
Abstract
This study aims to assess organizational resilience within medical alliances using the analytic hierarchy process (AHP) method, identify key factors, and improve their performance. It developed a model of organizational resilience factors for medical alliances, including 5 first-level sub-criteria, 15 second-level sub-criteria, and 43 third-level sub-criteria based on literature reviews and expert assessments. Nineteen experts from universities, health commissions, centers for disease control and preventions, and hospitals, including both management and technical specialists, were invited. AHP was utilized to calculate and prioritize the weights for each criterion of organizational resilience. A4 Integrated and A2 Self-regulating were identified as the key first-level sub-criteria for organizational resilience among medical alliances. In the third-level sub-criteria, the top three most important factors were C10 Leadership at the Decision-Making Level of the Medical Alliance (0.050), C29 Funds of the Medical Alliance Jointly Negotiated and Allocated by the Township Hospital and Each Branch Hospital (0.048), and C33 Integration of Medical and Preventive Services in the Medical Alliance (0.041). Sensitivity analysis was also conducted to check the stability of our results. In conclusion, this study offers a comprehensive evaluation tool for assessing the organizational resilience of medical alliances. It suggests that enhancing integration and self-regulation can improve both the operational effectiveness and service quality of medical alliances.
Similar content being viewed by others
Introduction
Improving an organization’s cohesion and running it efficiently has always been a key concern in the field of management practice. The concept of organizational resilience has emerged as a critical factor in ensuring that businesses can withstand and recover from various adversities, including economic downturns, market disruptions, and internal organizational crises. This concept, introduced to the field of management by Meyer in 1982, has shifted scholars’ focus towards understanding and defining the nuances of resilience1.
At present, the definition of organizational resilience can be divided into two perspectives: the static view and the dynamic view. Scholars adhering to the “static view” believe that organizational resilience should encompass the ability to adapt and bounce back from challenges, as well as the ability to maintain its core function after a crisis2,3. Scholars adhering to the “dynamic view” believe that organizational resilience should include the ability to absorb and adapt while maintaining functions in a changing environment, as well as the process of learning and creating through resource integration in unfavorable circumstances4,5.Most scholars align with the dynamic view and have introduced this concept into the field of public health6. In 2016, the World Health Organization (WHO) defined health system resilience as the ability of a system, community, or society to maintain its basic structure and function when in danger, and to recover quickly and effectively from a disaster through resistance, absorption, and adaptation7.
The evaluation of organizational resilience involves multiple dimensions, including awareness, adaptability, planning ability, resources, and learning ability. McManus proposed that organizational resilience can be measured across three dimensions: situational awareness, management of keystone vulnerabilities, and adaptive capacity, to reflect its stages of elastic change2. Hind used qualitative research to categorize organizational resilience into five dimensions: change ability, organizational commitment, social relationships, team cohesion, and reality perception8. Kantur and Iseri-Say developed an organizational resilience scale combining quantitative and qualitative methods, asserting that resilient organizations can actively adapt to changes and progress, structuring a framework with robustness, agility, and integrity9. Kruk proposed that the health system should possess the abilities to be aware, diverse, self-regulating, integrated, and adaptive in order to form a highly proactive and functioning healthcare delivery system7. Current resilience scales predominantly assess subjective indicators, with limited literature on objective ones. Scholars rarely gather both types of data to validate and enrich each other’s findings.
In recent years, to integrate and enhance primary healthcare, China has actively built medical alliances by incorporating township hospitals and their branch hospitals into medical groups. These medical alliances primarily rely on government policies to fully integrate and optimize regional health care resources. However, the organization structure of these medical alliances is relatively fragile, and the internal motivation of each branch hospitals is insufficient, resulting in low overall operational efficiency. In the current volatility, uncertainty, complexity, and ambiguity (VUCA) era, medical alliances face pressures from natural disasters, epidemics, digital transformation, and the increasing demand for personalized health services. Therefore, they need to possess resilience to adapt and withstand these pressures10. Based on previous literature, this study defines the organizational resilience of medical alliances as the advanced functional processes of redundant preparation, stable recovery, and autonomous coping displayed by medical alliances in response to emergencies, internal and external threats, and challenges that restrict the sustainable development of organizations, as well as their ability to absorb, adapt, and resist changes in interfering events11,12,13. This resilience not only maintains the basic structure and function of the organization but also enables the organization to grow against the trend.
