
Abstract
This study investigated the association between serum chloride levels and mortality risk in critically ill patients with sepsis. This retrospective cohort study utilized data from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database. Patients were stratified into four groups based on serum chloride quartiles. The primary outcome was 365-day mortality, while secondary outcomes included 30-day and 90-day mortality. Kaplan–Meier curves were constructed to compare survival probabilities across serum chloride quartiles. Multivariable Cox proportional hazards regression and restricted cubic spline regression analyses were employed to assess the relationship between serum chloride and mortality in sepsis patients. Subgroup and sensitivity analyses were also performed to validate the findings. A total of 17,743 patients (58.26% male) were included in the study. Kaplan–Meier survival curves revealed that sepsis patients in the lowest serum chloride quartile exhibited the highest mortality (log-rank P < 0.001). Multivariable Cox regression analysis demonstrated that serum chloride was independently associated with a decreased risk of 365-day mortality (HR 0.95, 95% CI 0.94–0.97). Compared with patients in the lowest quartile, those in the highest quartile of serum chloride had significantly lower 365-day mortality (HR 0.66, 95% CI 0.58–0.75), similar trends were observed for 30-day and 90-day mortality. Restricted cubic spline regression modeling indicated a non-linear relationship between serum chloride and mortality risk, with a threshold effect identified at 105 mmol/L (P for non-linearity < 0.05). Subgroup analyses further revealed an interaction between acute kidney injury and mortality in sepsis patients. Sensitivity analysis confirmed the stability of the results. Our study demonstrated an L-shaped association between serum chloride levels and 365-day mortality in sepsis patients, with higher serum chloride levels corresponding to a lower mortality risk. However, abnormal chloride levels are often secondary to disease severity, emphasizing the need for targeted interventions addressing the underlying pathology rather than chloride levels alone.
Similar content being viewed by others
Introduction
Sepsis is characterized by a dysregulated host response to infection and represents not only a clinical syndrome but also a significant public health challenge1. This condition progresses rapidly, with complex pathophysiology often leading to severe organ dysfunction and, in many cases, premature death2. Recent studies have shown that in 2017, sepsis-related mortality reached 11 million deaths globally, accounting for 19.7% of all global deaths3. In addition to its high mortality rate, sepsis imposes a substantial economic burden. In the United States, the average cost per septic patient is estimated at US$22,100, with the total annual cost of sepsis reaching US$16.7 billion4. More than half of sepsis patients require intensive care unit (ICU) admission5. Despite advancements in intensive care and the establishment of evidence-based management guidelines, sepsis remains a leading cause of morbidity and mortality in ICUs6,7. The complex pathophysiology of sepsis has led to the proposal of a variety of biomarkers involving multiple inflammatory mediators. These include the peripheral blood platelet-to-lymphocyte ratio (PLR), C-reactive protein, and procalcitonin8,9,10. Additionally, coagulation, complement activation, contact system activation, and apoptosis are all implicated in the sepsis process, with corresponding biomarkers proposed for each11,12,13. Other markers, such as presepsin, prognostic nutritional index (PNI), and neutrophil-to-lymphocyte ratio (NLR), have also been shown to correlate with the prognosis of inflammation-related disorders14,15,16. These biomarkers can serve as useful adjuncts for clinicians when additional information is needed to optimize patient care at the bedside17. Although numerous biomarkers and scoring systems are available for assessing the prognosis of sepsis, searching for more reliable and precise prognostic indicators remains an important research direction.
Serum chloride is the most abundant anion in the extracellular fluid of the human body and plays a crucial role in maintaining electrolyte balance and osmotic pressure. It is involved not only in regulating ion balance between the intracellular and extracellular environments but also in neuromuscular conduction, acid–base balance, and the activity of various enzymes18. Abnormalities in serum chloride levels are associated with a variety of disease states, including cardiac, renal, gastrointestinal, and metabolic disorders19,20,21,22. For instance, in cardiac diseases, serum chloride levels are correlated with the severity of heart failure and all-cause mortality23. In gastrointestinal diseases, serum chloride changes may be linked to pancreatitis and intestinal absorption function24,25. Additionally, chloride channels are strongly associated with extracellular inflammation, which is central to the pathophysiology of sepsis26. Previous studies have shown that hyperchloremia is associated with in-hospital mortality in sepsis patients, while hypochloremia is strongly associated with 28-day mortality in patients with septic shock admitted to the emergency department27,28. However, the relationship between serum chloride levels at the onset of sepsis and short- and long-term prognosis remains poorly defined.
