
Abstract
While extensive research has compared ICSI and c-IVF in general ART outcomes, limited evidence exists regarding their relative efficacy and safety in PGT-A cycles. Therefore, we conducted a large retrospective cohort study to evaluate the effect of conventional in vitro fertilization (c-IVF) on the outcomes of preimplantation genetic testing for aneuploidy (PGT-A) in couples with non-male factor infertility. We conducted a large retrospective cohort study including 578 PGT-A cycles with c-IVF performed on couples with non-male factor infertility at our center between January 2019 and October 2024. To control for confounding factors, 578 PGT-A cycles with ICSI during the same period were selected as a control group. Matching was based on maternal age (± 2 years), number of oocytes retrieved (± 3), and progressive motile sperm count (± 3 × 106). The primary outcome was PGT-A results, while secondary outcomes included the 2PN fertilization rate, blastocyst available for biopsy per 2PN zygote and blastocyst available for biopsy per oocyte retrieved. Baseline characteristics, including parental age, AMH, antral follicle count (AFC), BMI, progressive motile sperm count, and PGT indications, were comparable between groups. Although the 2PN fertilization rate was significantly higher in the ICSI-PGT-A group (65.88% vs. 78.46%, P < 0.001), the 2 PN fertilization rate per retrieved oocyte (65.88% vs. 60.48%, P < 0.001), transferable embryo rate on day 3 (76.67% vs. 74.38%, P = 0.029), blastocyst formation rate per 2PN zygote (51.54% vs. 48.32%, P = 0.008), blastocyst available for biopsy per 2PN zygote (35.60% vs. 29.46%, P < 0.001), and blastocyst available for biopsy per oocyte retrieved (23.45% vs. 17.82%, P < 0.001) were significantly lower in the ICSI-PGT-A group. PGT-A results from 1,268 biopsy samples in the c-IVF group and 936 samples in the ICSI group revealed no significant differences in chromosomal euploidy, aneuploidy, mosaicism, or “No-call” rates. However, after controlling the potential confounders, c-IVF demonstrated significantly higher euploid embryo rate compared to ICSI (adjusted RR = 1.611, 95% CI 1.228–2.114, P = 0.001). Patterns of chromosomal aberrations were similar between groups, with chromosomes 15, 16, 21, and 22 showing the highest frequencies of abnormalities. Notably, no parental contamination was detected in the c-IVF group, while one case of maternal contamination was reported in the ICSI group. Our data suggested c-IVF could improve PGT-A outcomes in couples with non-male factor infertility and exhibited a low risk of parental contamination. c-IVF-PGT-A represents a safe, effective, and cost-efficient strategy for these couples.
Similar content being viewed by others

Introduction
Preimplantation genetic testing for aneuploidy (PGT-A) has emerged as a critical tool in assisted reproductive technology (ART), facilitating the selection of euploid embryos to enhance implantation rates and reduce the risk of miscarriage. Traditionally, intracytoplasmic sperm injection (ICSI) has been the only preferred fertilization method for PGT-A, based on the assumption that it minimizes the risk of sperm DNA contamination in biopsy samples1. However, with advancements in embryonic genetic testing technologies, studies have reported that the impact of sperm DNA contamination on PGT-A outcomes is negligible2,3,4. In addition, ICSI is associated with several concerns, including potential mechanical damage to oocyte, increased risk of technical errors and the introduction of paternal genetic abnormalities that might otherwise be eliminated by natural sperm selection5. Furthermore, ICSI requires specialized equipment and expertise, which contributes to increased costs and limits its accessibility in resource-constrained settings. These challenges have spurred growing interest in conventional in vitro fertilization (c-IVF) as an alternative for PGT-A, as it more closely resembles the natural fertilization process.
