
Abstract
Patient-specific implant (PSI) has optimized the management for a wide range of complex craniofacial deformity over the past years by increasing the accuracy of surgical procedures and lowering the operating time. In hypertelorism (HTO) surgery particularly, the orbital bone repositioning is nowadays guided by patient-specific bone fixation plates that are usually made from non-resorbable alloplastic material (e.g., titanium). Developing resorbable personalized plates could be a relevant alternative to overcome the well-known drawbacks of titanium plates such as infection, exposure or even the lack of bone growth which is detrimental in pediatric patients. This study investigated the mechanical and structural characteristics of poly(lactic-co-glycolic acid) (PLGA) PSI as resorbable materials for HTO surgery. We assessed the feasibility of printing PLGA PSI by Fused Deposition Modeling additive manufacturing (FDM). The geometrical and the mechanical properties of the 3D-printed device were compared with standard resorbable plates and analyzed after sterilization process (i.e., hydrogen peroxide gas plasma). The Young’s modulus was greater than the standard resorbable plates while a decrease of 36% (p = 0.004) after the sterilization was observed. The sterilization also induced a plate deformation with an increase of 0.27 mm in Z-axis and a decrease of 0.8 mm in Y-axis due to annealing effect. Compared to the design, the PLGA PSI were successfully 3D-printed with a maximum deviation of 0.1 mm, making our custom-made plate promising for personalized craniofacial applications. Further investigations on the sterilization process must be considered in view of its mechanical and structural impact on resorbable PSI.
Similar content being viewed by others
Introduction
Patient specific implants (PSI) are routinely used in clinics, especially for complex craniofacial deformity. The role of such a device is to ensure the complex bone repositioning and a proper bone healing as well. In this field, titanium is the commonly used material due to its excellent biocompatibility and mechanical properties1. Nowadays, 3D-preoperative planning and additive manufacturing allow to get personalized titanium plates, which have clearly improved the accuracy of craniofacial surgery such as the orbital repositioning in hypertelorism2,3,4.
However, being a non-resorbable alloplastic material, some limits remain in using titanium PSI in pediatric cases particularly. Firstly, contrary to polymer materials, titanium creates artifacts in imaging techniques such as MRI and CT scans, often making the follow-up really challenging for craniofacial and brain areas. Moreover, it can impede the facial bone growth and it has inherent risk of infection or exposure5requiring sometimes additional surgical revisions to remove or replace the materials which directly impact the recovery time, the rate of complications and the healthcare cost6. In addition, the manufacture of titanium PSI remains an expensive process (e.g., direct metal laser sintering /DMLS or Selective Laser Melting/SLM technologies).
To overcome the drawbacks of titanium, resorbable plates have been developed and can be used in standardized craniofacial surgery7. Basically, they are predominantly made of two thermoplastics polymers: poly(lactic-co-glycolic acid) (PLGA) and poly(D, L-lactic acid) (PDLLA) which display optimal biocompatibility. PLGA has been also widely reported in various medical research fields including drug delivery8,9 or in tissue engineering10 for promoting cell growth in bone scaffolds by using additive manufacturing through Fused Deposition Modeling technology (FDM)11. Indeed, its surface roughness as well as its macro-microarchitecture have been reported as essential in bone ingrowth particularly12,13. However, this type of polymers is only reported for standardized surgical procedure (i.e., non-patient specific) in clinics using flat eyelet assemblies of various shapes and lengths. The plates can be manually shaped and cut preoperatively to fit the patient’s anatomy after immersing in hot water slightly exceeding the glass transition temperature (Tg) (i.e., 55 to 60 °C)14,15. Thus, the manufacture of resorbable PSI could potentially improve the outcomes of craniofacial surgeries. However, contrary to titanium, sterilization of polymers presents major structural and physicochemical challenges especially when heat sterilization is used (e.g., deformation, altered mechanical properties)16. Consequently, there is no patient-specific fixation plate made from resorbable materials that is used in clinical practice17 so far. Other methods like gamma or beta irradiation, though effective, are less accessible and may require outsourcing, leading to delays and logistical challenges in the production of patient-specific osteosynthesis devices. Furthermore, gamma or beta irradiation may induce chain scission in PLGA18leading to a decrease in both resorption time and mechanical properties. Chemical sterilization is another relevant option ensuring pathogen elimination while maintaining materials biocompatibility and structural integrity that could lower the risk of polymers alteration. As an example, Hydrogen Peroxide Gas Plasma Sterilization (HPGP) offers low-temperature sterilization process (i.e., 50 °C) allowing for effective bacterial elimination on PLGA scaffold19,20 with a no risk of toxicity. However, its impact on PLGA integrity needs more investigations.
The aim of this work was to design and assess the accuracy for printing resorbable PLGA PSI using FDM technology for HTO surgery application. Thermal and mechanical properties of the 3D printed PLGA were analyzed before and after HPGP sterilization. PLGA PSI mechanical characteristics were also compared with commercially available resorbable plates used in standardized craniofacial surgery.
Materials and methods
Materials
PLGA filament consisted of 85% Poly(L-lactic acid) and 15% Poly(glycolic acid). It was supplied as a 2.85 mm in diameter filament spool under the name Glycolactisse by Lattice Medical (Loos, France). Filaments were produced from PURASORAB PLG 8523 pellets, sourced from PURAC (CORBION, Gorinchem, The Netherlands). The spools were stored in vacuum-sealed, airtight bags with desiccant at 4 °C. Prior to printing, the filaments were dried for 12 h at 40 °C.
Resorb X® plates (RX) made of PDLLA with a thickness of 1 mm served as gold standard in our study (reference 52-876-22-04, KLS Martin, Germany).
