
Abstract
To explore the correlation between Psychosexual Health development (APDS) and non-suicidal self-injury behaviors (NSSI) in adolescence, and investigate the mediating effects by adult attachment (AAS) and social supports (SSRS) between them. This study employs a missed design with quantitative pretests and tracing post-tests involving 1193 college students majoring in preschool and primary education. The participants are first-year (freshmen) and second-year students (sophmore), primarily women, at a higher vocational college in Shaanxi, utilizing APDS, AAS, SSRS and the NSSI questionnaires to evaluate the positive proportion of NSSI behaviors and obtained the ratio of 12.53% among normal individuals, and using SPSS Pearson relevant to analyse correlation of the variables and to test the mediating effect through Amos SEM equation model and Bootstrap method. Confirmed Psychosexual Health impacts on NSSI behaviors significantly, and the Chained mediating effect of AAS and SSRS between them. APDS can significantly negatively predict NSSI under the mediating effects of AAS and SSRS respectively, and insignificantly effect with the chained mediating effect of AAS and SSRS. Improving individual psychosexual health levels is conducive to developing secure adult attachment and promoting good social supports, with certain enlightening significance for decreasing and preventing NSSI behaviors among adolescents. We discussed future research directions based on our results, and revealed important significance timely intervening those with personality disorders and NSSI behaviors through carrying out psychosexual health education to cultivate their secure adult attachment and good social supports. In the meanwhile, to support individuals with psychological growth and group intervention on NSSI behaviors during adolescence, and put forward schools more effective educational guidance and methods of psychological health, by promoting their psychosexual health to enhance individual personality development and mental health levels. With anticipation to provide more scientific theoretical evidence and practical strategies for early educational guidance and group prevention measures in favor of implementing psychosexual health education to prevent NSSI behaviors timely among children and adolescents on campus.
Similar content being viewed by others


Introduction
Adolescence is a crucial period for establishing sexual morality and normal sexual behaviors in various aspects of social life. Psychosexual health development (APDS) in adolescence positively correlates with mental health1. Psychosexual is an significant component of personality, and refers to the psychological state and psychological process related to sexual characteristics, sexual desire and sexual behavior on the basis of sexual physiology, including as well as marriage and love, interaction with the opposite sex2. Psychosexual health in adolescence is reflected in three aspects: sexual cognition (physiological and sexual knowledge), sexual values (sexual concepts and attitudes), and sexual adaptation (social adaptation, sexual control and self-adaptation)3. Psychosexual health means learning physical and psychological knowledge in the correct ways and possessing positive sexual value and adaptive capacity. Psychosexual development impacts adolescents’ personality traits, personal development, social development, and maturity4. As Freud (1905) noted, “Neurosis is the negative side of Paraphilia”. Psychosexual Health is closely related to psychological problems, parapsychosexuality, sexual disease, and sexual crime, among others5, and adolescents might experience self-denial, uptight and despairing feelings, and even sexual perversion or parasexuality issues. College students’ sexual physiology tends to mature during adolescence. The level of APDS has a decisive impact on the attitude and cognition of sexual health, and the high level is beneficial to the formation of correct values6. The development and maturity of Psychosexual Health are of great significance to teenagers’ interpersonal action, the formation of sexual moral qualities, as well as to the success of love and the happiness of marriage7. The scholars have verified adolescents will possess definite knowledge, skills, attitudes, and values about sex with ensuring health, blessing, and dignity after accepting comprehensive sexual education8. Systematic sexual education is beneficial to students’ Psychosexual Health in adolescence9. The scholars have verified adolescents will possess definite knowledge, skills, attitudes, and values about sex with ensuring health, blessing, and dignity after accepting comprehensive sexual education10.
Non-suicidal self-injury (abbreviated as ‘NSSI’), refers to the action of an individual intentionally and repeatedly self-injury of their own body, with non-suicidal purposes. Relevant data disclosed the incidence of NSSI is increasing year by year among teenagers in China11, and it is the highest in early adolescence, and it decreases in late adolescence and adulthood12. Research shows that the occurrence rate of non-suicidal self-injury (NSSI) in college students is 12.12–15.1%13. The incidence of NSSI among Chinese college students was 16.6%14. Relevant research have confirmed that NSSI behaviors are highly correlated with borderline personality disorder (BPD) or poor personality development, depressive disorder, adverse life events, meaningless feelings of life, low dignity, and relevant factors15. For individuals, NSSI can relieve negative feelings and cognitive states, create a positive state, or solve interpersonal difficulties16,17. However, clinical treatment and intervention are challenging due to the complex characteristics of NSSI. Hence, to understand associated protective factors of adolescents’ NSSI behavior with early prevention, it would have a positive impact on their social functions, interpersonal relationships and future personality development.
Nock regards NSSI as a coping mechanism to manage one’s mood and recognition. In the meantime, communicatively, the communication is handled by NSSI behaviors or affects others to achieve one’s aims18 (Nock,2009). Adult attachments (AAS) is influenced by experience and affects an individual’s future interpersonal interactions19. AAS impacts on college students’ mental health, such as emotional regulation, self-identity, interpersonal relationships, academic achievement, love, and making friends19. Relevant research shows that the childhood trauma of college students, under the mediating effects of AAS, has an essential influence on post-traumatic stress disorder (PTSD) and post-traumatic growth (PTG)20. Compared with secure attachment individuals, insecure attachment is a risk factor for NSSI21. According to The Decay Theory of NSSI, the personality development of individuals in adulthood is relatively stable after adolescence, and secure attachment pattern plays a regulating role in the development of NSSI15. The Psychosexual Health level (APDS) of students is significantly correlated with adult attachment (AAS) in vocational colleges and universities10.
As a protective factor for mental health, the social supports (SSRS) has received high attention from scholars worldwide22. SSRS with universal protective effects is efficient in alleviating individual psychological stress, suppressing negative emotions, providing positive emotional experiences, and promoting mental health23. SSRS is one of the most effective measures dealing with and adjusting difficult and stressful events, which can buffer the adverse effects causing by stress on mental and physical health24. Studies have shown that SSRS have universal gain effects and play an important role in maintaining individual’s physical and mental Health, therefore, SSRS may also be a protective factor for Psychosexual Health (APDS)25. SSRS refers to the series of interpersonal help individuals get from their daily lives26, including visible and objective practical support and emotional support that people experience subjectively. Shuiyuan Xiao also believes that SSRS should include individuals who utilize condition to the support27. No matter what indicators are taken, SSRS is inevitably linked to individuals’ physical and mental health, and relevant research confirmed that SSRS is medium-grade correlative with psychological health28. Shen and Gao proposed that SSRS is one of the vital influential factors in psychological health and brought it into an essential part of psychological education29. The study shows that individuals with a lack of SSRS easily generate NSSI behaviors. Since the end of the nineteenth century, French sociologist Durkheim has pointed out that the loss of social relationships is one of the critical reasons for suicide. SSRS has a general promoting effect on keeping an individual’s physical and mental health and plays an important role, therefore, SSRS may be a protective factor on APDS2.
