
Abstract
Advances in biologic and targeted synthetic DMARDs have expanded treatment options for spondylarthritis. Despite improvements with TNF inhibitors, many patients remain refractory. Secukinumab, an IL-17A inhibitor, has shown promise in controlled trials. This study evaluates its real-world retention, efficacy, and safety in a Polish cohort. We conducted a retrospective analysis using electronic records from the largest biological treatment center in Poland. Adult patients (≥ 18 years) who initiated secukinumab therapy under the National Health Fund program between November 2018 and October 2024 were included. Primary outcomes were overall drug survival and treatment response at 90 and 180 days. Among 279 patients (139 psoriatic arthritis, 112 ankylosing spondylitis, 28 non-radiographic spondylarthritis; median follow-up 23 months), treatment response rates were 88.2% at 3 months and 88.9% at 6 months, with significant improvements in all evaluated parameters. One-year drug survival was 87%, declining to 59% at 58 months. Dose escalation to 300 mg/month was required in 32.9% of patients, with most (77%) showing subsequent benefit. The risk factor for treatment failure was enthesitis (OR 2.2 95% CI 1.05–4.62), while the factor favoring continuing secukinumab therapy was dactylitis (OR 14.69 95% CI 1.88–114.69). Secukinumab demonstrated robust real-world efficacy, safety, and retention in spondylarthritis patients, supporting its role as an effective treatment.
Similar content being viewed by others

Introduction
The treatment options for spondylarthritis (SpA) patients have improved during the last years with the introduction of biologic disease-modifying antirheumatic drugs (bDMARDs) and targeted synthetic DMARDs (tsDMARDs). The first approved group of bDMARDs, TNF inhibitors (TNFi), although improved patients’ treatment options, still left unmet needs for a significant proportion of patients. Data from European registries show that only about half of PsA1 and one-third of axSpA2 patients achieve remission during TNFi treatment.
In recent years, interleukin-17 inhibitors, have become an alternative treatment to TNFi in SpA patients, also as a first-line bDMARD per EULAR guidelines3,4. The pro-inflammatory cytokine IL-17A plays a key role in the pathogenesis of SpA5. As a result, secukinumab, a fully human IgG1 monoclonal antibody targeting interleukin-17A, was approved for use in PsA patients in the European Union in 2015. Under the Polish National Health Fund drug program, secukinumab has been reimbursed for the AS and PsA patients since November 2018, and for the patients with nrSpA since July 2022. Secukinumab has demonstrated good efficacy and safety in randomized controlled trials (RCTs) for all SpA indications—ankylosing spondylitis (AS)6, psoriatic arthritis (PsA)7, as well as non-radiographic spondylarthritis (nrSpA)8.
While RCTs are regarded as the gold standard for assessing efficacy, their findings may not fully generalize to patients in routine clinical practice. This limitation arises from the intrinsic heterogeneity of real-world patient populations, which include a wide spectrum of comorbidities and concurrent pharmacotherapies. Everyday clinical practice is better reflected by long-term, real-life observational studies. However, real-world data regarding secukinumab treatment outcomes are still limited. Our retrospective cohort study aimed to assess the real-life retention rate, efficacy, and safety of secukinumab in a Polish cohort of patients.
Methods
Study design
Using electronic medical records from the largest biological treatment center in Poland retrospective analysis of patients treated with secukinumab was performed. The study included all adult patients (> 18 years of age) who initiated secukinumab therapy under the National Health Fund drug program between November 2018 and October 2024.