Additive manufacturing
The FDM printer was an Ultimaker S3 (Ultimaker, Utrecht, The Netherlands) using Ultimaker Cura (5.6.0, Ultimaker, Utrecht, The Netherlands) as slicer. The printing parameters followed the manufacturer’s recommendations: nozzle temperature at 220 °C, build plate temperature at 50 °C, fan speed at 100%, print speed at 20 mm.s− 1, brim width of 5 mm, layer height of 0.15 mm, and line width of 0.4 mm. All parts were printed with the printer chamber open, at room temperature. All parts were printed with two walls and 100% infill. If the overhang exceeded 50°, tree supports were automatically added.
To perform standardized tensile tests, specimens conforming to ISO 527-2 Type 5B were printed. The printed specimens were flat, with a square gauge section of 4 mm² and a gauge length of 10 mm, conforming to the EP ISO 527-2 type 5B dimensions. Three printing orientations were evaluated: the “Flat” orientation corresponding to the largest surface in contact with the print bed; the “Vertical” one being the smallest surface of the specimen, with the length aligned along the Z-axis during printing; and the “Trench” one, being the third flat surface, requiring supports for the working part of the specimen.
Resorbable patient-specific plate characteristics
The segmented 3D scan images of an anonymized 8-year-old patient displaying craniofrontonasal dysplasia and hypertelorism served as the base file for the design and printing of the custom-made plate in our study. All experimental protocols were reviewed and approved by the local Ethics Committee of the CHRU de Tours (approval no. 2025-044). All methods were carried out in accordance with the relevant guidelines and regulations. A written informed consent was obtained from the legal representative of the participant. A box osteotomy technique was selected as surgical correction21. The simulated planning of the orbital repositioning as well as the patient specific plate design were carried out using Blender software (4.1.0, Blender Institute, The Netherlands) (Fig. 1a and b).

Stages of Custom Plate Design. (a) 3D bone reconstruction of a patient with hypertelorism. (b) 3D simulation of box osteotomy surgery. (c) The red objects represent the modeled plates, with the upper one for the fronto-temporal area and the lower one for the zygomatic bone. (d) Illustration showing the zygomatic plate on the left, and the fronto-temporal plate on the right. The blue supports are used exclusively in the pin holes, providing support for the overhang and stabilizing the piece to limit wobbling.
The customized plate had the following characteristics (Fig. 1c and d):
-
Conically shaped holes to accommodate RX pins, with a 5 mm center-to-center spacing and a minimum distance of 2.5 mm from the center to the edge of the plate, matching with RX plates.
-
Maximal congruence between the plate and the bone.
-
The surface in contact with the bone was as perpendicular as possible to the print bed to enhance print quality, ensure accurate curve management, and minimize the need for support structures on the bone-contacting surface.
-
A flat surface contact with the print bed to improve adhesion, decrease the risk of detachment during printing, and consequently lower the likelihood of print failure.
-
Constant thickness of 1.2 mm to allow printing with three parallel extrusion lines.
-
Conical cylinders were placed, considering the surgical approach and ensuring at least 2.5 mm of bone around each cylinder. Their orientation was designed to facilitate proper drilling (i.e., perpendicular to the bone). To ensure correct spacing, 5 mm diameter concentric cylinders were used to check the minimum space between each hole.
-
Two surfaces, roughly corresponding to the future plate, were extracted.
-
The nearest vertices of these surfaces were connected to avoid overlap with the bone.
-
The surface was transformed into a volume using the offset modifier to ensure a uniform thickness of 1.2 mm, as simple extrusion did not guarantee consistent thickness.
-
Conical holes were then created, and the rough plate was trimmed with planes to get a flat surface for printing and to remove unexpected material.
-
We assumed that the main mechanical stresses would align with the direction of bone displacement, which also corresponds to our chosen printing orientation, as no specific studies exist regarding the forces applied in this surgical context.
Sterilization
The HPGP sterilization process was based on the Sterrad 100NX system (Advanced Sterilization Products, Johnson & Johnson, USA) in a standard cycle. Each half-cycle consisted in phases involving pressure variations, ranging from atmospheric pressure down to 40 Pa. These pressure changes eased the removal of air and water from the sterilization chamber and the introduction of hydrogen peroxide vapor as well. The plasma phase lasted 4 min at approximately 130 Pa, generated by a low-frequency plasma system operating at 50 kHz and 500 W. The temperature during this phase varied from 47 °C to 56 °C, with an average of 50 °C. The complete standard cycle was two half-cycles and lasted 47 min.
Thermogravimetric analysis (TGA)
TGA tests were performed on a TGA 2 (Mettler Toledo, USA). Each sample weighed approximately 10 mg. The samples were heated from 25 °C to 600 °C at a rate of 10 °C.min− 1 under a nitrogen atmosphere at a constant flow rate of 80 mL.min− 1. The onset temperature of degradation, maximum degradation temperature, residual weight, and moisture percentage were determined using Stare Software (V17.00, Mettler Toledo, USA). For each sample group, the tests were repeated three times to ensure reproducibility. The onset temperature was calculated according to ISO 11358-1:2022. It is defined as the intersection between the tangent to the baseline before degradation and the tangent at the point of maximum degradation rate. The temperature corresponding to the maximum degradation rate is identified as the peak of the first derivative of the mass loss curve.
Differential scanning calorimetry (DSC)
DSC measurements were performed on a DSC 200 F3 Maia (Netzsch, Germany). Each sample weighed about 10 mg, and each test was conducted under a nitrogen atmosphere. The crucible was a perforated aluminum pan. The cycle consisted of heating at 10 °C.min− 1 from 20 °C to 220 °C, with stabilization for 5 min, followed by cooling from 220 °C to 20 °C, with a 5-minute hold, and finally a second heating from 20 °C to 220 °C at the same rate. The glass transition temperature, melting point and enthalpy of melting were calculated using Proteus Thermal Analysis (8.0.3, Netzsch, Germany). The crystalline weight fraction was determined using the melting enthalpy of 100% crystallized PLGA, \(\:{\varDelta\:H}_{m}^{0}\)=108 J.g−122. Each experiment was repeated three times for each sample group.