Psychosexual repression is closely relevant to one’s potential personality, meanwhile, psychosexual Health during adolescence is a noteworthy component and significant sign of psychological health and affects an individual’s psychological health and personality development15. Relevant studies have pointed out that NSSI behaviors are influenced by sociodemographic factors and individual mental health levels, which are difficult to change demographic factors, and it is facilitated to intervene continuously to pay more attention to psychological factors of individuals, in the meantime, BPD is highly correlated with NSSI behaviors occurring, as personality is stable and difficult to intervene directly, therefore,it is in favour of Prevention and effective intervention on adolescent NSSI behaviors to explore the modifiable factors between them30.
Given the above, we find APDS is singnificantly correlated with personality development, and BPD, AAS and SSRS correlate with NSSI. Based on relevant theories1,4,15,19,27,31, we propose the following hypothesis:
Hypothesis 1
APDS correlates with NSSI.
Hypothesis 2
Significant Pairwise Correlations among APDS, AAS and SSRS.
Hypothesis 3
APDS is related to SSRS, with AAS as a mediating effect between them.
Hypothesis 4
Both of AAS and SSRS play a mediating role respectively between APDS and NSSI behavior.
Hypothesis 5
The Chained Mediation by AAS and SSRS plays a effect role in the relationship between APDS and NSSI behavior, and influencing NSSI behavior.
Previous studies on NSSI behaviors have mostly focused on clinical research and patients with comorbidities, however, there are few studies on the general population with relatively NSSI behavior, furthermore, the discrepancy of results varies greatly on the behavioral risk of NSSI behavior among adolescents. Our study will explore the correlation between APDS and NSSI behavior under controlling for demographic variables such as sex, grade etc., and investigate the mediating effects by AAS and SSRS between them, which is of in consideration there are no relevant studies conducting the relationship between APDS and NSSI behavior in adolescence.
In the research, we attempt to explore more factors underlying NSSI behaviors that can be changed or adjusted in adolescence, promoting the level of Psychosexual Health to develop secure AAS and high-quality SSRS through school education and guidance, improving and declining the ratio of NSSI behaviors. Further more, we make efforts to provide a scientific theoretical basis for implementing school Psychosexual education and enhancing group interventions onprevention NSSI behaviors.
Methods
Participants
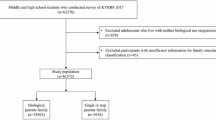
This study employs a missed design with quantitative pretests and tracing post-tests involving 1193 college students majoring in preschool and primary education. The participants are first-year (freshmen) and second-year students (sophmore), primarily women, at a higher vocational college in Shaanxi. We administered the APDS, AAS, SSRS, and the NSSI severity rating scale for clinicians through the “Sojump” online platform. Questionnaires were distributed and collected via web links, QR codes, WeChat, and through administrative classes before the semester began. We took an online survey and evaluated it based on the informed and willingness principle and collected 958 questionnaires. For the research and according to certain conditions, we excluded repetitively and carelessly answered questionnaires (answer time too long or short, with highly similar choices, etc.), and finally obtained valid 774 copies, as the object research for Pre-test. Afterward, we promoted APDS development and collective assistance (AAS and SSRS) through group games and activities. Further, 4 months later, we implemented the real-name measurements and evaluations at the semester’s final test by releasing the APDS scale and NSSI scale on “Sojump” again. We sent the web link and QR code to students through WeChat, using their classes as units, and received 1709 completed questionnaires (including some students submitted more than once), and excluding repeated includes 1172 copies, according to conditions as well as on pretest, after comparison by student number when students fill the questionnaires in the 774 copies of the pretest and 1172 on the post-test, we obtained the correspondent copies on the same object in total 463 copies for study in Post-test.
Tools
The adolescent psychosexual development scale (APDS)
This study put psychosexual health as the basis for characteristic variables by the series of psychoanalysis theories including Fred’s sexual motivation and Jung’s theory of personality development. The adolescent psychosexual development scale (APDS) used was designed by China’s Yi LUO and Yong ZHENG3. It includes 46 items (including 4 lie detection questions), comprising three sub-scales: psychosexual knowledge, psychosexual values, and adaptability. Psychosexual cognition contains two factors: physiological and psychosexual knowledge. Psychosexual values refer to two factors: psychosexual concepts and attitudes. Further, psychosexual adaptability includes three aspects: social adaptability, psychosexual control, and self-adaptation. The questionnaire is taking the Likert 5-level scoring method,that is fill the number and get the corresponding score, and the higher score demonstrates higher level of psychosexual health32. This scale has good reliability and validity; Cronbach α is 0.857.
Adult attachment scale (AAS)
Chinese scholar Weili WU thinks that adult attachment (AAS) refers to adults’ recollection, reproduction and evaluation of their early attachment experience in childhood. The scale used in this research was the Chinese edition Adult Attachment Scale33 (AAS-1996 revision) which was translated by Weili WU et al.34,35, was initially designed by Collins et al. and was revised in 1996. It is more suitable to evaluate adults’ intimate and partner relationships35. The scale includes 18 items, classifying as 3 subscales respectively about intimacy, dependence and anxiety. Each subscale is made up of 6 items and taking the Likert 5-level scoring method, that is fill the number and get the corresponding score. With the close dependence dimension that formed between attachment closeness and dependence, and in combination with the closeness dependence and attachment anxiety scores, we can get 4 types of attachments, respectively security, preoccupation, rejection and fear types. In the scale, items 2, 7, 8, 13, 16, 17, and 18 are reverse scoring entries and thus scores shall be conversely calculated. The scale has good reliability and validity and its revised version is suitable for Chinese people, whose Cronbachα values are 0.683 and 0.845 respectively on close dependence and attachment anxiety.
The previous scale was lack of the choice and classification for value = 3. Therefore, in this study, we made the following revisions to the scale’s classification during analysis and model construction (in total 155 pieces of data). ① close dependence = 3, and anxiety > 3 (2 preoccupied type). ② close dependence = 3, and anxiety < 3 (3 rejective type). ③ close dependence > 3, and anxiety = 3 (1 security type). ④close dependence < 3, and anxiety = 3 (4 fear type) ⑤ close dependence = 3, and anxiety = 3 (1 security type).