This study aims to investigate the relationship between serum chloride levels in patients with sepsis and all-cause mortality, thereby providing valuable insights into the short- and long-term prognosis of sepsis survivors. These findings may serve as a basis for developing strategies to improve survival and recovery in this patient population.
Methods
Data source and population
The data for this study were extracted from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database, a large, openly accessible, and meticulously curated critical care database29. Developed at the Laboratory of Computer Science at the Massachusetts Institute of Technology (MIT), MIMIC-IV is designed to facilitate research in critical care medicine by providing deidentified electronic health record (EHR) data for ICU patients. One of the authors of this study, Zhichao Zhao, has passed the training exam to access the MIMIC database (Record ID: 64701219). The use of the MIMIC database for research purposes has been approved by the Committee on the Use of Human Subjects (COUHES) at MIT, and no additional ethical approval was required for this study.
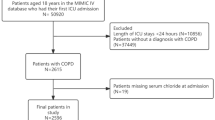
Patients who met the diagnostic criteria for sepsis 3.0 and had an increase of ≥ 2 points in Sequential Organ Failure Assessment (SOFA) score compared to baseline values were enrolled in this study2. The inclusion criteria were as follows: (a) a confirmed diagnosis of sepsis; and (b) first admission to the ICU. The exclusion criteria included: (a) ICU admission duration of less than 24 h; and (b) missing data on serum chloride or other covariates. Ultimately, a total of 17,743 critically ill patients with sepsis were included in our study (Fig. 1).

Flowchart of our sepsis patients.
Selection of covariates
The selection of covariates in our study was guided by prior literature, theoretical considerations, and available data in the MIMIC-IV database. The covariates included the following categories: (1) Demographic characteristics: age, gender, and weight; (2) Laboratory parameters: white blood cell (WBC) count, red blood cell (RBC) count, platelet count, red blood cell distribution width (RDW), sodium, potassium, glucose, anion gap, blood urea nitrogen, bicarbonate, and creatinine levels; (3) Coagulation indices: prothrombin time (PT) and partial thromboplastin time (PTT); (4) Organ dysfunction scores: SOFA score, Acute Physiology Score III (APS III), Simplified Acute Physiology Score II (SAPS II), Oxford Acute Severity of Illness Score (OASIS), and acute kidney injury (AKI) status; (5) Hemodynamic and respiratory variables: heart rate, respiratory rate, systolic blood pressure (SBP), diastolic blood pressure (DBP), mean blood pressure (MBP), and transcutaneous arterial oxygen saturation (SpO₂); (6) Comorbidities: hypertension, diabetes mellitus (DM), atrial fibrillation, heart failure, myocardial infarction, malignant tumors, stroke, chronic kidney disease (CKD), and chronic obstructive pulmonary disease (COPD); (7) Supportive therapies: mechanical ventilation, input amount, and continuous renal replacement therapy (CRRT); (8) Medication: diuretic use.
To handle the missing values, we first excluded variables with missing rates exceeding 20%. Then, among the remaining participants, we removed those who still had missing values. At the same time, to reduce the errors caused by randomly deleting missing values, we employed two imputation methods for missing values: random forest imputation and mean imputation, to verify the stability of our results.
Independent and dependent variables
The main independent variable in our study was the serum chloride level measured on the first day of ICU admission. The primary dependent variable was 365-day all-cause mortality among sepsis patients, secondary dependent variables included 30-day and 90-day mortality.