Attenuated total reflection-Fourier transform infrared (ATR-FTIR)
The ATR-FTIR spectrum were collected using a Thermo Fisher IS20 spectrometer (Thermo Fisher Scientific, USA), equipped with a diamond ATR crystal. The spectral resolution was set to 4 cm⁻¹, covering a mid-IR spectrum range of 400 to 4000 cm⁻¹. A single spectrum was obtained by co-adding 64 scans and ratioed against the single beam spectrum of the blank ATR crystal at room temperature. The baseline was subtracted using the Adaptive Iteratively Reweighted Penalized Least Squares23. To observe changes in peak intensities, the spectra were normalized to the CH₃ peak at 1380 cm⁻¹, associated with the lactic component of PLGA, as it is the last to degrade24.
Tensile strength test
The mechanical tests were conducted using a Z010 universal testing machine (Zwick Roell, Germany) in a closed chamber with controlled temperature. The tests were performed at 37 °C, which is the average human body temperature, as well as at 50 °C, the average temperature during HPGP. The force was measured using a 1 kN load cell, class 0.5, and the displacement was measured via the machine’s crosshead sensor. The tensile tests were conducted at a speed of 1 mm.min− 1 until the samples exceeded the plastic deformation threshold. In addition to the printed specimens, RX plates and custom zygomatic arch plates were also tested to compare their mechanical performance under the same conditions.
Microtomography
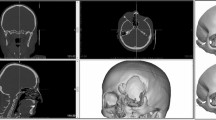
For studying the geometry of the custom-made resorbable plate, a micro-CT scan was performed using the Easytom 160 (RX Solutions, France), set at a tube voltage of 60 kV, a current of 200 µA, with a resolution of 16 μm per voxel, and equipped with flat-panel detector. Segmentation was carried out using AVIZO 3D software (2022.2, Thermo Fisher Scientific, USA). The same plate was subsequently scanned post-sterilization to assess the effects of sterilization on its geometry and internal structure.
Statistical analysis
Data were presented as median values with standard deviations. Statistical analyses were conducted using Prism 10 software (GraphPad, United States). The normality of the distribution was assessed using the Shapiro-Wilk test. For comparisons between two samples, an unpaired, two-tailed test was used. For multiple sample comparisons, ANOVA was employed. If the ANOVA results were significant, post-hoc multiple comparisons were performed using Tukey’s test. In cases where the Shapiro-Wilk test indicated a non-normal distribution, a non-parametric Kruskal-Wallis test was employed. Statistical significance was set at p < 0.05.
The complete methodology is summarized in Fig. 2, while photographs of the machines are provided in Supplementary Figure S1.

Diagram illustrating the overall research methodology, from the initial surgery planning to the mechanical evaluation of the manufactured plates. The process begins with the custom plate design, incorporating parameters such as localization on the bone, geometry, thickness… The designed plate is then manufactured using 3D printing, where biomaterial selection, printing speed, and layer height are critical factors. After fabrication, the plates undergo sterilization, with parameters such as temperature, gas type, pressure, and exposure time considered. Subsequently, the PLGA structure and geometry are analyzed using thermogravimetric analysis (TGA), attenuated total reflection-Fourier transform infrared (FTIR) spectrometer, the differential scanning calorimetry (DSC), and micro-CT scan to assess material properties and potential alterations. The mechanical response of the plates is then evaluated through tensile tests and compared to a standard resorbable plate. The iterative nature of the process allows adjustments at various stages to optimize the final design.
Results and discussion
Thermo-chemical change of 3D printed PLGA
Figure 3a illustrates the degradation profiles of PLGA at various stages of the process: PLGAf refers to the initial commercial filament, PLGAp refers to the filament after 3D printing following the conditions described in the Additive Manufacturing section, and PLGAps refers to the post-sterilization specimens with HPGP. There was no significant difference in the onset temperature of degradation among PLGAps, PLGAp, and PLGAf,, with respective values of 347.3 ± 0.7 °C, 348.8 ± 1.9 °C and 349.1 ± 0.5 °C (one-way ANOVA, p = 0.20). The maximum degradation peak temperatures were similar across the different variants, recorded as 372.5 ± 0.9 °C for PLGAf, 370.0 ± 0.7 °C for PLGAp, and 372.2 ± 1.6 °C for PLGAps (one-way ANOVA, p = 0.15). Prior to printing, the filaments underwent a drying process, but residual moisture was detected in PLGAf at 0.24 ± 0.02%. Following printing, the moisture levels increased to 0.47 ± 0.03% and further to 0.65 ± 0.04% post-sterilization. This increase in moisture content was statistically significant, (ANOVA, p < 0.05, Tukey’s post hoc test, p < 0.001). Although these differences confirm variations in water content, they are not directly visible in Fig. 3 since the graph begins at 250 °C, above the temperature at which any residual water would have evaporated.

( a) TGA curves of PLGA filament, printed PLGA, and printed and sterilized PLGA. (b) First derivative thermogravimetric curves focusing on the decomposition phase of PLGA.
Derivative thermogravimetric analysis (Fig. 3b) reveals a two-step degradation mechanism for all samples, with closely aligned onset and peak temperatures25. The initial step likely corresponds to lower molecular weight chains that degrade earlier. While the 3D printing and sterilization processes slightly increase the proportion of these shorter chains—evidenced by a minor shift of the first degradation peak towards lower temperatures—they do not substantially degrade the overall material. Instead, the process primarily affects only the smaller molecular weight fractions, leaving the bulk polymer properties largely unchanged.
Regarding the DSC analysis (see Fig. 4), the glass transition temperature Tg1 observed during the first heating was 53.6 ± 1.3 °C for the sterilized PLGA, 55.9 ± 1.1 °C for the printed PLGA, and 59.3 ± 0.7 °C for the PLGA filament. Tg1 of PLGAps was broader and did not exhibit an endothermic relaxation peak, suggesting internal stress relaxation26. The Tg1 reduction could be attributed to the presence of water in the samples, exerting a plasticizing effect, and is consistent with the percentage of water estimated by TGA.