Social support rating scale (SSRS)
This study takes the Social Support Rating Scale compiled by Shuiyuan XIAO in 1986 to measure social support levels27, which includes 10 items, measuring from three dimensions respectively as objective supports (3 items), subjective supports (4 items) and the utilizing rate of social support (3 items). With the Likert-type self-reported 4-level scoring and Less than 9 points for the total score, that is fill the number and get the corresponding score, and as a rule the higher score shows more higher degree of SSRS. The scale demonstrates good reliability and validity, Cronbachα is 0.695.
Non-suicidal self-injury (NSSI) severe degree rating scale for clinicians
According to Muehlenkamp research (2012), using of a single NSSI measurement tool it can effectively obtain a consistent estimation on the incidence rate of NSSI behaviors36. For better analysis and positive screening, this study uses the NSSI Severe Degree Rating Scale for Clinicians (NSSI). This scale only has one item: Do you presently have or have you ever had NSSI behaviors in the past 1 year, rating by 0–4 assessment on five-level?
Study design procedures and protocol
We collected longitudinal data points of the two semesters by questionnaire: interval was one semester (six months) between pretest and post-test, questionnaires were collected at the end of the first semester (September ~ December, 2022) for pretest, and the end of the second semester (March ~ June, 2023) for post-test.
We surveyed students before the semester by questionnaire, which is the original data and the reference of course design. The teaching method combined questioning and interaction with group games. This approach fosters group collaboration, broadens perspectives, and enhances understanding of psychosexual knowledge. It promotes the development of AAS and SSRS, helps change sexual cognition, and shapes sexual attitudes and values. We designed the courses for psychosexual health (APDS) development and games with collective assistance (AAS and SSRS). This was achieved through group games and activities in the semester’s 4 h in two psychological health courses approximately every two weeks apart.
For second-year students (sophmore), taught by 8 h over four courses in two semesters, with one 2-h course approximately every two weeks. The first semester courses were from September to November 2022. The content was as follows: (1) Emotion, feeling, and personality. (2) Love (including AAS) and study planning. The second-semester courses were from March to May 2023, with content as (3) Psychosexual health (APDS) and self-identification. (4) Career planning and social relationships (including SSRS). First-year students (freshmen) received 4 h of instruction over two courses in one semester. For first-year students, just a one-course semester was from March to May 2023, with content as (1) Psychosexual health (APDS) and self-identification. (2) Love (including AAS) and social relationships (including SSRS).
Statistical methodology
In the pretest study, firstly, we used Common method deviation test (CMB) and performed descriptive statistics on the samples, and through independent sample t-test and one-way ANOVAs to explore demographic differences and correlations for the core variables using SPSS Windows software version 26.0. Afterward, we conducted Pearson Relevant analysis, separate hierarchical linear regressions and Logistics Regression Model to analyze the paths relevant and to test the relevance of APDS-AAS-SSRS-NSSI. Finally, we have found the discrepancy in statistical population variances on NSSI. Further, we established the chained mediating model through the SEM equation using Amos Windows software version 26.0, explored APDS’s impaction on NSSI, and analyzed the chained mediating effect of AAS and SSRS between APDS and NSSI through Bootstrap method to address the hypotheses of the relationship of the variables. We also tested the model’s fit index by setting CMIN/DF to less than 5, RMSEA to less than 0.08, and GFI, IFI, TLI, and CFI to greater than 0.80.
In the post-test, this was achieved through observing and statistical comparisons in sex, grades, and with or without psychological counseling experience through descriptive statistics on the samples, and then comparing and analyzing the variation of APDS and NSSI before and after intervention by paired sample t-test in SPSS Windows software version 26.0.
Results
Sample condition
We have collected Pre-test questionnaires in total 958, according to research conditions and severe levels (answer time too long or too short, or with high similar choices, etc.), we excluded 67 questionnaires that answered with more than 2400 s and 117 that below 600 s and finally obtained valid 774 questionnaires, as the object research for Pre-test, effective rate 80.79%.
We collected 1709 completed questionnaires by Post-test. For the research and according to the preset conditions, we excluded repetitively and carelessly answered questionnaires (answer time too long or short, with highly similar choices, etc.). The remaining part includes 1172 of 1193 questionnaires, excluding 82 that answer time below 300 s, 68 above 1800s (include), and 277 repeated, with a valid rate of 98.24%. After comparison by student number when students fill the questionnaires in the 774 copies of the pretest and 1172 on the post-test, we obtained the correspondent questionnaires on the same object in total 463 copies, which as post-test research data.
The demographic Characteristic of sample are shown in Table 1.
Common method bias test—CMB
As the data adopted the questionnaire method to collect, in order to reduce the common method bias caused by the self-reports of the participants, first of all, the anonymity and confidentiality of the questionnaires were emphasized and it was stated that the data was only for scientific research use when distributing the questionnaires. Moreover, it was explained again in the questionnaire guidance to control the sources of CMB as much as possible. Secondly, we selected Scales with higher reliability and validity, includind a certain number of reverse scoring items. Meanwhile, we used Harman one-way ANOVAs exploratory factor analysis (EFA) after data collection using SPSS 26.0, with a total of 11 factors Packaging, including APDS (3 dimensions), AAS (2 dimensions), SSRS (5 dimensions) and NSSI (1 item). The results showed that: there were 4 factors with eigenvalues greater than 1 and the variance explained by the first factor was 26.15%, which was less than 40%. Therefore, there was no obvious CMB in our study.
The reliability and validity test of scales
We achieved higher reliability and validity Scales through exploratory and confirmatory factor analysis (EFA/CFA), using KMO and Bartlett’s test. The results showed that the coefficient of the KMO was 0.864 (The value range was between 0 and 1, and the closer the value was to 1, the higher the validity of the questionnaire). Furthermore, we analyzed reliability and validity of scales with the standard loading and reliability analysis (Cronbach’s α) of each factor of core Variables, as well as combined reliability (CR) and mean variance extraction (AVE). The results displayed that the scales are with reliability of the good Cronbach’s Alpha coefficients, and CR values were all greater than 0.9 (0.927, 0.955, and 0.993 respectively), and the AVE values were all greater than 0.6 (0.648, 0.913, and 0.9661 respectively), indicating that the scales had good internal consistency and convergent validity. The results of the differential validity test showed that the square root values of the latent variable AVE on the diagonal are all greater than the pairwise correlation coefficients between the latent variables, indicating that the scale has good discriminative validity. It indicates that the questionnaire used in this study has good reliability and validity.
Correlative analysis of the pretest variables
We employed descriptive statistics and Pearson correlation analysis on the pretest variables through SPSS 26.0. The results are shown in Table 2.
The above results show significant pairwise correlations among APDS, AAS, SSRS and NSSI behaviors.