Over the past decades, the utilization of ICSI has risen substantially. According to the 2024 report by the International Committee for Monitoring Assisted Reproductive Technology (ICMART), approximately 72% of ART cycles in Europe in 2016 utilized ICSI6 even among couples without male-factor infertility. This trend highlights a significant shift in clinical practice, yet the benefits of ICSI over c-IVF in couples with non-male factor infertility remain a topic of ongoing debate. A meta-analysis published in 2024 demonstrated that c-IVF achieved comparable live birth rates and fertilization rates per oocyte retrieved compared to ICSI in non-male factor infertility7. Interestingly, a large meta-analysis by De Bantel-Finet et al., encompassing 21 studies and nearly one million ART cycles, found that c-IVF was associated with a significantly higher live birth rate per cycle compared to ICSI in couples with non-male factor infertility (RR: 1.10; 95% CI 1.02–1.18)8.
While extensive research has compared ICSI and c-IVF in general ART outcomes, limited evidence exists regarding their relative efficacy and safety in PGT-A cycles. Retrospective cohort studies investigating the impact of fertilization methods on aneuploidy rates in PGT-A have yielded conflicting findings. Some studies suggest higher rates of aneuploidy in embryos derived from ICSI9,10 whereas others report no significant differences11,12. Additionally, it remains unclear whether fertilization methods influence the incidence of aneuploidy in specific chromosomal pairs. To address these gaps, we conducted a large retrospective cohort study to compare the efficacy and safety of c-IVF and ICSI in PGT-A cycles for couples with non-male factor infertility. This study aims to provide further insights into the role of fertilization methods in ART outcomes and inform clinical decision-making in the context of PGT-A.
Methods
Study population
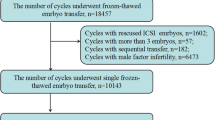
The study group comprised 578 PGT-A cycles performed with conventional in vitro fertilization (c-IVF) in patients diagnosed with non-male factor infertility. To ensure comparability and control for potential confounding variables, a matched control group was established, consisting of 578 PGT-A cycles conducted with intracytoplasmic sperm injection (ICSI) during the same period. Matching criteria included maternal age (± 2 years), the number of oocytes retrieved (± 3), and the number of progressively motile sperm (PR; ± 3 × 106).
We conducted a large retrospective cohort study at the Reproductive Medicine Center of the Sixth Affiliated Hospital of Sun Yat-sen University from January 2019 to October 2024. The study group comprised 578 PGT-A cycles performed with c-IVF) in patients with non-male factor infertility. To ensure comparability and control for potential confounding variables, a matched control group was established, consisting of 578 PGT-A cycles conducted with ICSI in patients with non-male factor infertility during the same period. Matching criteria included maternal age (± 2 years), the number of oocytes retrieved (± 3), and the number of progressively motile sperm (PR; ±3 × 106).
The indications for PGT-A included advanced maternal age (≥ 38 years), recurrent miscarriage (≥ 3 miscarriages or ≥ 2 miscarriages with at least one associated with chromosomal abnormalities), and repeated implantation failure (defined as ≥ 3 transfers of high-quality embryos or ≥ 10 transferable embryos without successful implantation).Exclusion criteria were as follows: (1) sperm parameters not meeting standard thresholds (concentration ≥ 15 × 106/mL, progressive motility ≥ 32%, or strict morphology ≥ 4% normal forms), (2) presence of chromosomal rearrangements or single-gene disorders, (3) use of cryopreserved sperm samples, (4) previous cycles with fertilization failure or low fertilization rates (< 30%).
This study was approved by the Ethics Committee (Institutional Review Board) of the Sixth Affiliated Hospital of Sun Yat-sen University and adhered to the Declaration of Helsinki for medical research. Informed consent was obtained from all participants following comprehensive counseling on infertility treatments and routine ART procedures. All procedures were conducted in compliance with relevant guidelines and regulations.
