analysis are presented in Fig. 4. Regarding stroke prevalence, EASIX showed a positive correlation with stroke in subgroups of age over 60 years, male, Hispanic populations, hypertension, hyperlipidemia, non-CHD, non-CKD, non-cancer, and non-diabetes (all P < 0.05). Interactions were observed between EASIX and hypertension, CHD, CKD, cancer, and diabetes (all P < 0.05).
Regarding ACM, in most subgroups, EASIX showed a positive correlation with ACM except for age < 60 years (P = 0.12). Regarding CVM, EASIX showed a positive correlation with stroke in subgroups of age over 60 years, male, Hispanic populations, hypertension, hyperlipidemia, CHD, non-CKD, non-cancer, and diabetes (all P < 0.05). The interaction test revealed no significant interactions between EASIX and any categorical covariates for CVM (all Pinteraction > 0.05), and most categorical covariates for ACM except for gender (Pinteraction = 0.03).

Subgroup analysis as well as interaction test of the interplay between EASIX and (A) the prevalence, (B) ACM, (C) and CVM of stroke. The black rectangles correspond to the central estimates, and The black lines indicate the 95% CIs.
The predictive value of EASIX for stroke prevalence and mortality outcomes
According to Model 3, the ROC curves illustrated that the cutoff value of EASIX for stroke incidence and CVM was 0.56, and 0.58 for ACM, with an AUC of 0.663 (95% CI: 0.649–0.677) for stroke prevalence, as well as for ACM with an AUC of 0.620 (95% CI: 0.595–0.649) and for CVM with an AUC of 0.587 (95% CI: 0.549–0.626) (Fig. 5).

The ROC curves of EASIX for predicting (A) stroke prevalence, (B) ACM, and (C) CVM.
Discussion
This cohort study, encompassing 43,853 participants representing over 1.7 billion U.S. residents, analyzed 1999–2018 NHANES data to delve into the interplay between the EASIX and the prevalence and mortality outcomes of stroke. The findings revealed a significant positive non-linear link between the prevalence and mortality outcomes of this population. A higher EASIX was related to an escalated stroke prevalence and mortality outcomes, with significant differences persisting among Q3/Q4 compared to Q1, even in fully adjusted models for stroke risk and ACM, as well as statistical differences in Q4 compared to Q1 for CVM. Interaction analysis showed no significant interactions between EASIX and any categorical covariates for CVM, whereas significant interaction effects were observed between EASIX and the prevalence of stroke in categorical covariates: Hypertension, diabetes, and CHD, as well as between EASIX and ACM in the categorical covariate of gender. Taken together, EASIX may be a reliable marker for the ultimate prediction of the prevalence and mortality outcomes of stroke, making it a practical tool for prognosis. Additionally, the findings indicate that improving endothelial function through interventions could be a promising strategy to decrease the prevalence and mortality of stroke.
EASIX was originally developed and validated as a reliable overall survival predictor in patients who have steroid-refractory graft-versus-host disease after transplantation of allogeneic stem cells, a condition related to thrombotic microangiopathy via endothelial malfunction9. Subsequently, EASIX prognostic significance, which integrates LDH, serum creatinine, and PLT, has been validated in a variety of patient populations. These include individuals with diffuse large B-cell lymphoma, multiple myeloma, lower-risk myelodysplastic syndromes, small-cell lung cancer, COVID-19, sepsis, and coronary artery disease12,13,14,15,16,17, as well as critically ill patients who have advanced liver disease, cancer, and acute myocardial infarction21,22,23. Additionally, a significant connection has been demonstrated between EASIX and various endothelial activation markers: IL-18, CXCL8/9, insulin-like growth factor-1,angiopoietin-2, tumorigenicity-2 suppressor, and soluble thrombomodulin10,11.
As an endothelial injury marker, EASIX is easily clinically obtainable and cost-effective for evaluating complication risk and prognosis. The LDH component of EASIX increases because of its release from damaged endothelium, PLTs, and leukocytes once the vascular endothelium is compromised24,25. Endothelial malfunction represents a pivotal pathophysiological mechanism in numerous renal diseases: Acute kidney injury, CkD, and diabetic nephropathy26,27,28. Elevated serum creatinine levels reflect the impact of renal endothelial malfunction on impaired kidney functionality. Furthermore, reduced PLT levels may partially result from endothelial injury and complement activation. Vascular endothelial damage leads to increased exposure of collagen, tissue factor, and von Willebrand factor, which promote PLT hyperactivation and aggregation29. Previous studies have confirmed that levels of LDH, serum creatinine, and PLT are associated with stroke mortality30,31,32. However, the combined correlation of these EASIX components with the prevalence and prognosis of stroke as indicators of vascular endothelial injury has yet to be fully established.