Research on organizational resilience evaluation in public health remains limited, with existing studies primarily focused on health systems and single hospitals6,14. Medical alliances, as composite organizations characterized by multi-institutional collaboration, have not yet undergone comprehensive resilience assessment. This study introduces the Analytic Hierarchy Process (AHP) to construct a comprehensive evaluation index system for the organizational resilience of medical alliances, tailored to China’s national conditions. The AHP method innovatively structures complex resilience factors hierarchically, integrates qualitative and quantitative indicators, and determines the weight order of each criterion through pairwise comparisons. The final research results provide a tool for leaders of medical alliances to identify key elements and focus on the factors that contribute to organizational resilience, thereby enabling the implementation of policy measures to improve performance.
Methods
The model of organizational resilience factors for medical alliance
In this study, we construct the conceptual framework of health community organization resilience by referring to the 5 elements of health system resilience proposed by Professor Kruk. She indicated that the health system resilience should have the abilities of aware, diverse, self-regulating, integrated, and adaptive6. Huang and Wen believe that organizational resilience can be analyzed through a dual framework of structure and function15. Structural resilience refers to the ability of multiple agents within an organization to form a stable and enduring structure that performs specific functions. This involves two aspects: the diversity and integration of these multiple agents. Functional resilience, on the other hand, is the comprehensive capability of an organization to handle complex governance challenges. During the governance process, it manifests as a functional progression and a virtuous cycle through three stages: aware, self-regulating, and adaptive. Based on the above key articles, this study constructed a model of organizational resilience factors for medical alliances, and the 5 first-level sub-criteria are shown in Fig. 1.

The organizational resilience assessment framework for medical alliance.
Literature review and modeling process
A literature review was conducted using Web of Science, Science Direct, Google Scholar, PubMed, Wangfang, and CNKI. The retrieval period spanned from the inception of these databases to September 2023. We searched for literature using the following search terms: (resilience), (organizational resilience), (health system resilience), (medical group resilience), (hospital resilience), and (health care resilience). Inclusion criteria: (1) research topic focuses on the concept, connotation, and evaluation framework of organizational resilience within health systems or hospitals; (2) standardized and clear research methods and processes with reliable content; (3) research results include analysis and evaluation of resilience in health systems or hospital organizations. Exclusion criteria: (1) unclear definition of organizational resilience; (2) inadequate research methods relying on subjective judgment and unverifiable authenticity; (3) conference abstracts lacking full methodological disclosure.
Based on the selected literatures and group discussions, we constructed second-level and third-level sub-criteria for the organizational resilience of medical alliance (Table 1). Firstly, we identified and marked keywords related to organizational resilience, analyzed their frequency and occurrence rate, and selected important keyword with a frequency > 5% and an occurrence rate > 15%. “Frequency” indicates the number of times a keyword appears, while “occurrence rate” is the proportion of a keyword’s appearances relative to all keywords, calculated as occurrence rate = frequency/total number of keywords16. These were classified into five first-level sub-criteria frameworks, resulting in 15 second-level sub-criteria through group discussions. Secondly, we formed an initial pool of sub-criteria was formed by collecting and summarizing relevant evaluation indicators of organizational resilience from the selected literatures. Our research group screened these sub-criteria, sorted and organized them based on first-level and second-level sub-criteria frameworks. Then five experts (two university professors, two hospital directors and one director of health administration department) and our research group conducted two rounds of discussions to finalize the 43 three-level sub-criteria (Table 1, Fig. 2). Finally, we obtained the weights and rankings of the first-, second-, and third-level sub-criteria through a survey of 19 experts from universities, health commissions, centers for disease control and preventions (CDC), and hospitals using the AHP method, thereby identifying the critical factors.
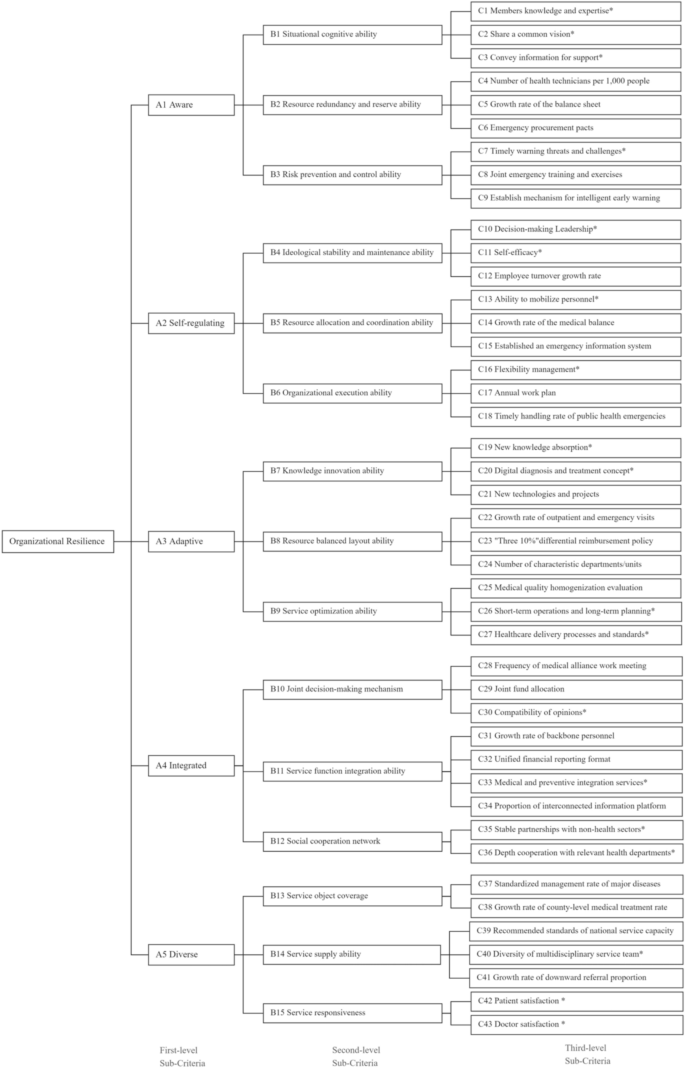
The hierarchical structure of AHP for organizational resilience assessment. *Indicates subjective items; the rest are objective items.