Assisted reproductive technology procedure
The stimulation protocols and gonadotropin dosages were individualized based on patient characteristics, including age, body mass index (BMI), day 3 follicle-stimulating hormone (FSH), anti-Müllerian hormone (AMH) levels, and antral follicle count (AFC). Controlled ovarian stimulation (COS) protocols employed included the gonadotropin-releasing hormone antagonist (GnRH-A) protocol, gonadotropin-releasing hormone agonist (GnRH-a) protocol, and the progesterone priming ovarian stimulation (PPOS) protocol. When 2–3 follicles reached a diameter of 16–18 mm, 4000–10,000 IU of human chorionic gonadotropin (hCG) (Livzon Group, China) was administered intramuscularly. Oocyte retrieval was performed 34–38 h later under transvaginal ultrasound guidance.
The fertilization method was determined by the attending physician. On the day of oocyte retrieval, sperm samples were collected via masturbation, liquefied at room temperature, and processed using density gradient centrifugation. In the c-IVF group, cumulus-oocyte complexes (COCs) were co-incubated with sperm in G-IVF PLUS medium (Vitrolife, Sweden). After 16–19 h, cumulus cells were completely removed from inseminated oocytes to evaluate fertilization. For ICSI group, cumulus stripping was performed 2–4 h post-retrieval by gentle pipetting to assess oocyte maturity. Only mature oocytes at the metaphase II (MII) stage, identified by the presence of a first polar body, were selected for ICSI. Fertilization assessment was conducted 16–19 h after insemination. The presence of two pronuclei and two polar bodies was considered indicative of normal fertilization.
Embryos were then cultured in G1/G2 sequential media (Vitrolife, Sweden) at 37 °C in incubators with 6% CO₂ and monitored until days 5–6 post-ovulation. Blastocyst quality was evaluated using the Gardner grading system: grades AA, AB, and BA were classified as good quality; BB as fair quality; and AC, BC, and CB as poor quality. Blastocysts deemed suitable for transfer underwent trophectoderm (TE) cell biopsy following established methods. Approximately 5–10 TE cells were aspirated, and the biopsied blastocysts were vitrified following the manufacturer’s instructions (VT101, Kitazato).
Preimplantation genetic testing for aneuploidy
Biopsied trophectoderm cells were transferred into RNase- and DNase-free PCR tubes containing 5 µL of cell lysis buffer (XK043, Yikon Genomics, China). Whole genome amplification (WGA) was performed using the multiple annealing and looping-based amplification cycles (MALBAC) method. The amplified products were subjected to copy number variant (CNV) analysis following a previously described protocol13. CNV library fragments were enriched using the Universal DNA Fragmentation Kit (Yikon Genomics, China), and the library was constructed accordingly. High-throughput sequencing was performed on the Illumina NextSeq 550 platform. For each sample, 3 million reads were generated for ICSI samples, while about 30 million reads were generated for c-IVF samples. Ploidy status was determined based on CNV profiles, with mosaicism thresholds set at 30–70%. Samples with mosaicism levels below 30% were classified as euploid, while those exceeding 70% were categorized as aneuploid. Aneuploid embryos with a single abnormal chromosome were classified as simple aneuploidy, those with two abnormal chromosomes as double aneuploidy, and those with three or more abnormal chromosomes as complex aneuploidy.
Quality control in PGT-A data analysis
Raw sequencing data were aligned to the reference genome, which was divided into contiguous 400-Kb bins with 200-Kb overlaps. Quality control metrics included as following: (1) MAPD (Median of the Absolute Pairwise Difference), calculated as the median of absolute differences between adjacent bin values (MAPD = median(|Xi + 1 - Xi|), where “i” denotes the genomic position); (2) Bin CV, the coefficient of variation (CV) of read ratios (RR) across all bins on each chromosome, represented as the median of CV across all chromosomes, calculated as median (each chromosome RR standard deviation / each chromosome RR mean); (3) CNV Merge CV, the CV of CNV segment-level variation across chromosomes, calculated as CNV segment standard deviation / CNV segment mean; (4) CNV pq, the CV of CNV variation across chromosomal arms, defined as the standard deviation of whole-arm CNV / mean of whole-arm CNV. Samples were deemed to have failed quality control if MAPD ≥ 0.25 or Bin CV ≥ 0.20, and simultaneously CNV Merge CV ≥ 0.20 or CNV pq ≥ 0.15, resulting in a “no call.”
