
Abstract
Branched-chain amino acids (BCAAs) are known to be associated with cardiovascular disease risk in adults. The aim of this study is to investigate whether an increased cardiometabolic risk profile can be observed in the amino acid profile of young adult offspring of women with type 1 diabetes. This cross-sectional case-control study included 73 offspring born to women with type 1 diabetes (cases) and 82 control participants (controls). At the age of 18–23 years, they participated in a clinical assessment including laboratory tests and questionnaires. Amino acid levels were analyzed from venous serum samples after 10 h of fasting using nuclear magnetic resonance (NMR) spectroscopy. No differences in cardiovascular disease or cardiometabolic risk factors were observed between the cases and the controls. Circulating amino acid levels were similar in both groups. The glucogenic score (combined alanine, glycine) was higher in overweight case men (case versus controls adjusted p = 0.015 (mean ratio 1.25 [95% CI 1.11 to 1.49]). The present findings do not support our hypothesis that serum amino acid profiles, determined in early adulthood, are associated with a more adverse cardiometabolic risk profile in offspring of women with type 1 diabetes. Further studies are warranted to clarify the potential role of amino acids in the development of cardiovascular disease in offspring of women with type 1 diabetes.
Similar content being viewed by others

Introduction
Cardiovascular diseases (CVD) are multifactorial, and healthy lifestyle choices can largely reduce the risk of developing CVD1,2. Well-known CVD risk factors include elevated blood pressure, hyperglycemia, dyslipidemia, as well as overweight and obesity3. However, more information on risk factors that characterize specific patient subgroups is needed to improve individualized primary and secondary prevention of CVDs4,5. Amino acids (AAs) play a key role in metabolic pathways6. They are involved in energy production and regulation, acting as signaling molecules influencing insulin sensitivity, lipid metabolism, and inflammation7,8,9,10. All these processes are linked to cardiometabolic risk factors such as obesity, hypertension and type 2 diabetes (T2D)11,12. The nuclear factor-κB (NF-κB) signaling pathway regulates immune responses and inflammatory processes13. Dysregulation of this pathway has been documented in chronic diseases, including type 1 diabetes (T1D)13,14. In a mouse model, diabetes during pregnancy has been shown to cause dysregulation of NF-κB in the mouse embryos15.
Nuclear magnetic resonance (NMR) is a spectroscopic technique used in metabolomics to identify metabolites, such as circulating lipids and AAs, on a larger scale16. Alterations in metabolic pathways can be detected and can be used to predict disease risk and potentially to guide therapy17,18,19. Elevated circulating levels of branched-chain amino acids (BCAAs) have been reported to be associated with obesity-related conditions such as insulin resistance, T2D, and CVD20,21,22,23. Five BCAAs and aromatic amino acids (AAAs), namely isoleucine, leucine, valine, tyrosine, and phenylalanine have shown highly significant associations with future development of T2D19. BCAAs are associated with obesity during childhood and adolescence and predict insulin resistance in this age group24. A Finnish study showed that circulating leucine and isoleucine levels are related to triglyceride levels in young women25. BCAAs regulate protein synthesis, cell growth, and autophagy, as well as insulin secretion through mammalian target of rapamycin (mTOR) activation26,27,28. Overstimulation of mTOR causes insulin resistance29. High concentrations of BCAAs have also been associated with increased production of reactive oxygen species and mitochondrial dysfunction, contributing to oxidative stress and inflammation9.
To the best of our knowledge, no previous studies have examined circulating AA concentrations in young adult offspring of women with T1D. Offspring of women with T1D have an increased risk of diabetes and early-onset CVD30. This can be explained by fetal programming: High blood glucose levels during pregnancy can alter fetal development, leading to long-term metabolic and vascular dysfunction31,32. Exposure to hyperglycemia can impair blood vessel function, increasing the risk of hypertension and atherosclerosis33,34. Maternal diabetes can influence gene expression through epigenetic changes, predisposing the child to metabolic and cardiovascular diseases later in life35,36,37. Offspring born to women with T1D are more likely to develop impaired glucose tolerance, insulin resistance, and eventually T2D, all of which increase the risk of CVD38,39. Studies suggest that offspring of women with T1D show early signs of arterial stiffness and endothelial dysfunction, which increase long-term CVD risk40,41. In addition, T1D during pregnancy is associated with altered lipid metabolism in offspring, predisposing them to CVD42,43.
