
Abstract
Self-advocacy is essential for self-management in stroke patients. However, a validated scale to assess the level of self-advocacy in this population is lacking. This study aimed to develop a self-advocacy scale for stroke patients and validate its psychometric properties. This cross-sectional study involved instrument development and psychometric testing, conducted in three stages. In stage 1, dimensions and items were generated through concept analysis, semi-structured interviews, and refined through a Delphi survey. Stage 2 focused on content and face validity assessment. Stage 3 evaluated psychometric properties. A total of 565 stroke patients participated in the items selection from August 2024 to November 2024. The self-advocacy scale was assessed through content validity, construct validity, internal consistency, and test-retest reliability. The study adhered to the STROBE checklist for reporting. From an initial 40-item pool, 24 items were retained after expert consultation and item analysis. The scale demonstrated a content validity index of 0.967. Exploratory factor analysis revealed a five-factor structure, explaining 68.285% of the total variance. Confirmatory factor analysis supported this structure with acceptable fit indices. The scale’s overall Cronbach’s α coefficient was 0.936, with the dimensions’ Cronbach’s α values ranging from 0.816 to 0.898. Split-half reliability was 0.874, and test-retest reliability was 0.885 (2-week interval). The 24-item self-advocacy scale for stroke patients demonstrated robust psychometric properties, providing a valid tool for clinical and research applications.
Similar content being viewed by others


Introduction
According to Global Burden of Disease (GBD) studies, stroke ranks as the second leading cause of disability-adjusted life years (DALYs) and mortality worldwide1. In China, it is the foremost cause of death and disability among adults2. At present, the health management status of stroke patients in China is not optimistic. In addition to poor control of risk factors such as hypertension, diabetes and dyslipidemia, stroke patients also have the status quo of smoking, drinking, poor eating habits, insufficient exercise and poor medication compliance3,4. Addressing these challenges requires innovative strategies, with health management playing a pivotal role in secondary prevention. Self-advocacy may offer a novel approach to enhancing the health management of stroke patients.
Self-advocacy refers to the willingness and ability of patients to represent their own interests when managing diseases or disabilities, including obtaining relevant information and communicating their own needs and care preferences effectively with health care providers5,6. Self-advocacy emphasizes the active participation of patients, focusing on their experiences and needs, and interacts with medical staff and the environment, which fully reflects the patient-centered nursing model7,8. Empirical studies9,10,11 demonstrates that self-advocacy can directly or indirectly improve patient health outcomes, such as improving patient compliance, quality of life and satisfaction with care. Individuals obtain the information and support they need to manage related diseases through self-advocacy10, thereby obtaining higher-quality, patient-centered care12.
At present, foreign studies related to self-advocacy mainly originate from cancer13, AIDS5,12, mental illness9,14, patients with acquired brain injury15, and the elderly16. Some self-advocacy related assessment tools have been constructed and verified in this process. but the relevant assessment tools have variability depending on the research subjects and measurement indicators. In China, Self-advocacy related research is still in the exploratory stage17,18, with the research object mostly focusing on tumor patients, and the research content involves the Chineseization of the scale, validation, and the exploration of influencing factors. In general, there is still a lack of domestic and international research on self-advocacy in stroke patients, and there is no specific assessment tool. Moreover, there are significant differences in the applicable population, construction methods and contents of self-advocacy assessment tools, which cannot better reflect the population characteristics of stroke patients. In view of this, it is necessary to carry out basic research work such as the development of assessment tools, in order to provide reference for further research on self-advocacy of chronic disease groups such as stroke. In conclusion, this study aims to conceptualize self-advocacy in stroke patients through systematic concept analysis and qualitative exploration, integrating theoretical frameworks with clinical insights, and develop a psychometrically robust assessment instrument to enable healthcare providers to quantitatively evaluate patients’ self-advocacy levels, thereby informing the design of targeted intervention strategies.
Methods
Aim
The aim of this study was to develop a new instrument for assessing the self-advocacy for patients who had a stroke and to examine its psychometric properties.
Design
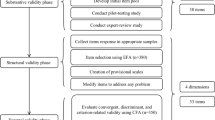
A cross-sectional, three-stage study was conducted using both quantitative and qualitative approaches to develop and validate self-advocacy scale for patients with stroke. It involved three stages: (1) item generation and revision; (2) content and face validation; (3) psychometric properties evaluation. The development process of the scale is shown in Fig. 1. The study report followed the STROBE statement: standards for reporting observational studies (supplementary file 1)19.

