
Abstract
The advent of disease modifying therapies in spinal muscular atrophy (SMA) has increased life expectancy but also raising new challenges. We aimed to explore the neurobehavioral profile in SMA type I subjects and in those identified by newborn screening (NBS). Behavioral assessment included screening questionnaires (strengths and difficulties questionnaire (SDQ), social communication questionnaire (SCQ), and sensory profile 2 (SP2)), neurobehavioral observation, CARS2 and DSM-5 criteria. The cohort included thirty-one children (25 type I and 6 NBS) aged 2–10 years. On SDQ prosocial scale, 14/31 showed borderline or abnormal results. 6/14 had borderline scores at the SCQ questionnaire, while none had abnormal scores. Neurobehavioral observation suggested the presence of ASD in 3/31, confirmed by CARS2 and DSM-5 criteria. 5/31 showed other behavioral disorders. Our findings suggest that autism is present in SMA infants in a percentage slightly higher than in the general population. Other neurobehavioral difficulties are less frequent. Our study highlighted the challenges to select appropriate tools in infants with limited mobility and the need for a clear diagnostic pathway, starting with screening questionnaires followed by more appropriate diagnostic tools to reduce the number of false positive results.
Similar content being viewed by others

Introduction
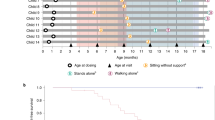
Spinal muscular atrophy (SMA) is a rare autosomal recessive neuromuscular disorder caused by mutations in the survival motor neuron 1 (SMN1) gene on chromosome 5q11.2, leading to progressive muscular atrophy and weakness1. Type I is the most severe pediatric form of SMA, with onset before 6 months of age and severe motor, respiratory, and feeding impairment. In the past, infants with type I SMA did not survive after the age of two years2. The advent of disease modifying therapies has increased life expectancy associated with some functional improvements even if, because of the persistence of some muscle weakness, they never achieve the skills observed in typically developing infants. Treated type I infants often achieve head control and sitting but independent walking is only achieved in a minority of treated type I infants. They also often develop some language abilities, never previously observed in untreated type I infants3,4,5,6,7,8,9,10,11,12, with production of intelligible words/sentences and preserved comprehension6.
While SMA is known to be a disorder predominantly affecting motoneurons, over the last few years there has been increasing interest in determining to which extent SMA should be considered as a multi-system disorder13. The rationale behind this is that SMN protein is ubiquitously expressed, and its reduction may affect several physiological mechanisms and various cell types other than motoneurons. There is however limited evidence of the involvement of other organs14,15 with anecdotal reports of cardiac or autonomic system dysfunction that more often occurs in the most severe early-onset forms16,17. More attention has been devoted to the role of the SMN protein during the early stages of brain development and to possible cognitive and neurodevelopmental comorbidities. Brain involvement in SMA has been suggested since the late 1990s18,19, especially in the most severe forms (types Ia or 0), but the evidence from neuropathological and imaging studies reporting brain involvement is limited20,21,22,23,24,25. The brain magnetic resonance imaging (MRI) changes consist in ventricular dilatation and atrophy, or destructive changes rather than brain malformations related to early prenatal insults. As the studies were performed in infants who also had severe respiratory involvement it was not always easy to ascertain whether the changes observed on MRI could also be at least partly possibly related to postnatal acute or chronic hypoxic ischemic insults.
In the last few years, there has been an increasing number of reports which have focused on the possible involvement of clinical aspects of neurodevelopment as part of the emerging phenotypes in treated type I infants26,27,28, including possible cognitive impairment29,30. A recent international survey reported an overall prevalence of 43% of neurodevelopmental comorbidities in children with early onset SMA26, including autism spectrum disorder (ASD), intellectual disabilities, and severe language delay. In particular, the observation of uncommonly reported ASD symptoms in untreated Type I children has raised specific concerns. Overall, these findings highlighted the need for more systematic prospective studies to better understand the extent to which each neurodevelopmental domains related to different neural networks are affected in type I SMA.