Statistical analysis
Descriptive statistics were used to summarize the baseline characteristics of the study population. Comparisons of continuous variables were performed using the Student’s t-test or the Mann–Whitney U test, depending on the data distribution, while comparisons of categorical variables were conducted using the chi-square test or Fisher’s exact test, as appropriate. Kaplan–Meier survival curves were constructed to illustrate survival probabilities across different serum chloride quartiles, with comparisons made using the log-rank test. The relationship between serum chloride levels and mortality was assessed using three multivariate Cox proportional hazards regression models. Model 1 was unadjusted; Model 2 was adjusted for age, gender, and body weight; and Model 3 included adjustments for all variables associated with prognosis. Restricted cubic spline (RCS) analyses were performed to explore potential non-linear relationships between serum chloride levels and the risk of death. Subgroup analyses and interaction tests were also conducted to further investigate the association between serum chloride and mortality in critically ill sepsis patients across different populations. Finally, three sensitivity analyses were performed to validate the robustness of the association between serum chloride and mortality risk. These included: (1) excluding patients with malignancies, and (2) imputing missing values using two methods-Random Forest imputation and mean value imputation.
All statistical analyses were performed using R software (version 4.2.1). The following packages and functions were used: “tableone”, “survival”, “tidyverse”, “missForest”, and “survminer”. All statistical tests were two-tailed, and a P value of less than 0.05 was considered statistically significant.
Results
Baseline characteristics
Among the 17,743 sepsis patients, the 365-day mortality rate was 32.5%, with a mean age at follow-up of 66.49 years; 58.26% of the patients were male (Table 1). Significant differences were observed between survivors and non-survivors across several variables. Non-survivors were older, had a higher proportion of females, and exhibited higher WBC, platelet, RDW, and serum phosphorus levels. Additionally, non-survivors had higher blood glucose levels, anion gap, PT, PTT, blood urea nitrogen, and creatinine levels, while having lower body weight, RBC, sodium, chloride, input amount, and bicarbonate levels. Higher disease severity scores (SOFA, APS III, SAPS II, and OASIS) and the presence of comorbidities such as hypertension, type 2 DM, CKD, and heart failure were more common in the non-survivor group. Finally, the use of CRRT and mechanical ventilation was significantly higher among non-survivors.
Table 2 presents significant differences in demographic and clinical parameters across participants with varying serum chloride quartiles. Patients in the highest serum chloride quartile were older and had a higher proportion of males. Conversely, patients in the lowest serum chloride quartile had the highest body weight. Hematological parameters, including WBC, RBC, platelet, RDW, sodium, potassium, input amount, and calcium, exhibited varying degrees of variability across quartiles. Blood glucose levels, anion gap, and bicarbonate levels increased with decreasing serum chloride levels. PT and PTT were longer in lower quartiles. Renal function, organ dysfunction scores (e.g., SOFA), and heart rate decreased with increasing serum chloride levels. The highest serum chloride quartile (Q4) was associated with the shortest length of stay and lowest mortality. Additionally, patients in Q4 used diuretics more frequently than those in the lowest quartile (Q1).
Association between serum chloride and mortality in sepsis patients
The Kaplan–Meier survival curves demonstrate the relationship between serum chloride quartiles and survival probability among patients with sepsis (Fig. 2). Patients in the higher chloride quartiles (Q3 and Q4) exhibited significantly higher survival probabilities compared to those in the lower quartiles (Q1 and Q2). The log-rank test confirmed that the differences in survival probabilities across quartiles were statistically significant (log-rank P < 0.001).

Kaplan–Meier survival analysis curves for mortality (A: 30-day mortality, B: 90-day mortality, and C: 365-day mortality).
Multivariate Cox regression analyses were conducted to examine the relationship between serum chloride levels and mortality in patients with sepsis (Table 3). In the unadjusted model (Model 1), each 1 mmol/L increase in serum chloride was associated with a 3% reduction in the risk of 365-day mortality (HR 0.97, 95% CI 0.96–0.97). In the fully adjusted model (Model 3), which accounted for a range of clinical and laboratory variables, a robust inverse relationship was confirmed (HR 0.95, 95% CI 0.94–0.97). When participants were stratified by serum chloride quartiles, the fully adjusted model revealed that patients in the highest quartile (Q4) had a 34% lower risk of 365-day mortality compared to those in the lowest quartile (Q1) (HR 0.66, 95% CI 0.58–0.75). The effect on mortality varied significantly across serum chloride quartiles (P for trend < 0.05). Similar trends were observed for 30-day and 90-day mortality.