The development process of the self-advocacy scale for patients with stroke.
Stage 1: items generation and revision
Concept analysis
In the first stage, literature review was conducted. Using the Rodgers evolutionary concept analysis method20, with “self-advocacy” and “advocacy” as the main topics, we searched PubMed, Web of Science, EBSCO, Embase, PsycINFO, CNKI, Wanfang database, VIP database and CBMdisc database. The search period was from the establishment of the database to August 30, 2023. The search results showed that there were few literatures related to self-advocacy in stroke patients, and the search scope was expanded to include chronic disease patients. Through systematic literature review and analysis, this paper analyzes and integrates the relevant contents of the concept of self-advocacy, and summarizes the conceptual attributes of the self-advocacy of patients with chronic diseases into four core characteristics: self-cognition, self-decision making, effective communication and connection power. The definition of the concept attributes provides a theoretical reference for the division of the initial scale dimensions, the results of this part have been published21.
Qualitative interview
A descriptive qualitative design was implemented, involving semi-structured interviews with 19 stroke patients, 6 caregivers and 8 medical staff from Zhengzhou Central Hospital and Luoyang Central Hospital in Henan Province, China from October 2023 to February 2024, to explore the cognitive experience of stroke patients’ self-advocacy. This phase aimed to operationalize the conceptual framework of self-advocacy in stroke patients and inform scale development. The interview outline were shown in supplementary file 2. The data were analyzed by the method of content analysis and partial reference to grounded theory22,23. The results showed that the concept of self-advocacy in stroke patients included 5 themes and 14 sub-themes. They are as follows: awareness of rights and interests (clear scope of rights, use of health services, maintain firm beliefs), self-cognition (accept the facts of the disease, have knowledge of the disease, know their needs), effective communication (express their needs, take the initiative to get satisfied), seeking support (self-support, family support, social support, social participation), and self-decision making (weighing pros and cons/risks, conscious not to follow blindly). According to the theme and content extracted by qualitative research, the scale item dimension and item pool were adjusted and supplemented to form the initial scale item pool (including 5 dimensions and 40 items).
Delphi consultation
The next, we invited experts from multiple fields: chronic disease management, rehabilitation, neurology, health service and nursing for Delphi consultation from May 2024 to June 2024. Consultation experts were chosen based on three criteria: (1) having at least ten years of work experience, (2) holding an intermediate or advanced level certificate, and (3) willing to participate in the study. A total of 18 experts from eight provinces of China participated in the survey. After two rounds of consultation, the content of the dimensions and items were agreed upon by the experts. Kendall’s concordance coefficient was used to determine the level of agreement among the experts24. In the two Delphi consultation rounds, Kendall’s W test was statistically significant (p < 0.01), indicating that the experts were in agreement. A total of 13 items were modified, 7 were deleted, 11 were combined, 3 items were added, and 9 were altered. This resulted in a final draft of 30 items.
Stage 2: content and face validation
Following item generation, 18 experts were invited to assess the scale’s content validity. The experts were from multiple fields, and the inclusion criteria are the same as in stage 1. To gather expert opinions, a four-point Likert scale was used, with one point (irrelevant) and four points (highly relevant). The item’s content validity index (I-CVI) was calculated by dividing the number of experts who gave it 3 or 4 points by the total number of experts. Each item’s I-CVI score was averaged to calculate the scale’s content validity index (S-CVI). An S-CVI score of 0.90 or higher and an I-CVI score of 0.78 or higher were required to meet the content validity standards25.
Following the experts’ evaluation of the content validity, we conducted an preliminary exploration of the 30-item scale. Since the 5-point scale form was most frequently chosen as the easiest to complete and item omission was least prevalent, we employed the 5-level Likert scoring method (Strongly disagree = 1, disagree = 2, General = 3, agree = 4, Strongly agree = 5)26,27. The preliminary scale was piloted on 20 stroke survivors prior to the formal investigation to make sure it was understandable and appropriate for formal research. After completing the instrument, stroke survivors were asked to assess a problem’s significance, ease of use, accuracy, ambiguity, and whether there is a better way to describe it28. They were also invited to offer ideas on how the instrument could be made better.