Parental contamination testing
Single nucleotide polymorphism (SNP) loci with alleles A and B were analyzed using B allele frequency (BAF). The BAF distributions for diploid, triploid, and haploid samples should be approximately [0.0, 0.5, 1.0], [0.0, 0.33, 0.66, 1.0], and [0.0, 1.0], respectively. A significant deviation from these expected distributions indicates contamination. Maternal contamination typically shifts the BAF of embryo samples toward the maternal genotype, causing heterozygous SNPs, expected to have a BAF of 0.5, to deviate closer to 0 or 1. In contrast, paternal contamination results in a shift in the opposite direction, causing heterozygous SNPs to exhibit an opposite bias.
Study outcomes
The primary outcomes included the rates of euploidy, aneuploidy, mosaicism and contamination per biopsy in c-IVF versus ICSI group. Secondary outcomes comprised 2PN rate per retrieved oocyte, blastocyst available for biopsy per 2PN zygotes, rates of aneuploidy subtype (simple, double, or complex) and patterns of chromosomal aberrations.
Statistics
Continuous data were shown as mean ± standard deviation [SD] for normally distributed data and median (interquartile range) for non-normally distributed data. Categorical data were presented as percentage (the number of cases). Continuous variables were compared using Student’s t-test or Wilcoxon signed ranks test when appropriate, and categorical variables were compared using the chi-square test. Negative Binomial Regression Analysis, selected based on the over-dispersed count data distribution of euploid embryos with deviance-to-degrees-of-freedom ratio = 2.684, was employed to assess associations between clinical factors and euploidy rate. In this analysis, the dependent variable was defined as the count of euploid embryos, with the logarithm of the total number of biopsied embryos serving as an offset to account for variations in sample size. All analyses were performed using SPSS software (version 25.0; IBM Corp., Armonk, NY, USA). A two-tailed P-value < 0.05 was considered as statistical significance.
Results
This retrospective analysis study included 1156 PGT-A cycles in total. The demographic and baseline characteristics of eligible patients were summarized in Table 1. No significant differences were observed between the c-IVF and ICSI groups in terms of maternal age, parental age, AMH, AFC, BMI and numbers of PR sperm. Mean maternal age was 39.11 ± 3.85 years in c-IVF group and 39.31 ± 3.89 years in ICSI group, respectively. Most patients in both groups were diagnosed as secondary infertility. Overall, the primary indications for PGT-A were recurrent pregnancy loss and advanced maternal age, with repeated implantation failure also being a notable factor (11.07–12.63%).
As shown in Table 2, the constituent ratio of stimulation protocols was similar between the two groups with the PPOS protocol being the most frequently used, accounting for 62.98% of cycles in the c-IVF group and 63.67% in the ICSI group. While no in-between group difference was observed in the number of oocytes retrieved (9.35 ± 5.96vs. 9.09 ± 6.02, P = 0.45), patients yielded significantly higher 2PN fertilization rate per oocytes retrieved (65.88% vs. 60.48%, P < 0.001) and blastocyst available for biopsy per oocyte retrieve (23.45% vs. 17.82%, P < 0.001) in the c-IVF group. Moreover, while the 2PN fertilization rate per inseminated oocyte in the ICSI group was higher compared to the c-IVF group (78.46% vs. 65.88%, P < 0.001), the c-IVF group showed superior outcomes in several other parameters, including transferrable embryo rate (74.38% vs. 76.67%, P = 0.029), blastocyst formation rate per 2PN zygote (48.32% vs. 51.54%, P = 0.008) and blastocyst available for biopsy per 2PN zygote (29.46% vs. 35.60%, P < 0.001) (Table 3).