Herein, EASIX was significantly escalated in stroke participants and was efficient in mortality outcome prediction. Multiple mechanisms may elucidate the interplay between EASIX and both stroke prevalence and mortality. First, endothelial dysfunction compromises vascular homeostasis: under normal conditions, endothelial cells regulate vascular tone, inflammation, and coagulation by secreting nitric oxide (NO) as well as endothelin-1 (ET-1). When dysfunction occurs, NO production decreases while ET-1 increases, causing persistent vasoconstriction, thrombosis, and a pro-inflammatory milieu conducive to stroke33. Second, a breach of the BBB intensifies neuronal damage; altered tight junctions allow infiltration of toxic substances and inflammatory mediators, fostering cerebral edema, lesion expansion, and increased mortality34. Third, chronic low-grade inflammation and oxidative stress form a vicious cycle that accelerates vascular wall injury and plaque destabilization, exacerbating lesion growth and neuronal necrosis35. Fourth, vascular remodeling and microcirculatory deficits arise from long-standing endothelial dysfunction, reducing vascular compliance and impairing autoregulation, thus magnifying infarct size and lethality36. Finally, during acute stroke, endothelial dysfunction heightens ischemia-reperfusion injury and hemorrhagic transformation, while in later stages, impaired vascular repair elevates recurrence risk and long-term mortality37. Given these findings, interventions aimed at restoring endothelial function—through rigorous risk-factor control (e.g., hypertension, dyslipidemia, diabetes), balancing vasoactive substances, and dampening oxidative stress—may reduce both initial and recurrent strokes. Ongoing studies into molecular signaling pathways such as endothelial NO synthase, prostaglandin I2, and ET-1 could inspire novel therapies that transform stroke prevention and treatment.
Strengths and limitations
The present study possesses diverse considerable strengths. First, the sample was derived from a nationally representative cohort, and by applying the appropriate NHANES weights, the findings are generalizable to the whole U.S. stroke patient population. This enhances the external validity of our results. Second, this research is pioneering in its examination of the relationship between the EASIX and both the prevalence and mortality outcomes of stroke. Moreover, we defined a significant non-linear, positive correlation between the EASIX and both stroke prevalence and mortality outcomes, with higher EASIX scores being related to heightened stroke prevalence and mortality risks. Third, the robustness of our findings was reinforced through comprehensive statistical analyses, which confirmed the stability of the observed associations. By utilizing the EASIX—a comprehensive marker of reflecting endothelial function—to assess the prevalence and mortality outcomes of stroke, our study facilitates earlier and more effective clinical interventions, which is crucial for improving national health outcomes and extending life expectancy.
However, the study also has several limitations. Firstly, the cross-sectional design of the NHANES dataset limits our ability to establish causality, as it only allows for the identification of associations between EASIX and stroke prevalence and mortality outcomes. Since we cannot track changes over time or assess the temporal relationship between EASIX levels and the onset or progression of stroke, the current study is unable to determine whether elevated EASIX levels are a cause or a consequence of stroke. To establish causal relationships, future longitudinal studies are needed. Such studies, which follow participants over time, could provide clearer insights into the role of EASIX in stroke and enhance our understanding of its potential as a biomarker. Secondly, we have explicitly acknowledged the statistical significance of the differences between the included and excluded samples for various variables, highlighting the potential presence of selection bias. We emphasize that such bias could limit the generalizability of the findings. To address this, we have employed weighted statistical analyses to correct for the impact of selection bias in this study. Furthermore, future research could benefit from using techniques such as propensity score matching to further mitigate the influence of selection bias. Thirdly, since NHANES is a U.S.-based dataset comprising participants exclusively from the U.S., the generalizability of our findings to global populations is limited. Consequently, further validation studies conducted in diverse countries and among various ethnic groups are essential. This is particularly important for regions such as Asia, which has a large and diverse population, as such studies could provide valuable insights into the applicability of our findings across different demographic groups. Although our sample size was substantial, future research could benefit from an even larger cohort to provide more nuanced insights. Additionally, despite adjusting for numerous conventional variables, our analysis did not account for probable confounders: Stroke subtype and clinical severity scales like the National Institutes of Health Stroke Scale or the Glasgow Coma Scale. These factors could influence mortality outcomes and should be considered in future studies. Lastly, It should be noted that self-reported data may be subject to recall bias, potentially affecting result accuracy. The NHANES database does not provide details on stroke subtypes, limiting exploration of the link between EASIX and different types of stroke. Nonetheless, because ischemic stroke is more common and generally has higher survival rates than hemorrhagic stroke, most stroke cases in this study population are likely ischemic. To address these limitations, we plan to collect detailed clinical data from hospital records, extend the sample size, and compare the predictive EASIX value with other markers of reflecting endothelial function in assessing the prevalence and mortality outcomes of stroke.