Stage 3: psychometric properties evaluation
Participants and setting
We recruited stroke patients from two hospitals (Zhengzhou City Central Hospital and Luoyang City Central Hospital) in Henan province, China, using convenience sampling between August 2024 and November 2024 after obtaining approval from the hospital’s administrative office. The study’s inclusion criteria were as follows: participants had to be 18 years of age or older, survivors of different types of stroke29; have communication skills (Token test ≥ 17 points)30; self-care capability (activities of daily living ≥ 40)31; individuals without cognitive dysfunction (mini mental state examination ≥ 17 points)32, and give their informed consent to participant in the study.
The sample size was established using the general rule of the factor analysis33,34, which suggested a sample size-to-item ratio between 5 and 10, and a 10% sample loss rate, and an absolute sample size of at least 20035. Ultimately, a total of 565 stroke survivors were finally included in the study. This sample were randomly assigned to two groups. Sample A comprised 265 stroke survivors for exploratory factor analysis (EFA), item analysis and reality analysis. Sample B comprised 300 stroke survivors for confirmatory factor analysis (CFA). A total of 30 out of the 265 stroke survivors indicated their interested and participated.
Item analysis
Every item on the self-advocacy scale for stroke patients was tested and examined using item analysis in order to screen and assess the items’ quality. For item analysis, a variety of analytical techniques were employed, such as critical ratio (CR) analysis, correlation coefficient analysis, and Cronbach’s α. To evaluate the discrimination of the items, the samples were separated into two groups: one with high scores (top 27%) and the other with low scores (bottom 27%). For every item, a critical ratio of 3.0 or more was considered acceptable and significant (P < 0.05)36. To evaluate the items’ applicability, item-total correlation coefficients were computed, with a minimum correlation coefficient of 0.4 being required. Cronbach’s α coefficient was used to evaluate the items’ homogeneity after each item was removed. Ideally, deleting any item should not increase the total Cronbach’s α coefficient. Items were removed from the initial scale if they failed to meet these requirements37,38.
Construct validity
To determine the scale’s factor structure, exploratory factor analysis (EFA) was used. The appropriateness of factor analysis was verified using the Bartlett’s test of sphericity (p < 0.05) and the Kaiser-Meyer-Olkin coefficient (KMO > 0.6). The number of retrieved elements was determined using a scree plot and eigenvalues > 1. We eliminated items that had a factor loading of less than 0.4, a factor loading across two or more factors, and a difference of less than 0.239. More than 40% of the total variance should be explained by all common components40,41,42.
To confirm the fit of the factor structure obtained from the EFA in sample B, confirmatory factor analysis (CFA) was carried out. For CFA, a sample size of 200 would be adequate43. By computing the following indices, the overall fit of the model was ascertained: the RMSEA (root mean square error of approximation), the TLI (tacker-lewis index), the IFI (incremental fit index), the GFI (goodness-of-fit index), the ratio between chi-square and the degrees of freedom (χ2/df), and the chi-square goodness-of-fit test. A model that was deemed acceptable was indicated by the GFI values being > 0.80 and the RMSEA being less than 0.08. A value > 0.90 for the CFI, TLI, and IFI indicates that the model path map and the real data fit each other well44,45.
The average variance extracted (AVE) and composite reliability (CR) values were computed in order to evaluate the convergent validity. When the AVE value is more than 0.50 and the CR value is more than 0.70, the scale has acceptable convergent validity46. Correlation coefficients between variables and the square root of the AVE value were used to assess discriminant validity. The square root of the AVE value must be greater than the correlation coefficients between the respective components46.
Internal consistency reliability and test-retest reliability
The internal consistency reliability of the scale was evaluated by computing the split-half reliability coefficient and the Cronbach’s α coefficient. In order to evaluate the scale’s consistency across time, 30 participants who had already completed the survey were asked to do so again two weeks later. The split-half reliability coefficient, the Cronbach’s α coefficient, and the test-retest reliability coefficient must all be 0.70 or more to demonstrate strong internal consistency, reliability, and test-retest reliability47,48.
Data collection
Informed permission and expert consultation questionnaire outlining the study’s purpose and significance were distributed to the experts via WeChat or email. Experts were requested to provided feedback and suggestions within two weeks of receiving the questionnaire. A total of 580 stroke survivors participated in the survey between August 2024 and November 2024 from two hospitals in Henan, China. Prior to formal investigation, the researchers were fully trained in conducting the questionnaire survey. Among the 580 invited stroke patients, 565 valid questionnaires were obtained.
