
Abstract
The C-reactive protein albumin lymphocyte (CALLY) index is a newly proposed indicator of immune, inflammatory, and nutritional status. However, there is no research on the relationship between CALLY index and peripheral artery disease (PAD). We utilized relevant data from NHANES 1999–2004 on lower limb diseases research. PAD was diagnosed as an ankle-brachial index < 0.9. CALLY index was calculated using the formula: albumin (g/L) × lymphocytes (109/L) ÷ [CRP (mg/L) × 10]. Multivariable logistic regression and restricted cubic splines (RCS) were used to explore the relationship between CALLY index and the risk of PAD. Subgroup analysis was performed based on grouping variables. A total of 5283 participants aged 40 and above were included, with 419 PAD patients and 4864 non-PAD patients. Baseline data showed that PAD patients had significantly higher CALLY values. Multivariable logistic regression results indicated a significant negative correlation between CALLY index and the risk of PAD after adjusting for covariates (OR, 0.813, 95%CI, 0.717–0.923). RCS confirmed a significant linear negative correlation between CALLY index and the risk of PAD (P for nonlinearity = 0.989, P for overall = 0.002). Subgroup analysis revealed that the negative correlation between CALLY index and the risk of PAD remained significant in subgroups of male, white, other races, normal weight, former smoking, now drinking, as well as those with hypertension, without CKD, with or without diabetes, and with or without CVD. In other subgroups, there was also a negative correlation trend between ln CALLY and the risk of PAD. CALLY index is significantly negatively correlated with the risk of PAD. Future research should further validate the clinical application value of the CALLY index.
Similar content being viewed by others
Introduction
Peripheral artery disease (PAD) is a common atherosclerotic disease, which is characterized by lower limb artery stenosis leading to distal blood supply insufficiency, causing pain and intermittent claudication1,2. Epidemiological studies indicate that PAD affects over 200 million middle-aged and elderly individuals globally and is closely associated with increased rates of amputation and mortality3,4,5,6. With the aging population, the prevalence of PAD is expected to rise4. However, early PAD symptoms may be mild, or patients may mistakenly believe that leg vascular diseases are not life-threatening, resulting in underdiagnosis and undertreatment7,8. When local ischemia worsens or is accompanied by foot infection or even gangrene, conventional drugs and other treatment methods often have poor efficacy9. Even if blood flow is restored through lower limb revascularization, postoperative vascular restenosis and other issues often affect the long-term prognosis of patients10,11. Early diagnosis and intervention are crucial for PAD patients12.
The C-reactive protein-albumin-lymphocyte (CALLY) index is an emerging biomarker that combines albumin, lymphocytes, and C-reactive protein (CRP) to assess patients’ nutritional status, immune response, and inflammatory state13. Previous studies have shown that CALLY index is closely associated with the risk of sarcopenia, cardiorenal syndrome, and rheumatoid arthritis disease activity14,15,16. Given that nutritional status, systemic inflammation, and immune response are central to the pathophysiology of atherosclerosis, the CALLY index could be a potential indicator for predicting the risk of PAD. However, the relationship between CALLY index and PAD remains insufficiently explored. Understanding this relationship is essential for early screening of high-risk PAD populations and intervention. This study aimed to explore the relationship between CALLY index and the risk of PAD in the general U.S. population using the data from NHANES 1999–2004.
Methods
Data source
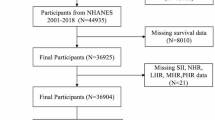
The National Health and Nutrition Examination Survey (NHANES), conducted by the National Center for Health Statistics (NCHS), is a nationally representative survey designed to assess the relationship between nutrition and health in the U.S. general population. A total of 31,126 participants took part in the NHANES 1999–2004, with relevant data on lower limb diseases available for those aged 40 and above (n = 9970). We initially included all subjects who underwent lower limb disease examinations in NHANES 1999–2004. Exclusion criteria: (1) Participants with an ankle brachial index (ABI) > 1.4 (n = 113), (2) Participants with missing ABI data (n = 3020), (3) Participants with missing CALLY index related data (n = 344), (4) Rheumatoid arthritis patients (n = 448), (5) Participants with missing covariates (n = 762). A total of 5283 participants were included in the final analysis, with 419 diagnosed with PAD and 4864 without PAD. (Fig. 1).

Process flowchart for screening participants for inclusion in the study.