DSC curves for PLGA as a filament, after printing, and after printing followed by sterilization.
Contrary to the initial filament, once printed, PLGA exhibited an endothermic reaction at 154 ± 3.5 °C, and at 156.3 ± 3.4 °C after sterilization, corresponding to the melting temperature of PLGA27. Additionally, an exothermic reaction was visible before the melting point for both PLGA and PLGAps, which was attributed to cold crystallization28. The crystallinity for PLGAp is 0.27 ± 0.17%, decreasing to 0% after HPGP sterilization. No melting or cold crystallization was detected during the second heating, confirming that the cold crystallization observed during the first heating of the 3D-printed parts is influenced by the printing parameters29. All the samples can be considered amorphous.
After the second heating, an endothermic relaxation peak persisted just after the glass transition which was due to the relatively slow cooling during the experiment30,31. The glass transition temperature Tg2 during the second heating, which eliminates the material’s thermal history and water, was 58.7 ± 0.2 °C for PLGAf, 58.5 ± 2.5 °C for PLGAp, and significantly decreased to 57.3 ± 0.4 °C after sterilization (one-way ANOVA, p = 0.0033), which is consistent with the literature32. This decrease in Tg2 may be related to an increase in the free amorphous fraction and a reduction in internal stresses33.
The DSC analysis indicates that 3D printing and sterilization impact the thermal properties of PLGA, notably lowering the glass transition temperature due to moisture absorption and internal stresses.
The characteristic functional groups of PLGA were identified by ATR-FTIR of each sample (Fig. 5)24,34. In the single bond region, between 2850 and 3000 cm⁻¹, peaks of CH stretching were observed. The only peak in the double bond region corresponds to the C = O stretching at 1745 cm⁻¹. Characteristic bonds of the glycolic part were found in the fingerprint region between 800 and 1500 cm⁻¹; with CH₂ bending at 1425 cm⁻¹, CH₂ twisting at 1269 cm⁻¹, and CH₂ rocking at 848 cm⁻¹. The lactic part was recognizable by CH₃ at 956, 1383, and 1450 cm⁻¹. Compared to printed PLGA, the PLGA filament showed more pronounced peaks related to ester bonds, particularly the C = O stretching at 1745 cm⁻¹ and COC at 1086 and 1180 cm⁻¹. The reduction in peaks associated with C = O ester bonds after 3D printing could be related to a decrease in molecular weight, a phenomenon already observed and caused by extrusion processes of PLGA18. For PLGAp, it is also noted that the peaks corresponding to CH2 stretching at 2920 and 2850 cm⁻¹ and CH2 twisting at 1269 cm⁻¹ were more pronounced. These results were found by Kister et al. on a polyglycolic acid transitioning from amorphous to crystalline. The DSC results had shown that the PLGA was amorphous, thus the increase in CH2 could be related to the increase in internal stresses after 3D printing35.

ATR - FTIR spectra of PLGA filament, after printing, and after printing and sterilization. ν, stretching; δ, bending; τ, twisting; s, symmetric; as, anti-symmetric.
Mechanical characterization of 3D printed PLGA
During tensile tests conducted at 37 °C (Fig. 6), there was no significant difference in Young’s modulus between the different printing orientations, either before or after sterilization. The median Young’s modulus for all orientations was 1889 ± 293 MPa (Supplementary Table S1) before sterilization, which significantly decreased to 1194 ± 224 MPa after sterilization (t-test, p = 0.0001). The effects of HPGP on PLGA have been relatively understudied. Del Monaco et al.20 examined the impact of HPGP sterilization on PLGA films and did not report a reduction in Young’s modulus. However, their samples were not standardized, and the elastic modulus they measured was significantly lower than that reported in other studies36. For other thermoplastics, the response to HPGP sterilization varies. PLA presents a slight decrease in tensile Young’s modulus after HPGP, while PA12 and PCL show a greater reduction16,37. Annealing 3D-printed polymers generally improves the rigidity of most thermoplastics, even at high temperatures above the glass transition26,38. However, this is not the case for all materials. For example, PETG sometimes shows a decrease in tensile Young’s modulus as the annealing temperature increases39. This behavior is due to the reversal of strain hardening and changes in the amorphous structure, which together lead to a decrease in Young’s modulus. A similar behavior is observed in PLGA, as demonstrated by De Castro et al.40where the compressive modulus of PLGA 85/15 decreases after heat treatment at 70 °C for 90 s.

Representative tensile test curves of PLGA with standardized specimens, before and after sterilization, according to orientation. The black dots indicate tests stopped after reaching maximum stress, while the arrows indicate tests stopped after rupture.
Before sterilization, the vertical orientation samples consistently failed before reaching yield stress at 13.1 ± 3.3 MPa. In contrast, the flat and trench orientations exhibited yield stresses of 27.3 ± 3.4 MPa and 31.2 ± 2.3 MPa, respectively (t-test, p = 0.29). After sterilization, vertical orientation samples reached the yield stress at 22.9 ± 2.8 MPa without premature failure. For the flat and trench orientations, there was no significant difference between the two after sterilization, with yield stresses of 24.6 ± 9.2 MPa and 27.1 ± 9.9 MPa, respectively (t-test, p = 0.36). Regarding the flat and trench orientations, the median yield stress did not change significantly. Before sterilization, it was 28.5 ± 3.1 MPa, and after sterilization, it was 25.6 ± 6.7 MPa (t-test, p = 0.65).
The observed increase in yield stress in the vertical orientation is related to improved interlayer bonding, similar to the effects seen after annealing, where the vertical orientation’s yield stress approaches that of the other orientations41. Enhanced interlayer adhesion improves the mechanical properties of the plates and would simplify finite element simulations for testing various geometries.