As summarized in Table 3, no significant differences were observed between the two groups in the following PGT-A outcomes: euploidy rate (39.98% vs. 41.56%), aneuploidy rate (47.56% vs. 45.30%), mosaicism rate (12.22% vs. 12.50%), or "No-call" rate (0.24% vs. 0.53%). Similarly, the distribution of aneuploidy types, including single, double and complex aneuploidy were comparable. Notably, no parental contamination was detected in the c-IVF group, whereas one case of maternal contamination was identified in the ICSI group. In terms of euploidy rates per oocyte retrieved, we found that this rate was significantly higher in the c-IVF group compared to the ICSI group (9.38% vs. 7.41%, P < 0.001), with a statistically significant difference noted.
To further elucidate the impact of insemination techniques on euploidy rates, we performed a multivariate analysis incorporating the number of biopsied embryos (as an offset term) and potential confounding factors, as outlined in Table 4. After controlling for these potential confounders, c-IVF demonstrated a significantly higher euploid embryo rate compared to ICSI (adjusted PR = 1.611, 95% CI 1.228–2.114, P = 0.001).
To assess the potential impact of fertilization methods on chromosomal aberration patterns, aneuploidy data were summarized in Fig. 1. The chromosomal pairs implicated in abnormalities, involving both autosomes and sex chromosomes, were similar between the two groups (P = 0.561), with chromosomes 15, 16, 21, and 22 showing the highest frequencies of aberrations.

Percentage of aneuploidies affecting each chromosome. Data are from 1027 blastocysts.
Discussion
The impact of c-IVF on the outcomes of PGT-A in couples with non-male factor infertility is still uncertain due to limited evidence. In this large retrospective study, we demonstrated that c-IVF resulted in significantly better embryological outcomes, with more blastocysts available for biopsy compared to ICSI. Furthermore, the two fertilization methods yielded similar PGT-A results, including comparable euploidy rates and analogous spectrums of chromosomal abnormalities, involving both autosomes and sex chromosomes. Importantly, c-IVF didn’t increase the risk of parental contamination under the conditions employed in our laboratory. Collectively, these findings suggest that c-IVF provides advantages over ICSI in the context of PGT-A for couples with non-male factor infertility.
ICSI has been widely used as an assisted reproductive technique in severe male infertility since its introduction in the 1990s14. However, its application has expanded significantly, even to cases without male factor infertility. Reports showed dramatically increase in the proportion of ICSI cycles in non-male factor infertility in European countries6,15. Despite this trend, most studies suggest that ICSI fails to confer advantages in couples with non-male factor infertility. Bhattacharya et al.16 conducted a randomized trial involving 415 patients with non-male factor infertility and observed a significantly lower fertilization rate per oocyte retrieved in the ICSI (47% vs. 58%), which was in line with our findings. They also reported significantly lower clinical pregnancy rate in ICSI group. Similarly, Shoukir et al.17 found that blastocyst formulation rate was significantly higher in IVF-derived embryos (47.3% vs. 26.8%). Other studies have demonstrated superior outcomes in c-IVF, including higher high-quality blastulation rates18 better embryo quality, and more cycles with embryos available for cryopreservation19. In this study, we discovered that, although ICSI increased the 2pn rate per inseminated oocyte, the c-IVF group yielded a significantly higher 2PN fertilization rate per oocyte and more blastocyst for biopsy. The poorer embryological outcomes associated with ICSI may be explained by several factors. Firstly, ICSI bypasses the natural sperm selection process, potentially increasing the risk of fertilization with defective spermatozoa20 thereby affecting embryo quality. Second, c-IVF allows immature oocytes to complete maturation in culture and subsequently undergo fertilization, whereas ICSI only utilizes mature oocytes for insemination. Consequently, ICSI may result in the loss of oocytes with developmental potential. Third, c-IVF preserves cumulus-oocyte interactions, which may enhance developmental potential21. Last but not least, damage from the ICSI procedure itself, such as mechanical injury, introduction of unwanted material during the ICSI process or exposure to various synthetic media22 might compromised embryo development potential.