Peripheral artery disease
Measure systolic blood pressure at the brachial artery of the right arm, and if the condition of the right arm interferes with the measurement (Presence of rash or open wounds, dialysis diversion surgery, right radical mastectomy, or any other factors that may interfere with accurate measurements), measure it at the left arm. Measure ankle joint systolic pressure at the posterior tibial artery of both lower limbs. ABI is calculated by dividing the posterior tibial artery systolic pressure by the brachial artery systolic pressure. PAD was diagnosed when at least one side had an ABI < 0.9.
C-reactive protein-albumin-lymphocyte index
Blood samples were collected after participants fasted for at least 8.5 but no more than 24 h. The CALLY index was calculated as follows: albumin (g/L) × lymphocytes (109/L) ÷ [CRP (mg/L) × 10].
Covariates
The selection of covariates is based on previous research and references to high-risk factors for PAD and factors that may affect the CALLY index2,3,4,15,17. Covariates included age, sex, race, poverty-income ratio (PIR), body mass index (BMI), total cholesterol, smoking history, drinking history, and the presence of hypertension, diabetes, cardiovascular disease (CVD), and chronic kidney disease (CKD). PIR was calculated by dividing family income by the poverty guidelines, specific to family size, as well as the appropriate year and state. We divided them into normal (< 25 kg/m2), overweight (25–30 kg/m2), and obesity (≥ 30 kg/m2) groups based on BMI values. We categorize smoking history into never (smoking less than 100 cigarettes in one’s lifetime), former (smoking over 100 cigarettes but now completely quitting), and now. At the same time, we categorize drinking history into never (drinking less than 12 drinks in a lifetime), former (not drinking since last year but drinking ≥ 12 drinks in a lifetime), and now. Hypertension was defined as an average systolic BP ≥ 140 mmHg and/or average diastolic BP ≥ 90 mmHg, or self-reported diagnosis or use of antihypertensive medications. Diabetes was defined as fasting blood glucose ≥ 7 mmol/L, random blood glucose ≥ 11.1 mmol/L, or 2-hour OGTT glucose ≥ 11.1 mmol/L, or glycated hemoglobin ≥ 6.5%, or self-reported diagnosis or use of antidiabetic medications. CVD was assessed via questionnaires. CKD was defined as an estimated glomerular filtration rate < 60 mL/min/1.73 m².
Statistical analysis
Data were analyzed using R (version 4.2.1). All statistical analyses were weighted using the “wtmec4yr” and “wtmec2yr” weights. Continuous variables are presented as mean (standard error), and categorical variables are presented as frequencies (weighted percentage). The CALLY index values were converted to natural logarithm, and participants were grouped into tertiles based on the ln CALLY values. Multivariable logistic regression was used to explore the relationship between CALLY index and PAD. Three models were constructed: Model 1 was not adjusted; Model 2 was adjusted based on demographic data (age, gender, race, PIR, BMI); Model 3 adjusted for all covariates. RCS was applied to detect the dose-response relationship between CALLY index and PAD. According to the ln CALLY level, groups were divided into three percentiles, Q1 ≤ 5.388, 5.388 < Q2 ≤ 6.404, and Q3 > 6.404. Subgroup analysis was conducted based on grouping variables. Interaction tests were performed using likelihood ratio tests to assess whether grouping variables interact with the relationship between CALLY index and PAD. Additionally, the area under the curve (AUC) of the receiver operating characteristic (ROC) was used to evaluate the predictive ability of CALLY index for PAD.
Results
Baseline characteristics of the study population
Table 1 presents the baseline characteristics of the participants, grouped by PAD status. The ln CALLY was significantly higher in the PAD group compared to the non-PAD group. Additionally, significant differences were observed between the two groups in terms of age, race, PIR, smoking history, alcohol consumption, and the prevalence of chronic conditions such as hypertension, diabetes, CVD, and CKD.
Multivariate logistic regression
The multivariate logistic regression analysis revealed a significant negative association between the ln CALLY and the risk of PAD, after adjusting for confounding variables (OR, 0.813, 95%CI, 0.717–0.923). For every 1-unit increase in ln CALLY, the risk of PAD decreased by approximately 18.7%. Compared with the first tertile of ln CALLY, the third tertile of ln CALLY was associated with a significantly lower risk of PAD (OR, 0.643, 95%CI, 0.444–0.930). (Table 2)
Restricted cubic splines
The RCS analysis demonstrated a dose-response relationship between ln CALLY and the risk of PAD. The results indicated a significant linear negative correlation between ln CALLY and the risk of PAD (P for nonlinearity = 0.989, P for overall = 0.002). (Fig. 2)

The dose-response relationship between CALLY index and the risk of PAD.