Diagnosing neurodevelopmental and, more generally, mental disorders in children with SMA may however be challenging as many of the commonly used tools have an important motor component in their items. The ASD diagnosis relies on the clinical observation of behaviors consistent with criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5)31 and the International Classification of Diseases (ICD, World Health Organization)32. Clinicians may employ structured tools along with direct observations (ADOS2) and information from multiple sources, such as the child/adolescent, parents (ADI-R), and teachers, to address diagnostic uncertainty33. These tools are considered extremely valuable both in clinical and research settings, as they are highly standardized, structured, reliable and with a high sensitivity. As they include items that require motor abilities, their use in some vulnerable populations, such as those affected by neuromuscular disorders is however limited34,35,36,37,38,39,40,41.
In this study, a multidisciplinary team, including expert clinicians in SMA and neurodevelopmental disorders administered a comprehensive clinical evaluation, including the use of direct clinical observation, a set of parental questionnaires focused on neurodevelopmental disorders related behaviors and structured test focused on ASD symptoms. The aim was to investigate social and behavioral functioning of children with SMA, also adopting a sensitive approach to establish how the that may be useful for adjusting findings from the used tools were influenced by motor performances.
Results
This study prospectively enrolled thirty-four children with genetically confirmed SMA diagnoses. Of these, twenty-eight children had a diagnosis of type I (age range: 2.6–9 years; mean age: 6.15 ± 1.92), and six children were identified by newborn screening (age range: 3.2–3.8 years; mean age: 3.59 ± 0.23). Among children identified by newborn screening, five were clinically asymptomatic at diagnosis and were treated before the clinical manifestation of symptoms, while one had minimal signs and was labeled as paucisymptomatic. All thirty-four subjects received at least one of the disease-modifying treatments (DMT) (Nusinersen, Risdiplam, Onasemnogene abeparvovec) approved in Italy.
The initial cohort includes thirty-four children, of these two had a CHOP INTEND < 8 and one had a profound intellectual disability with a mental age < 2 years, and since they were not assessable on any of the subsequent questionnaires/observation, this resulted in a final cohort of thirty-one children. Developmental and cognitive data assessed through structured instruments were available for all children. Eight children were assessed using Weschler scales42, five using Leiter43, six using Raven44, and twelve were assessed using developmental scales45,46. The cognitive level scored within the normal range for sixteen children (51%), borderline range in six children (19%), intellectual disability was detected in nine children (29%), All but one of the thirty-one children were able to speak.
Details on the demographic and clinical characteristics of the sample are summarized in Table 1.
Social and material vulnerability index was 102.25 (SD 3.03), with 3 subjects in the medium–high risk of vulnerability (98.6/100.29) and 28 at high risk of vulnerability (100.30/119.64).
Parental questionnaires
Strengths and difficulties questionnaire
Thirty-one parents filled out the SDQ questionnaire (version 4–16 years = 22; version 2–4 years = 9). When the parents were requested to indicate any SDQ item they considered unsuitable for their child’s motor ability level none of them indicated any item as “not appropriate” and all questions seemed suitable. Table 2 summarizes SDQ-P scores.
Social communication questionnaire
Thirty-one parents returned the SCQ questionnaire (version lifetime = 22; version current = 9).
None of the SCQ scored > 15, and six SCQ (19%) scored in the borderline range (11–14).
When the parents were requested to indicate any of the SCQ items some parents considered unsuitable for their child’s motor ability level up to ten items. The ten items that were found to be unsuitable for some subjects with SMA1, included:
-
“Are his facial expressions usually appropriate to the situation?” (question 9)
-
Does she/he ever use your hand like a tool or as if it were part of her/his own body? (question 10)
-
“Does he spontaneously point to things around him?” (question 22)
-
Does he nod his head to say yes?” (question 24)
-
“Does he engage in imaginative play with other children in a manner that allows each of them to understand what the other is pretending?” (question 39).
Statistical analysis on association between results at SCQ and patient characteristics showed no correlation except for an association between the parents school level and the SCQ results.
Sensory profile 2
Thirty-one parents returned the SP2 questionnaire (version 7–36 months = 1; version 3–10 years = 30). Twenty-seven parents perceived their children’s motor problems as a confounding factor for at least 80% of the behaviors in the questionnaire. Therefore is not described in the tables or analysis of the results.
Table 3 describes individual results.
Neurobehavioral observation
Thirty-one children completed the neurobehavioral observation. Deficits in communication and social interaction and restricted and repetitive behaviors were detected in three children. Similar, less intensive symptoms were observed in three children. Other behavioral problems detected in children were oppositive behaviors (n.3), anxiety (n.1), and hyperactivity (n.1). Emotional dysregulation was observed in eight children. Table 3 describes individual results.