The potential for parental contamination has been a critical concern in the application of c-IVF for PGT-A. Historically, ICSI has been preferred for PGT-A to mitigate contamination risks. Regarding paternal contamination from sperm DNA, recent advancements in DNA amplification techniques have demonstrated their capability to minimize the amplification of tightly packed sperm DNA, rendering the risk of sperm contamination negligible2,23. The DNA amplification method utilized in this study aligns with the approach described by Dong et al.4, which confirmed that sperm DNA could be rendered entirely non-amplifiable. Consistent with these findings, no cases of paternal contamination were identified in the c-IVF group in our study. Maternal contamination, primarily originating from cumulus granulosa cells, poses a challenge in both c-IVF and ICSI. The DNA from cumulus granulosa cells is readily amplifiable, making their thorough removal a critical step in minimizing contamination risks. In our center, embryologists perform meticulous removal of cumulus granulosa cells prior to ICSI or on Day 1 following insemination in c-IVF cycles. This procedural rigor is essential to reducing maternal contamination and ensuring the accuracy of PGT results. Furthermore, the parental contamination testing adopted in our center has been reported as a sensitive and reliable method for detecting and quantifying maternal contamination4 further enhancing the reliability of PGT outcomes. In line with previous studies2,10,23,24 our results demonstrated no maternal contamination in embryos from the c-IVF group. In contrast, one instance of maternal contamination was observed in the ICSI group, which was attributed to residual cumulus granulosa cells. These findings suggest that c-IVF, when performed under optimized laboratory conditions, presents a low risk of parental contamination, comparable to that of ICSI.
The impact of c-IVF on PGT outcomes remains a critical focus of current research, as existing literature reports inconsistent findings. Most studies evaluating c-IVF vs. ICSI in PGT program have demonstrated similar rates of euploidy, aneuploidy, and mosaicism rate between the two insemination methods2,11,12,23,24. Although Palmerola et al.11 hypothesized that c-IVF might lead to an increase in mosaic cells compared to ICSI, the difference didn’t reach statistical significance and it remains ambiguous whether this was attributed to sample contamination. Conversely, Patel K et al.25. performed a large-sample retrospective analysis in 2023 and reported a significantly higher aneuploidy rate in embryos derived from ICSI. The authors attributed this finding to the possible introduction of abnormal spermatozoa during the ICSI process, which may adversely affect chromosomal integrity. In alignment with the majority of prior investigations, our initial unadjusted analysis demonstrated comparable embryo euploidy rates between the c-IVF and ICSI groups. However, subsequent multivariate modeling incorporating adjustments for the number of biopsied embryos (offset term) and rigorous control of key confounders - including maternal age, ovarian reserve biomarkers and so on, revealed statistically significant increase in euploid embryo likelihood with c-IVF compared to ICSI. This finding implied that IVF may confer a distinct advantage in optimizing euploid embryo yield for non-male factor infertility populations. Notably, we further demonstrated a comparable constitution of different aneuploidy types and identified a similar spectrum of chromosomal abnormalities, which included autosomes and sex chromosomes. Some studies reported a significantly higher incidence of sex chromosome abnormalities in abortus from ICSI26–27 In our study, which exclusively included couples with non-male factor infertility, no significant differences in abnormal chromosomes profiles were observed, supporting the hypothesis that the underlying etiology of infertility plays a more critical role in chromosomal anomalies than the fertilization method employed.
Our study has several strengths. By matching for key confounding factors, such as maternal age and semen parameters, we ensured a robust comparison of c-IVF and ICSI outcomes. Moreover, we provided comprehensive analyses of embryological outcomes, chromosomal profiles, and parental contamination risks, reinforcing the reliability and safety of c-IVF in PGT-A. Nonetheless, the retrospective nature of our study introduces potential confounding factors and biases. Further prospective, randomized controlled trials are warranted to validate our findings and elucidate the underlying mechanisms.