Non-linear association
RCS plots were used to assess the non-linear relationship between serum chloride levels and mortality hazard ratios in patients with sepsis (Fig. 3). The RCS analysis revealed a significant non-linear relationship, with a decrease in 365-day mortality risk observed over a specific threshold range as serum chloride levels increased (P for non-linearity < 0.05). In our study, the median serum chloride level was used as the threshold value, which was 105 mmol/L. For patients with sepsis whose serum chloride levels exceeded 105 mmol/L, the risk of 365-day death decreased with increasing serum chloride levels, although this decrease was not statistically significant. Similar trends were observed for 30-day and 90-day mortality.

Restricted cubic spline curve for the chloride hazard ratio (A: 30-day mortality, B: 90-day mortality, and C: 365-day mortality).
Subgroup analyses
Subgroup analyses of serum chloride levels in patients with sepsis revealed a consistent reduction in 365-day mortality risk across various patient categories (Fig. 4). In all subgroups, higher serum chloride levels were associated with a reduced risk of 365-day mortality among sepsis patients. Similar trends were observed for 30-day and 90-day mortality (Supplementary Figs. 1 and 2). Notably, the association between serum chloride and 365-day mortality risk was more pronounced in patients without AKI and those receiving mechanical ventilation (P for interaction < 0.05).

Subgroup analysis of serum chloride on the effect of 365-day mortality in the sepsis population.
Sensitivity analysis
To further validate the association between serum chloride levels and 365-day mortality, we conducted sensitivity analyses by excluding patients with confirmed malignancies, given their potentially higher risk of death (Table 4). The results of these sensitivity analyses were consistent with our primary findings, demonstrating a significant inverse relationship between serum chloride levels and the risk of 365-day mortality. Specifically, higher serum chloride levels were associated with a lower risk of 365-day death, even after adjusting for potential covariates (HR 0.97, 95% CI 0.97–0.98). Analysis by chloride quartiles further confirmed these findings, with each successive quartile showing a stepwise reduction in 365-day mortality risk compared to the lowest quartile (Q1). Similar trends were observed for 30-day and 90-day mortality.
Additionally, we used two methods of imputation for missing values to further assess the reliability and robustness of our results. Data interpolated using these methods also confirmed the negative correlation between serum chloride levels and mortality risk in critically ill patients with sepsis (Supplementary Tables 1 and 2).
Discussion
This study leveraged the comprehensive MIMIC-IV database to examine the relationship between serum chloride levels and 365-day mortality in patients with sepsis. Our findings indicate that higher serum chloride levels are associated with a lower risk of death, even after accounting for other factors that may influence mortality in critically ill sepsis patients. RCS analyses further revealed that this association is nonlinear. Additionally, subgroup analyses demonstrated that the presence of AKI modifies this inverse relationship.
Serum chloride is a vital electrolyte that plays a key role in maintaining acid–base balance and cellular function. Over the past few years, several studies have uncovered associations between serum chloride levels and the onset and progression of various diseases. For instance, a prospective cohort study of patients with stage 3 and 4 CKD from a single medical center renal clinic demonstrated that serum chloride levels were associated with mortality in CKD patients30. Specifically, low serum chloride levels were linked to a higher risk of death, likely due to the kidneys’ critical role in regulating chloride concentrations. In cardiovascular medicine, serum chloride levels also hold significant prognostic value. A study of 870 patients with heart failure, with a mean follow-up of 1.8 years, revealed that low serum chloride levels were associated with increased mortality and cardiovascular events, this association was particularly pronounced in patients with acute heart failure, where reduced serum chloride levels were strongly correlated with a poor prognosis31,32. Similarly, in the field of pulmonary medicine, serum chloride levels have been implicated in COPD. Research has identified an L-shaped relationship between serum chloride levels and all-cause mortality in COPD patients, suggesting that both low and high serum chloride levels may increase the risk of death33. In critical care, the prognostic significance of serum chloride levels has been emphasized. For example, among patients with AKI, low serum chloride levels have been associated with increased in-hospital mortality34. These findings align with our results, which demonstrate an L-shaped association between serum chloride concentrations and mortality in sepsis patients.
Although our study did not directly explore the mechanisms underlying the association between higher serum chloride and decreased mortality risk in critically ill sepsis patients, we speculate that this inverse relationship may be attributable to several physiological mechanisms. Firstly, sepsis patients frequently experience metabolic acidosis, and changes in serum chloride levels can influence blood pH, thereby affecting cellular function and patient survival35,36. As the predominant extracellular anion, chloride is essential for maintaining osmotic balance and transmembrane electrical gradients. In the context of sepsis, dysregulation of chloride homeostasis has been linked to alterations in vascular tone, cellular oxygen consumption, and acid–base status which can impact patient prognosis37,38,39.