Regression analysis indicates:APDS (β = − 0.149, p < 0.001) has a significant negative predictive effect on NSSI, and APDS (β = − 0.130, p < 0.001) as well as effect on AAS, and APDS (β = 0.297, p < 0.001) has a Significant positive predictive effect on SSRS. AAS (β = − 0.320, p < 0.001) has a significant negative predictive effect on SSRS, and AAS (β = 0.169, p < 0.001) has a Significant positive predictive effect on NSSI. SSRS (β = − 0.165, p < 0.001) has a significant negative predictive effect on NSSI.
On the above, Both of APDS and SSRS can significantly negatively correlated with NSSI behavior, while AAS was significantly positively correlated with NSSI behavior. APDS was significantly negatively correlated with AAS but Significantly positive predictive effect on SSRS. AAS was significantly negatively correlated with SSRS.
Therefore, our hypothesis 1 and hypothesis 2 were Verified.
Hypothesis 1
APDS correlates with NSSI.
Hypothesis 2
Significant Pairwise Correlations among APDS, AAS and SSRS.
Structural equation modeling and mediation effect analysis
Based on the existing theories1,4,15,29,31. We established the initial model with demographic variables controlling such as gender, age, and grade in Amos 26.0, as shown in Fig. 1. The model’s fitting index is CMIN/DF = 2.262 (RMSEA = 0.044, GFI = 0.984, CFI = 0.963, TLI = 0.946, IFI = 0.963), indicating an excellent model.

Mediating model of psychosexual health, AAS and SSRS.
Analyzing each path of the initial model, and mediating effect tests through Bootstrap method, result as shown in Table 3.
Regression analysis and the results showing of able 3 indicate:
When a 95% confidence interval of all the mediating effects does not include 0 and p < 0.01, the direct and indirect impacts are significant. APDS was Significantly positive predictive effect on SSRS, with the direct effect of APDS on SSRS (β = 0.384, p < 0.001) after adding the mediating variable AAS between them, asβ increased from |0.297| to |0.384|, it shows that the mediating effect of AAS is significantly.
In the 95% confidence interval of three all mediating pathways excluded 0, including APDS → AAS the mediating pathway 1 (β = − 0.129, p < 0.01), AAS → SSRS the mediating path 2 (β = − 0.356, p < 0.01) and APDS → AAS → SSRS the mediating path 3 of (β = 0.046, p < 0.01), it shows that APDS has significantly positive predictive effect on SSRS under the mediating effect of AAS.
Among all the mediating pathways, the proportion of direct effects was 89.3%, and the proportion of total indirect effects was 11.7%: (1) The proportion of indirect effects by Path 1 APDS → AAS was 8.59%. (2) The proportion of indirect effects by Path 2 SSRS → AAS was 3.11%.
On the above, our hypothesis 3 were Verified.
Hypothesis 3
APDS is related to SSRS, with AAS as a mediating effect between them.
To further verify the correlation between APDS and NSSI and to explore the mediating effect on ASS and SSRS, we established a new model based on the initial model in Amos 26.0. After analyzing the model’s fitting index and actual data through multiple observations and revisions in the calculation process, we obtained the ideal model, as shown in Fig. 2. Its fitting index is CMIN/DF = 2.483 (RMSEA = 0.044, GFI = 0.980, CFI = 0.949, TLI = 0.926, IFI = 0.950), which indicates the excellent model.

A Chained mediating model of psychosexual health, AAS, SSRS and NSSI.
Through each path analysis and mediating effect tests of the model by Bootstrap method, as shown in Table 4.
Regression analysis and the results showing of Table 4 indicate:
-
(1)
APDS was Significantly negatively predict on NSSI, the 95% confidence interval of the total effect value (β = -0.155, p < 0.01) excluding 0, indicating that the total effect was significantly.
-
(2)
The 95% confidence interval of the direct effect (β = -0.059, p = 0.293) including 0, and p > 0.05, indicating that the direct effect is non-significantly.
-
(3)
The 95% confidence interval of the total indirect effects value (β = − 0.096, p < 0.01) excluding 0, indicating that the total indirect effects was significantly.
-
(4)
This mediating effect of total indirect effects is specifically composed of three indirect pathways:
① With adding the mediating variable AAS between APDS and NSSI, the direct effect of value (β = − 0.129, p < 0.001) , as β declined from |− 0.149| to |− 0.129|, it shows that the mediating effect of AAS holds true between them. The 95% confidence interval of indirect effect by APDS → AAS → NSSI the mediating pathway 1 (β = 0.004, p = 0.137) including 0, and p > 0.05, indicating that the indirect effect is non-significantly.
② With adding the mediating variable SSRS between APDS and NSSI, the direct effect of value (β = − 0.110, p < 0.01), as β declined from |− 0.149| to |− 0.110|, it shows that the mediating effect of SSRS holds true between them. The 95% confidence interval of indirect effect by APDS → SSRS → NSSI the mediating pathway 2 (β = − 0.077, p < 0.01) excluding 0, indicating that the indirect effect is significantly.
③ With adding the mediating variables AAS and SSRS at the same time between APDS and NSSI, the direct effect of value (β = − 0.059, p = 0.293), as β declined from |− 0.149| to |− 0.059|, it shows that the Chained mediating effect of conduction by AAS and SSRS holds true between them. The 95% confidence interval of indirect effect by APDS → AAS → SSRS → NSSI the mediating pathway 3 (β = − 0.009, p < 0.01) excluding 0, indicating that the indirect effect is significantly, and the total indirect effects (β = − 0.096, p < 0.01) is significantly, in the meanwhile the direct effect is non-significantly, therefore, this Chained mediating role plays a complete mediating role between APDS and NSSI.
Among all the mediating pathways, the proportion of direct effect was 38.06%, and the proportion of total indirect effects was 61.94%: (1) The proportion of indirect effects by Path 1 APDS → AAS → NSSI was 1.87%. (2) The proportion of indirect effects by Path 2 APDS → SSRS → NSSI was 36.02%. (3) The proportion of indirect effects by Path 3 APDS → AAS → SSRS → NSSI was 5.81%.
In conclusion, our hypothesis 4 and hypothesis 5 were Verified.
Hypothesis 4
Both of AAS and SSRS plays a mediating role respectively between APDS and NSSI behaviors.
Hypothesis 5
The Chained Mediation by AAS and SSRS plays a effect role in the relationship between APDS and NSSI behavior, and influencing NSSI behaviors.
Comparison of the positive detection rate of NSSI behavior
To observe the positive detection rate of NSSI behavior, we compared pretest and post-test, as Table 5 shown.
The results show total proportion of NSSI behavior was 12.53%, and a clear downtrend on NSSI various data in post-test.
In the meanwhile, we observed and compared the variation of the independent variables in Pre-test and Post-test, as shown in Table 6.