The analytic hierarchy process method
AHP is a sophisticated method for subjective decision-making, pioneered by Saaty in the early 1970s31. The AHP method is valuable for its ability to structure complex decisions, involve multiple perspectives, and provide a quantitative framework for evaluating qualitative criteria, leading to more informed and objective decision-making processes. The AHP involves several steps: First, structure the decision problem into a hierarchy with a clear goal, criteria, and alternatives. Next, conduct pairwise comparisons of the criteria to assess their relative importance using a nine-point scale. Then, calculate the weights for each criterion to represent their significance in relation to the others. After that, synthesize the priorities to determine an overall score for each alternative by combining the criteria weights with the alternatives’ scores. It’s crucial to perform a consistency check using the consistency ratio to ensure the judgments made in the pairwise comparisons are consistent; if the ratio exceeds a certain threshold, the comparisons may need revision. Finally, based on the calculated scores and rankings, the alternative with the highest score is selected as the best option31,32.
The steps of the AHP in this study are as follows:
Step 1 Define and state the organizational resilience for medical alliance clearly. The hierarchal structure of organizational resilience is divided into three levels, including 5 first-level sub-criteria, 15 second-level sub-criteria, and 43 third-level sub-criteria.
Step 2 Obtain the paired comparison matrix from each expert. According to the consistent matrix method proposed by Saaty et al., a judgment matrix A for pairwise comparison is constructed using the relative importance scores of pairwise indicators at the same level, as provided by expert consultation, as shown in Eq. (1). The element α of the paired comparison matrix is determined by Saaty’s 9-point Likert scale (from “equally important” to “absolutely important”).
Step 3 Calculate the relative weights between criteria. Formula (2) is used to calculate the product \({M}_{i}\) of each row element in the paired comparison matrix. Formula (3) is used to calculate the n-th root of \({M}_{i}\), where n is the order of the matrix. Formula (4) is used to obtain the eigenvector \({W}_{i}\) of each matrix, and further determine the influence degree of each index on the resilience of the organization.
Step 4 Check the consistency of the paired comparison matrix provided by each individual expert. The random consistency ratio (CR) for each expert’s judgment matrix is used to test the consistency of that expert’s scores. When CR < 0.1, it indicates that the expert’s constructed judgment matrix has satisfactory consistency. When CR ≥ 0.1, the minimum forward method and the maximum change method are used to make corrections. For each expert’s matrix, the general consistency index (CI) is calculated by formula (5), where \({\uplambda }_{max}\) is the largest eigenvalue of the paired comparison matrix. Formula (6) is used to calculate the random CR. For different matrix sizes, the respective values of the random consistency (RI) index are shown in Supplementary Table S1. Only judgement matrices from experts achieving CR < 0.1 were included in the subsequent aggregation process.
Sensitivity analysis
To evaluate the robustness of the AHP weights derived from the expert data, a sensitivity analysis was conducted using a Monte Carlo simulation approach to perturb the expert authority levels. First, the AHP weights were structured for computational processing, with baseline authority values assigned to each expert. Second, a Monte Carlo simulation with 10,000 iterations was executed. In each iteration, the expert authority levels were randomly adjusted by ± 10% of their base values. Third, in each iteration, the AHP weights were recalculated using the adjusted expert authority levels. Fourth, the stability of the weights was assessed by measuring the fluctuation of each weight across all iterations. The 95%CI for each weight were recorded, and the percentage change relative to the original weight was calculated.