Considering what is already known about BCAAs and the pathogenesis of CVD/T2D, we hypothesized that the AA profile of offspring of women with T1D would differ from that of offspring of women without diabetes.
The aim of this study was to investigate whether there are differences in the AA profile in early adulthood between offspring of women with T1D and offspring of women without diabetes, and whether this is associated with a more adverse cardiometabolic risk profile.
Methods
Design and participants
This study is a cross-sectional case-control study conducted in the Hospital District of Helsinki and Uusimaa, Finland. The study population included individuals born between January 1, 1996, and December 31, 2000, in the Helsinki metropolitan area.
The case group (n = 238) consisted of singleton offspring of women with T1D who were delivered by elective cesarean section at the Department of Obstetrics and Gynecology, Helsinki University Hospital, Finland. During the study period, all deliveries of women with T1D in the Hospital District of Helsinki and Uusimaa were centralized at this hospital.
The control group (n = 276) comprised of the first or second singleton child born after each case to women without diabetes within the same hospital district.
At 18–23 years of age, all participants were invited to take part in a clinical study and received an invitation letter. A total of 81 cases (36%) and 86 controls (20%) agreed to participate. Blood samples were available and analyzed in 75 cases and 82 controls. Two cases were excluded due to overt diabetes, resulting in a final sample size of 73 cases and 82 controls.
Clinical study
The methods applied have been described previously44. All participants were examined by trained study nurses. Weight and body composition were measured in light indoor clothing without shoes or socks on using a bioimpedance body composition device (InBody 3.0, Biospace, Seoul, South Korea). Body weight and fat mass were recorded with an accuracy of 0.1 kg, and fat percentage was calculated. Height was measured without shoes or socks on against a wall-mounted stadiometer (SECA Telescopic measuring rod, SHZ, cm INT) with an accuracy of 0.1 cm. Body mass index (BMI) was calculated as kg/m2. Normal weight was defined as BMI < 25.0 kg/m2, and overweight was defined as BMI ≥25.0 kg/m2. Blood pressure was measured three times from the right arm in a sitting position after at least 15 min of rest using a cuff size 22 × 42 cm (Omron Intellisense M6 AC, Omron Healthcare Co. Ltd., Japan) and the mean value of the measurements was documented. Between the measurements there was at least a one-minute pause.
Laboratory analyses, physical activity, and questionnaires
Venous blood samples were taken in a sitting position with a light stasis after 10 h of fasting. A 2-hour 75 g oral glucose tolerance test was performed according to the WHO 1999 guidelines. Fasting insulin, glycated hemoglobin A1c, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglycerides, and high-sensitivity C-reactive protein were measured. Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) was calculated.
Physical activity was determined using the Kuopio Ischaemic Heart Disease (KIHD) questionnaire and reported as Metabolic Equivalent of Task-hours per week (MET-h/week)45. The standardized questionnaire estimates physical activity during the previous 12-month period by type of physical activity, duration, and frequency. Each type of activity is assigned a MET-value. 1 MET = 3.5ml O2/kg/min, which roughly corresponds to the energy expenditure of metabolic state at rest. MET-h/week describes the sum of the product of each activity’s MET value, duration and frequency.
Smoking habits and chronic diseases were self-reported using validated questionnaires. Participants who reported hypertension, heart failure, arrhythmia, coronary heart disease or myocardial infarction, other heart disease, stroke, or cerebral hemorrhage were considered to have CVD.
Metabolomics
Nightingale NMR was applied for the quantification of metabolite measures from serum samples. In this study, we focused on AAs, namely alanine, glycine, histidine, phenylalanine, tyrosine, leucine, isoleucine, and valine. We grouped the AAs, as done previously and according to Mikkola et al.46. Sum scores were created for glucogenic (GAA) (alanine and glycine), aromatic (AAA) (histidine, phenylalanine, and tyrosine), and BCAA (leucine, isoleucine, and valine).