Subgroup analysis
In subgroup analysis, we adjusted for all variables except for grouping variables. Subgroup analysis based on all stratified variables showed that the negative correlation between ln CALLY and the risk of PAD remained significant in subgroups of male, white, other races, normal weight, former smoking, now drinking, as well as those with hypertension, without CKD, with or without diabetes, and with or without CVD. In other subgroups, there was also a negative correlation trend between ln CALLY and the risk of PAD. This supports the robustness of the findings. (Fig. 3)

Forest plot for subgroup analysis.
ROC curves of CALLY index in relation to PAD
We perform ROC analysis based on weighted data. The results showed that the AUC value of CALLY index was 0.629, indicating moderate predictive ability. (Fig. 4)

ROC curves of CALLY index in relation to PAD.
Discussion
In this study, we explored the relationship between the CALLY index and PAD using NHANES data from 1999 to 2004. The results from multiple logistic regression and RCS analysis indicate a significant linear negative correlation between CALLY index and the risk of PAD. Further subgroup analysis confirmed the stability of this negative correlation across different demographic and clinical variables. Our study provides new evidence for the potential of CALLY index as a biomarker for PAD and suggests its potential utility as an assessment tool for the risk of PAD in clinical settings.
To our knowledge, this is the first study to evaluate the relationship between the CALLY index and PAD in a large, nationally representative population. The CALLY index integrates three widely used clinical parameters: albumin, lymphocyte count, and CRP, which reflect nutritional status, immune capacity, and systemic inflammation respectively. Biological plausibility for the observed association is supported by the known roles of these components in vascular health.
Malnutrition, impaired immune function, and chronic low-grade inflammation are recognized risk factors for the development of PAD18,19. First, albumin is an important marker of nutritional status. Low levels of albumin are often associated with anemia, malnutrition, and an increased risk of cardiovascular diseases such as atherosclerosis20,21,22. Previous studies have shown that low albumin levels can promote inflammatory responses and accelerate atherosclerosis, potentially increasing the risk of PAD23. Second, lymphocyte count serves as an indicator of immune function. Lymphopenia has been linked to chronic inflammation and poor outcomes in cardiovascular disease. Reduced lymphocyte levels may reflect immunosenescence or stress-induced immune suppression, both of which contribute to endothelial injury and atherogenesis24,25,26. Thus, maintaining a normal lymphocyte count may protect blood vessels from inflammation-induced damage, potentially reducing the risk of PAD. Finally, CRP is a well-established biomarker of inflammation and has a direct pathogenic role in vascular remodeling and plaque instability27. Numerous studies have shown that elevated CRP levels are closely associated with the onset and progression of PAD28,29,30. High CRP levels typically indicate systemic inflammation, which plays a critical role in the development of PAD. Therefore, a higher CALLY index indicates better nutritional, immune, and inflammatory status, which may provide vascular protection and reduce the risk of PAD. The negative correlation between the CALLY index and the risk of PAD further emphasizes the importance of good nutritional status and immune function in mitigating the risk of PAD.
The findings of this study have significant clinical implications. The CALLY index is an easily measurable composite biomarker that reflects an individual’s nutritional status, immune function, and level of inflammation. Given the high incidence and disability rate of PAD, as well as its strong association with other cardiovascular diseases, early identification of high-risk populations is crucial for timely intervention and disease prevention31,32. Our study validated the relationship between CALLY index and PAD risk through a cross-sectional approach. The conclusion is that participants with lower CALLY indices may face a higher risk of developing PAD. The CALLY index may serve as a novel tool for assessing the risk of PAD in clinical settings and could help guide the development of tailored treatment strategies. This is particularly relevant for the elderly population, where PAD often coexists with other chronic diseases33,34. By evaluating the CALLY index, clinicians can gain a comprehensive understanding of a patient’s health status and implement early interventions.