Data analysis
Data were analyzed using SPSS 26.0 and AMOS 26.0 software. The scale’s items were revised, and its content validity was assessed through the Delphi survey. To investigate the underlying factor structure, the maximum variance rotation was used in the EFA. The structural equation model for the CFA was established using the maximum likelihood method in order to confirm that the factor structure and the predicted dimension were consistent. In order to verify the reliability of the scales, internal consistency analysis and test-retest reliability analysis were used to evaluate the stability and homogeneity of the scales, respectively.
Ethical consideration
This study was approved by the Research Ethics Committee of Zhengzhou University (ZZUIRB2023-277). For formal investigation, the participants were explained the purpose and procedure of the research and invited to sign an informed consent form. Participants had complete autonomy to discontinue participation in the study at any time.
Results
Content and face validity
Content validity was assessed via email or WeChat consultations with 18 experts. In the first round of content validity evaluation, the scale content validity index (S-CVI) was 0.814, whereas the item content validity index (I-CVI) varied between 0.389 and 1.000. 13 items were altered, 7 were removed, 11 were combined, 3 were added, and 4 were changed. Consequently, a draft of 30 items was produced. During the second evaluation round, the scale content validity index (S-CVI) was 0.967, while the item content validity index (I-CVI) varied between 0.833 and 1.000. Minor refinements were made to 5 items in this phase, including the addition of two guiding words and no items deletions, resulting in total of 30 retained items.
A pilot survey was administered to 20 stroke survivors. The completion time of the scale was approximately 11 min, indicating appropriate item count and complexity. In addition, additional explanations were made based on the unclear presentation of individual items in the stroke survivor feedback scale, such as the addition of “(e.g., daily needs and medical needs)” to item 12 and item 20. As a result, the revised 30-item self-advocacy scale was chosen as the psychometric test version.
Psychometric testing of the scale
Participants characteristics
A total of 580 participants surveyed, 565 (97.4%) completed the questionnaire. The participants’ demographic characteristics are shown in Table 1.
Item analysis
The item analysis results of the self-advocacy scale are presented in Table 2. Items with a CR with p > 0.05, items with a corrected item-total correlation coefficient value lower than 0.4, and items with Cronbach’s α of the scale more than 0.950 were considered for deletion. Results indicated that item 24 failed to meet the correlation coefficient threshold. However, considering that family and friends are an important source of social support for stroke patients and that the correlation coefficient between this item and the total scale and 0.4 is relatively close, this item was retained after team discussion. Ultimately, no items were deleted based on item analysis criteria.
Construct validity
The KMO value was 0.923 and Bartlett’s test of sphericity (χ2 = 5161.682, p < 0.001) reached significance, confirming data suitability for EFA. Scree plot analysis supported a five-factor solution. Items 13, 20, and 25 were deleted because their factor loadings were less than 0.4. Items 2, 6, and 28 were deleted because they had cross loadings. Then we performed the second EFA for the remaining 24 items. The KMO value was 0.908 and Bartlett’s test of sphericity (χ2 = 4009.113, p < 0.001). The five-factor structure (Fig. 2) expialined 68.285% of the total variance, with individual factor contributions as follows: 17.076%, 14.464%, 12.784%, 12.250%, and 11.711%. Detailed results are shown in Table 3.

Screen plot of exploratory factor analysis for the self-advocacy scale(n = 265).
The initial structural model was modified in CFA based on the modification index, and the adjusted fitting indices were analyzed (Fig. 3). The following fit indices demonstrated an acceptable fit for the five-factor structure: χ2/df = 2.586, RMSEA = 0.073, GFI = 0.845, CFI = 0.924, TLI = 0.912, IFI = 0.925. The selected fitting indices provided further evidence consistent with the EFA results, indicating that the five-factor structure scale exhibited an appropriate fit. In the convergent validity analysis, the AVE values ranged from 0.570 to 0.674, and CR values ranged from 0.864 to 0.912. In the discriminant validity analysis, the square root values of AVE fluctuated between 0.755 and 0.821, each exceeding the correlation coefficients of their respective factors (Table 4).

The five-factor model of the self-advocacy scale (n = 300). F1 (Factor 1): awareness of rights and interests; F2 (Factor 2): self-cognition; F3 (Factor 3): effective communication; F4 (Factor 4): seeking support; F5 (Factor 5): self-decision making. V1-V30 indicates specific items in different dimensions.