Data collection
This study was carried out from August to September 2023, the expert questionnaire was sent by email for two rounds, and respondents were asked to complete the survey within 10 days for each round. Based on the outcomes of the first round of expert consultation and the feedback provided by the experts, the indicator system for organizational resilience of medical alliance was revised, and the foundation for the second round of expert consultation was established. In the second round, the experts’ relative importance scores for the pairwise comparisons between indicators at the same level were aggregated to determine the final weight coefficients for the indicators at each level.
The selection of the 19 experts in the study considered factors such as geographical location, occupation type, and age distribution to ensure the representativeness of their views. Geographically, the experts were drawn from northern provinces (n = 6), southeastern provinces (n = 8), and southwestern provinces (n = 5) of China, representing first-tier cities, coastal areas, and western mountainous districts, respectively. This distribution reflects China’s socioeconomic gradient. In terms of occupation type, the experts included individuals from scientific research institutions (n = 6), health administration departments (n = 6), and hospitals (n = 7), covering both management and technical roles. Regarding age distribution, the experts ranged in age from 37 to 63 years old. The selection criteria for the participants were as follows: (1) more than 5 years of working experience in the field of medical alliance; (2) management and technical experts on the organizational resilience; (3) can actively and voluntarily participated in this consultation. This study met the requirements of the AHP analysis method.
Ethical issues
This study was conducted in accordance with the 1964 Declaration of Helsinki and received the approval of the Ethics Committee of Hangzhou Normal University Ethics Board (No.2019065). Informed consent was obtained from all individual participants included in the study.
Results
Demographic characteristics of experts in AHP survey
Table 2 shows the demographic characteristics of the 19 experts. All participants were between the ages of 34 and 63, and 42.11% of them were over the age of 45. 78.95% of participants were male. 36.84% of participants were director or vice-directors of hospitals, and 31.58% were professors at universities. They were highly educated, 68.42% of them had a Master’s degree or above. 73.68% of participants had an associate senior or above professional title. 89.47% of participants had more than 10 years of work experience.
Pairwise comparison of evaluation criteria for organizational resilience
Table 3 and Supplementary Table S2 presents the weight outcomes for 19 expect panelists. The CR and CI are both below 0.1, signifying that the matrix has passed the consistency assessment. The outcomes encompass the local and global weights of the first-level and second-level sub-criteria for organizational resilience among medical alliance. In the first-level sub-criteria, the local and global weights were ranked as follows: A4 Integrated (0.282) > A2 Self-regulating (0.228) > A1 Aware (0.182) > A5 Diverse (0.155) > A3 Adaptive (0.153).
In the second-level sub-criteria, the important factors for local weights were as follows: (1) B1 Situational Cognitive Ability (0.397) as one of A1 aware, (2) B6 Organizational Execution Ability (0.385) as one of A2 Self-Regulating, (3) B9 Service Optimization Ability (0.397) as one of A3 Adaptive, (4) B11 Service Function Integration Ability (0.408) as one of A4 Integrated, (5) B14 Service Supply Ability (0.471) as one of A5 Diverse. The three most important factors for global weights in the second-level sub-criteria were B11 Service Function Integration Ability (0.119) as part of A4 Integrated, B10 Joint Decision-making Mechanism (0.118) as part of A4 Integrated, and B6 Organizational Execution Ability (0.091) as part of A2 Self-regulating.
Table 4 presents the three most important factors for global weights in the third-level sub-criteria: (1) C10 Leadership at the decision-making level of the medical alliance (0.050) as part of B4 Ideological Stability and Maintenance Ability, (2) C29 Funds of the medical alliance are jointly negotiated and allocated by the township hospital and each branch hospital (0.048) as part of B10 Joint Decision-making Mechanism, (3) C33 The integration of medical and preventive integration services in the medical alliance (0.041) as part of B11 Service Function Integration Ability.
Sensitivity analysis
Supplementary Table S3 shows the weights of the first-level indicators exhibited robust stability. The variation coefficients of the first-level indicators are all below 0.08, indicating high stability. Among them, A4 has the largest absolute fluctuation (± 0.021), but its impact on the relative proportion is controllable. This indicates that the weight allocation scheme is robust and reliable.