Our main advantage lies in conducting a large-scale cross-sectional study using NHANES, a nationally representative sample. In addition, we use ABI to diagnose PAD. In fact, few large sample studies have measured ABI. Although this study provides preliminary evidence for the association between the CALLY index and PAD, several limitations should be noted. First, the cross-sectional nature of the data limits our ability to establish causal relationships. Future prospective studies are needed to explore the causal link between the CALLY index and PAD and to validate its effectiveness as a predictive tool for PAD. Second, although we have adjusted for multiple potential confounders in this study, some residual confounding factors may still influence the results. Finally, due to the large number of missing values for the ABI and CALLY index, potential selection bias may have been introduced.
Conclusion
This study demonstrates a significant negative correlation between the CALLY index and the risk of PAD. The CALLY index, which combines indicators of nutritional status, immune function, and inflammation, provides a new tool for assessing the risk of PAD. Future research should further validate the clinical application of the CALLY index and explore its potential value in the early screening and treatment of PAD.
Data availability
All data are publicly available at https://www.cdc.gov/nchs/nhanes/.
References
Bevan, G. H. & White Solaru, K. T. Evidence-Based medical management of peripheral artery disease. Arterioscler. Thromb. Vasc Biol. 40, 541–553 (2020).
Firnhaber, J. M. & Powell, C. S. Lower extremity peripheral artery disease: diagnosis and treatment. Am. Fam Physician. 99, 362–369 (2019).
Mandaglio-Collados, D., Marín, F. & Rivera-Caravaca, J. M. Peripheral artery disease: update on etiology, pathophysiology, diagnosis and treatment. Med. Clin. (Barc). 161, 344–350 (2023).
Criqui, M. H. & Aboyans, V. Epidemiology of peripheral artery disease. Circ. Res. 116, 1509–1526 (2015).
Barnes, J. A., Eid, M. A., Creager, M. A. & Goodney, P. P. Epidemiology and risk of amputation in patients with diabetes mellitus and peripheral artery disease. Arterioscler. Thromb. Vasc Biol. 40, 1808–1817 (2020).
Sigvant, B., Lundin, F. & Wahlberg, E. The risk of disease progression in peripheral arterial disease is higher than expected: A Meta-Analysis of mortality and disease progression in peripheral arterial disease. Eur. J. Vasc Endovasc Surg. 51, 395–403 (2016).
Campia, U., Gerhard-Herman, M., Piazza, G. & Goldhaber, S. Z. Peripheral artery disease: past, present, and future. Am. J. Med. 132, 1133–1141 (2019).
Anagnostis, P. et al. Peripheral arterial disease: an underestimated aspect of Menopause-related cardiovascular disease. Curr. Vasc Pharmacol. 22, 153–154 (2024).
Thomas, D. R. Managing peripheral arterial disease and vascular ulcers. Clin. Geriatr. Med. 29, 425–431 (2013).
Houghton, J. S. M., Saratzis, A. N., Sayers, R. D. & Haunton, V. J. New horizons in peripheral artery disease. Age Ageing. 53, afae114 (2024).
Shamaki, G. R. et al. Peripheral artery disease: A comprehensive updated review. Curr. Probl. Cardiol. 47, 101082 (2022).
Mascarenhas, J. V., Albayati, M. A., Shearman, C. P. & Jude, E. B. Peripheral arterial disease. Endocrinol. Metab. Clin. North. Am. 43, 149–166 (2014).
Iida, H. et al. Superiority of CRP-albumin-lymphocyte index (CALLY index) as a non-invasive prognostic biomarker after hepatectomy for hepatocellular carcinoma. HPB (Oxford). 24, 101–115 (2022).
Kılıç, Ö. et al. Immune nutrition indices are associated with disease activity in rheumatoid arthritis: a cross-sectional study. Biomark. Med. 18, 1093–1102 (2024).
Xu, Z. et al. Associations of C-reactive protein-albumin-lymphocyte (CALLY) index with cardiorenal syndrome: insights from a population-based study. Heliyon 10, e37197 (2024).
Li, Y. et al. Higher CALLY index levels indicate lower sarcopenia risk among middle-aged and elderly community residents as well as hospitalized patients. Sci. Rep. 14, 24591 (2024).
Chen, Y. et al. Association between C-reactive protein-albumin-lymphocyte index and stroke: an NHANES analysis (1999–2010). Front. Neurol. 16, 1548666 (2025).
Delaney, C. L., Smale, M. K. & Miller, M. D. Nutritional considerations for peripheral arterial disease: A narrative review. Nutrients 11, 1219 (2019).