To evaluate the mechanical properties during sterilization using the HPGP sterilization, a tensile test was performed at 50 °C on the same type of specimen with the flat orientation. As expected, there was a significant decrease in Young’s modulus and yield stress to 135 ± 19 MPa (t-test, p = 0.0001) and 4 ± 0.7 MPa (t-test, p = 0.0027), respectively. This is explained by the progressive transition from the glassy state at 37 °C to the rubbery state at 50 °C, a temperature close to Tg.
Geometrical and mechanical characteristics of PLGA PSI
FDM printing of PLGA can be challenging initially. The objective was to produce the thinnest plate possible. 0.4 mm nozzle was selected, resulting in extrusion lines of 0.4 mm. Tests with plates of 0.8 mm thickness, with only two parallel extrusion lines of this width led to systematic failures when small overhangs were present. In contrast, plates with a thickness of 1.2 mm, achieved by using three parallel extrusion lines, were successfully printed. The primary printing issues encountered were heat creep, which caused partial nozzle clog and consequently led to under-extrusion. Heat creep occurs when the filament is overheated in the hot end (e.g., excessively high nozzle temperature, printing speed being too slow, insufficient cooling of the hot end, excessively high ambient temperatures). Slightly reducing the printing temperature resulted in layer adhesion defaults, resulting in a narrow optimal printing temperature window for successful PLGA printing.
To evaluate the print accuracy and potential dimensional changes resulting from sterilization, a micro-CT scan was performed on one of the frontotemporal plates, as illustrated in Fig. 1. The same plate was scanned before and after the sterilization process. During microtomography acquisition, hot glue was used to attach the plates to the carbon support. The hot glue has almost the same density as PLGA, making segmentation at these points impossible. All 3 models were truncated at the same location.
To evaluate deviations from the original file, the 3D file was aligned with the two tomographic scans using landmarking with 3D Slicer software42 (Brigham and Women’s Hospital, Boston, Massachussetts, United States). Two distance comparisons were conducted using the ModelToModelDistance extension in 3D Slicer: one comparing the model to the plate before sterilization and the other after sterilization. A color legend was employed to illustrate the distances (ShapePopulationViewer extension, 3D Slicer). While this distance comparison method does not detect defects in small volumes, such as minor overhang-related defects around the holes, it effectively highlights overall deformations. To accurately perform the alignment, we selected 10 feature points on the plate, specifically at distinct locations where extrusion started or ended. These areas exhibited small, repeatable irregularities before and after sterilization, allowing for consistent landmark identification and minimizing positioning errors.
After printing, the plates exhibited excellent dimensional accuracy relative to the original 3D model, with a maximum deviation of 0.1 mm, as shown in Fig. 7. The acceptable error margin for craniofacial surgery is not yet standardized so far but it basically remains under than 0.4 mm for patient-specific implants43. However, the entire process and the final outcomes do not only depend on the PSI itself. It also includes scanning, segmentation, 3D printing and the surgical procedure as well. Interestingly, We previously reported a case series displaying satisfactory outcomes with a root mean square deviation of 1.39 mm between the planned and the postoperative CT scans for hypertelorism patients treated with PSI titanium plates2. Thus, further investigations on resorbable PSI comparing the preoperative planification with the postoperative imaging would be required for a better comprehensive assessment of the accuracy.

Colormap Comparison of the Fronto-Temporal Plate. Panels a and b illustrate the comparison between the PLGA-printed plate and its 3D model across different orientations. Panels c and d show the comparison between the same PLGA-printed plate after sterilization and the 3D model.
Sterilization altered the shape of the plate (Supplementary Figure S2). Specifically, the plate expanded along the Z-axis by 0.27 mm and contracted along the Y-axis by 0.8 mm. The plate was deformed with a displacement of the three vertical holes in the X axis. The volume of the original 3D file is 280 mm³. Once printed, the volume is reduced to 267 mm³, it remains unchanged after sterilization.
These dimensional changes are commonly observed during the annealing of 3D-printed parts38. An increase along the Z-axis is reported, accompanied by a decrease in dimensions along the other two axes. The dimension along the Y axis did not change, likely due to the lack of resolution and the small size of this axis compared to the two others. These changes were related to the internal stresses generated during the 3D printing process, particularly due to rapid cooling. The material was predominantly stretched along the X and Y directions and compressed along the layer thickness (Z direction). During annealing, the relaxation of these stresses leads to contraction in the X and Y dimensions and expansion in the Z dimension39.
In addition to dimensional changes, the frontotemporal plate has bent. During sterilization, the parts were not placed on a flat support but on grids. At a temperature of 50 °C for several tens of minutes, as already mentioned, PLGA becomes rubber-like with a strong decrease of its mechanical properties compared to 37 °C. It is likely that under the influence of gravity and its own weight, the material undergoes plastic deformation. This type of deformation has been observed in the study by Lee et al.19where HPGP of PLGA scaffolds resulted in a reduction in pore size. Regarding other thermoplastics such as PLA, HPGP appears to cause minor deformations, but these are considered negligible by the authors for their applications16,44,45.
The micro-CT scans cross-sectional images in Fig. 8 share the same orientation reference as Fig. 7, in an XZ plane. The first printed layer, which was in contact with the build plate, was positioned at the bottom. The part was not perfectly printed, with occasional under-extrusions characterized by narrower extrusion lines, leading to gaps between two extruded lines. At the bottom right of the parts, a residual brim, used to aid adhesion to the build plate, was visible, as it was not fully removed during post-processing. After sterilization, no internal damage is visible, and the increase in height along the Z-axis is consistent across all layers.

Micro-CT scans of the fronto-temporal piece, before (a) and after sterilization (b), using the same scale and reconstruction plane. The red arrows indicate examples of under-extrusion, and the asterisk (*) marks the residual brim.