Variance analysis on core variables of the same participants in Pre-test and Post-test
In the pretest, carrying an independent sample t-test on demographic variables, The results show significant discrepancy of APDS in grade level, an only child or family’s anual income, but of NSSI behavior in ethnicity (Han or non-Han) and grade level. Both of the independent and the dependent variables are significantly correlated with the grade (amount to age) variable. Moreover, the variation of the APDS is significantly in the different grades (between Sophomore and Freshman) in pretest and post-test.
We compared and analyzed the variation of two core variables in Pre-test and Post-test using a paired sample t-test, as shown in Table 7.
Through analyzing the above comparison as shown in Table 7, we can find that, the value of APDS increased significantly after intervention, with a mean average increase of 6.907 (t = − 7.621, p < 0.001), and also NSSI decreased, with a mean average decrease of 0.060 (t = 1.812, p = 0.071). According to the range of p, we found that the comparison of APDS has statistical significance in Pre-test and Post-test. Thus, the results of this study validated we can intervene further in the occurrence of NSSI behavior by promoting the development level of psychosexual health through games of class group mutual assistance (by AAS and SSRS).
In order to obtained the further differences between two grades, we grouped the post-test samples according to Sophomore and Freshman, to compare the differences between two groups using a paired sample t-test. After comparing and analyzing variation of independent and dependent variables from the same participant in Pre-test and Post-test, Table 8 was shown.
Through the results from Table 8, we can find that the significantly variations of two variables in the two groups, and the value of Psychosexual Health in the post-test of Sophomore has significantly increased, with an average increase of 7.538 (t = − 7.856, p < 0.001). The larger the absolute value of t is, the smaller the p value will be. Compared with two groups, it is obvious that the intervention effect from sophomore is better, while the variation of APDS from freshman are not significant in pretest and post-test. In consideration of both Psychosexual Health and NSSI behaviors were significantly correlated with grade (amount to age) variable, we suppose that it might be caused by the different class hours for sophomore one hand, in addition, due to the adaptation to campus environment as well as the interpersonal relationships.
Therefore, all of our hypothesizes have been verified.
Discussion
In our pretest study found the total proportion of 774 questionnaires contains 97 copies with NSSI behavior accounting for 12.53%. This study concords with the relevant study and report37,38. which the ratio of Chinese college students is 10.7% ~ 24.7%37, and the relevance ratio of medical students at Guangxi Medical University is 15.13%14. Studies have shown that the incidence of NSSI behavior among Chinese adolescents (13–18 years old) is higher in girls than in boys13,38. The relevant research showed that sex and age have significant relevance with NSSI39, and our results in pretest have shown the grade (amount to age) variable has significantly relevance with NSSI behavior, which match a previous study40. Nevertheless, the reason might be, why no difference in our research between gender groups, that our samples were mainly female. In the post-test study, NSSI behavior Significantly correlated with psychological counseling experience (amount to with and without intervention).
The results of Pearson correlation analysis indicated that APDS was significantly correlated pairwise with AAS, SSRS and NSSI behaviors, precisely verifying our Hypothesis 1 and Hypothesis 2. And the initial model in Fig. 1 perfectly validates our Hypothesis 3. The ideal model in Fig. 2 just verified our Hypothesis 4 and Hypothesis 5, which is APDS’s impacts on NSSI, with AAS and SSRS playing chained mediating roles in the relationship and influencing NSSI. The study’s results indicate that emphasizing the importance of APDS development levels of adolescents aimed at NSSI behavioral decrease.
Our results in pretest demonstrate Psychosexual Health’s impact on Non-Suicidal Self-Injury behavior, and the influence of the chained moderating role with AAS and SSRS between them, it is crucial of the great importance of the development level of APDS for reducing NSSI behaviors among adolescents.
The findings showed that both the variations of APDS is significantly in sophomore but unsignificantly in freshman in pretest and post-test, compared with two groups, in consideration of correlation with grade (amount to age) variable, we are unsure whether it is caused by the different class hours or grades. Perhaps second-year students’ adaptability to learning and interpersonal relations on campus is more beneficial to APDS, AAS, and SSRS development. It may be confirmed in future research.
It should be noted that we did not divide the testees into control groups and compare them before the class or process. We intervened with all the testees by group and compared them, then analyzed all the data about the positive group with NSSI. Therefore, there may be some unknown error in the process or the result, and deviation may be caused.
Our results verify that AAS can negatively predict SSRS and positively predict NSSI, which mean individuals with insecure adult attachment (AAS) develop unhealthy relationship patterns and scarce SSRS easily, and more tend to NSSI behaviors. Brausch & Muehlenkamp41 support that individuals with NSSI have higher levels of anxiety (worrying about being abandoned and disliked) compared with those without NSSI and lower levels of intimacy (comfort about being closed and intimate with others) and insecure attachment is a risk factor on individual develop an emotional and actional problem42. Liu et al.43 indicated that insecure attachment plays a crucial role in the progress of individuals in developing risky actions, which is caused by more trauma relevant to the insecure attachment schema of an individual with NSSI, such as losing and being mistreated. These views exactly right supports our research results.
Our results in pretest study showed that the better level of APDS, the higher degree of SSRS obtained, and the lower positive detection rate of NSSI behaviors. It is the fact that the positive detection rate of NSSI behavior is higher in subjects with insecure attachment than insecure adult attachment. Our research results just confirm that an individual’s insecure AAS and lack of SSRS are more likely to lead to NSSI behavior.
The research confirms that SSRS can negatively predict NSSI behaviors44, and a high-quality SSRS system will enhance stress capacity and reduce the risks of NSSI psychological health problems45. The study showed that SSRS can positively predict APDS in adolescents in later periods, which a higher level of SSRS with higher APDS2. These points match our results.
Relative study showed that can further improve the social functions of adolescent patients with NSSI behaviors by group skills training46. Relevant research shows that individual’s attachment category can be changed with the time and process of psychotherapy31. Our results just demonstrated that group mutual assistance for promoting APDS on the development of AAS and SSRS, which would have a positive impact on reducing NSSI behaviors. This result is consistent with previous related studies2,19,28.
In conclusion, conducting educational guidance to promote the development of Psychosexual Health and group mutual assistance on campus, which is conducive to the formation of secure adult attachment and good social supports. Therefore, promoting APDS with well-developed, secure AAS and high-quality SSRS formation will prevent and improve NSSI behaviors.
Limitation and innovative value of the research
Limitation and future research direction
Although this study has proposed a theoretical model of chain mediation for APDS, AAS, SSRS and NSSI, which has certain value and significance, it still exists certain limitations.
The first limitation of the study is that the sample objects are all willing participants from fixed majors, who can not represent all college students.
Secondly, this study used a design characterized by quantitative combinative follow-up studies and direct manipulation of variables, which can provide more conclusive evidence of causality.