Discussion
The study of organizational resilience among medical alliances holds significant theoretical and practical importance for understanding and enhancing the adaptability, resilience, and growth of medical alliance when confronted with various challenges. In today’s social environment, which is increasingly characterized by VUCA, organizational resilience enables medical alliances to cope with unpredictable adverse events and daily challenges13. The main characteristics of this study are as follows: firstly, the subject of the evaluation is the organizational resilience of the medical alliance, which is a composite organization consisting of a township hospital and several branch hospitals, differing from a single organization; secondly, current evaluation literature on organizational resilience primarily focuses on subjective evaluation. We believe that organizational resilience encompasses not only perceptual cognition but also an objective measure of resilience. Therefore, an evaluation index system that integrates both subjective and objective indicators has been designed, featuring 19 subjective indicators and 24 objective indicators, which can more comprehensively reflect the characteristics of organizational resilience; thirdly, experts utilizing the AHP selected provinces that represent different levels of economic development and geographical locations. In terms of personnel types, they included university scholars, health administrative leaders, and hospital directors at various levels to assign scores to the evaluation index system from multiple perspectives; fourthly, through the study of organizational resilience, it can foster the improvement of medical alliance performance and competitiveness33.
In the first-level sub-criteria weights, integration and self-regulation are the two domains with the greatest weight in organizational resilience among medical alliances. This differs from Kruk’s results, which found that awareness and diversity are the top two domains of organizational resilience in health system6. It may be because this concept is proposed for public health emergencies, focusing on stress response and early warning, and mobilizing resources to meet diverse health needs. In this study, although the medical alliance is also a composite organization, its construction is under the new health reform policy. The aim is to enhance the level of medical technology in rural areas by encouraging township hospitals and their branch hospitals to integrate and unify both personnel and assets to form a medical group34. Currently, medical alliances are established through the implementation of government policies. The hospitals within the medical alliance lack unified legal status, separate funding, and integrated staffing, resulting in weak overall cohesion35. Therefore, experts believe that enhancing integration is the most critical element for improving organizational resilience. Additionally, self-regulation in fully integrated hospitals within the medical alliance helps cope with threats and challenges, and effective management can stabilize staff, deploy available resources, and quickly respond to crises36. However, limited integration restricts these efforts, making it urgent to integrate personnel and assets across hospitals to enhance resilience.
In the second-level sub-criteria weights, the top three factors for medical alliance resilience are: “service function integration ability and joint decision-making mechanism in the integrated dimension”, “organizational execution ability and ideological stability and maintenance ability in the self-regulating dimension”, and “situational cognitive ability in the aware dimension”. These reflect the abilities of organizational management and decision-making in executive power, as well as situational perception and thought stability in cognitive power. This aligns with medical group literature37,38, which indicated that the ability of medical groups to form effective organizational structures is crucial, and to establish a multi-tiered medical group governance structure that aligns on strategic direction and major decisions. Domestic literature agrees that the biggest challenge after establishing the medical alliance is clarifying administrative and governance relationships among hospitals at different levels to create a unified management system and resource mobilization capability39. Additionally, this study highlights that cognitive situational awareness and thought stability, often overlooked in domestic literature34,39, are key aspects of organizational resilience in medical alliances. While effective management execution and performance assessment are important, ensuring unified staff cognition and a shared vision is equally crucial. Medical alliance leaders should hold regular staff meetings for two-way communication to align them with medical alliance goals, boosting their sense of belonging and organizational cohesion27.
In the third-level sub-criteria, the greatest weight is attributed to a softer indicator: “the leadership at the decision-making level of the medical alliance”. The characteristic behaviors exhibited by leaders when guiding, directing, motivating, and influencing employee performance are crucial21. There is a majority literature on the impact of leadership on medical organizations21,40,41, which indicates that leadership styles not only play a crucial role in driving sustainable development within the healthcare sector, but also assist organizations in rapidly adapting to the ever-changing medical environment, thereby achieving better performance. For the medical alliance, leadership is particularly important. Medical alliance leaders face the challenge of managing a group composed of multiple hospitals. In addition to promoting the development of individual hospitals, it is crucial to coordinate the differentiated development and service provision between township hospitals and their branch hospitals, as well as to foster coordinated development and orderly competition among branch hospitals36. As leaders of the medical alliance, they must possess personal charisma and decisive decision-making abilities to communicate with and coordinate among multiple hospitals within the group, forming a unified vision and setting a clear development direction. This is an essential ability to lead the entire medical group towards stable development40.
The second most critical indicator is that “the funds of the medical alliance are jointly negotiated and allocated by the township hospital and each branch hospital”. This is similar to literature reported in Mayo’s medical group, which identifies that a key component of successful clinical integration is the centralization of essential shared administrative and financial functions42. During the grassroots visits and surveys conducted in this study, many medical alliance leaders mentioned this view, believing that the overall allocation of funds is an important symbol of the medical alliance’s integration. Medical alliance leaders can establish a unified fund management system and set up a special account to centrally manage funds. Through the formulation of a unified budget system, they can scientifically allocate medical and public health funds according to the business volume of each hospital and the population served36,43. Additionally, setting up a fund adjustment pool to draw funds in proportion can help support weak hospital and respond to emergencies, thereby promoting coordinated development and improving overall efficiency.
