
Abstract
Worldwide, thousands of people suffer from laryngeal diseases, many of which involve the posterior glottis or subglottis. These laryngeal areas are challenging to visualize with conventional transnasal and transoral laryngoscopes because the view from above is obscured by the disease itself, thereby limiting the efficacy of endoscopy in diagnosis and treatment. Advancements in miniaturized optical systems overcome these limitations and allow for real-time visualization of difficult-to-access laryngeal subsites such as the posterior glottis and subglottis. The present study introduces a novel device, the subglottic imaging puncture scope (SIPS), to access and image the subglottic space via a transcervical puncture. The SIPS has a miniature, high-resolution camera integrated within a medical-grade gauge 18 needle. The small-diameter needle allows for minimal invasiveness, similar to established laryngeal therapeutic drug delivery techniques. A detailed description of the camera and light source alignments are provided. Images from video footage obtained in human cadavers are provided, validating the hypothesis that a minimally invasive device allows imaging of the subglottis. The SIPS will improve diagnostic accuracy and patient comfort, enabling the full extent of subglottic pathology to be imaged on awake patients in a clinical office setting.
Similar content being viewed by others

Introduction
Subglottic stenosis may result from airway manipulation during endotracheal intubation or idiopathic etiologies. While mechanical injury is the most frequent cause of subglottic stenosis, dysregulated immune responses by T-cells in the subglottic mucosa can also contribute to severe stenosis due to collagen and extracellular matrix deposition in idiopathic cases1,2,3,4,5.
Direct visualization of the posterior glottis and subglottis is an essential part of accurately diagnosing the extent and severity of the disease. Imaging the subglottic space can differentiate between subglottic stenosis6,7, posterior glottic stenosis and diastasis8,9, infracordal and subglottic pathology10,11, and laryngeal tumors12,13.
Transnasal/transoral laryngoscopy remains the primary method for visualizing the larynx and upper airway. Flexible laryngoscopes, which are inserted through the nose and follow the path through the nasopharynx and oropharynx to reach the larynx, can cause significant discomfort, irritation, and a feeling of nausea14,15,16. While local anesthetics, nasal decongestants, topical anesthetics, lubricants, saline irrigation, and visual distractions are commonly used to reduce discomfort, many patients continue to experience distress due to the sensation of the instrument passing through the nose into the throat17,18,19,20. More importantly, optimal visualization is often limited by an inability to pass the scope beyond or through the stenosis to assess the inferior extent of the disease.
Alternatively, laryngoscopy can be conducted in the operating room while the patient is asleep with general anesthesia. Nevertheless, this involves the inherent risk of general anesthesia in people who already have a compromised airway and can directly contribute to further morbidity17,18,19,20,21,22.
Given the limitations in subglottic imaging via conventional means, there is a clear need for a method to visualize the subglottis space more optimally. Ideally, the diagnostic device would enable the examination in an awake patient with topical anesthesia rather than the operating room with general anesthesia. Such a tool would be particularly valuable for evaluating patients with chronic conditions not associated with acute airway compromise—such as stable cases of glottic or subglottic stenosis or vocal fold immobility—typically assessed in an ENT clinic. The imaging system should be safe, effective, easy to use, tolerable, and cost-effective to ensure broad accessibility and become a routine part of subglottic assessment.
Recent advancements in microfabrication techniques in photonics, including reductions in pixel size and the application of wafer-level optics (WLO), have facilitated the development of high-resolution, miniaturized optical systems, with cameras now reduced to sub-millimeter-scale dimensions. WLO uses semiconductor stacking techniques to create optical elements in layered wafer structures23, allowing for the combination of image sensors and lenses into a single compact camera unit24. These fully integrated systems produce ultra-thin devices that provide high-quality imaging, making them ideal for designing smaller, less invasive endoscopic instruments. They are particularly beneficial in medical disciplines such as ear, nose, and throat (ENT), where precise visualization is essential. For instance, these systems have been integrated into cochlear implant electrode arrays for human cadaveric temporal bone studies, enabling continuous visual guidance to minimize electrode contact with the cochlear wall25. Other examples include robotic bronchoscope systems for navigating and performing biopsies on pulmonary lesions26 and angioscopic solutions for endovascular interventions27. The ultra-small dimensions of these systems facilitate access to hard-to-reach areas, offering new opportunities for minimally invasive clinical evaluations that enhance diagnostic precision while improving patient comfort.
This study introduces the subglottic imaging puncture scope (SIPS), which integrates a sub-millimeter-sized camera into a medical-grade gauge 18 needle. SIPS facilitates access to the subglottic area via transcervical puncture and allows real-time visual monitoring of different laryngeal subsites28.