Statistics
Summary statistics are described using mean and standard deviation (SD), or numbers as percentages. Statistical evaluation between groups (case and controls) were analyzed by using Student’s t-test, Permutation test, Pearson’s chi-squared test, and Fisher’s exact test. Relationships between BMI groups (< 25.0 and ≥ 25.0) and case and controls were analyzed using permutation type two-way analysis of variance (ANOVA). In cases of violation of the assumptions (e.g., non-normality), a bootstraptype method was used for the continuous variables, and Monte Carlo p-values (small number of observations) were used for the categorical variables. The Stata 18.0 (StataCorp LP; College Station, Texas, USA) statistical package was used for the analysis.
Results
No differences in characteristics were observed between cases and controls (Table 1). The mean age in both groups was 21 years. 59 (81%) of the cases and 61 (74%) of the controls were non-smokers. Physical activity was similar in both groups (30.9 MET-h/week [SD 28.5] versus 37.2 MET-h/week [SD 45.0]). Mean BMI was at the top of the normal reference range in both groups (24,7 kg/m2 [SD 5.0] among cases and 24,2 kg/m2 [SD 5.3] among controls). Body fat percentage was similar in both groups (33.0% [SD 7.8] versus 30.4% [SD 9.5] in women and 19.1% [SD 10.6] versus 17.4% [SD 7.1] in men). Mean blood pressure was within the normotensive range in both groups (118/74 mmHg among cases and 119/74 mmHg among controls). No differences between the two groups were observed in laboratory tests evaluating glucose metabolism. Mean lipid values were in the reference range for both groups, and no major differences were observed. 7% of cases and 5% of controls reported CVD.
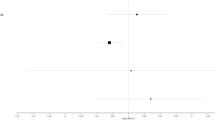
AA concentrations in cases and controls are reported separately for women and men in Table 2. No statistically significant differences were found between the two groups. Adjusted (physical activity, fasting glucose and smoking) amino acid concentrations across BMI for cases and controls are shown in Fig. 1. The glucogenic score was higher in overweight case men vs. overweight controls (p = 0.015 (mean ratio 1.25 [95% CI 1.11 to 1.49]).

Adjusted (physical activity, fasting glucose and smoking) amino acid concentrations for men and women across body mass index (BMI) for offspring of women without diabetes (controls) and offspring of women with type 1 diabetes (cases). BMI \(\:\ge\:\) 25.0 indicates overweight. Sum scores were created for glucogenic (alanine and glycine), aromatic (histidine, phenylalanine, and tyrosine), and branched chain (leucine, isoleucine, and valine) amino acids.
Discussion
Our findings suggest that young adult offspring of women with T1D do not possess a distinctive cardiometabolic risk factor profile or widely deviant levels of circulating AAs potentially associated with CVD, compared to offspring of women without diabetes. The GAA score (a combination of alanine and glycine) was higher in overweight men born to women with T1D compared to men born to women without diabetes during pregnancy. The same phenomenon was not observed among overweight women. Among the eight AAs measured, no significant differences were observed between cases and controls. AA scores were BMI-dependent, with overweight status being associated with higher AA scores.
The use of GAA score is not well-established in research. In our case, this sum score was formed by the two AAs that did not belong to the BCAA or AAA category, which have been linked to CVD development22. The higher GAA score among overweight men born to women with T1D is surprising, since glycine has been inversely associated with BMI and CVD risk-factors, usually indicating favorable metabolic health47,48,49. Alanine has been linked to CVD risk factors including high blood pressure and insulin resistance, and therefore the results are expected50,51. In a Finnish study, in an age group significantly older than our study population, alanine was associated with coronary artery disease52.
The reason why the glucogenic score does not follow a similar pattern in men and women remains unknown. Hormonal factors may influence the results. Mikkola et al. investigated the association between body composition in older men and women and the same eight AAs and sum scores we considered in our study46. In their study, glucogenic score was associated with fat mass only in women. Alanine showed a positively association with fat mass in both women and men, while glycine was inversely associated with lean mass in men46. It remains speculative whether more subgroups with distinctive AA profiles could have been identified if there had been a bigger weight difference between cases and controls. Metabolic flexibility and AA levels are impacted by obesity53,54.