The third important weighting indicator is “the integration of medical and preventive services within the medical alliance”. Since the establishment of the medical alliance in China, there has been a strong push for the integration of medical and preventive services44. The government aims to control rising medical costs and build a health-centered medical alliance by emphasizing preventive care within the medical process45,46. However, integration is hindered as specialist and public health doctors are managed by separate hospital and CDC systems. To address this, medical alliance leaders should break down these barriers, promote cooperation, and improve service efficiency47,48. Additionally, incorporating residents’ health status into performance evaluations can encourage a shift from medical-centered to health-centered service behavior among doctors.
Limitations
There are several limitations to this study. Firstly, the AHP may introduce a certain degree of subjective judgment bias during the indicator screening and expert evaluation processes. Secondly, the current evaluation indicators system needs to be simplified and refined to improve its practicality and ease of use. Thirdly, lack of analysis regarding regional variations in the priority of factors that may affect organizational resilience.
Conclusion
In this study, a panel of 19 experts was selected to construct an evaluation framework for organizational resilience, including 5 first-level sub-criteria, 15 second-level sub-criteria, and 43 third-level sub-criteria. Using the Analytic Hierarchy Process, we identified integration and self-regulation are key factors affecting the organizational resilience of the medical alliance. The three indicators with the greatest impact are the leadership within the medical alliance, the overall allocation of funds among hospitals at various levels, and the provision of integrated medical and preventive services. This study provides a comprehensive evaluation tool for assessing the organizational resilience of the medical alliance, leaders should focus on the effective integration of internal human and financial resources, ensuring unified staff cognition and a shared vision, thereby enhancing the resilience of the medical alliance and improving operational efficiency.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Meyer, A. D. Adapting to environmental jolts. Adm. Sci. Q. 27(4), 515. https://doi.org/10.2307/2392528 (1982).
McManus, S., Seville, E., Vargo, J. & Brunsdon, D. Facilitated process for improving organizational resilience. Nat. Hazards Rev. 9(2), 81–90. https://doi.org/10.1061/(ASCE)1527-6988(2008)9:2(81) (2008).
Jia, M., Xiang, Y. & Zhang, Z. Corporate social responsibility and organizational resilience. Manag. Q. 3, 25–39. https://doi.org/10.3969/j.issn.1672-884x.2023.07.009 (2020).
Patriarca, R., Di Gravio, G., Costantino, F., Falegnami, A. & Bilotta, F. An analytic framework to assess organizational resilience. Saf. Health Work 9(3), 265–276. https://doi.org/10.1016/j.shaw.2017.10.005 (2018).
Gilson, L., Ellokor, S., Lehmann, U. & Brady, L. Organizational change and everyday health system resilience: Lessons from cape town, South Africa. Soc. Sci. Med 266, 113407. https://doi.org/10.1016/j.socscimed.2020.113407 (2020).
Kruk, D. M. E. What is a resilient health system?. Lessons Ebola 385, 1910–1912. https://doi.org/10.1016/s0140-6736(15)60755-3 (2015).
Wang, L. et al. The situation and implication of the study on the resilience of health systems in foreign countries. Chin. J. Emerg. Resuse Disaster Med. 16(2), 205–210. https://doi.org/10.11936/bjutxb2023050018 (2021).
Hind, P., Frost, M. & Rowley, S. The resilience audit and the psychological contract. J. Manag. Psychol 11(7), 18–29. https://doi.org/10.1108/02683949610148838 (1996).
Kantur, D. Measuring organizational resilience: a scale development. Pressacademia 4(3), 456–456. https://doi.org/10.17261/Pressacademia.2015313066 (2015).
Zhang, G. Y., Zhang, C. & Liu, W. Q. Turning danger into safety: a literature review and prospect of organizational resilience. Econ. Manag. 10, 192–208. https://doi.org/10.3724/j.issn.1674-4969.22052303 (2020).
Chen, S. Construction of an early risk warning model of organizational resilience: An empirical study based on samples of R&D teams. Discrete Dyn. Nat. Soc. 2016(1), 4602870. https://doi.org/10.1155/2016/4602870 (2016).
Chen, R., Xie, Y. & Liu, Y. Defining, conceptualizing, and measuring organizational resilience: A multiple case study. Sustainability 13(5), 2517. https://doi.org/10.3390/su13052517 (2021).
Duchek, S. Organizational resilience: A capability-based conceptualization. Bus. Res. 13(1), 215–246. https://doi.org/10.1007/s40685-019-0085-7 (2020).
Zhang, J., Chen, H., Liu, G. D., Li, X. M. & Sun, T. Organizational resilience of public hospitals: A conceptual framework. Chin. Hosp. Manag. 39(09), 1–3 (2019).