Conclusion
The EASIX demonstrated a positive non-linear association with the prevalence and mortality outcomes amongst individuals aged 20 years and above who experienced a stroke, as identified in the NHANES dataset. Heightened EASIX scores were significantly connected with an escalated risk of both stroke prevalence and mortality outcomes. Taken together, EASIX may be a valuable biomarker for assessing mortality risks in stroke patients and stroke prevalence. Looking forward, implementing the EASIX in primary care settings could facilitate the early screening of endothelial function, thereby identifying high-risk patients and guiding appropriate referrals for specialized medical care. This can enhance patient outcomes and reduce mortality rates among those who have suffered a stroke. Nevertheless, further validation in diverse countries and among various ethnic groups is necessary.
Data availability
Available upon a reasonable request from the corresponding author.
References
Imoisili, O. E., Chung, A., Tong, X., Hayes, D. K. & Loustalot, F. Prevalence of Stroke - Behavioral risk factor surveillance system, united states, 2011–2022. MMWR Morb Mortal. Wkly. Rep. 73, 449–455. https://doi.org/10.15585/mmwr.mm7320a1 (2024).
Massot, A. et al. Decreased levels of angiogenic growth factors in intracranial atherosclerotic disease despite severity-related increase in endothelial progenitor cell counts. Cerebrovasc. Dis. 35, 81–88. https://doi.org/10.1159/000346097 (2013).
Bohm, F. & Pernow, J. The importance of endothelin-1 for vascular dysfunction in cardiovascular disease. Cardiovasc. Res. 76, 8–18. https://doi.org/10.1016/j.cardiores.2007.06.004 (2007).
Roberts, A. C. & Porter, K. E. Cellular and molecular mechanisms of endothelial dysfunction in diabetes. Diab Vasc Dis. Res. 10, 472–482. https://doi.org/10.1177/1479164113500680 (2013).
Shekhar, S. et al. Targeting vascular inflammation in ischemic stroke: recent developments on novel Immunomodulatory approaches. Eur. J. Pharmacol. 833, 531–544. https://doi.org/10.1016/j.ejphar.2018.06.028 (2018).
Gong, S. et al. Endothelial conditional knockdown of NMMHC IIA (Nonmuscle myosin heavy chain IIA) attenuates Blood-Brain barrier damage during Ischemia-Reperfusion injury. Stroke 52, 1053–1064. https://doi.org/10.1161/STROKEAHA.120.031410 (2021).
Yang, K. et al. A systematic review of the research progress of non-coding RNA in neuroinflammation and immune regulation in cerebral infarction/ischemia-reperfusion injury. Front. Immunol. 13, 930171. https://doi.org/10.3389/fimmu.2022.930171 (2022).
Li, Y. J., Shi, S. X., Liu, Q., Shi, F. D. & Gonzales, R. J. Targeted role for sphingosine-1-phosphate receptor 1 in cerebrovascular integrity and inflammation during acute ischemic stroke. Neurosci. Lett. 735, 135160. https://doi.org/10.1016/j.neulet.2020.135160 (2020).
Luft, T. et al. EASIX in patients with acute graft-versus-host disease: a retrospective cohort analysis. Lancet Haematol. 4, e414–e423 (2017).
Kordelas, L. et al. EASIX-1 year and late mortality after allogeneic stem cell transplantation. Blood Adv. https://doi.org/10.1182/bloodadvances.2022008617 (2023).