In view of the previous results on PLGA samples, similar mechanical tests were conducted on PLGA PSI. A tensile test was performed under the same conditions as for ISO 527-2 type 5B specimens at 37 °C to compare KLS Martin plates (reference 52-876-22-04) made of PDLLA with custom-made plates called zygomatics, shown in Fig. 1c and sterilized with HPGP. The KLS plates were cut to the same length as the custom-made plates. No special adaptation system was used for the grips, as the “zygomatics” plates were relatively flat within the grips, maintaining an unchanged initial distance between the grips (L0) of 10 mm. The maximum force recorded at the yield point for the KLS Martin plates was 76.0 ± 1.2 N, with an elongation of 3.6 ± 0.1%. For the zygomatics plates, the maximum force at yielding was significantly higher 150.0 ± 18.2 N (t test, p = 0.004), with no difference in elastic elongation, at 3.5 ± 0.2% (t-test, p = 0.1). Compared to KLS Martin Resorb X plates, a PLGA printed plate, even after sterilization, exhibited greater stiffness and greater load at yield. Although the two solutions are not directly comparable due to their differences in shape and material, the design presented here is able to meet surgical expectations. This increased rigidity is not necessary in the craniofacial context, as the forces exerted on the face are minimal, suggesting the potential for optimizing the shape and reducing the amount of material used.
Despite being classified as a low-temperature process, the thermal treatment associated with HPGP had a significant impact on the material’s mechanical properties. Additionally, there was a reduction in Young’s modulus post-sterilization. When combined with the observed modifications in DSC and the dimensional changes, these results suggest a release of internal stresses, consistent with an annealing effect38,46.The observed deformation of the plates during sterilization is likely due to the collapse in Young’s modulus and the stress at deformation at 50 °C, a temperature close to the Tg of the printed PLGA. Additionally, the low-pressure conditions during HPGP may further reduce the Tg47 and mechanical properties48exacerbating the risk of deformation, although the specific effects of low pressure on this copolymer require further study.
Conclusion
This study demonstrates the potential of PLGA as a promising material for the manufacturing of resorbable patient-specific devices using FDM technology, specifically for craniofacial surgery. The shapes obtained after 3D printing closely matched the original 3D file. The manufacturing quality of PLGA filament spools, along with the precision and repeatability of FDM printers, enables the production of osteosynthesis plates with sufficient accuracy for craniofacial applications. The geometry during the design of the plates must consider the constraints associated with FDM printing to achieve the best result as possible. Sterilization is an essential step in the development of implantable medical devices, and in case of HGPG, it introduces significant dimensional and morphological changes.
The limitations of this study include the fact that only one sterilization protocol was tested. It would have been interesting to try the rapid cycle, which lasts 24 min and could potentially limit the observed deformations, reduce sterilization efficacy, necessitating bacteriological testing. As it stands, only gamma rays seem possible for sterilizing PLGA medical devices without deformation, which would not be compatible with a fully in-house manufacturing process32. Additionally, only one plate was evaluated using microtomography. It would be beneficial to conduct multiple trials and anticipate deformations related to HPGP. If the deformations and the positioning of the printed objects in the sterilization chamber are known and controlled, it may be possible to anticipate and compensate for these deformations during the design phase of the implant, similar to the approach used in the 3D printing of ceramics49.
Our study showed promising findings in terms of mechanical features. More investigations on the macro and microarchitecture (e.g., surface roughness, porosity and specific surface area) as well as on the cell behavior (e.g., cell attachment and cell differentiation) are required in further experimentations.
The results on the effects of plasma hydrogen peroxide sterilization on PLGA are consistent with the literature, indicating a reduction in mechanical properties and morphological changes post-sterilization.
Sterility and cytotoxicity tests remain to be conducted for this specific application. Future studies should also explore the deformations caused by the sterilization process to develop strategies for anticipating and mitigating these issues during the design phase. Overcoming these challenges could lead to advancements in personalized craniofacial surgery, potentially reducing the need for secondary interventions and improving patient outcomes.
Data availability
The data are available upon request from the corresponding author.
References
Ahmad, W. et al. Fixation in maxillofacial Surgery—Past, present and future: A narrative review Article. FACE 5, 126–132. https://doi.org/10.1177/27325016231221424 (2024).
Batut, C., Paré, A., Kulker, D., Listrat, A. & Laure, B. How accurate is Computer-Assisted orbital hypertelorism surgery?? Comparison of the Three-Dimensional surgical planning with the postoperative outcomes. Facial Plast. Surg. Aesthet. Med. 22, 433–440. https://doi.org/10.1089/fpsam.2020.0129 (2020).
Schlund, M., Paré, A., Joly, A. & Laure, B. Computer-assisted surgery in facial bipartition surgery. J. Maxillofac. Oral Surg. 76 https://doi.org/10.1016/j.joms.2017.12.013 (2018).
Calluaud, G., Pare, A., Kulker, D., Listrat, A. & Laure, B. Computer-Assisted frontofacial monobloc advancement and facial bipartition for Pfeiffer syndrome: surgical technique. World Neurosurg. 161, 97–102. https://doi.org/10.1016/j.wneu.2022.02.031 (2022).
Berryhill, W. E., Rimell, F. L., Ness, J., Marentette, L. & Haines, S. J. Fate of rigid fixation in pediatric craniofacial surgery. Otolaryngol. --head Neck Surg. 121, 269–273. https://doi.org/10.1016/S0194-5998(99)70183-X (1999).
Heye, P. et al. Making hardware removal unnecessary by using resorbable implants for osteosynthesis in children. Children 9, 471. https://doi.org/10.3390/children9040471 (2022).
Branch, L. G. et al. Long-Term outcomes of pediatric cranial reconstruction using resorbable plating systems for the treatment of craniosynostosis. J. Craniofac. Surg. 28, 26–29. https://doi.org/10.1097/SCS.0000000000003166 (2017).
Chavan, Y. R., Tambe, S. M., Jain, D. D., Khairnar, S. V. & Amin, P. D. Redefining the importance of polylactide-co-glycolide acid (PLGA) in drug delivery. Ann. Pharm. Fr. 80, 603–616. https://doi.org/10.1016/j.pharma.2021.11.009 (2022).