Patients
According to National Health Fund drug program reimbursement guidelines, secukinumab treatment may be administered to patients diagnosed with AS based on the modified New York criteria9, PsA based on the CASPAR criteria10, or nrSpA based on the ASAS criteria11. In patients with the axial form of the disease, the biologic drug may be given in the case of persistent high disease activity (BASDAI ≥ 4 or ASDAS ≥ 2.1 and spinal pain ≥ 4 cm in visual-analog scale in two assessments at least 4 weeks apart) despite treatment with at least two nonsteroidal anti-inflammatory drugs (NSAID; for at least 4 weeks each, at the maximum tolerated dose). In the case of the peripheral form of the disease, the biologic drug may be prescribed if at least moderate disease activity persists (in two assessments at least 4 weeks apart) despite an attempt at treatment with at least two classic disease-modifying antirheumatic drugs (cDMARDs). Moderate disease activity is defined in the case of nrSpA and PsA in PsARC as number of tender and swollen joints and/or entheses ≥ 3 and global assessment of disease activity by the patient and physician on the Likert scale ≥ 4 and for PsA in DAS28 as value > 3.2. According to the provisions of the drug program, patients may receive secukinumab at a dose of 150 mg or 300 mg in the case of previous ineffective TNFi treatment and the case of severe PsA psoriasis.
Outcomes and safety assessment
Primary outcomes were drug survival (time from secukinumab initiation to discontinuation of the drug for any reason or loss of follow-up) and treatment response after 90 and 180 days. Treatment response was defined according to the National Health Fund drug program. After 90 days patients were classified as responders if they achieved at least moderate disease activity measured by the DAS28 ≤ 5.1 or, in the case of PsARC assessment, a reduction of at least 30% compared to the baseline in the total number of affected joints and entheses (taking into account the Achilles tendons and plantar fasciae) and a reduction in disease activity on the Likert scale by at least one unit, both in the assessment of the patient and the physician or, in the case of axial disease, a reduction in the BASDAI value of ≥ 50% or ≥ 2 units. After 180 days, response to treatment was defined as achieving at least low disease activity as measured by a DAS 28 score of ≤ 3.2 or, in the case of PsARC assessment, achieving low disease activity defined as a reduction of at least 50% from the pre-treatment value in the total number of affected joints and entheses and disease activity on the Likert scale, as assessed by both the patient and the physician, or, in the case of axial disease, achieving low disease activity as measured by a BASDAI score of < 3. Secondary outcome measures included a change of BASDAI, pain VAS, DAS28, number of tender joints (of 28 in patients assessed with DAS28 or 68 in patients assessed with PsARC), number of swollen joints (of 28 and 66 respectively), physician disease activity global assessment, patient disease activity global assessment, C-reactive protein, and ESR between baseline and after 90 and 180 days.
Statistics
The compliance of the data with the normal distribution was assessed using the Shapiro–Wilk test. The significance of the observed differences between the two groups was assessed using the Student’s T test for variables with a normal distribution, the Mann–Whitney U test for variables without a normal distribution, and for categorical variables the Chi-square test or Fisher’s exact test (for tables with values less than 5). Differences between multiple dependent groups were assessed using the Friedman test (due to its nonparametric nature), with post hoc analysis with Dunn’s test. The significance of the results after adjusting for confounding factors was checked by linear regression. Logistic regression and odds ratio (OR) with 95% CI were used to identify predictive factors associated with lack of response and discontinuation of treatment due to adverse events. The probability of drug survival was estimated with a Kaplan–Mayer estimator. The difference in the probability of drug survival between groups was assessed with a Log-rank test. Statistical analysis was performed using Statistica 13.3 software (StatSoft Polska, Cracow, Poland).
Results
During the study period, 279 patients initiated secukinumab therapy. The study included 139 patients with PsA, 112 with AS, and 28 with nrSpA. Patients were observed for a total of 616.5 patient-years (median follow-up 23 months, range 3–69 months). Detailed patients characteristic is presented in Table 1 (demographics and disease characteristics) and Table 2 (current and previous biological disease treatment). A comparable number of patients had the axial and peripheral form (approx. 70% each), and over 40% had both axial and peripheral involvement. The patients were relatively young (median age 43 years), and a median of 7 years had passed from the moment of diagnosis to the start of secukinumab treatment. A comparable number of women and men (approx. 50% each) were treated with secukinumab. Despite high initial disease activity (median BASDAI 6.6, DAS28 5.3), patients had low inflammatory parameters (median CRP and ESR 5 mg/L and 12 mm/h, respectively). In almost half of the patients, the treatment was used in combination therapy with cDMARDs (48%) and in more than half with NSAIDs (58%). For 41% of patients, secukinumab treatment was a second or subsequent line of b/tsDMARD treatment. 42 patients started therapy with an increased dose of secukinumab of 300 mg—mostly (83.3%) due to previous TNFi treatment, with only a minority due to severe psoriasis (16.7%).