Conclusions
Despite the inherent limitations of its retrospective design, this study provides evidence suggesting that c-IVF has a favorable impact on PGT-A outcomes in couples with non-male factor infertility. Our findings support c-IVF as a safe, effective, and cost-efficient fertilization method in this patient population. Importantly, the outcomes of PGT-A are influenced by a multitude of factors, including genetic testing platforms, embryological practices, and biopsy techniques. As such, the generalizability of our findings requires further validation through multicenter studies and data integration from diverse genetic laboratories.
Data availability
The raw sequence data reported in this paper have been deposited in the Genome Sequence Archive (Genomics, Proteomics & Bioinformatics 2021) in the National Genomics Data Center (Nucleic Acids Res 2024), China National Center for Bioinformation / Beijing Institute of Genomics, Chinese Academy of Sciences (GSA-Human: HRA010479), and are publicly accessible at https://ngdc.cncb.ac.cn/gsa-human.
References
Thornhill, A. R. et al. Best practice guidelines for clinical preimplantation genetic diagnosis (PGD) and preimplantation genetic screening (PGS). Hum. Reprod. 20, 35–48 (2005).
Lynch, C. et al. Intracytoplasmic sperm injection is not necessary as a preventive measure against paternal cell contamination in preimplantation genetic testing. Reprod. Biomed. Online. 39, e24–e25 (2019).
Bo, L. et al. A method for determining potential parental contamination: Linkage disequilibrium-based log-likelihood ratio analysis for IVF-PGT. Reprod. Biol. Endocrinol. 22, 1–12 (2024).
Dong, Y. et al. Preimplantation genetic testing for human blastocysts with potential parental contamination using a quantitative parental contamination test (qPCT): An evidence-based study. Reprod. Biomed. Online. 46, 69–79 (2023).
Neelke, D. M. et al. Intracytoplasmic sperm injection is not superior to conventional IVF in couples with non-male factor infertility and preimplantation genetic testing for aneuploidies (PGT-A). Hum. Reprod. 35, 317–327 (2020).
Kupka, M. S. et al. International committee for monitoring assisted reproductive technology world report: Assisted reproductive technology, 2015 and 2016. Fertil. Steril. 122, 875–893 (2024).
Yang, L. et al. Efficacy of intracytoplasmic sperm injection in women with non-male factor infertility: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 103, (2024).
Bantel-Finet, A. D. et al. Does intracytoplasmic sperm injection improve live birth rate when compared with conventional in vitro fertilization in non-male factor infertility? A systematic review and meta-analysis. F&S Rev. 3, 57–68 (2022).
Patel, K., Vaughan, D. A., Rodday, A. M., Penzias, A. & Sakkas, D. Compared with conventional insemination, intracytoplasmic sperm injection provides no benefit in cases of nonmale factor infertility as evidenced by comparable euploidy rate. Fertil. Steril. 120, 277–286 (2023).
Swearman, H. K. et al. Fertilization by ICSI results in significantly higher aneuploidy rates compared to IVF, in embryos analysed by next-generation sequencing (NGS) or comparative genome hybridization (CGH) array. Fertil. Steril. 110, e346–e347 (2018).
Palmerola, K. L. et al. Minimizing mosaicism: Assessing the impact of fertilization method on rate of mosaicism after next-generation sequencing (NGS) preimplantation genetic testing for aneuploidy (PGT-A). J. Assist. Reprod. Genet. 36, 153–157 (2019).
Deng, J. et al. Comparison of Aneuploidy Rates between Conventional in Vitro Fertilization (IVF) and Intracytoplasmic Sperm Injection (ICSI) in IVF-ICSI Split Insemination Cycles (F&S Rep, 2020).
Liu, W. et al. The performance of MALBAC and MDA methods in the identification of concurrent mutations and aneuploidy screening to diagnose beta-thalassaemia disorders at the single- and multiple-cell levels. J. Clin. Lab. Anal. 32, (2018).