Luft, T. et al. EASIX and mortality after allogeneic stem cell transplantation. Bone Marrow Transpl. 55, 553–561. https://doi.org/10.1038/s41409-019-0703-1 (2020).
Song, G. Y. et al. Endothelial activation and stress index (EASIX) is a reliable predictor for overall survival in patients with multiple myeloma. BMC Cancer. 20, 803. https://doi.org/10.1186/s12885-020-07317-y (2020).
Pérez-García, F. et al. Age-adjusted endothelial activation and stress index for coronavirus disease 2019 at admission is a reliable predictor for 28-day mortality in hospitalized patients with coronavirus disease 2019. Front. Med. 8, 736028. https://doi.org/10.3389/fmed.2021.736028 (2021).
Park, S., Go, S. I. & Lee, G. W. The endothelial activation and stress index (EASIX) score is an independent prognostic factor in patients with difuse large B-cell lymphoma. BMC Cancer. 22, 816. https://doi.org/10.1186/s12885-022-09915-4 (2022).
Go, S. I. et al. Endothelial activation and stress index (EASIX) as a predictive biomarker in small cell lung cancer. Cancer Biomark. 35, 217–225. https://doi.org/10.3233/CBM-220032 (2022).
Xu, H. B. et al. Association between endothelial activation and stress index and 28-day mortality in septic ICU patients: a retrospective cohort study. Int. J. Med. Sci. 20, 1165–1173. https://doi.org/10.7150/ijms.85870 (2023).
Finke, D., Hund, H., Frey, N., Luft, T. & Lehmann, L. H. EASIX (endothelial activation and stress index) predicts mortality in patients with coronary artery disease. Clin. Res. Cardiol. https://doi.org/10.1007/s00392-024-02534-y (2024).
Paulose-Ram, R., Graber, J. E., Woodwell, D. & Ahluwalia, N. The National health and nutrition examination survey (NHANES), 2021–2022: adapting data collection in a COVID-19 environment. Am. J. Public. Health. 111, 2149–2156. https://doi.org/10.2105/ajph.2021.306517 (2021).
Johnson, C. L. et al. 1999–2010. Vital Health Stat. 2 2013(161), 1–24 .
NHANES questionnaires, datasets, and related documentation. https://wwwn.cdc.gov/nchs/nhanes/Default.aspx. [Accessed May 25 2024].
Schult, D., Rasch, S., Schmid, R. M., Lahmer, T. & Mayr, U. EASIX is an accurate and easily available prognostic score in critically ill patients with advanced liver disease. J. Clin. Med. 12, 2553. https://doi.org/10.3390/jcm12072553 (2023).
Deng, F., Lin, J. & Lin, H. Association between EASIX and acute kidney injury in critically ill cancer patients. BMC Nephrol. 25, 453. https://doi.org/10.1186/s12882-024-03887-2 (2024).
Sang, M., Ma, X., Zhu, F., Zhu, C. & Ying, Z. Association between endothelial activation and stress index and 30-day mortality risk in acute myocardial infarction patients: a study based on the medical information Mart for intensive care-IV database. BMC Cardiovasc. Disord. 24, 699. https://doi.org/10.1186/s12872-024-04353-5 (2024).
Coppo, P. et al. Predictive features of severe acquired ADAMTS13 defciency in idiopathic thrombotic microangiopathies: the French TMA reference center experience. PLoS ONE. 5, e10208. https://doi.org/10.1371/journal.pone.0010208 (2010).
Chopra, J., Joist, J. H. & Webster, R. O. Loss of 51chromium, lactate dehydrogenase, and 111indium as indicators of endothelial cell injury. Lab. Investig. 57, 578–584 (1987).
Verma, S. K. & Molitoris, B. A. Renal endothelial injury and microvascular dysfunction in acute kidney injury. Semin Nephrol. 35, 96–107. https://doi.org/10.1016/j.semnephrol.2015.01.010 (2015).
Cheng, H. & Harris, R. C. Renal endothelial dysfunction in diabetic nephropathy. Cardiovasc. Hematol. Disord Drug Targets. 14, 22–33. https://doi.org/10.2174/1871529x14666140401110841 (2014).
Malyszko, J. Mechanism of endothelial dysfunction in chronic kidney disease. Clin. Chim. Acta. 411, 1412–1420. https://doi.org/10.1016/j.cca.2010.06.019 (2010).