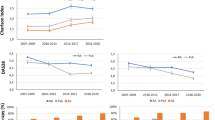
Response to treatment was achieved by 88.2% of patients after 3 months, and by 88.9% of patients after 6 months. Good response was achieved to a similar extent in all patients, irrespective of the disease activity scale used for measurement of response, disease type, and diagnosis (Supp Table 1). A statistically significant decrease in disease activity was observed both after 90 and 180 days compared to baseline according to all the indicators and inflammation parameters used (Fig. 1). Additionally, statistically significant improvements at 180 days compared to after 90 days were observed for BASDAI, number of tender joints, pain, and patient and physician global assessment. In 32.9% of patients, the secukinumab dose was increased to 300 mg/month to improve efficacy, on average after 7 months (median). Among 76.7% of dose-escalated individuals, this strategy allowed treatment retention. Logistic regression did not identify any factors favoring the need to increase the dose of secukinumab. Patients who did not achieve a response after 3 months had a longer time between the start of secukinumab treatment and diagnosis of SpA, more often had a non-radiographic form of SpA, higher BASDAI, ESR, VAS, and higher number of tender and swollen joints at the baseline, and were more often treated with b/tsDMARDs in the past (Supp Table 2). Those who did not achieve a response after 6 months of treatment only had a higher number of swollen joints at the baseline (Supp Table 3). However, after multivariate analysis (using logistic regression) none of the risk factors for lack of response to treatment at 3 and 6 months remained statistically significant.

Decrease in disease activity following secukinumab treatment. Differences between groups were assessed using the Friedman test, with post hoc analysis with Dunn’s test. * difference compared to baseline p = 0.001, † difference compared to after 90 days p = 0.001, †† difference compared to after 90 days p = 0.04. BASDAI Bath Ankylosing Spondylitis.
Secukinumab showed a good probability of drug survival over the whole observation period, with the estimated probability of drug survival after 12 months at 87%, after 24 months at 80%, falling after 58 months to 59% as shown in Fig. 2. The main reasons for drug discontinuation were ineffectiveness in 66.7% of patients (in 14 patients primary and 30 patients secondary ineffectiveness) and adverse events (27.3%, mostly infections). Detailed data on the reasons for discontinuation of treatment are presented in Table 3. The risk factor as assessed by logistic regression for treatment failure (discontinuation due to ineffectiveness) was enthesitis (OR 2.2 95% CI 1.05–4.62) and for continuing secukinumab therapy favoring factor was dactylitis (OR 14.69 95% CI 1.88–114.69). No risk factors for treatment discontinuation due to adverse events were identified.

Drug survival of secukinumab shown in Kaplan–Meier estimator.
There was no difference in drug survival probability between biologic naïve and non-naïve patients (p = 0.12; Supp Fig. 1). It is significant that of all patients treated with secukinumab, only 5% had primary treatment failure. In the group of patients previously treated with TNFi primary secukinumab treatment failure occurred in 6.7% of patients compared to primary TNFi failure observed in 55.8% (p < 0.001). A similar situation was observed in the case of secukinumab adverse events leading to treatment discontinuation, which were observed in only 6.7% of patients previously treated with TNFi, while AE leading to treatment discontinuation after TNFi in the same group occurred in 27.8% of patients (p < 0.001).