In our study, RCS analyses further confirmed the existence of a non-linear relationship between serum chloride levels and mortality risk, suggesting that an optimal range of chloride levels may be associated with the lowest risk of death. Additionally, subgroup analyses revealed particularly noteworthy results in patients with AKI, where higher chloride levels exhibited a more pronounced protective effect. This finding may be related to the increased susceptibility of sepsis patients to comorbid conditions. Specifically, AKI can predispose individuals to septic episodes through its influence on the innate immune system, which in turn may exacerbate the severity of AKI34,40. Therefore, higher chloride levels may offer greater protection in patients with concurrent AKI. Our results suggest that maintaining chloride levels within an optimal range may be particularly important in this susceptible population. It should be emphasized, however, that abnormal chloride levels (e.g., hypochlorhydria) are often secondary to the pathophysiologic process of sepsis and may be closely related to factors such as renal insufficiency and acidosis41,42. Therefore, clinical interventions should prioritize targeting the underlying etiology of the chloride imbalance (e.g., correcting shock, improving renal perfusion, optimizing fluid therapy, etc.) rather than pursuing mechanical adjustments in chloride levels alone. In addition, monitoring and maintaining chloride in a reasonable range (e.g., > 105 mmol/L) while actively treating the primary pathology may provide additional benefits in improving patient prognosis.
However, our study has several limitations that warrant consideration. First, as a retrospective analysis, our study is subject to inherent biases and confounders that cannot be fully adjusted for in observational data. For example, we were unable to account for variables such as pregnancy, intermittent hemodialysis, and whether patients received chronic or acute dialysis due to missing data. Additionally, we did not include the APACHE III and APACHE II scores, which are important metrics commonly used to assess the severity of illness in critically ill patients. These omissions may have influenced our results. Second, although the MIMIC-IV database is a rich resource, its data were derived from a single center, which may limit the generalizability of our findings to broader populations. Furthermore, the timing and frequency of serum chloride measurements varied across patients, which may introduce variability in our analyses and affect the robustness of our conclusions.
Conclusion
The present study demonstrated an L-shaped association between serum chloride levels and 365-day mortality in patients with sepsis, suggesting that higher chloride levels may have a protective effect. However, abnormal chloride levels are more a reflection of disease severity and complications. Therefore, clinical management should focus on the underlying treatment of sepsis, while using chloride as an auxiliary indicator for dynamic monitoring to optimize the overall therapeutic strategy.
Data availability
The datasets generated and analyzed during the current study are available in the MIMIC-IV database. The link is https://physionet.org/content/mimiciv/2.2/.
Abbreviations
- MIMIC-IV:
-
Medical Information Mart for Intensive Care-IV
- ICU:
-
Intensive care unit
- AKI:
-
Acute kidney injury
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- RCS:
-
Restricted cubic spline
- WBC:
-
White blood cell
- RBC:
-
Red blood cell
- RDW:
-
Red cell distribution width
- PT:
-
Prothrombin time
- PTT:
-
Partial thromboplastin time
- SOFA:
-
Sequential Organ Failure Assessment
- APS III:
-
Acute physiology score III
- SAPS II:
-
Simplified acute physiology score II
- OASIS:
-
Oxford acute severity of illness score
- SpO2 :
-
Transcutaneous arterial oxygen saturation
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- MBP:
-
Mean blood pressure
- CRRT:
-
Continuous renal replacement therapy
- COPD:
-
Chronic obstructive pulmonary disease
- DM:
-
Diabetes mellitus
- CKD:
-
Chronic kidney disease
- PHI:
-
Personal health information
- COUHES:
-
Committee on the Use of Human Subjects
- MIT:
-
Massachusetts Institute of Technology
- EHR:
-
Electronic health record
References
Fleischmann, C. et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am. J. Respir. Crit. Care Med. 193(3), 259–272 (2016).
Singer, M. et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315(8), 801–810 (2016).
Rudd, K. E. et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 395(10219), 200–211 (2020).