Thirdly, we did not divide all subjects into groups before and during the class but made group intervention and comparative analysis on all, that is, no control group and comparative group, and thus, there may be some unknown errors during the process and biased results.
Fourthly, students may not give their answers out of their feelings, considering that the post-test might have something to do with their completion evaluation (though the questionnaire had declared in its introduction).
Lastly, we could not conduct specific interviews and investigations on the selected NSSI subjects; we could only classify with or not and their severe degrees. Moreover, it should be recognized we have designed initial study and used subjects without control groups, and the function of classroom group intervention games designed based on hands-on case experience and relevant literature inevitably has some limitations.
According to Erikson’s theory of self-identity (SIS), along with physical development and gradual maturity, thus new issues such as gender identity will compulsively enter the lives of adolescents with interpersonal relationships, and it would become a fundamental part of Psychosexual Health for adolescents1.
Erikson considered that self-identity formation process is of personality formation, and its development continue an individual’s whole life, and it is the most crucial stage for self-identity establishing in adolescence47. A large number of studies have shown the adolescence NSSI behavior is significantly positively correlated with self-identity confusion48,49, and it was pointed out that it is necessary for future studies to examine the dynamic process and internal mechanism of the interaction between these two variables by tracking research design39.
In future studies, here we put forward suggestions, according to the theories of Freud, Jung, and Erikson, a much longer follow-up study will better reveal the mutual promotion relationship among adolescent APDS development, mental health, and personality development. It will also better connect personality development with the integrity and continuity of self-identity, form a good and stable adult attachment relationship, promote harmonious interpersonal relationships, obtain good social support, and improve personal physical and mental health conditions and happiness index.
Currently, the treatments of NSSI heavily rely on clinical intervention or even hospitalization. Therefore, we suggest that future studies focus on educational therapy and guidance and verify the results of this study through a control group experiment. We can conduct intervention follow-up studies on the routine and control groups and conduct detailed interviews and situation surveys on selected NSSI subjects to understand the individual experience and psychological processes better, through a certain period of intervention and psychotherapy and with some qualitative research and analysis, we will hopefully summarize more methods and expertise and design better group games and schemes in the psychological health education class in college.
Innovation value and practical meaning of the research
Previous studies mainly focused on the relationship between NSSI and personality disorder, between NSSI and depression disorder, and between depression and personality, which pays more attention to cause analysis and symptom elimination, and It mainly focuses on the treatment of behavioral addiction and related psychological problems in clinical adolescents.
However, the important innovation of this study is that it reviews, studies, and analyzes NSSI-related research literature to examine NSSI behavior’s development trend and its decisive characteristics. Our study emphasizes discovering the existence of NSSI behavior among individuals and better understanding the positive factors that can be changed and adjusted. Based on the results, we conducted empirical studies using a horizontal and tracking research design and by questionnaire, interview, and case intervention process analysis. Through the structural equation model, we examine college students (primarily girls) as the object to find APDS’s influence on NSSI under the chained mediating effect of AAS and SSRS.
Despite limitations, it still has certain innovations as follows.
Firstly, it is the first attempt tracing study on the impact of adolescent psychosexual health development on non-suicidal self-injury according to developmental psychology in domestic, to supplement the previous and existing theories, enrich and improve the current research status in relevant field. Furthermore, we provides references and offers strong empirical supports for conducting related research in the future.
Secondly, this study is unique using psychosexual health in Freud’s sexual driven theory, a beneficial factor for personality development of adolescent. It the view of positive perspective to explore effective measures for group intervention on NSSI behaviors among adolescents. To help individuals develop self-identity and personality independence during adolescence through school education guidance.
Lastly, our study Multiple chain mediation model provides theoretical basis and intervention plans for helping adolescent to develop secure adult attachment, establish harmonious interpersonal relationships, and it provides intervention programs for reducing the occurrence of NSSI behaviors in the campus environment. It also offers theoretical supports for establishing and improving a systematic curriculum for adolescent psychosexual health and self-identity development on campus.
According to the above, we conducted specific Practical values and practical significances.
Adolescence is also a critical period in forming views toward the world. If adolescents can achieve a healthy development in all aspects of psychological health, their psychological contradiction will decrease significantly, promoting the sound development of their overall psychological mechanism and personality. Therefore, psychosexual health education shall be accorded the same importance as positive physical and psychological development. Building and perfecting a systematical sex, the psychologically healthy educational system is crucial to an adolescent’s psychosexual health and life-long happiness. This also plays a decisive role in an adolescent’s all-round development, including personality development, physical and psychological health, and establishing social relations.
With anticipation, we can provide more schools with practical educational guidance, prevention measures and effective strategies to prevent NSSI behaviors among children and adolescents on campus, in the meanwhile, to support individuals with psychological growth and to put forward group intervention on NSSI behaviors during adolescence. Which are of significant meanings for NSSI patients providing effective educational guidance and prevention strategies for more families and schools education, we attempt to summarize some universally applicable intervention scheme and valuable research information or data for use in clinical or psychological counseling.
Our study results will help the future preschool and primary school education practitioners smoothly to go over their psychological task of adolescent development. And provide more supports to implement the educational guidance of the psychosexual development and self-identity for the future preschool and primary school teachers at an early stage, to promote their overall development on personality, health both in both body and mind as well as the establishment of social links and etc., to prevent unhealthy personality development. To know the mental sub-health status of those future preschool and primary school practitioners, and promoting their personality healthy development through cultivating their social support and adult attachment; and timely and timely intervening those with personality disorders and directing them to go through psychological health education.
Conclusion
In conclusion, Developing PSYCHOSEXUAL HEALTH can decrease and prevent NSSI behavior among adolescents intervention by promoting AAS and SSRS. The study seeks to assess the impact of PSYCHOSEXUAL HEALTH on adolescents’ NSSI behaviors through promoting AAS and SSRS, We utilized PSYCHOSEXUAL HEALTH, AAS, SSRS, and NSSI questionnaires to evaluate college students’ PSYCHOSEXUAL health conditions and determine the proportion of NSSI among normal individuals, which validate the correlation of PSYCHOSEXUAL HEALTH and NSSI as well as the chained mediating effect of AAS and SSRS.
In conclusion, we confirmed developing APDS can decrease and prevent NSSI behavior among adolescents intervention by promoting AAS and SSRS, utilizing APDS, AAS, SSRS, and NSSI questionnaires to evaluate college students’ APDS conditions and determine the proportion of NSSI among normal individuals, which validate the correlation of APDS and NSSI as well as the chained mediating effect of AAS and SSRS. In our study, APDS could significantly negatively predict NSSI and AAS, and directly positively predict SSRS at the same time. AAS can negatively predict SSRS and positively predict NSSI. SSRS can negatively predict NSSI. Thus, this study indicates that improving individual psychosexual health levels is conducive to the development of secure adult attachment and the formation of good social support, and all three are protective factors for NSSI behaviors.