Discussion
Our study showed efficacy of secukinumab reaching 88.2% after 3 months of therapy and 88.9% after 6 months. In our study, secukinumab proved effective in the assessment after 3 and 6 months regardless of the disease, its form, and the disease activity index used. Additionally, efficacy increased between months 3 and 6 when considering BASDAI, tender joint count, and patient and physician assessments. However, these data are difficult to compare with real-world efficacy data, depending on the disease and its presentation, with different adopted treatment response indexes, at different time points in different studies. Therefore, a better indicator of the uncontrolled conditions of real life is drug survival. Drug survival depends primarily on the drug’s efficacy and the occurrence of adverse events.
Our study showed a drug survival rate of 87% at 1 year. Our data thus ranks among the studies with one of the highest drug survival of secukinumab. The reported 1-year drug survival in large cohorts of patients ranges between 59 and 63% for axSpA, 70.8 and 85.8% for AS, and 55–85.2% for PsA12,13,14,15,16,17,18,19,20,21,22. The biggest study up to date, including data from 16 European registries associated with the European Spondyloarthritis Research Collaboration Network, showed a 1-year drug survival rate of 70.8% in 3087 patients with axSpA and 74.7% in 3246 PsA patients from 14 registries12. Significant differences in retention rates across the registries were observed, e.g. 12-month retention rates in PsA patients varying from 51% (ROB-FIN) to 92% (RRBR and ATTRA)13. The described differences in drug survival are most likely due to differences between individual countries in the criteria for qualifying patients for biological treatment.
An important issue remains trying to identify factors of good and bad response to treatment, which will allow for a more personalized approach to treating patients. In our study, the risk factor for treatment failure was enthesitis, while the factor favoring continuing secukinumab therapy was dactylitis. This is partly consistent with the literature data. The factor that negatively influenced drug survival in most studies was the prior use of b/tsDMARDs12,13,16,17,21,23,24, contrary to our results, though some studies also found no differences18,19,22,25. Other risk factors for discontinuation of secukinumab mentioned in the literature include a long time since diagnosis in patients with PsA23 and axSpA25, inflammatory bowel disease in axSpA patients16, and peripheral involvement in axSpA25.
Perhaps one of the factors that allows the drug to remain effective during long-term therapy is the ability to safely increase the dose. Among our patients, as many as 32.9% increased the dose to 300 mg/month. 77% of patients with suboptimal response continued treatment after dose increase, suggesting that dose escalation was a good strategy for most patients. The literature data is not conclusive on this topic. Data from RCTs in PsA show that a dose of 300 mg compared to 150 mg provides greater efficacy, especially in patients previously treated with TNFi, with the same safety profile26. However, an RCT designed to evaluate the efficacy of increasing the dose of secukinumab in patients with AS not achieving inactive disease after 16 weeks of treatment did not show an effect of increasing the dose to 300 mg27.
The reasons for discontinuation in our study (66.7% of patients due to ineffectiveness and 27.3% due to adverse events) are comparable to the literature data in that the most common reason for discontinuation is ineffectiveness, while AE is rare. However, there is variation in the numerical values. In the 4-year follow-up of patients from European registries treated with secukinumab, the drug was discontinued due to ineffectiveness in 62% and 64% of patients with axSpA and PsA, and due to AE in 21% and 20%, respectively23. But for example, in the SERENA registry, 33.6% and 12% of AS and 38.7% and 15% of PsA patients, discontinued the drug due to ineffectiveness and AE respectively15. In our study, secukinumab proved to be safe and well-tolerated. Only 6.5% of all included in the study patients discontinued the drug due to AEs. The most common AEs leading to discontinuation of treatment were infections, which is consistent with literature data16,19,28. Interestingly, in our study, as many as two patients discontinued treatment due to malignancies. However, studies to date have not shown an increased risk of malignancies after secukinumab29. In our study, we did not identify risk factors for drug discontinuation due to AEs.