Carrizzo, A. et al. The main determinants of diabetes mellitus vascular complications: endothelial dysfunction and platelet hyperaggregation. Int. J. Mol. Sci. 19, 2968. https://doi.org/10.3390/ijms19102968 (2018).
Jin, H. et al. Elevated serum lactate dehydrogenase predicts unfavorable outcomes after rt-PA thrombolysis in ischemic stroke patients. Front. Neurol. 13, 816216. https://doi.org/10.3389/fneur.2022.816216 (2022).
Zhong, Y. et al. Association between serum creatinine and 30 days all-cause mortality in critically ill patients with non-traumatic subarachnoid hemorrhage: analysis of the MIMIC-IV database. Front. Neurol. 15, 1359749. https://doi.org/10.3389/fneur.2024.1359749 (2024).
Wang, L. X., Liu, R. L., Zhou, P., Hu, H. F. & Deng, Z. Nonlinear relationship between platelet count and 30-day in-hospital mortality in intensive care unit stroke patients: a multicenter retrospective cohort study. Front. Neurol. 15, 1374159. https://doi.org/10.3389/fneur.2024.1374159 (2024).
de la Riva, P., Marta-Enguita, J., Rodríguez-Antigüedad, J., Bergareche, A. & de Munain, A. L. Understanding endothelial dysfunction and its role in ischemic stroke after the outbreak of recanalization therapies. Int. J. Mol. Sci. 25, 11631. https://doi.org/10.3390/ijms252111631 (2024).
Rosenberg, G. A. Neurological diseases in relation to the blood-brain barrier. J. Cereb. Blood Flow. Metab. 32, 1139–1151. https://doi.org/10.1038/jcbfm.2011.197 (2012).
Iadecola, C. & Anrather, J. The immunology of stroke: from mechanisms to translation. Nat. Med. 17, 796–808. https://doi.org/10.1038/nm.2399 (2011).
Tregub, P. P., Averchuk, A. S., Baranich, T. I., Ryazanova, M. V. & Salmina, A. B. Physiological and pathological remodeling of cerebral microvessels. Int. J. Mol. Sci. 23, 12683. https://doi.org/10.3390/ijms232012683 (2022).
Chamorro, Á., Dirnagl, U., Urra, X. & Planas, A. M. Neuroprotection in acute stroke: targeting excitotoxicity, oxidative and nitrosative stress, and inflammation. Lancet Neurol. 15, 869–881. https://doi.org/10.1016/S1474-4422(16)00114-9 (2016).
Acknowledgements
We thank the dedicated researchers, staff, and NHANES study participants, whose invaluable participation provided the critical data and methodological foundation for our research.
Funding
The National Natural Science Foundation of China (NSFC; 82400758) and the NHC Key Laboratory of Nuclear Technology Medical Transformation at Mianyang Central Hospital (2023HYX032).
Author information
Authors and Affiliations
Contributions
The study was conceptualized by Yongwei Huang, Zongping Li, and Xiaoshuang Yin. Data extraction, compilation, and analysis were carried out by Yongwei Huang, Jianjun Wang, and Decai Wang. Xiaoshuang Yin was responsible for the development of tables and figures. The manuscript was drafted and refined through the collaborative efforts of all authors, with each contributing significantly and approving the final submission.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This research adhered to the Declaration of Helsinki. The NHANES database was cleared for usage by the NCHS Review Committees under the auspices of the CDC. Due to the database’s public accessibility and the presence of de-identified patient information, with no need for further ethical approval or informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, Y., Li, Z., Wang, J. et al. Endothelial activation and stress index is a reliable predictor for the prevalence and mortality outcomes of stroke. Sci Rep 15, 23285 (2025). https://doi.org/10.1038/s41598-025-06595-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-06595-5
Keywords
This article is cited by
-
Endothelial Activation and Stress Index (EASIX) as a novel index associated with no-reflow phenomenon in STEMI: a bi-center retrospective study
BMC Cardiovascular Disorders (2026)
-
Association between the endothelial activation and stress index and the risk of severe consciousness disorder and in-hospital mortality in ICU patients with non-traumatic intracerebral hemorrhage: A retrospective analysis based on the MIMIC database
Neurosurgical Review (2026)