To sum up, here are conclusions as follow:
-
(1)
Psychosexual health has a significant impact on adult attachment, social supports and non-suicidal self-injury behaviors.
-
(2)
There is a significant correlation between each pair among APDS, AAS, SSRS and NSSI behavior under controlling for demographic variables such as sex, grade etc.
-
(3)
APDS positively predict SSRS significantly, and AAS plays an intermediary role between them.
-
(4)
APDS negatively predict NSSI behavior significantly, AAS and SSRS play separate mediating roles respectively between them.
-
(5)
The chained mediating by AAS and SSRS plays complete mediating effect role between APDS and NSSI behavior, impact on NSSI behavior.
-
(6)
In practice, when conducting psychological counseling and treatment for adolescents with NSSI behavior, we can integrate the development of individual psychosexual health and self-identity into cognitive emotional therapy and intervention simultaneously, in order to enhance individual personality development and mental health levels.
Data availability
No datasets were generated or analysed during the current study.
References
Yi, L. & Yong, Z. A preliminary study of puberty psychosexual health. Psychol. Sci. 29(3), 661–664 (2006).
Luo, D. M. et al. Bachelor nursing students’ psychosexual health and social supports relevant study. Occupation Health 32(9), 1256–1259 (2016).
Luo, Y. Adolescent Psychopsychosexual Health Questionaire initial authorization 2005 (Western Southern Normal University, 2005).
Freud, S. Three essays on sexology and love psychology (Y. Li, Trans.). (Taihai Press, 2016).
Liu, Y. C. Sexual education and psychosexual health. Chin. Sex. Sci. 10(3), 25–27 (2001).
Zhang, K. & Zheng, Y. The relationship between learning ways about sexual knowledge and psychosexual health. J. Third Military Med. Univ. 32(23), 2482–2502 (2010).
Deng, X. L. Mental health education for college students (Second Edition). In 21st century higher vocational college planning textbook - general education course series, (Renmin University of China Press. 2015)
UNESCO. United Nations Educational, Scientific and Cultural Organization.International technical guidance on sexuality education, pp. 16–20. (Paris: UNESCO.2018; 2018).
Cao, Y., F., Chen, ,. Zheng, L., L., Zhang,Y., Gou, P., The effectiveness of systematically conducting sex education for adolescent students from the perspective of sexual mental health. School Health in China. 2021, 42(11). https://doi.org/10.16835/j.cnki.1000-9817.2021.11.033.
Yin, Z. C., Zhang, Z., W., & Ma, B. X. Sichuan agricultural university. Luzhou polytechnic, research on the sexual mental health status and influencing factors of vocational colleges and universities psychological monthly. 2021(21) (2021). https://doi.org/10.19738/j.cnki.psy.2021.21.014.
Peng, H. L. & Yue, J. The causes and responses of non-suicidal self-harm among children and adolescents. Women Children’s Health Guide 3(6), 8–9 (2024).
Hao, Y. & Lv, X. Stressful life events and non-suicidal self-harm among adolescents: There is a moderating mediating effect. Chin. J. Disease Control 26(06), 668–672 (2022).
Wang, P., Zhou, X., Jia, C., Liu, S., Zheng, W., Hu, A., Pang, Q., Liu, C., Zhang, S., Wang, M., & Henan University. (2008). Epidemiologic study on the aggressive behaviors of college students, preventive medicine and hygiene. 330.21, Medical Health Technology, (Vol. R181) (32).
Pan, Z. et al. Meta-analysis on non-suicidal self-injury among college students in China. Chin. J. School Health 37(6), 878–881. https://doi.org/10.16835/j.cnki.1000-9817.2017.11.019 (2016).
Zhao, T. & Wang, X. (2022). The characteristics and influence factors of borderline personality disorder and depressive disorder NSSI. Med. Health Technol. Pathergasiol. Psychiatry Mental Health, (02). https://doi.org/10.27111/d.cnki.ghyku.2021.000265.
Zhang, D. Diagnostic and statistical manual of mental disorders. 788 (Peking University Press, 2015).
Groschwitz, R. C. et al. The association of non-suicidal self-injury and suicidal behavior according to DSM-5 in adolescent psychiatric inpatients. Psychiatry Res. 228(3), 454–461. https://doi.org/10.1016/j.psychres.2015.06.019 (2015).
Nock, M. K. Why do people hurt themselves? New insights into the nature and functions of self-injury. Curr. Dir. Psychol. Sci. 18(2), 78–83. https://doi.org/10.1111/j.1467-8721.2009.01613.x (2009).
Zhang, Q. The influence of types of adult attachment on interpersonal communication. Sci. Educat. Lit. Rev. 550, 148–150. https://doi.org/10.16871/j.cnki.kjwha.2021.12.046 (2021).
Cheng, H. & Zhang, Y. Effect of childhood trauma on PTSD and PTG among college students: The mediating role of attachment. In 2023 the 7th international conference on medical and health informatics (ICMHI) (ICMHI 2023), May 12–14, 2023, Kyoto, Japan. p 5 (ACM, New York, NY, USA; 2023), https://doi.org/10.1145/3608298.3608358.
Pei, Y. Relationship between suicide attitude and adult attachment in non-suicidal self-injury. J. Int. Psychiatry 49(1), 1673–2952. https://doi.org/10.13479/j.cnki.jip.2022.01.001 (2022).
Menec, V. H. et al. Examining social isolation and loneliness in combination in relation to social support and psychological distress using Canadian Longitudinal Study of Aging (CLSA) data. PLoS ONE 15(3), e0230673 (2020).
Liu, Q. et al. Social support, resilience, and self-esteem protect against common mental health problems in early adolescence: A nonrecursive analysis from a two-year longitudinal study. Medicine (Baltimore) 100(4), e24334 (2021).
Chen, Z. et al. The mediating role of coping styles in the relationship between perceived social support and antenatal depression among pregnant women: A cross-sectional study. BMC Pregnancy Childbirth 22(1), 188 (2022).
Yang, Y., Lu, X. Z. & Kong, F. Effects of parent–child communication on psychosexual health of junior middle school students: Mediating role of social support and coping style. Chin. J. Clin. Psychol. 30(4), 842–846. https://doi.org/10.16128/j.cnki.1005-3611.2022.04.017 (2022).
Litwin, H. & Landau, R. Social network type and social support among the old-old. J. Aging Stud. 14(2), 213–228. https://doi.org/10.1016/S0890-4065(00)80012-2 (2000).