The limitation of our study is that the data came from a single center, which limited the number of patients. Unfortunately, there is no registry of rheumatology patients in Poland. However, our data come from the largest center for biological treatment in Poland. In addition, the study is subject to selection bias as in some patient groups (with uveitis or inflammatory bowel disease) other biologics are preferred over IL-17 inhibitors. This limits the generalizability of the study results to all SpA patients. The strength of our study is the long observation period (up to 69 months) and the comprehensiveness of the data from electronic medical records, which allowed us to analyze the efficacy, safety, and overall drug survival, along with the factors influencing them.
Conclusions
Our study showed good efficacy, safety, and drug survival of secukinumab in the Polish cohort of patients. Noteworthy is the very low primary ineffectiveness of secukinumab, the possibility of improving the efficacy by increasing the drug dose, maintaining high efficacy also among patients previously treated with other b/tsDMARDs, and the small number of discontinuations due to adverse events. In addition, secukinumab seems to be a particularly good option for patients with dactylitis.
Data availability
Data presented in the paper will be made available upon reasonable request sent to the corresponding author.
References
Brahe, C. H. et al. Retention and response rates in 14 261 PsA patients starting TNF inhibitor treatment-results from 12 countries in EuroSpA. Rheumatology (Oxford) 59, 1640–1650 (2020).
Ørnbjerg, L. M. et al. Treatment response and drug retention rates in 24 195 biologic-naïve patients with axial spondyloarthritis initiating TNFi treatment: Routine care data from 12 registries in the EuroSpA collaboration. Ann. Rheum. Dis. 78, 1536–1544 (2019).
Ramiro, S. et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann. Rheum. Dis. 82, 19–34 (2023).
Gossec, L. et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2023 update. Ann. Rheum. Dis. 83, 706–719 (2024).
Davydova, A., Kurochkina, Y., Goncharova, V., Vorobyeva, M. & Korolev, M. The interleukine-17 cytokine family: Role in development and progression of spondyloarthritis, current and potential therapeutic inhibitors. Biomedicines 1, 1328 (2023).
Braun, J. et al. Effect of secukinumab on clinical and radiographic outcomes in ankylosing spondylitis: 2-year results from the randomised phase III MEASURE 1 study. Ann. Rheum. Dis. 76, 1070–1077 (2017).
McInnes, I. B. et al. Secukinumab sustains improvement in signs and symptoms of psoriatic arthritis: 2 year results from the phase 3 FUTURE 2 study. Rheumatology 56, 1993 (2017).
Deodhar, A. et al. Improvement of signs and symptoms of nonradiographic axial spondyloarthritis in patients treated with secukinumab: Primary results of a randomized, placebo-controlled phase III study. Arthrit. Rheumatol. 73, 110–120 (2021).
Linden, S. V. D., Valkenburg, H. A. & Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 27, 361–368 (1984).
Taylor, W. et al. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheum. 54, 2665–2673 (2006).
Rudwaleit, M. et al. The development of assessment of spondyloarthritis international society classification criteria for axial spondyloarthritis (part II): Validation and final selection. Ann. Rheum. Dis. 68, 777–783 (2009).
Christiansen, S. N. et al. Patient-reported outcomes in axial spondyloarthritis and psoriatic arthritis patients treated with secukinumab for 24 months in daily clinical practice. Semin. Arthritis Rheum. 65, 152388 (2024).
Michelsen, B. et al. Real-world six- and twelve-month drug retention, remission, and response rates of secukinumab in 2017 patients with psoriatic arthritis in thirteen European countries. Arthritis Care Res. (Hoboken) 74, 1205–1218 (2022).
Perrone, V. et al. Analysis of the pharmacoutilization of biological drugs in psoriatic arthritis patients: A real-world retrospective study among an Italian population. Rheumatol. Ther. 9, 875–890 (2022).
Kiltz, U. et al. Interim 2-year analysis from SERENA: A real-world study in patients with psoriatic arthritis or ankylosing spondylitis treated with secukinumab. Rheumatol. Ther. 9, 1129 (2022).
Dougados, M. et al. Factors associated with the retention of secukinumab in patients with axial spondyloarthritis in real-world practice: Results from a retrospective study (FORSYA). RMD Open 9, e002802 (2023).