Internal consistency reliability and test-reliability
For the self-advocacy scale, the split-half reliability and Cronbach’s α were 0.874 and 0.936, respectively. The split-half reliability and Cronbach’s α of each scale dimension ranged from 0.756 to 0.871 and from 0.816 to 0.898, respectively. The retest reliability of each dimension ranged from 0.755 to 0.853, while the average test-retest reliability of the overall scale was 0.885. Table 5 presents the results of this investigation.
Final instrument
The self-advocacy scale for stroke patients comprises 30 items across 5 dimensions: (1) Awareness of rights and interests (4 items); (2) Self-cognition (6 items); (3) Effective communication (5 items); (4) Seeking support (5 items); and (5) Self-decision making (4 items). All items are rated on a 5-point Likert scale (1 = Strongly disagree, 5 = Strongly agree) to assess the current self-advocacy status of stroke survivors. The scale score ranges from 24 to 120, with higher scores indicating better self-advocacy.
Discussion
Accurate and objective assessment of the self-advocacy level in stroke patients may provide a new breakthrough for research related to stroke patients’ health management. It also helps nursing staff to formulate targeted and individualized health education and nursing intervention plans. In recent years, international scholars10,11,49 have increasingly focused on self-advocacy, achieving significant research outcomes. However, domestic studies in this field remain in their infancy, primarily focusing on female cancer patients17,18, with a lack of scientific and effective assessment tools for other study populations. This study developed and verified the reliability and validity of a 30-item self-advocacy scale for stroke patients. The research results showed that it had sufficient content validity, internal consistency, structural validity and re-test reliability. In the scale development process of this study, the principles and procedures of scale development were strictly followed.
This study developed the initial draft of the scale through concept analysis, semi-structured interviews, and other methods, following a scientific and standardized process. The initial draft was revised via the Delphi method and pre-survey to form the initial scale. The concept analysis of self-advocacy among patients with chronic diseases identified four concept attributes, namely self-cognition, self-decision making, effective communication, and connection with power, providing theoretical references for the dimension division of the initial scale. Through semi-structured interviews with stroke patients, caregivers, and medical staff, five concept connotations of self-advocacy among stroke patients were deeply explored, namely awareness of rights and interests, self-cognition, effective communication, seeking support, and self-decision making, offering rich information for determination the initial scale dimensions and establishing the item pool. The selection of experts for the Delphi method fully considered the authority and representativeness of the experts, covering related fields such as medicine, nursing, management, and psychology. The 18 experts were from eight different provinces in China, with an average working experience of over 10 years, and possessed good scientific research literacy and ability. The positive response rates of the two rounds of expert inquiries were both > 70%, and the Kendall’s coefficient of concordance of the two rounds of experts were 0.167 and 0.130 respectively, both P < 0.001, indicating that the expert opinions were relatively coordinated and concentrated. The expert opinions and suggestions ensured the quality of the items.
The validity includes content validity, structural validity, and calibration validity. Content validity is established when each item’s content validity index (I-CVI) exceeds 0.78 and the overall scale’s content validity index (S-CVI) surpasses 0.9050. In this study, the scale’s S-CVI was 0.967, with individual item I-CVIs ranging from 0.833 to 1.000, indicating strong content validity and confirming that the scale accurately reflects the intended constructs. Currently, self-advocacy evaluation tools have been primarily developed for female cancer patients51, AIDS patients52, and brain injury patients15, etc. Due to significant differences in evaluation criteria and content, this study did not assess criterion validity. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used to evaluate structural validity. After two rounds of EFA, the cumulative variance explained by the five common factors was 68.285%, with all items having factor loadings exceeding 0.4. which is considered to demonstrate good structural validity53. The final dimensions and item attributions were consistent with theoretical hypotheses. The CFA model fit was satisfactory, further supporting the scale’s validity54. Additionally, acceptable average variance extracted (AVE) and composite reliability (CR) values, along with AVE square roots greater than inter-construct correlations, indicate strong convergent and discriminant validity46.