Since CVD typically manifests later in life, it can be assumed that the young age of the participants may have influenced the result2. AA levels are often age-dependent55. However, BCAAs have been associated with obesity and insulin resistance even in children24,56. In addition, some AAs have been shown to predict insulin resistance and T2D years in advance19. A recent study in adolescents with prediabetes or T2D identified a distinct AA profile, characterized by elevated levels of BCAAs and AAAs along with reduced glycine concentration57. Similar findings might have been expected in our study, given that offspring of women with T1D have an increased risk of T2D39. Our results are likely influenced by the overall good health of the participants. This may, in turn, be affected by selection bias, as those in better health may have been more likely to participate in the study.
Metabolomic measures are relatively dynamic and affected by intrinsic and extrinsic exposures18. This makes it difficult to define the clinical relevance of our study findings. In addition to the fact that most of the examined AAs are dietary essential, it is also known that the gut microbiome affects the bioavailability of AAs58. It would have been interesting to consider the participants’ diet, but, unfortunately, nutritional data was not collected in the present study. A follow-up study including dietary analysis could provide additional information on the effect of T1D during pregnancy on circulating AA levels in offspring. Diet should be considered holistically when examining cardiometabolic diseases. In addition to AAs, special attention should be paid to carbohydrates and fats59,60.
Moreover, our limited sample size might have led to some degree of selection bias, and the fact that the cohort included only participants from the Hospital District of Helsinki and Uusimaa, Finland, may reduce the generalizability of our findings. It would have been valuable to consider the characteristics of the mothers of the study participants, such as the age at onset of type 1 diabetes or the duration of the disease. However, these data were not available to us. In addition, it should be noted that the participants are relatively young in the context of CVD risk.
Despite its limitations, the present study is important considering our limited knowledge on the long-term metabolic impacts of in-utero exposure to maternal T1D. One key strength of our research is the thorough clinical examination of the participants, which reduces the likelihood of errors due to reporting bias. Although the NMR technique offers possibilities for more extensive metabolomic analyses, we decided to focus on the manageable entity of eight circulating AAs. In the future, using a more comprehensive GAA score could help detect more finite differences between the AA profiles of offspring born to women with T1D vs. offspring of women without diabetes.
Conclusions
The present results do not support our hypothesis that serum AA profile, determined in early adulthood, is associated with a more adverse CVD risk profile in offspring of women with T1D. However, the GAA score was higher in overweight men born to women with diabetes during pregnancy, compared to men born to women without diabetes during pregnancy. Further studies should be performed to find out whether these AAs could serve as early biomarkers of CVD development or whether changes in the AA levels over years could be used to monitor CVD progression in offspring of women with T1D.
Data availability
Due to legal restrictions, the data cannot be shared publicly; however, requests for access can be directed to the corresponding author.
Abbreviations
- AA:
-
Amino acid
- AAA:
-
Aromatic amino acid
- BCAA:
-
Branched chain amino acid
- CVD:
-
Cardiovascular disease
- GAA:
-
Glucogenic amino acid
- mTOR:
-
Mammalian target of rapamycin
- NF-κB:
-
Nuclear factor-κB
- NMR:
-
Nuclear magnetic resonance
- T1D:
-
Type 1 diabetes
- T2D:
-
Type 2 diabetes
References
Barbaresko, J., Rienks, J. & Nöthlings, U. Lifestyle indices and cardiovascular disease risk: A Meta-analysis. Am. J. Prev. Med. 55 (4), 555–564 (2018).
Kaminsky, L. A. et al. The importance of healthy lifestyle behaviors in the prevention of cardiovascular disease. Prog Cardiovasc. Dis. 70, 8–15 (2022).
WHO, Cardiovascular diseases & WHO. ; [ (2023). Available from: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1
Karunathilake, S. P. & Ganegoda, G. U. Secondary prevention of cardiovascular diseases and application of technology for early diagnosis. Biomed. Res. Int. 2018, 5767864 (2018).