Xiao, S. (1999). Social support rating scale. In Manual of the mental health rating scale (X. D.Wang, X. L. Wang, & H. Ma, Eds.). Chinese Journal of Mental Health Press. pp. 127–131
Xiao, S. & Yang, D. Effects of social support on physical and mental health. Chin. J. Mental Health 1(4), 183–187 (1987).
Shen, H. & Gao, L. Psychological health 1st edn. (Ji’nan University Press, 1995).
Ma, Y. Q. Research on the current situation and influencing factors of non-suicidal self-harm behaviors among rural middle school students. Huazhong University of Science and Technology, (2016).
Cabaniss. D. L. Psychodynamics case conceptualization (M) (L. Sun et al., Trans.) 2:453–459 (2015)
Xu, J. Analysis on influencing factors and status of psychosexual health of higher vocational school students. Vocat. Tech. Educat. 17, 1008–3219 (2014).
Wu, W., Zhang, W. & Liu, X. Adult attachment scale (AAS-1996 Revised Edition)’s reliability and validity in China. J. Sichuan Univ. (Medical Edition) 35(4), 536–538 (2004).
Hazan, C. & Shaver, P. Romantic love is conceptualized as an attachment process. J. Pers. Soc. Psychol. 52(3), 511–524. https://doi.org/10.1037/0022-3514.52.3.511 (1987).
Wu, W., & Fang, L. Adult attachment measurement study. Chin. J. Clin. Psychol. 2004(4) (2004).
Luo, X. H. A follow-up study on the impact of adolescent psychological distress on non-suicidal self-harm behaviors, Guangzhou University, Master’s Thesis. (2024).
Huang, X. L. et al. The mediating effect of social support on depression and non-suicidal self-injury among medical students. J. Guangxi Med. Univ. 40(10), 1005–1930. https://doi.org/10.16190/j.cnki.45-1211/r.2023.10.012 (2023).
Yao, S. & Wang, M, Institute of Medical Psychology, The Xiangya 2nd Hospital, Central South University, Investigation on China’s Adolescent Health Relevant Dangerous Behaviors Conditions: Self-injury Conditions, Changsha, 410011 (2011).
Gu, H. L., Huang, J. & Li, J. C. The relationship between identity confusion and adolescent self-harm: The mediating role of alienation and the moderating role of difficulty in emotion regulation. Psychol. Dev. Educat. 41(1), 126–134. https://doi.org/10.16187/j.cnki.issn1001-4918.2025.01.14 (2025).
Gou, S. et al. A meta-analysis of the detection rate of non-suicidal self-injury in Chinese adolescents. Modern Prevent. Med. 50(02), 10–20043 (2023).
Brausch, A. M. & Muehlenkamp, J. J. Perceived effectiveness of NSSI in achieving functions on severity and suicide risk. Psychiatry Res. 2018(265), 144–150. https://doi.org/10.1016/j.psychres.2018.04.038 (2018).
Silva, E., Machado, B. C., Moreira, C. S., Ramalho, S. & Gonçalves, S. Romantic relationships and non-suicidal self-injury among college students: The mediating role of emotion regulation. J. Appl. Dev. Psychol. 2017(50), 36–44. https://doi.org/10.1016/j.appdev.2017.04.001 (2017).
Liu, X. et al. Nightmares are associated with future suicide attempts and non-suicidal self-injury in adolescents. J. Clin. Psychiatry 80(4), 12806. https://doi.org/10.4088/JCP.18m12181 (2019).
Wang, A., Bai, X., Lou, T., Pang, J. & Tang, S. Mitigating distress and promoting positive aspects of caring in caregivers of children and adolescents with schizophrenia: Mediation effects of resilience, hope, and social support. Int. J. Mental Health Nurs. 29(1), 80–91. https://doi.org/10.1111/inm.12651 (2020).
He, A. M., Hui, Q. P. & Liu, H. S. Relationship between social support and loneliness in undergraduates: The mediating role of gratitude. Chin. J. Clin. Psychol. 23(01), 150–153 (2015).
Xie, H. X. et al. The effect of group skills training on adolescents’ non-suicidal self-injury negative psychology and self-efficacy. Maternal Child Health Care China 37(9), 1001–4411 (2022).
Li, Y. A., Lou, W. & J. The reliability and validity test of the self-identity scale among adolescent students. Chin. J. Health Psychol. 17(02) (2009). https://doi.org/10.13342/j.cnki.cjhp.2009.02.057.
Gandhi, A. et al. Maternal and peer attachment, identity formation, and non-suicidal self-injury: A longitudinal mediation study. Child Adolescent Psychiatry Mental Health 13, 7. https://doi.org/10.1186/s13034-019-0267-2 (2019).
Gu, H., Ma, P. & Xia, T. Childhood emotional abuse and adolescent nonsuicidal self-injury: The mediating role of identity confusion and moderating role of rumination. Child Abuse Neglect 106, 104474. https://doi.org/10.1016/j.chiabu.2020.104474 (2020).
Acknowledgements
Recommended Reviewers •Ka Tat Tsang, Professor Factor-Inwentash Faculty of Social Work University of Toronto 246 Bloor Street West, Toronto, Ontario, Canada M5S 1V4 k.tsang@utoronto.ca •Nina Liu, MD, PhD Child, Adolescent and Adult Psychiatrist Department of Psychiatry and Behavioral Neurosciences Endeavor Health, Northshore University Health Systems. Clinical Assistant Professor University of Chicago, Pritzker School of Medicine Phone: 847-400-8451 Fax: 847-400-8445 nliu@northshore.org •Johnston Wong, Professor Applied Psychology, BNU-HKBU United International College johnstonhuang@UIC.edu.cn •Yin xu Department of Sociology and Psychology, School of Public Administration, SICHUAN University, CHINA yin.xu@scu.edu.cn
Author information
Authors and Affiliations
Contributions
Ping GAO conceived and designed the study, performed the statistical analysis, and drafted the article, and collected the data. Yuqing ZHANG took charge of the study design, and Mei ZHAO contributed to the article’s critical revision. All authors revised the article and approved the final version.
Corresponding authors
Ethics declarations
Competing interest
The authors declare no competing interests.
Ethics statement
This work was conducted in accordance with the principles of the Declaration of Helsinki and ethics approval (Nov.10th,2023/grant no. H23128) was obtained from the Ethics Committee of the Institute of Psychology, Chinese Academy of Sciences: The effect and mechanism of meditation intervention on teachers, parents and adolescents’ mental health,
Informed consent
In the study, voluntary and informed consent was obtained from all participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gao, P., Zhang, Y. & Zhao, M. Psychosexual health’s impact on non-suicidal self-injury of college students. Sci Rep 15, 33897 (2025). https://doi.org/10.1038/s41598-025-08900-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-08900-8