Angus, D. C. et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 29(7), 1303–1310 (2001).
Rhee, C. et al. Incidence and trends of sepsis in US hospitals using clinical versus claims data, 2009–2014. JAMA 318(13), 1241–1249 (2017).
Driessen, R. G. H. et al. Early ICU-mortality in sepsis: Causes, influencing factors and variability in clinical judgement—a retrospective cohort study. Infect. Dis. (Lond.) 53(1), 61–68 (2021).
Wang, D. et al. A Machine learning model for accurate prediction of sepsis in ICU patients. Front. Public Health 9, 754348 (2021).
Marshall, J. C. et al. Measures, markers, and mediators: toward a staging system for clinical sepsis. A report of the Fifth Toronto Sepsis Roundtable, Toronto, Ontario, Canada, October 25–26, 2000. Crit. Care. Med. 31(5), 1560–1567 (2003).
Pierrakos, C. & Vincent, J. L. Sepsis biomarkers: A review. Crit. Care 14(1), R15 (2010).
Wang, G. et al. Prognostic value of platelet to lymphocyte ratio in sepsis: A systematic review and meta-analysis. Biomed. Res. Int 2022, 9056363 (2022).
Pettila, V., Pentti, J., Pettila, M., Takkunen, O. & Jousela, I. Predictive value of antithrombin III and serum C-reactive protein concentration in critically ill patients with suspected sepsis. Crit. Care Med. 30(2), 271–275 (2002).
Orfanos, S. E. et al. Angiopoietin-2 is increased in severe sepsis: Correlation with inflammatory mediators. Crit. Care Med. 35(1), 199–206 (2007).
Williams, J. P. et al. Nociceptin and urotensin-II concentrations in critically ill patients with sepsis. Br. J. Anaesth. 100(6), 810–814 (2008).
Shimoyama, Y., Umegaki, O., Kadono, N. & Minami, T. Presepsin and prognostic nutritional index are predictors of septic acute kidney injury, renal replacement therapy initiation in sepsis patients, and prognosis in septic acute kidney injury patients: A pilot study. BMC Nephrol. 22(1), 219 (2021).
Chen, J. J. et al. Neutrophil-to-lymphocyte ratio is a marker for acute kidney injury progression and mortality in critically ill populations: A population-based, multi-institutional study. J. Nephrol. 35(3), 911–920 (2022).
Serban, D. et al. The significance of preoperative neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and systemic inflammatory index (SII) in predicting severity and adverse outcomes in acute calculous cholecystitis. J. Clin. Med. 12(21), 6946 (2023).
Povoa, P. et al. How to use biomarkers of infection or sepsis at the bedside: guide to clinicians. Intensive Care Med. 49(2), 142–153 (2023).
Marunaka, Y. Physiological roles of chloride ions in bodily and cellular functions. J. Physiol. Sci. 73(1), 31 (2023).
Kawada, T. Effect of serum chloride on mortality in hypertensive patients. Hypertension 63(3), e14 (2014).
De Bacquer, D., De Backer, G., De Buyzere, M. & Kornitzer, M. Is low serum chloride level a risk factor for cardiovascular mortality?. J. Cardiovasc. Risk 5(3), 177–184 (1998).
Mao, W. et al. Increase in serum chloride and chloride exposure are associated with acute kidney injury in moderately severe and severe acute pancreatitis patients. Pancreatology 19(1), 136–142 (2019).
Berend, K., van Hulsteijn, L. H. & Gans, R. O. Chloride: the queen of electrolytes?. Eur. J. Intern. Med. 23(3), 203–211 (2012).
Wu, F., Lan, Q. & Yan, L. Prognostic impact of serum chloride concentrations in acute heart failure patients: A systematic review and meta-analysis. Am. J. Emerg. Med. 71, 109–116 (2023).
Ye, B. et al. The impact of normal saline or balanced crystalloid on plasma chloride concentration and acute kidney injury in patients with predicted severe acute pancreatitis: Protocol of a phase II, multicenter, stepped-wedge, cluster-randomized, controlled trial. Front. Med. (Lausanne) 8, 731955 (2021).
Bansal, A. et al. Gastrointestinal complications in acute and chronic pancreatitis. JGH Open 3(6), 450–455 (2019).