Hoogeveen, R. M. et al. Improved cardiovascular risk prediction using targeted plasma proteomics in primary prevention. Eur. Heart J. 41 (41), 3998–4007 (2020).
Ling, Z. N. et al. Amino acid metabolism in health and disease. Signal. Transduct. Target. Ther. 8 (1), 345 (2023).
Newsholme, P., Bender, K., Kiely, A. & Brennan, L. Amino acid metabolism, insulin secretion and diabetes. Biochem. Soc. Trans. 35 (Pt 5), 1180–1186 (2007).
Xiao, F. & Guo, F. Impacts of essential amino acids on energy balance. Mol. Metab. 57, 101393 (2022).
Zhenyukh, O. et al. High concentration of branched-chain amino acids promotes oxidative stress, inflammation and migration of human peripheral blood mononuclear cells via mTORC1 activation. Free Radic Biol. Med. 104, 165–177 (2017).
Tang, L. et al. Integrated transcriptome and metabolome analysis to investigate the mechanism of intranasal insulin treatment in a rat model of vascular dementia. Front. Pharmacol. 14, 1182803 (2023).
Drozdz, D. et al. Obesity and cardiometabolic risk factors: from childhood to adulthood. Nutrients ;13(11). (2021).
Chakraborty, S., Verma, A., Garg, R., Singh, J. & Verma, H. Cardiometabolic risk factors associated with type 2 diabetes mellitus: A mechanistic insight. Clin. Med. Insights Endocrinol. Diabetes. 16, 11795514231220780 (2023).
Liu, T., Zhang, L., Joo, D. & Sun, S. C. NF-κB signaling in inflammation. Signal. Transduct. Target. Ther. 2, 17023 (2017).
Bierhaus, A. et al. Diabetes-associated sustained activation of the transcription factor nuclear factor-kappaB. Diabetes 50 (12), 2792–2808 (2001).
Liu, X. et al. NF-κB activation impedes the transdifferentiation of hypertrophic chondrocytes at the growth plate of mouse embryos in diabetic pregnancy. J. Orthop. Translat. 31, 52–61 (2021).
Soininen, P. et al. High-throughput serum NMR metabonomics for cost-effective holistic studies on systemic metabolism. Analyst 134 (9), 1781–1785 (2009).
McGarrah, R. W., Crown, S. B., Zhang, G. F., Shah, S. H. & Newgard, C. B. Cardiovascular metabolomics. Circ. Res. 122 (9), 1238–1258 (2018).
Cheng, S. et al. Potential impact and study considerations of metabolomics in cardiovascular health and disease: A scientific statement from the American heart association. Circ. Cardiovasc. Genet. ;10(2). (2017).
Wang, T. J. et al. Metabolite profiles and the risk of developing diabetes. Nat. Med. 17 (4), 448–453 (2011).
Newgard, C. B. et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell. Metab. 9 (4), 311–326 (2009).
Lynch, C. J. & Adams, S. H. Branched-chain amino acids in metabolic signalling and insulin resistance. Nat. Rev. Endocrinol. 10 (12), 723–736 (2014).
Magnusson, M. et al. A diabetes-predictive amino acid score and future cardiovascular disease. Eur. Heart J. 34 (26), 1982–1989 (2013).
McGarrah, R. W. & White, P. J. Branched-chain amino acids in cardiovascular disease. Nat. Rev. Cardiol. 20 (2), 77–89 (2023).
McCormack, S. E. et al. Circulating branched-chain amino acid concentrations are associated with obesity and future insulin resistance in children and adolescents. Pediatr. Obes. 8 (1), 52–61 (2013).
Wiklund, P. et al. Serum amino acid profiles in childhood predict triglyceride level in adulthood: A 7-Year longitudinal study in girls. J. Clin. Endocrinol. Metab. 101 (5), 2047–2055 (2016).
Zhang, Z. Y., Monleon, D., Verhamme, P. & Staessen, J. A. Branched-Chain amino acids as critical switches in health and disease. Hypertension 72 (5), 1012–1022 (2018).