Huang, L. Z. & Wen, Z. Q. How can dual resilience resolve structural risks in poverty-stricken relocated communities? Based on a county case study in Guinan city. J. Party School Tianjin Munic. Comm. CPC 24(4), 84–95. https://doi.org/10.16029/j.cnki.1008-410X.2022.04.009 (2022).
Yang, S.Y., Huang, J.Y., Li, J.R. Weng, Y.Y., Wu, D., Chen, J.C. & Zhou, C. Conceptual study of organizational resilience in county medical consortia based on atomic spectroscopy. Chin. Hosp. Manag. 45, 33–36+69 (2025).
Wang, Y. & Cai, J. Organizational resilience scale development and its reliability and validity verification. Stat. Decis. 5, 178–181. https://doi.org/10.13546/j.cnki.tjyjc.2019.05.040 (2019).
Gleeson, L., O’Brien, G. L., O’Mahony, D. & Byrne, S. Interprofessional communication in the hospital setting: A systematic review of the qualitative literature. J. Interprof. Care 37(2), 203–213. https://doi.org/10.1080/13561820.2022.2028746 (2023).
Hadian, S. A., Rezayatmand, R., Shaarbafchizadeh, N., Ketabi, S. & Pourghaderi, A. R. Hospital performance evaluation indicators: A scoping review. BMC Health Serv. Res 24(1), 561. https://doi.org/10.1186/s12913-024-10940-1 (2024).
World Health Organization. Hospital emergency response checklist: an all-hazards tool for hospital administrators and emergency managers. in Hospital emergency response checklist: an all-hazards tool for hospital administrators and emergency managers. (2011).
Wu, Y., Awang, S. R., Ahmad, T. & You, C. A systematic review of leadership styles in healthcare sector: Insights and future directions. Geriatr. Nur. (Lond.) 59, 48–59. https://doi.org/10.1016/j.gerinurse.2024.06.033 (2024).
Imani, A., Alibabayee, R., Golestani, M. & Dalal, K. Key indicators affecting hospital efficiency: A systematic review. Front. Publ. Health 10, 830102. https://doi.org/10.3389/fpubh.2022.830102 (2022).
Wang, X. P. et al. Construction of evaluation index system for public health performance of county medical community. Prev. Med. 32(9), 869–872. https://doi.org/10.19485/j.cnki.issn2096-5087.2020.09.002 (2020).
Thune, T. & Mina, A. Hospitals as innovators in the health-care system: A literature review and research agenda. Res. Policy 45(8), 1545–1557. https://doi.org/10.1016/j.respol.2016.03.010 (2016).
National Health Commission Office of Primary Health. Notice on issuing the evaluation standards and monitoring indicator system for the construction of integrated county medical and health communities (Trial). https://www.gov.cn/zhengce/zhengceku/2020-09/18/content_5544471.htm (2020)
Shortell, S. M., Schmittdiel, J., Wang, M. C., Li, R. & Gillies, R. R. An empirical assessment of high-performing medical groups: Results from a national study. Med. Care Res. Rev. 62(4), 407–434. https://doi.org/10.1177/1077558705277389 (2005).
Richtnér, A. & Löfsten, H. Managing in turbulence: How the capacity for resilience influences creativity. RD Manag. 44(2), 137–151. https://doi.org/10.1111/radm.12050 (2014).
Liang, J. et al. The experience and challenges of healthcare-reform-driven medical consortia and regional health information technologies in China: A longitudinal study. Int. J. Med. Inf. 131, 103954. https://doi.org/10.1016/j.ijmedinf.2019.103954 (2019).
Cai, Y., Cui, X., Su, B. & Wu, S. Changes in mortality rates of major chronic diseases among populations aged over 60 years and their contributions to life expectancy increase —China, 2005–2020. China CDC Wkly 4(39), 866–870. https://doi.org/10.46234/ccdcw2022.179 (2022).
Schmidt, M., Steigenberger, N., Berndtzon, M. & Uman, T. Cultural diversity in health care teams: A systematic integrative review and research agenda. Health Care Manage. Rev. 48(4), 311–322. https://doi.org/10.1097/HMR.0000000000000379 (2023).
Saaty, R. W. The analytic hierarchy process—What it is and how it is used. Mathl. Modell. 9(3–5), 161–176. https://doi.org/10.1016/0270-0255(87)90473-8 (1987).
Taherdoost, H. Decision making using the analytic hierarchy process (AHP): A step by step approach. Int. J. Econ. Manag. Syst. 2, 243–246. https://doi.org/10.11936/bjutxb2023050018 (2017).
Hillmann, J. & Guenther, E. Organizational resilience: A valuable construct for management research?. Int. J. Manag. Rev. 23, 7–44. https://doi.org/10.1111/ijmr.12239 (2021).