Material and methods
Optical system
The optical system in the SIPS incorporates the OCHTA10 camera, providing a 400 × 400-pixel resolution with a 1 μm pixel size24. This compact unit, measuring 0.65 × 0.65 mm2 with a z-height of 1.19 mm, integrates essential components such as the image array, signal processing, control circuitry, and microlenses into a single chip module. The system delivers high-quality images and video up to 30 frames per second. For illumination, there are three multimode optical fibers with a core size of 100 μm, a cladding thickness of 10 μm, and a numerical aperture of 0.22 (Edmund Optics, United States) that were connected to an external cold white light emitting diode (LED, MCWHF2, Thorlabs, United States). The captured images were processed by a video bridge chip that converts analog signals to digital format, and the digital signals were displayed on a computer for real-time analysis.
Manufacturing of the SIPS device
A medical-grade gauge 18 needle with a thin wall (inner diameter 0.91 mm, outer diameter 1.27 mm; Shaotong, China) was used. The micro-camera OCHTA10 and illumination source (optical fibers) were positioned within polyimide tubing (MicroLumen, United States), serving as a trocar system, and this assembly was then inserted into the needle. The system was secured into the polyimide tubing with OrmoComp®, a UV-curable biocompatible polymer (Kayaku Advanced Materials, Westborough, United States).
Cadaveric human specimens
Four cadaveric human specimens were used to validate the SIPS device. The cadavers were prepared and studied in the anatomical laboratory at Feinberg School of Medicine, Northwestern University, in compliance with institutional ethical guidelines (for more details, see the statement of ethics in this manuscript). They were carefully preserved and prepared to maintain anatomical integrity, particularly in the subglottic area relevant to the study. The SIPS was tested under simulated clinical conditions to evaluate its ability to provide real-time visualization. No live human subjects were involved, and all procedures adhered to ethical standards and regulatory approvals.
Insertion procedure for subglottic access
The SIPS device was inserted into the airway at the level of the subglottis via transcervical puncture through the cricothyroid space. After inserting the gauge 18 needle, the trocar system—housing the micro-camera and illumination source—was carefully advanced through the needle to the target area. This technique enabled the delivery of the micro-camera into an area that would be optimal for subglottic imaging. Real-time visualization guided the insertion, ensuring accurate placement and continuous observation of the subglottis.
Statement of ethics
The study adhered to the ethical guidelines of the Declaration of Helsinki, including the 2013 (7th revision) updates, for research involving human subjects. Human cadaveric specimens were donated to the Feinberg School of Medicine, Northwestern University, for educational and research purposes. The management of the human bodies was conducted according to the donors’ informed consent or under a waiver granted by the Institutional Review Board (IRB) or Ethics Committee, in compliance with 45 CFR 46, the Protection of Human Subjects regulations. The procedure was reviewed by Northwestern University’s IRB and classified as a non-human research study under reference number STU00221992.
Results
Prototyping
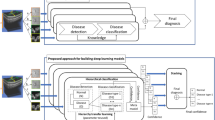
Figure 1 shows a prototype of the SIPS device, with the optical system housed in polyimide tubing and placed within a gauge 18 medical-grade needle. The polyimide tubing can easily slide into the needle, allowing precise positioning. At the front of the SIPS, two bright spots represent the light emitted from the optical fibers (Fig. 1B).

SIPS device. (A) Full view of the medical-grade gauge 18 needle (inner diameter 0.91 mm, outer diameter 1.27 mm) with the integrated optical system. Scale bar: 10 mm. (B) Magnified view of the needle tip with the micro-camera OCHTA10 and illumination source (three multimode optical fibers connected to a cold white LED) housed in an ultra-thin wall polyimide tubing. These fibers were secured using the polymer OrmoComp. Scale bar: 2 mm.
Performance of the SIPS device
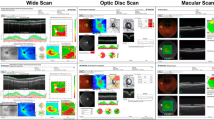
After inserting the needle into the subglottis of the cadaveric human specimen, the trocar system was introduced to check for any tissue obstruction. Once verified, the trocar was advanced easily to reach the target region. Real-time video (Supplementary Information) was recorded, maintaining continuous visualization for precise imaging. The intensity of light delivered and micro-camera resolution were adequate for visualization of laryngeal subsites, including the rima glottidis, undersurface of the vocal folds (Fig. 2A), and epiglottis (Fig. 2B).