Reliability includes internal consistency and stability50. Cronbach’s α coefficient and split-half reliability are used to measure internal consistency, with a Cronbach’s α between 0.8 and 0.9 indicating high internal consistency. Split-half reliability should generally exceed 0.7. Retest reliability measures stability, with values closer to 1 indicating higher stability. A retest reliability above 0.7 signifies adequate stability55. In this study, the total scale’s Cronbach’s α was 0.936, and the Cronbach’s α for the five dimensions ranged from 0.816 to 0.898, demonstrating strong internal consistency. The total scale’s split-half reliability was 0.874, and the split-half reliability for each dimension ranged from 0.756 to 0.874, all exceeding 0.7. Two weeks later, the retest reliability for 30 stroke patients was 0.885, with retest reliabilities for all dimensions ranging from 0.755 to 0.853. These results confirm the scale’s excellent internal consistency and stability55.
Finally, the scale consists of 5 dimensions and 24 items, with a moderate number of items and an estimated completion time of 11 min. The content is clear, easy to understandable, and user-friendly, ensuring strong operational feasibility and high practicality. The self-advocacy scale for stroke patients developed in this study can provide a more practical assessment tool and theoretical basis for promoting the study of self-advocacy in stroke patients in China.
Limitations
Our research also has some limitations. First, we only recruited participants who had no cognitive or communication issues so that more information could be gathered more quickly and easily in a shorter amount of time. Since the participants had a disability score of greater than 40, the results might not apply to those who have had more severe strokes. Second, no other relevant scales were tested in this study due to the large differences in the study population, assessment indicators, and content. Third, this study only investigated stroke patients in two tertiary hospitals. Future research could conduct multi-center investigations to verify the applicability of the scale.
Conclusion
This study developed a self-advocacy scale for stroke patients following a standardized scale development process. The scale comprises 5 dimensions and 24 items, with all indicators meeting the criteria for scale development, demonstrating good scientific and practical value. This scale can serve as an effective assessment tool for evaluating self-advocacy in stroke patients, aiding in the exploration of the current status of self-advocacy and related influencing factors among this population. It provides a reliable basis for formulating targeted, individualized, and precise self-advocacy intervention measures.
Data availability
The data supporting the findings of this study are available on request from the corresponding author.
References
Feigin, V., Stark, B., Johnson, C. & Roth, G. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. 20 (10), 795–820 (2021).
Brief report on stroke center in China. Chin. J. Cerebrovasc. Dis. 21 (08), 565–576 (2022).
Wang, W. et al. Independent predictors of medication adherence among Singaporean patients following an ischemic stroke or transient ischemic attack. J. Clin. Nurs. 26 (23–24), 5016–5024 (2017).
Li, Y. et al. Effects of self-management intervention programs based on the health belief model and planned behavior theory on self-management behavior and quality of life in middle-aged stroke patients. Evid. Based Compl. Alt. 2021, 8911143 (2021).
Brashers, D. E., Basinger, E. D., Rintamaki, L. S., Caughlin, J. P. & Para, M. Taking control: the efficacy and durability of a Peer-Led uncertainty management intervention for people recently diagnosed with HIV. Health Commun. 32 (1), 11–21 (2017).
Hagan, T., Rosenzweig, M., Zorn, K. K., Londen, G. & Donovan, H. Perspectives on Self-Advocacy: comparing perceived uses, benefits, and drawbacks among survivors and providers. Oncol. Nurs. Forum 44, 52–59 (2017).
Ciccone, M. M. et al. Feasibility and effectiveness of a disease and care management model in the primary health care system for patients with heart failure and diabetes (Project Leonardo). Vasc. Health Risk Man 6, 297–305 (2010).
Aujoulat, I., D’Hoore, W. & Deccache, A. Patient empowerment in theory and practice: polysemy or cacophony? Patient Educ. Couns. 66 (1), 13–20 (2007).
Pickett, S. et al. Consumer empowerment and Self-Advocacy outcomes in a randomized study of Peer-Led education. Commun. Ment. HlT J. 48 (4), 420–430 (2012).
Schmidt, E. K., Faieta, J. & Tanner, K. Scoping review of Self-Advocacy education interventions to improve care. OTJR-Occup. Part Heal. 40 (1), 50–56 (2020).
Hawley, L. et al. Enhancing Self-Advocacy after traumatic brain injury: a randomized controlled trial. J. Head Trauma Rehab. 37 (2), 114–124 (2022).
Daniels, J. et al. Building self-advocacy in HIV care: the use of role-play to examine healthcare access for HIV-positive MSM in rural South Africa. Glob. Health Promot. 28 (3), 32–40 (2021).
Thomas, T. H. et al. I was never one of those people who just jumped right in for me: patient perspectives on self-advocacy training for women with advanced cancer. Support Care Cancer 31 (1), 96 (2023).