Cui, Z. H. & Wang, H. F. The construction logic and implementation path of the merged county medical community from the perspective of holistic governance. Chin. J. Health Policy 14(2), 1–7. https://doi.org/10.3969/j.issn.1674-2982.2021.02.001 (2021).
Yang, F., Yang, Y. & Liao, Z. Evaluation and analysis for Chinese medical alliance’s governance structure modes based on Preker-Harding model. Int. J. Integr. Care 20(4), 14. https://doi.org/10.5334/ijic.5417 (2020).
Zhou, C. et al. Study on the construction and countermeasure of health-centered integrated health care service system. Chin. J. Hosp. Admin. 36(7), 539–543. https://doi.org/10.3760/cma.j.cn111325-20200402-01001 (2020).
Kara, W. & Tamara, B. Medical group governance for better organizational integration. Manag. Healthc. 8(4), 337–343. https://doi.org/10.69554/OKVN5072 (2024).
Tan, T., Mills, G. R., Papadonikolaki, E. & Chen, K. Building information modelling in healthcare design and construction: A bibliometric review and systematic review. Int. Conf. Comput. Civil Build. Eng. 357, 401–415. https://doi.org/10.1007/978-3-031-35399-4_30 (2024).
Tan, H. W. et al. The construction of integrated urban medical groups in China: Typical models, key issues and path optimization. Chin. J. Health Policy 17(1), 9–16. https://doi.org/10.3969/j.issn.1674-2982.2024.01.002 (2024).
Warren, O. J. & Carnall, R. Medical leadership: Why it’s important, what is required, and how we develop it. Postgrad. Med. J. 87(1023), 27–32. https://doi.org/10.1136/pgmj.2009.093807 (2011).
AL-Hashimi, N. M. & AL-Hashimi, M. A systematic review on medical leadership in hospital setting. in The Importance of New Technologies and Entrepreneurship in Business Development, Vol. 194, 661–669. https://doi.org/10.1007/978-3-030-69221-6_50 (2021).
Helmers, R. A. & Harper, C. M. The mayo clinic model of clinical integration. Healthcare 7(3), 100330. https://doi.org/10.1016/j.hjdsi.2018.06.006 (2019).
Mason, A., Goddard, M., Weatherly, H. & Chalkley, M. Integrating funds for health and social care: An evidence review. J. Health Serv. Res. Policy 20(3), 177–188. https://doi.org/10.1177/1355819614566832 (2015).
Zhou, C., Lai, S. H., Zhang, L. & Tan, F. Analysis on the operation mode and effect of medical preventive integration in county scale medical alliances in Hangzhou. Chin. J. Hosp. Admin. 37(9), 709–712. https://doi.org/10.3760/cma.j/cn111325-20210311-00210 (2021).
Redwood, S., Brangan, E., Leach, V., Horwood, J. & Donovan, J. L. Integration of research and practice to improve public health and healthcare delivery through a collaborative “health integration team” model—A qualitative investigation. BMC Health Serv. Res. 16(1), 201. https://doi.org/10.1186/s12913-016-1445-z (2016).
Lê, G. et al. Can service integration work for universal health coverage? Evidence from around the globe. Health Policy 120(4), 406–419. https://doi.org/10.1016/j.healthpol.2016.02.007 (2016).
Hu, L. et al. Integrating health and care in China: Lessons learned and future outlook. Int. J. Integr. Care 21(4), 18. https://doi.org/10.5334/ijic.5681 (2021).
Wang, J., Zhu, J. M. & Wang, X. Y. Integration and coordination of public health system, medical service system and healthcare security system: Theoretical mechanism and case study. Sci. Found. China 34(6), 703–711. https://doi.org/10.3969/j.issn.2095-4026.2022.02.005 (2020).
Acknowledgements
We thank the experts for their useful comments and suggestions.
Funding
This study was supported by the National Natural Science Foundation of China (No: 72274050), Shanghai Municipal TCM and Integrated Medicine Society Research Fund for Community Medicine and Health Management (No: 2024-13).
Author information
Authors and Affiliations
Contributions
All authors contributed to the interpretation of the findings, the writing of the manuscript, and have approved the final version. C.Z. and W.M.C. wrote the manuscript text; Q.F.H., X.L.L., J.C.C., Y.X.Z., and W.J.L. collected data and performed statistical analysis; Z.J.W. and M.M.J. reviewed and guided the article.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhou, C., Cao, W., Huang, Q. et al. Identifying key factors for organizational resilience among medical alliance using the analytic hierarchy process method. Sci Rep 15, 29728 (2025). https://doi.org/10.1038/s41598-025-11994-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-11994-9