Palermo, G., Joris, H., Devroey, P. & Van Steirteghem, A. C. Pregnancies after intracytoplasmic injection of single spermatozoon into an oocyte. Lancet 340, 17–18 (1992).
de Mouzon, J. et al. International committee for monitoring assisted reproductive technologies world report: Assisted reproductive technology 2012. Hum. Reprod. 35, 1900–1913 (2020).
Bhattacharya, S. et al. Conventional in-vitro fertilisation versus intracytoplasmic sperm injection for the treatment of non-male-factor infertility: A randomised controlled trial. Lancet 357, 2075–2079 (2001).
Shoukir, Y., Chardonnens, D., Campana, A. & Sakkas, D. Blastocyst development from supernumerary embryos after intracytoplasmic sperm injection: A paternal influence? Hum. Reprod. 13, 1632–1637 (1998).
Sauerbrun-Cutler, M. T. et al. Is intracytoplasmic sperm injection (ICSI) better than traditional in vitro fertilization (IVF): Confirmation of higher blastocyst rates per oocyte using a split insemination design. J. Assist. Reprod. Genet. 37, 1661–1667 (2020).
Tannus, S. et al. The role of intracytoplasmic sperm injection in non-male factor infertility in advanced maternal age. Hum. Reprod. 32, 119–124 (2017).
Oseguera-Lopez, I., Ruiz-Díaz, S., Ramos-Ibeas, P. & Perez-Cerezales, S. Novel techniques of sperm selection for improving IVF and ICSI outcomes. Front. Cell. Dev. Biol. 7, 298 (2019).
McPherson, N. O., Vincent, A. D., Pacella-Ince, L. & Tremellen, K. Comparison of in vitro fertilisation/intracytoplasmic sperm injection on live birth rates in couples with non-male factor infertility and advanced maternal age. J. Assist. Reprod. Genet. 38, 669–678 (2021).
Sustar, K. et al. Use of intracytoplasmic sperm injection (ICSI) in normospermic men May result in lower clinical pregnancy and live birth rates. Aust. N. Z. J. Obstet. Gynaecol. 59, 706–711 (2019).
De Munck, N., Khatib, E. & Abdala, I. Intracytoplasmic sperm injection is not superior to conventional IVF in couples with non-male factor infertility and preimplantation genetic testing for aneuploidies (PGT-A). Hum. Reprod. 35, 317–327 (2020).
Feldman, B. et al. Pre-implantation genetic diagnosis—Should we use ICSI for all? J. Assist. Reprod. Genet. 34, 1179–1183 (2017).
Kim, J. W. et al. Chromosomal abnormalities in spontaneous abortion after assisted reproductive treatment. BMC Med. Genet. 11, 153 (2010).
Kushnir, J. L. Aneuploidy in abortuses following IVF and ICSI. J. Assist. Reprod. Genet. 26, 93–97 (2009).
Acknowledgements
I would like to gratefully acknowledge all participants for their significant contributions to this work.
Funding
This work was supported by the Science and Technology Projects in Guangzhou (Grant No. 2023A04J2243).
Author information
Authors and Affiliations
Contributions
XL, XL and ZZ raised the question and developed design of the study and all authors contributed to the research discussion. XL, QL, YC, SH and YW participated in patient follow-up, data collection and contributed to the data analysis. XL wrote the initial manuscript and all authors contributed to the revised revision. All authors contributed to this article and approved the submitted version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics statement
The study protocol was approved by the Ethics Committee (Institutional Review Board) of the sixth affiliated hospital of Sun-Yet san university. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, X., Li, Q., Chang, Y. et al. Conventional in vitro fertilization enhances preimplantation genetic testing for aneuploidy outcomes in couples with non-male factor infertility. Sci Rep 15, 24904 (2025). https://doi.org/10.1038/s41598-025-10300-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-10300-x