Images of the glottic and supraglottic spaces acquired with the SIPS from the subglottic area in a cadaveric human subject. (A) Rima glottidis, left and right posterior vocal folds. (B) Epiglottis and right vestibular fold.
Discussion
This study describes SIPS, a novel miniaturized optical system that integrates a sub-millimeter-sized camera within a medical-grade needle for minimally invasive subglottic imaging and diagnostics in individuals with non-acute airway compromise. Designed for transcervical insertion using an 18-gauge needle, SIPS enables direct visualization of the subglottis—a laryngeal subsite not adequately accessed by conventional methods—in a clinical office setting and without general anesthesia. With a diameter of 1.27 mm, SIPS provides a significantly smaller alternative to flexible laryngoscopes, which typically range from 1.8 to 3.5 mm in diameter, cannot be inserted via transcervical puncture, and generally do not extend beyond the glottis to reach the subglottic space. By offering direct access through a minimally invasive approach, SIPS has the potential to reduce patient discomfort, shorten diagnostic timelines, and enable in-office assessment of a region that currently lacks adequate direct visualization.
The micro‐camera OCHTA10, shown in Fig. 1, fits within the lumen of a gauge 18 needle. The thin-wall design increases the internal lumen to house the optical system. Medical-grade needles are available in different wall thicknesses—regular, thin, extra-thin, and ultra-thin. The assembly could also be placed into a gauge 19 (outer diameter 1.10 mm) with an extra‐thin or ultra-thin wall, providing inner sections of 0.85 mm and 0.89 mm, respectively, to ensure a precise alignment for the optical components. Despite this system’s reduced scale, the current proportions of the micro-camera preclude use in needles with lumens smaller than 19 gauge.
The optical components in SIPS were enclosed within a polyimide tubing, serving as a trocar system. In early prototypes, where the micro-camera and optical fibers were fixed directly inside the needle, small amounts of tissue would occasionally become lodged at the tip during insertion, blocking the view. Cleaning the camera lens under these conditions proved challenging, as the tissue trapped was difficult to remove. By first inserting the needle, the trocar system allows for careful inspection with the micro-camera to verify if the needle tip is clear. An empty sterilized polyimide tubing with gentle suction can remove debris if an obstruction is detected. Alternatively, if debris cannot be safely removed, the needle can be gently withdrawn, cleared, and reinserted before introducing the tubing containing the optical assembly, ensuring an unobstructed view of the subglottic area.
Increased miniaturization of SIPS can be achieved by decreasing the imaging chip size (currently 0.65 × 0.65 × 1.19 mm3). This can be performed in two ways: reducing the number of pixels on the sensor while maintaining the current pixel size of 1 µm or reducing the pixel size. In its present configuration, the sensor has a resolution of 400 × 400 pixels (160,000 pixels total). Whereas reducing the pixel count lowers the overall resolution, it can still provide sufficient detail when imaging a minor area (field of view), provided the spatial resolution remains adequate. Reducing pixel size, however, introduces additional challenges, such as increased shot noise and lower light sensitivity29, greater optical crosstalk30, and reduced quantum efficiency31, all of which degrade image quality. Scaling down the optical sensor would also require precise lens engineering to minimize distortions and aberrations, ensuring that miniaturization does not compromise visual details.
An option for the micro-camera is fiber optic image conduits. These consist of thousands of individual optical fibers arranged in a fixed, coherent alignment, each functioning as a pixel that transmits a portion of the image. While these bundles are widely implemented in flexible endoscopes, adapting them within a needle would provide a considerably reduced resolution than the micro-camera. This limitation results from the size of individual fibers in a bundle, which typically have diameters bigger than 4 µm—significantly larger than the pixels in the OCHTA10 sensor. Because each fiber requires individual cladding to avoid light leakage and a core size larger than the wavelength of light for effective transmission, the minimum core diameter for visible light is about 0.7 µm, which constrains achievable resolution. For example, the image conduit produced by Sumita Optical Glass, Inc. (Tajima, Japan) consists of 8,100 fibers (pixels), each with a diameter of 4.6 µm—almost 20 times lower than the 160,000 pixels provided by SIPS. Other image guides, such as those manufactured by SCHOTT (Mainz, Germany), have fibers with diameters spanning from 4 to 6 µm and fiber counts between 4000 and 18,000 per bundle.
In conclusion, SIPS provides an effective, minimally invasive solution for accessing and visualizing the subglottis. A clinical trial will be conducted to evaluate the endoscopic visualization capabilities of the SIPS. Additional innovations are in progress, including wireless imaging capabilities, a curved needle design to better direct access towards the subglottic aperture, and a steerable trocar system that enables active directional control after insertion. A funnel-shaped profile at the proximal part of the needle is being developed to ease polyimide tubing insertion. Efforts are also focused on miniaturizing the micro-camera while preserving its resolution. Moreover, synchronizing the camera’s frame rate with precise illumination timing can enable stroboscopic imaging of vocal fold vibration from the subglottis.