Neinast, M., Murashige, D. & Arany, Z. Branched chain amino acids. Annu. Rev. Physiol. 81, 139–164 (2019).
Flores-Guerrero, J. L. et al. Concentration of Branched-Chain amino acids is a strong risk marker for incident hypertension. Hypertension 74 (6), 1428–1435 (2019).
Yoon, M. S. The emerging role of Branched-Chain amino acids in insulin resistance and metabolism. Nutrients ;8(7). (2016).
Yu, Y. et al. Maternal diabetes during pregnancy and early onset of cardiovascular disease in offspring: population based cohort study with 40 years of follow-up. BMJ :l6398. (2019).
Monteiro, L. J., Norman, J. E., Rice, G. E. & Illanes, S. E. Fetal programming and gestational diabetes mellitus. Placenta 48 (Suppl 1), S54–s60 (2016).
Bianco, M. E. & Josefson, J. L. Hyperglycemia during pregnancy and Long-Term offspring outcomes. Curr. Diab Rep. 19 (12), 143 (2019).
Pathirana, M. M., Lassi, Z. S., Roberts, C. T. & Andraweera, P. H. Cardiovascular risk factors in offspring exposed to gestational diabetes mellitus in utero: systematic review and meta-analysis. J. Dev. Orig Health Dis. 11 (6), 599–616 (2020).
Funk, S. D., Yurdagul, A. Jr. & Orr, A. W. Hyperglycemia and endothelial dysfunction in atherosclerosis: lessons from type 1 diabetes. Int. J. Vasc Med. 2012, 569654 (2012).
Lehnen, H., Zechner, U. & Haaf, T. Epigenetics of gestational diabetes mellitus and offspring health: the time for action is in early stages of life. Mol. Hum. Reprod. 19 (7), 415–422 (2013).
Sun, C. et al. Effects of early-life environment and epigenetics on cardiovascular disease risk in children: highlighting the role of twin studies. Pediatr. Res. 73 (4 Pt 2), 523–530 (2013).
Knorr, S. et al. Epigenetic and transcriptomic alterations in offspring born to women with type 1 diabetes (the EPICOM study). BMC Med. 20 (1), 338 (2022).
Weiss, P. A. et al. Long-term follow-up of infants of mothers with type 1 diabetes: evidence for hereditary and nonhereditary transmission of diabetes and precursors. Diabetes Care. 23 (7), 905–911 (2000).
Clausen, T. D. et al. High prevalence of type 2 diabetes and pre-diabetes in adult offspring of women with gestational diabetes mellitus or type 1 diabetes: the role of intrauterine hyperglycemia. Diabetes Care. 31 (2), 340–346 (2008).
Nelson, S. M., Sattar, N., Freeman, D. J., Walker, J. D. & Lindsay, R. S. Inflammation and endothelial activation is evident at birth in offspring of mothers with type 1 diabetes. Diabetes 56 (11), 2697–2704 (2007).
Korpijaakko, C. A. et al. Higher pulse wave velocity in young adult offspring of mothers with type 1 diabetes: a case-control study. Cardiovasc. Diabetol. 21 (1), 178 (2022).
Yessoufou, A. & Moutairou, K. Maternal diabetes in pregnancy: early and long-term outcomes on the offspring and the concept of metabolic memory. Exp. Diabetes Res. 2011, 218598 (2011).
Clausen, T. D. et al. Overweight and the metabolic syndrome in adult offspring of women with diet-treated gestational diabetes mellitus or type 1 diabetes. J. Clin. Endocrinol. Metab. 94 (7), 2464–2470 (2009).
Somersalo, E. et al. Circulating cytokine levels and cardiovascular disease risk profile in young adult offspring of women with type 1 diabetes. Diabetes Ther. 14 (8), 1427–1436 (2023).
Lakka, T. A. & Salonen, J. T. Intra-person variability of various physical activity assessments in the Kuopio ischaemic heart disease risk factor study. Int. J. Epidemiol. 21 (3), 467–472 (1992).