Tilley, E., Strnadova, I., Danker, J., Walmsley, J. & Loblinzk, J. The impact of self-advocacy organizations on the subjective well-being of people with intellectual disabilities: a systematic review of the literature. J. Appl. Res. Intellect. 33 (6), 1151–1165 (2020).
Hawley, L., Gerber, D., Pretz, C., Morey, C. & Whiteneck, G. Initial validation of personal self-advocacy measures for individuals with acquired brain injury. Rehabil. Psychol. 61 (3), 308–316 (2016).
Novinmehr, N. et al. Older adults’ self-advocacy in patient safety: a cross-sectional study. Br. J. Nurs. 28 (16), 1076–1084 (2019).
Feng, L., Tan, L. H. & Yu, H. D. Chinese version of female Self-Advocacy in Cancer survivorship and its reliability and validity test. Chin. Nurs. Res. 35 (03), 377–381 (2021).
He, L. et al. Status and influencing factors of self-advocacy in breast cancer patients with chemotherapy. Chin. J. Nurs. 58 (07), 788–793 (2023).
von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. LANCET 370 (9596), 1453–1457 (2007).
Tofthagen, R. & Fagerstrom, L. M. Rodgers’ evolutionary concept analysis–a valid method for developing knowledge in nursing science. Scand. J. Caring Sci. 24 (1), 21–31 (2010).
Zhao, Z. et al. Concept of self-advocacy in the patients with chronic diseases:an evolutionary concept analysis. Mod. Clin. Nurs. 23 (12), 73–80 (2024).
Graneheim, U. H., Lindgren, B. M. & Lundman, B. Methodological challenges in qualitative content analysis: a discussion paper. Nurs. Educ. Today 56, 29–34 (2017).
Charmaz, K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis (SAGE Publication Inc, 2006).
Toronto, C. Considerations when conducting e-Delphi research: a case study. Nurse Res. 25 (1), 10–15 (2017).
Almanasreh, E., Moles, R. & Chen, T. F. Evaluation of methods used for estimating content validity. Res. Soc. Admin. Pharm. 15 (2), 214–221 (2019).
Nagata, C., Ido, M., Shimizu, H., Misao, A. & Matsuura, H. Choice of response scale for health measurement: comparison of 4, 5, and 7-point scales and visual analog scale. J. Epidemiol. 6 (4), 192–197 (1996).
Preston, C. C. & Colman, A. M. Optimal number of response categories in rating scales: reliability, validity, discriminating power, and respondent preferences. Acta Psychol. 104 (1), 1–15 (2000).
Palese, A. et al. Nursing activity score for estimating nursing care need in intensive care units: findings from a face and content validity study. J. Nurs. Manage. 24 (4), 549–559 (2016).
Chinese Academy Of Neurology. Classification of cerebrovascular diseases in China 2015. Chin. J. Neurol. 50 (3), 168–171 (2017).
Jarzebska, E. Validity of the token test as a selective test in aphasia patients and in brain damaged patients without aphasia. Pol. Merkur Lekarski 22 (129), 196–199 (2007).
Leung, S. O., Chan, C. C. & Shah, S. Development of a Chinese version of the modified Barthel Index– validity and reliability. Clin. Rehabil.. 21 (10), 912–922 (2007).
Gao, M. Y., Yang, M., Kuang, W. H. & Qiu, P. Y. Factors and validity analysis of Mini-Mental state examination in Chinese elderly people. Beijing Da Xue Xue Bao Yi Xue Ban 47 (3), 443–449 (2015).
Sapnas, K. G. & Zeller, R. A. Minimizing sample size when using exploratory factor analysis for measurement. J. Nurs. Meas. 10 (2), 135–154 (2002).
Costello, A. B. & Osborne, J. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 10, 1–9 (2005).
Comrey, A. L. & Lee, H. B. A First Course in Factor Analysis (Psychology Press, 1992).
Ferketich, S. Focus on psychometrics. Aspects of item analysis. Res. Nurs. Health 14 (2), 165–168 (1991).
Yang, Z., Wang, H. & Wang, A. Psychometric evaluation of the Chinese version of advance care planning self-efficacy scale among clinical nurses. BMC Palliat. Care 21 (1), 175 (2022).