Data availability
All relevant data is contained within the article. The original contributions presented in the study are included in the article; further inquiries can be directed to the corresponding author.
References
Motz, K. M. et al. Quantification of inflammatory markers in laryngotracheal stenosis. Otolaryngol. Head Neck Surg. 157, 466–472. https://doi.org/10.1177/0194599817706930 (2017).
Gelbard, A. et al. Disease homogeneity and treatment heterogeneity in idiopathic subglottic stenosis. Laryngoscope 126, 1390–1396. https://doi.org/10.1002/lary.25708 (2016).
Gelbard, A. et al. Idiopathic subglottic stenosis is associated with activation of the inflammatory IL-17A/IL-23 axis. Laryngoscope 126, E356–E361. https://doi.org/10.1002/lary.26098 (2016).
Gelbard, A. et al. Molecular analysis of idiopathic subglottic stenosis for Mycobacterium species. Laryngoscope 127, 179–185. https://doi.org/10.1002/lary.26097 (2017).
Morrison, R. J. et al. Pathologic fibroblasts in idiopathic subglottic stenosis amplify local inflammatory signals. Otolaryngol. Head Neck Surg. 160, 107–115. https://doi.org/10.1177/0194599818803584 (2019).
Jefferson, N. D., Cohen, A. P. & Rutter, M. J. Subglottic stenosis. Semin. Pediatr. Surg. 25, 138–143. https://doi.org/10.1053/j.sempedsurg.2016.02.006 (2016).
Pasick, L. J., Anis, M. M. & Rosow, D. E. An updated review of subglottic stenosis: Etiology, evaluation, and management. Curr. Pulmonol. Rep. 11, 29–38. https://doi.org/10.1007/s13665-022-00286-6 (2022).
Zeitels, S. M., de Alarcon, A., Burns, J. A., Lopez-Guerra, G. & Hillman, R. E. Posterior glottic diastasis: Mechanically deceptive and often overlooked. Ann. Otol. Rhinol. Laryngol. 120, 71–80. https://doi.org/10.1177/000348941112000201 (2011).
Hillel, A. T., Ochsner, M. C., Johns, M. M. 3rd. & Klein, A. M. A cost and time analysis of laryngology procedures in the endoscopy suite versus the operating room. Laryngoscope 126, 1385–1389. https://doi.org/10.1002/lary.25653 (2016).
Hong, K. H. & Kim, H. K. Diplophonia in unilateral vocal fold paralysis and intracordal cyst. Otolaryngol. Head Neck Surg. 121, 815–819. https://doi.org/10.1053/hn.1999.v121.a94214 (1999).
O-Lee, T. J. & Messner, A. Subglottic hemangioma. Otolaryngol. Clin. North Am. 41, 903–911. https://doi.org/10.1016/j.otc.2008.04.009 (2008).
Ni, X. G. et al. Endoscopic diagnosis of laryngeal cancer and precancerous lesions by narrow band imaging. J. Laryngol. Otol. 125, 288–296. https://doi.org/10.1017/S0022215110002033 (2011).
Kuo, C. F. J., Li, Y. C., Weng, W. H., Leon, K. B. P. & Chu, Y. H. Applied image processing techniques in video laryngoscope for occult tumor detection. Biomed. Signal Process. Control 55, 101633 (2020).
Seccia, V. et al. Patient-related and ENT-related predictive factors based on the pain experienced during flexible nasendoscopy. Laryngoscope 124, 1648–1652. https://doi.org/10.1002/lary.24535 (2014).
Tulaci, K. G., Arslan, E., Tulaci, T. & Yazici, H. Which one is favorable in the elderly? Transoral rigid laryngoscopy or transnasal flexible fiberoptic laryngoscopy. Am. J. Otolaryngol. 41, 102660. https://doi.org/10.1016/j.amjoto.2020.102660 (2020).
Joy, A. K., Philip, A., Mathews, S. S. & Albert, R. R. A. Transnasal flexible laryngoscopy using different topical preparations and methods of application—A randomized study. J. Voice 36, 847–852. https://doi.org/10.1016/j.jvoice.2020.10.009 (2022).