Mikkola, T. M., Salonen, M. K., Kajantie, E., Kautiainen, H. & Eriksson, J. G. Associations of fat and lean body mass with Circulating amino acids in older men and women. J. Gerontol. Biol. Sci. Med. Sci. 75 (5), 885–891 (2020).
Kraus, W. E. et al. Association of plasma Small-Molecule intermediate metabolites with age and body mass index across six diverse study populations. J. Gerontol. Biol. Sci. Med. Sci. 71 (11), 1507–1513 (2016).
Wittemans, L. B. L. et al. Assessing the causal association of glycine with risk of cardio-metabolic diseases. Nat. Commun. 10 (1), 1060 (2019).
Ding, Y. et al. Plasma Glycine and risk of acute myocardial infarction in patients with suspected stable angina pectoris. J. Am. Heart Assoc. ;5(1). (2015).
Deng, Y., Huang, C., Su, J., Pan, C. W. & Ke, C. Identification of biomarkers for essential hypertension based on metabolomics. Nutr. Metab. Cardiovasc. Dis. 31 (2), 382–395 (2021).
Vangipurapu, J., Stancáková, A., Smith, U., Kuusisto, J. & Laakso, M. Nine amino acids are associated with decreased insulin secretion and elevated glucose levels in a 7.4-Year Follow-up study of 5,181 Finnish men. Diabetes 68 (6), 1353–1358 (2019).
Jauhiainen, R. et al. The association of 9 amino acids with cardiovascular events in Finnish men in a 12-Year Follow-up study. J. Clin. Endocrinol. Metab. 106 (12), 3448–3454 (2021).
Galgani, J. E. & Fernández-Verdejo, R. Pathophysiological role of metabolic flexibility on metabolic health. Obes. Rev. 22 (2), e13131 (2021).
Morris, C. et al. The relationship between BMI and metabolomic profiles: a focus on amino acids. Proc. Nutr. Soc. 71 (4), 634–638 (2012).
Hirschel, J. et al. Relation of whole blood amino acid and acylcarnitine metabolome to age, sex, BMI, puberty, and metabolic markers in children and adolescents. Metabolites ;10(4). (2020).
Butte, N. F. et al. Global metabolomic profiling targeting childhood obesity in the Hispanic population. Am. J. Clin. Nutr. 102 (2), 256–267 (2015).
Bacha, F. et al. Distinct amino acid profile characterizes youth with or at risk for type 2 diabetes. Diabetes 73 (4), 628–636 (2024).
Pedersen, H. K. et al. Human gut microbes impact host serum metabolome and insulin sensitivity. Nature 535 (7612), 376–381 (2016).
Chu, H. et al. MC-LR aggravates liver lipid metabolism disorders in obese mice fed a High-Fat diet via PI3K/AKT/mTOR/SREBP1 signaling pathway. Toxins (Basel) ;14(12). (2022).
Wang, X. F. et al. The therapeutic potential of plant polysaccharides in metabolic diseases. Pharmaceuticals (Basel) ;15(11). (2022).
Funding
Open access funded by Helsinki University Library. The Hospital District of Helsinki and Uusimaa, Finland, Finska Läkaresällskapet, and Liv och hälsa awarded a research grant for this study. The funding sources had no role in planning or designing the study, nor in data collection, analyses or writing the article.
Author information
Authors and Affiliations
Contributions
ES, HK, JGE and MKL designed the study. ES, HK, and MKL performed data- analysis. All authors (ES, HK, MMK, JGE and MKL) contributed to the writing of the final manuscript and revising it for critically important intellectual content. All authors agreed with the results and conclusions of the study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Hospital District of Helsinki and Uusimaa (HUS/898/2017) and the study was implemented in accordance with the Declaration of Helsinki. All study participants provided written informed consent before any study procedures took place.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Somersalo, E., Kautiainen, H., Klemetti, M.M. et al. Circulating amino acids and cardiometabolic risk profile in offspring of women with type 1 diabetes: cross-sectional case-control study. Sci Rep 15, 21847 (2025). https://doi.org/10.1038/s41598-025-07177-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-07177-1