Gorsuch, R. L. Exploratory factor analysis: its role in item analysis. J. Pers. Assess. 68 (3), 532–560 (1997).
Matsumura, K., Hamazaki, K., Tsuchida, A., Kasamatsu, H. & Inadera, H. Factor structure of the Edinburgh postnatal depression scale in the Japan environment and children’s study. Sci. Rep.-UK 10 (1), 11647 (2020).
Tobias, S. & Carlson, J. E. Brief report: bartlett’s test of sphericity and chance findings in factor analysis. Multivar. Behav. Res. 4 (3), 375–377 (1969).
Schreiber, J. B. Issues and recommendations for exploratory factor analysis and principal component analysis. Res. Soc. Admin. Pharm. 17 (5), 1004–1011 (2021).
Alavi, M. et al. Exploratory factor analysis and principal component analysis in clinical studies: which one should you use? J. Adv. Nurs. 76 (8), 1886–1889 (2020).
Anthoine Bataille, E., Moret, L., Regnault, A., Sébille, V. & Hardouin, J. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Out. 12, 176 (2014).
Shi, D., DiStefano, C., Maydeu-Olivares, A. & Lee, T. Evaluating SEM model fit with small degrees of freedom. Multivar. Behav. Res. 57 (2–3), 179–207 (2022).
Hooper, D., Coughlan, J. & Mullen, M. Structural equation modelling: guidelines for determining model fit structural equation modelling: guidelines for determining model fit. Electron. J. Bus. Res. Methods 6 (1), 53–60 (2008).
Fornell, C. & Larcker, D. Evaluating structural equation models with unobservable variable sand measurement error. J. Mark. Res. 18 (1), 39–50 (1981).
Tavakol, M. & Dennick, R. Making sense of cronbach’s alpha. Int. J. Med. Educ. 2, 53–55 (2011).
Frost, M. H., Reeve, B. B., Liepa, A. M., Stauffer, J. W. & Hays, R. D. What is sufficient evidence for the reliability and validity of patient-reported outcome measures? Value Health 10 (Suppl 2), S94–S105 (2007).
Thomas, T. H., Donovan, H. S., Rosenzweig, M. Q., Bender, C. M. & Schenker, Y. A conceptual framework of Self-advocacy in women with Cancer. Adv. Nurs. Sci. 44 (1), E1–E13 (2021).
DeVellis, R. F. Scale Development: Theory and Applications 3 (eds Xi, Z. E. & Du, Y.) (Chongqing University, 2016).
Hagan, T. L., Cohen, S., Stone, C. & Donovan, H. Theoretical to tangible: creating a measure of Self-Advocacy for female Cancer survivors. J. Nurs. Meas. 24 (3), 428–441 (2016).
Brashers, D. E., Haas, S. M. & Neidig, J. L. The patient self-advocacy scale: measuring patient involvement in health care decision-making interactions. Health Commun. 11 (2), 97–121 (1999).
Izquierdo, I., Olea, J. & Abad, F. J. Exploratory factor analysis in validation studies: uses and recommendations. Psicothema 26 (3), 395–400 (2014).
Wen, Z. L., Tang, D. D. & Gu, H. L. General simulation comparison between two-factor and higher-order factor models in a predictive perspective. Acta Psychol. Sin. 51 (3), 119–127 (2019).
Furr, R. M. Psychometrics: An Introduction 3 (SAGE, 2018).
Acknowledgements
We would like to express our appreciation to all stroke patients and 18 experts who participated in this survey.
Funding
This study was funded by the National Natural Science Foundation of China (72174184).
Author information
Authors and Affiliations
Contributions
Conceptualization, ZZX, and ZZX*; methodology, ZZX, CJ*, ZCH, and WSS; formal analysis, ZZX, WXX, and LBL; investigation, ZZX, LBL, WXX, and JH; writing—original draft preparation, ZZX; writing—review and editing, ZZX, CJ*, WSS, QYJ, MYX, and ZCH; supervision, CJ*, LBL, QYJ and ZZX*; project administration, ZZX*. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
A full compliance with ethical guidelines and regulations was observed in all methods used in this study. The Zhengzhou University Ethics Committee gave its approval to this study, and the subjects gave their informed consent before their data was collected.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhao, Z., Chen, J., Lin, B. et al. Development and psychometric test of self-advocacy scale for patients with stroke. Sci Rep 15, 27247 (2025). https://doi.org/10.1038/s41598-025-08109-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-08109-9