Conlin, A. E. & McLean, L. Systematic review and meta-analysis assessing the effectiveness of local anesthetic, vasoconstrictive, and lubricating agents in flexible fibre-optic nasolaryngoscopy. J. Otolaryngol. Head Neck Surg. 37, 240–249 (2008).
Nankivell, P. C. & Pothier, D. D. Nasal and instrument preparation prior to rigid and flexible nasendoscopy: A systematic review. J. Laryngol. Otol. 122, 1024–1028. https://doi.org/10.1017/S0022215108002533 (2008).
Sunkaraneni, V. S. & Jones, S. E. Topical anaesthetic or vasoconstrictor preparations for flexible fibre-optic nasal pharyngoscopy and laryngoscopy. Cochrane Database Syst. Rev. 3, CD005606. https://doi.org/10.1002/14651858.CD005606.pub2 (2011).
Biggs, T. C., Henderson, A., Shelton, F. & Patel, N. N. The use of visual distraction to improve the tolerability of flexible laryngoscopy. J. Laryngol. Otol. 132, 739–741. https://doi.org/10.1017/S0022215118001093 (2018).
Almeida, G., Costa, A. C. & Machado, H. S. Supraglottic airway devices: A review in a new era of airway management. J. Anesth. Clin. Res. 7(7), 2 (2016).
Cooper, R. M. Preparation for and management of “failed” laryngoscopy and/or intubation. Anesthesiology 130, 833–849. https://doi.org/10.1097/ALN.0000000000002555 (2019).
Voelkel, R., Weible, K. J. & Eisner, M. Wafer-level micro-optics: trends in manufacturing, testing, and packaging. In Optical Fabrication, Testing, and Metrology IV, SPIE , vol. 8169, 74–85 (2011).
Omnivision. CameraCubeChip® product overview (2023).
Cury, J. et al. Optical method to preserve residual hearing in patients receiving a cochlear implant. Front. Audiol. Otol. 2, 1376699 (2024).
Duan, X. et al. A novel robotic bronchoscope system for navigation and biopsy of pulmonary lesions. Cyborg. Bionic Syst. 4, 0013. https://doi.org/10.34133/cbsystems.0013 (2023).
Tahmasebi, M. et al. The CathCam: A novel angioscopic solution for endovascular interventions. Ann. Biomed. Eng. 51, 2812–2823. https://doi.org/10.1007/s10439-023-03344-5 (2023).
Cury, J., Burns, J., Richter, C.-P. & Delgado Ayala, A. K. Subglottic Imaging Puncture Scope. USA patent (2024).
Chen, T., Catrysse, P. B., El Gamal, A. & Wandell, B. A. How small should pixel size be? In Sensors and Camera Systems for Scientific, Industrial, and Digital Photography Applications (San Jose, CA: SPIE Proceedings) 451–459. https://doi.org/10.1117/12.385463 (2000).
Hirakawa, K. Cross-talk explained. In 2008 15th IEEE International Conference on Image Processing 677–680 (IEEE, 2008).
Bianconi, S. et al. Strategy for addressing the low quantum efficiency of nanowire photodetectors. ACS Photon. 9, 2280–2286. https://doi.org/10.1021/acsphotonics.2c00029 (2022).
Acknowledgements
This research was supported in part by a grant from the American Hearing Research Foundation (AH2024-003G), conducted at the Northwestern University Feinberg School of Medicine in Chicago, Illinois, United States.
Funding
This research was supported in part by a grant from the American Hearing Research Foundation (AH2024-003G), conducted at the Northwestern University Feinberg School of Medicine in Chicago, Illinois, United States.
Author information
Authors and Affiliations
Contributions
JC: Methodology, data acquisition, formal analysis, investigation, writing the original draft, review & editing. AD: Methodology, data acquisition, formal analysis, investigation, writing the original draft, review & editing. JB: Conceptualization, methodology, data acquisition, investigation, review & editing. CPR: Methodology, data acquisition, formal analysis, investigation, project administration, review & editing.
Corresponding author
Ethics declarations
Competing interests
JB, CPR, AD, and JC filed a patent on the design and fabrication of the minimally invasive subglottic imaging system. CPR and JC filed additional patents on the application of the miniaturized optical system. JB, CPR, AD, and JC are co-founders of Airway Optix, LLC. CPR and JC are also co-founders of Cochlear Vision, LLC and Vision100, LLC. The remaining authors declare that the research was conducted without commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cury, J., Delgado Ayala, A.K., Burns, J. et al. Subglottic imaging puncture scope (SIPS) for minimally invasive endoscopy. Sci Rep 15, 22350 (2025). https://doi.org/10.1038/s41598-025-06792-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-06792-2