Geale, K. et al. Persistence of biologic treatments in psoriatic arthritis: A population-based study in Sweden. Rheumatol. Adv. Pract. 4, rkaa070 (2020).
Haddad, A. et al. Treatment persistence of biologics among patients with psoriatic arthritis. Arthritis Res. Ther. 23, 1–9 (2021).
Weddell, J. et al. Real-world experience of IL-17Ai drug survival in a large cohort of axial spondyloarthritis and psoriatic arthritis. Rheumatol. Adv. Pract. 8, rkae018 (2024).
Joven, B. et al. Real-world persistence and treatment patterns in patients with psoriatic arthritis treated with anti-IL17 therapy in Spain: The PerfIL-17 study. Adv. Ther. 40, 5415–5431 (2023).
Sivera, F. et al. Real-world experience with secukinumab in the entire axial spondyloarthritis spectrum. Front. Med. (Lausanne) 10, 1156557 (2023).
Gladman, D. D. et al. Real-World retention and clinical effectiveness of secukinumab for psoriatic arthritis: Results from the Canadian spondyloarthritis research network. J. Rheumatol. 50, 641–648 (2023).
Pons, M. et al. Four-year secukinumab treatment outcomes in European real-world patients with axial spondyloarthritis and psoriatic arthritis. Jt. Bone Spine 92, 105824 (2024).
Glintborg, B. et al. One-year treatment outcomes of secukinumab versus tumor necrosis factor inhibitors in spondyloarthritis: Results from five Nordic biologic registries including more than 10000 treatment courses. Arthritis Care Res. (Hoboken) 74, 748–758 (2022).
Ramonda, R. et al. Four-year real-world experience of secukinumab in a large Italian cohort of axial spondyloarthritis. Front. Immunol. 15, 1435599 (2024).
Zhang, K. L., Hou, S. Y. & Wu, D. Efficacy and safety of secukinumab in patients with psoriatic arthritis: A meta-analysis of different dosing regimens. Clinics (Sao Paulo) 76, e2820 (2021).
Deodhar, A. et al. A secukinumab dose-escalation study in patients with ankylosing spondylitis not achieving inactive disease after 16 weeks of treatment. Rheumatology (Oxford) 64(4), 1864–1872 (2024).
He, C., Xue, C., Zhu, G. & Kang, P. Efficacy and safety of interleukin-17 inhibitors in the treatment of chronic rheumatic diseases: A combined and updated meta-analysis. J. Clin. Pharm. Ther. 46, 895–906 (2021).
Lebwohl, M. et al. The risk of malignancy in patients with secukinumab-treated psoriasis, psoriatic arthritis and ankylosing spondylitis: Analysis of clinical trial and postmarketing surveillance data with up to 5 years of follow-up. Br. J. Dermatol. 185, 935–944 (2021).
Author information
Authors and Affiliations
Contributions
Conceptualization, AF-G and JW; methodology, AF-G and JW; validation, JW; formal analysis, JW; investigation, AF-G, MS, KP, MW-S, MŁ, SS, JW-T and JW; data curation, JW; writing—original draft preparation, AF-G and JW; writing—review and editing, MS, KP, MW-S, MŁ, SS and JW-T; visualization, JW; supervision, JW; project administration, AF-G. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was conducted in compliance with the Declaration of Helsinki. The study received ethical approval from the bioethics committee of the National Institute of Geriatrics, Rheumatology, and Rehabilitation (approval number KBT-6/2/2020). Due to the retrospective nature of the study, bioethics committee of the National Institute of Geriatrics, Rheumatology, and Rehabilitation waived the need of obtaining informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Felis-Giemza, A., Stasiek, M., Palej, K. et al. Real world efficacy safety and drug survival of secukinumab over 6 years at the largest biological center in Poland. Sci Rep 15, 25212 (2025). https://doi.org/10.1038/s41598-025-11070-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-11070-2