Lin, Z. et al. Chloride channel and inflammation-mediated pathogenesis of osteoarthritis. J. Inflamm. Res. 15, 953–964 (2022).
Lee, M. S. et al. Hypochloraemia is associated with 28-day mortality in patients with septic shock: A retrospective analysis of a multicentre prospective registry. Emerg. Med. J. 38(6), 423–429 (2021).
Neyra, J. A. et al. Acute kidney injury in critical illness study G: Association of hyperchloremia with hospital mortality in critically ill septic patients. Crit. Care Med. 43(9), 1938–1944 (2015).
Johnson, A. E. W. et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci. Data 10(1), 1 (2023).
Khatri, M. et al. The association between serum chloride levels and chronic kidney disease progression: A cohort study. BMC Nephrol. 21(1), 165 (2020).
Seo, M. et al. Prognostic significance of serum chloride level in heart failure patients with preserved ejection fraction. ESC Heart Fail. 9(2), 1444–1453 (2022).
Kurashima, S. et al. Trajectory of serum chloride levels during decongestive therapy in acute heart failure. Int. J. Cardiol. 375, 36–43 (2023).
Wang, S. et al. L-shaped association between serum chloride levels with 90-day and 365-day all-cause mortality in critically ill patients with COPD: A retrospective cohort study. Sci. Rep. 14(1), 15900 (2024).
Li, R., Chen, Y., Liang, Q., Zhou, S. & An, S. Lower serum chloride concentrations are associated with an increased risk of death in ICU patients with acute kidney injury: An analysis of the MIMIC-IV database. Minerva Anestesiol. 89(3), 166–174 (2023).
Suetrong, B. & Walley, K. R. Lactic acidosis in sepsis: It’s not all anaerobicimplications for diagnosis and management. Chest 149(1), 252–261 (2016).
Maciel, A. T., Noritomi, D. T. & Park, M. Metabolic acidosis in sepsis. Endocr. Metab. Immune Disord. Drug Targets 10(3), 252–257 (2010).
Petrova, M., Lassanova, M., Tisonova, J. & Liskova, S. Ca(2+)-dependent Cl(-) channels in vascular tone regulation during aging. Int. J. Mol. Sci. 25(10), 5093 (2024).
Eveloff, J., Bayerdorffer, E., Silva, P. & Kinne, R. Sodium-chloride transport in the thick ascending limb of Henle’s loop. Oxygen consumption studies in isolated cells. Pflugers Arch. 389(3), 263–270 (1981).
Havlin, J., Matousovic, K. & Schuck, O. Sodium-chloride difference as a simple parameter for acid-base status assessment. Am. J. Kidney Dis. 69(5), 707–708 (2017).
Doyle, J. F. & Forni, L. G. Acute kidney injury: Short-term and long-term effects. Crit. Care 20(1), 188 (2016).
Oh, H. J. et al. An increased chloride level in hypochloremia is associated with decreased mortality in patients with severe sepsis or septic shock. Sci. Rep. 7(1), 15883 (2017).
Cetin Guvenc, R. et al. Effect of renal function on the prognostic importance of chloride in patients with heart failure. J. Investig Med. 71(4), 339–349 (2023).
Acknowledgements
We acknowledge the support from Yuyao People’s Hospital and the valuable feedback from anonymous reviewers.
Author information
Authors and Affiliations
Contributions
Zhichao Zhao and Fangfang Huang conceived the study design; Jiaqi Shen and Wenqian Lv performed the data analysis; Yabo Huang and Jiale Pan wrote the first draft; Ting Shen provided professional guidance and revised the manuscript. All authors reviewed and agreed on the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The use of the MIMIC database for research purposes has been approved by the Committee on the Use of Human Subjects (COUHES) at the Massachusetts Institute of Technology (MIT), and no additional ethical approval was required for this study. The data used in this study were de-identified, i.e., all personal health information (PHI) was removed or encrypted to protect patient privacy. Therefore, this retrospective analysis did not require informed consent from individual patients.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhao, Z., Huang, F., Shen, J. et al. L-shape association between serum chloride and 365-day mortality in critically ill patients with sepsis based on the MIMIC-IV database. Sci Rep 15, 20391 (2025). https://doi.org/10.1038/s41598-025-08630-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-08630-x