Henein, M. Y., Vancheri, S., Longo, G. & Vancheri, F. The role of inflammation in cardiovascular disease. Int. J. Mol. Sci. 23, 12906 (2022).
Evans, D. C. et al. The use of visceral proteins as nutrition markers: an ASPEN position paper. Nutr. Clin. Pract. 36, 22–28 (2021).
Zhu, M. et al. Nutritional risk and nutritional status at admission and discharge among Chinese hospitalized patients: A prospective, nationwide, multicenter study. J. Am. Coll. Nutr. 36, 357–363 (2017).
Lee, Y. T. et al. Artificial Intelligence-Enabled electrocardiography detects hypoalbuminemia and identifies the mechanism of hepatorenal and cardiovascular events. Front. Cardiovasc. Med. 9, 895201 (2022).
Manolis, A. A., Manolis, T. A., Melita, H., Mikhailidis, D. P. & Manolis, A. S. Low serum albumin: A neglected predictor in patients with cardiovascular disease. Eur. J. Intern. Med. 102, 24–39 (2022).
Fleisher, T. A. & Oliveira, J. B. Functional and molecular evaluation of lymphocytes. J Allergy Clin Immunol 114, 227–234; quiz 235 (2004).
Cronkite, D. A. & Strutt, T. M. The Regulation of Inflammation by Innate and Adaptive Lymphocytes. J Immunol Res 1467538 (2018). (2018).
Amersfoort, J., Eelen, G. & Carmeliet, P. Immunomodulation by endothelial cells - partnering up with the immune system? Nat. Rev. Immunol. 22, 576–588 (2022).
Pepys, M. B. & Hirschfield, G. M. C-reactive protein: a critical update. J. Clin. Invest. 111, 1805–1812 (2003).
Tzoulaki, I. et al. C-reactive protein, interleukin-6, and soluble adhesion molecules as predictors of progressive peripheral atherosclerosis in the general population: Edinburgh artery study. Circulation 112, 976–983 (2005).
Ridker, P. M., Cushman, M., Stampfer, M. J., Tracy, R. P. & Hennekens, C. H. Plasma concentration of C-reactive protein and risk of developing peripheral vascular disease. Circulation 97, 425–428 (1998).
Vainas, T. et al. C-reactive protein in peripheral arterial disease: relation to severity of the disease and to future cardiovascular events. J. Vasc Surg. 42, 243–251 (2005).
Mukherjee, D. & Eagle, K. The importance of early diagnosis and treatment in peripheral arterial disease: insights from the PARTNERS and REACH registries. Curr. Vasc Pharmacol. 8, 293–300 (2010).
Kohlman-Trigoboff, D. Updates and advances in cardiovascular nursing: peripheral arterial disease. Nurs. Clin. North. Am. 58, 337–356 (2023).
Li, L. G. & Ma, X. Early identification and treatment for peripheral arterial disease in patients with ischemic cerebrovascular disease. Eur. J. Med. Res. 28, 93 (2023).
Zia-Ur-Rehman & Ram, N. Peripheral arterial disease (PAD) in diabetics: diagnosis and management- a narrative review. J. Pak Med. Assoc. 73, 621–626 (2023).
Funding
This study was supported by the Shandong Provincial Natural Science Foundation Innovation and Development Joint Fund (ZR2022LZY011) and the Science and Technology Department of the State Administration of Traditional Chinese Medicine (GZY-KJS-SD-2023-046).
Author information
Authors and Affiliations
Contributions
ZW and LF led the study design and data collection. QW and CG contributed to the interpretation of the results. BW contributed to the manuscript writing. XL and WL responsible for revising and verifying the article. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics
The original NHANES research data were collected after obtaining informed consent from all participants, with ethical approval from the NCHS Institutional Review Board. Secondary analysis of publicly available data does not require ethical approval.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wu, Z., Fu, L., Liu, X. et al. The relationship between C-reactive protein-albumin-lymphocyte index and peripheral artery disease. Sci Rep 15, 24380 (2025). https://doi.org/10.1038/s41598-025-09898-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-09898-9
Keywords
This article is cited by
-
Evaluation of the C-reactive protein–albumin–lymphocyte (CALLY) index as a prognostic marker in patients with sepsis
BMC Emergency Medicine (2025)