Madani, F. et al. Combination chemotherapy via poloxamer 188 surface-modified PLGA nanoparticles that traverse the blood–brain–barrier in a glioblastoma model. Sci. Rep. 14, 19516. https://doi.org/10.1038/s41598-024-69888-1 (2024).
Pan, Z. & Ding, J. Poly(lactide- Co -glycolide) porous scaffolds for tissue engineering and regenerative medicine. Interface Focus. 2, 366–377. https://doi.org/10.1098/rsfs.2011.0123 (2012).
Sun, F. et al. Application of 3D-printed, PLGA-based Scaffolds in bone tissue engineering. IJMS. https://doi.org/10.3390/ijms23105831 (2022).
Zhang, M. et al. Personalized PLGA/BCL scaffold with hierarchical porous structure resembling Periosteum-Bone complex enables efficient repair of bone defect. Adv. Sci. (Weinh). 11, e2401589. https://doi.org/10.1002/advs.202401589 (2024).
Zhao, D. et al. Poly(lactic-co-glycolic acid)-based composite bone-substitute materials. Bioactive Mater. 6, 346–360. https://doi.org/10.1016/j.bioactmat.2020.08.016 (2021).
Pilling, E. et al. An experimental study of the Biomechanical stability of ultrasound-activated pinned (SonicWeld Rx®+Resorb-X®) and screwed fixed (Resorb-X®) resorbable materials for osteosynthesis in the treatment of simulated craniosynostosis in sheep. Br. J. Oral Maxillofac. Surg. 45, 451–456. https://doi.org/10.1016/j.bjoms.2006.12.008 (2007).
Gareb, B. et al. Comparison of the mechanical properties of biodegradable and titanium osteosynthesis systems used in oral and maxillofacial surgery. Sci. Rep. 10, 18143. https://doi.org/10.1038/s41598-020-75299-9 (2020).
Valls-Esteve, A. et al. A state-of-the-art guide about the effects of sterilization processes on 3D-printed materials for surgical planning and medical applications: A comparative study. IJB 9, 756. https://doi.org/10.18063/ijb.756 (2023).
Maintz, M. et al. Patient-specific implants made of 3D printed bioresorbable polymers at the point-of-care: material, technology, and scope of surgical application. 3D Print. Med. 10, 13. https://doi.org/10.1186/s41205-024-00207-0 (2024).
Gradwohl, M. et al. Effects of two melt extrusion based additive manufacturing technologies and common sterilization methods on the properties of a medical grade PLGA copolymer. Polymers 13, 572. https://doi.org/10.3390/polym13040572 (2021).
Lee, M. H. et al. Effects of low temperature hydrogen peroxide gas on sterilization and cytocompatibility of porous poly(d,l-lactic-co-glycolic acid) scaffolds. Surf. Coat. Technol. 202, 5762–5767. https://doi.org/10.1016/j.surfcoat.2008.06.114 (2008).
Del Monaco, A., Duek, E., Andrade, A. J. P. D. & Malmonge, S. Alternative methods of sterilization on films of polymers: Poly(-L-lactic acid) (PLLA), Poly(L-lactic acid-co-glycolic acid) (PLGA) and Poly(-LD-lactic acid) (PLDLA), for bioresorbable vascular scaffolds models. TASJ 248–256. https://doi.org/10.32640/tasj.2018.4.248 (2018).
Kulker, D. et al. Surgical management of hypertelorism: the 3D animated technical note. J. Craniofac. Surg. 34, 391–392. https://doi.org/10.1097/SCS.0000000000009014 (2023).
Murcia Valderrama, M. A., Van Putten, R. J. & Gruter, G. J. M. PLGA barrier materials from CO 2. The influence of lactide Co-monomer on glycolic acid polyesters. ACS Appl. Polym. Mater. 2, 2706–2718. https://doi.org/10.1021/acsapm.0c00315 (2020).
Zhang, Z. M., Chen, S. & Liang, Y. Z. Baseline correction using adaptive iteratively reweighted penalized least squares. Analyst 135, 1138. https://doi.org/10.1039/b922045c (2010).
Vey, E. et al. Degradation kinetics of poly(lactic-co-glycolic) acid block copolymer cast films in phosphate buffer solution as revealed by infrared and Raman spectroscopies. Polym. Degrad. Stab. 96, 1882–1889. https://doi.org/10.1016/j.polymdegradstab.2011.07.011 (2011).
Chen, Z. et al. Degradation behaviors of polylactic acid, polyglycolic acid, and their copolymer films in simulated marine environments. Polymers 16, 1765. https://doi.org/10.3390/polym16131765 (2024).
Zennaki, A. et al. Effect of annealing on thermal and dynamic mechanical properties of poly(lactic acid). J. Appl. Polym. Sci. 139, e53095. https://doi.org/10.1002/app.53095 (2022).
Melo, L. P. D., Salmoria, G. V., Fancello, E. A. & Roesler, C. R. D. M. Effect of injection molding melt temperatures on PLGA craniofacial plate properties during in vitro degradation. Int. J. Biomater. 1–11. https://doi.org/10.1155/2017/1256537 (2017).
Carmagnola, I. et al. Poly(Lactic Acid)-Based blends with tailored physicochemical properties for tissue engineering applications: A case study. Int. J. Polym. Mater. 64, 90–98. https://doi.org/10.1080/00914037.2014.886247 (2015).
Cadete, M. S., Gomes, T. E. P., Gonçalves, I. & Neto, V. Influence of 3D-printing deposition parameters on crystallinity and morphing properties of PLA-based materials. Prog Addit. Manuf. https://doi.org/10.1007/s40964-024-00608-x (2024).
Pan, P., Zhu, B. & Inoue, Y. Enthalpy relaxation and embrittlement of Poly(l -lactide) during Physical Aging. Macromolecules 40, 9664–9671. https://doi.org/10.1021/ma071737c (2007).
Surana, R., Pyne, A., Rani, M. & Suryanarayanan, R. Measurement of enthalpic relaxation by differential scanning calorimetry—effect of experimental conditions. Thermochim Acta. 433, 173–182. https://doi.org/10.1016/j.tca.2005.02.014 (2005).
Pérez Davila, S., González Rodríguez, L., Chiussi, S., Serra, J. & González, P. How to sterilize polylactic acid based medical devices?? Polymers 13, 2115. https://doi.org/10.3390/polym13132115 (2021).
Wei, Z. et al. Insight into the annealing peak and microstructural changes of poly(l-lactic acid) by annealing at elevated temperatures. Polymer 54, 3377–3384. https://doi.org/10.1016/j.polymer.2013.04.027 (2013).
Keles, H., Naylor, A., Clegg, F. & Sammon, C. Studying the release of hGH from gamma-irradiated PLGA microparticles using ATR-FTIR imaging. Vib. Spectrosc. 71, 76–84. https://doi.org/10.1016/j.vibspec.2014.01.012 (2014).
Kister, G., Cassanas, G. & Vert, M. Morphology of poly(glycolic acid) by IR and Raman spectroscopies. Spectrochim Acta Mol. Biomol. Spectrosc. 53, 1399–1403. https://doi.org/10.1016/S0584-8539(97)00039-1 (1997).
Biomaterials et al. Degradable polymeric materials for osteosynthesis: Tutorial. eCM 16, 80–91 (2008). https://doi.org/10.22203/eCM.v016a09
Sosnowski, E. P. & Morrison, J. Sterilization of medical 3D printed plastics: Is H2O2 vapour suitable? In CMBES Proceedings. Vol. 40 (2017).
Butt, J. & Bhaskar, R. Investigating the effects of annealing on the mechanical properties of FFF-printed thermoplastics. JMMP 4 (38). https://doi.org/10.3390/jmmp4020038 (2020).
Yu, W., Wang, X., Yin, X., Ferraris, E. & Zhang, J. The effects of thermal annealing on the performance of material extrusion 3D printed polymer parts. Mater. Design. 226, 111687. https://doi.org/10.1016/j.matdes.2023.111687 (2023).
de Castro, P. B., Salmoria, G. V., Roesler, C. R. D. M., Rosa, D., Fancello, E. A. A study on the response of PLGA 85/15 under compression and heat-treatment testing cycles. Mech. Time-Depend Mater. 25, 411–427. https://doi.org/10.1007/s11043-020-09451-3 (2021).
Szust, A. & Adamski, G. Using thermal annealing and salt remelting to increase tensile properties of 3D FDM prints. Eng. Fail. Anal. 132, 105932. https://doi.org/10.1016/j.engfailanal.2021.105932 (2022).
Kikinis, R., Pieper, S. D. & Vosburgh, K. G. 3D Slicer: A Platform for Subject-Specific Image Analysis, Visualization, and Clinical Support. In: Jolesz, F. A. (ed.) Intraoperative Imaging and Image-Guided Therapy, 277–289, Springer New York. https://doi.org/10.1007/978-1-4614-7657-3_19 (2014).
Wang, X. et al. 3D printing materials and 3D printed surgical devices in oral and maxillofacial surgery: design, workflow and effectiveness. Regenerative Biomaterials. 11, rbae066. https://doi.org/10.1093/rb/rbae066 (2024).
Oth, O., Dauchot, C., Orellana, M. & Glineur, R. How to sterilize 3D printed objects for surgical use? An evaluation of the volumetric deformation of 3D-printed genioplasty guide in PLA and PETG after sterilization by low-temperature hydrogen peroxide gas plasma. TODENTJ 13, 410–417. https://doi.org/10.2174/1874210601913010410 (2019).
Rynio, P. et al. Effects of sterilization methods on different 3D printable materials for templates of Physician-Modified aortic stent grafts used in vascular Surgery—A preliminary study. IJMS 23, 3539. https://doi.org/10.3390/ijms23073539 (2022).
Loo, C. J., Ooi, S., Elyna Wee, C. P. H. & Chiang Freddy Boey, Y. Effect of isothermal annealing on the hydrolytic degradation rate of poly(lactide-co-glycolide) (PLGA). Biomaterials 26, 2827–2833. https://doi.org/10.1016/j.biomaterials.2004.08.031 (2005).
Bianchi, U. Pressure dependence of glass transition temperature in polymers. Rheol Acta. 10, 213–213. https://doi.org/10.1007/BF02040443 (1971).
Aulova, A., Oseli, A., Bek, M., Prodan, T. & Emri, I. Effect of pressure on mechanical properties of polymers. in Encyclopedia of Continuum Mechanics (eds Altenbach, H. & Öchsner, A.) 1–14 https://doi.org/10.1007/978-3-662-53605-6_270-2 (Springer, 2019).
Zhu, Y. et al. 3D printed zirconia ceramic hip joint with precise structure and broad-spectrum antibacterial properties. IJN 14, 5977–5987. https://doi.org/10.2147/IJN.S202457 (2019).
Acknowledgements
We would like to thank CERMEL (Centre d’Etudes et de Recherche sur les Matériaux Elastomères) for providing access to the experimental equipment used in this project, and LaMé (Laboratoire de mécanique Gabriel Lamé) for purchasing the materials and lending the 3D printer.
Author information
Authors and Affiliations
Contributions
D.K. and A.P. drafted the manuscript. D.K. and M.V. conducted the experiments. D.K., J.P., M.V. and J.P. interpreted the data. B.L., B.R., J.B. and A.P. designed the experimental study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kulker, D., Pepin, J., Rosa, B. et al. Physico-mechanical characterization of 3D-printed PLGA for patient-specific resorbable implants in craniofacial surgery. Sci Rep 15, 22225 (2025). https://doi.org/10.1038/s41598-025-07617-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-07617-y