Childhood autism rating scale, 2nd edition
Thirty-one children completed the CARS2. Results scored within the moderate range in three children. Two items (body use and activity level) were scored as not appropriate for the weaker children.
Table 3 describes individual results.
DSM-5 diagnosis
Based on DSM-5 criteria, the multidisciplinary team assigned a formal diagnosis to eight children (23%): three diagnosis of ASD, three diagnosis of Oppositional Defiant Disorder (ODD), one diagnosis of anxiety Disorder, and one diagnosis of Attention Deficit and Hyperactivity Disorder. Table 3 describes individual results.
Figure 1 describes the results in a diagnostic flow-chart, subdividing subjects on the basis of the results at the SDQ screening questionnaire (positive to prosocial behavior, positive to other subscales, negative to all subscales).

Flow-chart of screening and diagnostic assessments. Key to figure: Pink = Positive to the screening/diagnostic tool; Green = Negative to the screening/diagnostic tool; *Emotional dysregulation.
Discussion
The recent reports of possible neurodevelopmental disorders in type I SMA has highlighted the challenge of defining ASD and other neurodevelopmental disorders in patients in whom the assessments are largely biased by weakness in the skeletal or phonatory muscles. Even when treated with the most advanced therapies, type I patients survive and achieve important milestones, never previously achieved in untreated patients such as sitting or the ability to talk , but still present a degree of weakness that affects both lower and upper limb performances and language.
At the time of selecting the tools to assess neurodevelopmental disorders, a multidisciplinary team had to make decisions based on the scarce literature existing on the use of these tools in children with motor impairment or, more specifically, in neuromuscular disorders. The possibility to use structured tools with direct observations (ADOS-2) was not suitable as ADOS-2 was developed for ambulant children47 and nearly all of the type I patients in our cohort was non ambulant. Other questionnaires such as M-CHAT and ADI-R were also considered not suitable as they also contain questions that are driven by motor performance (e.g. does your child walk? Does your child copy what you do e.g. clap hands, wave “bye bye”, does your child like climbing on things?)48. Similarly, other tools such as the ASEBA instrument also included questions that are not appropriate in this motor-impaired population (e.g. can’t sit still, restless or hyperactive, gets in many fights, physically attacks people, poorly coordinated or clumsy).
As this could produce a bias where abnormal scores reflect physical disability rather than behavioral symptoms, it was felt that the use of this tool was not ideal for our cohort of non-ambulant individuals.
While most of the standardized tools have been proved to be useful when adapted to specific populations, such as verbally impaired children49, there has been concern about their use in motor impaired cohorts with some recent efforts to develop an algorithm for cerebral palsy50. So far there has not been a similar effort for neuromuscular disorders in which the pattern of motor impairment is different and mainly related to weakness.
Furthermore, as the therapies have been available for a limited number of years, most of our patients were in the younger subgroups and we did not have the choice of selecting an older cohort in whom the choice of tests would have been easier.
Based on the existing literature, the age range and the relatively low impact of motor performances the multidisciplinary team identified a comprehensive clinical assessment aimed at detecting ASD also including other more general tests investigating other neurodevelopmental disorders and, in some cases, also other mental disorders. While we were aware that there were still some limitations for many of these tests and that none of them in isolation could detect the spectrum of disorders we were investigating, we felt that the only way to establish their value and limitations was to apply them to our cohort.
Behaviors consistent with ASD criteria outlined in the DSM-5 were found in approximately 10% of our cohort. When including other neurodevelopmental disorders, such as ADHD, the overall percentage was 12%. These findings are much lower than those reported in a recent international survey indicating that 43% of SMA I had some neurodevelopmental disorders26. The difference could be due to the fact that in the present study, the formal diagnosis of autism spectrum disorder or other neurodevelopmental disorders was conducted by strictly adopting the DSM-5 criteria. In the published international survey26, less than 15% underwent a structured observations while the great majority were reported by parents or clinicians with no clear indication of whether the assessment of the children was based on parental reports or structured tests administrated by clinicians.
When assessing for autism spectrum disorder, fourteen of the thirty-one children assessed had abnormal results on the prosocial difficulties SDQ subscale that has been reported to be associated with possible autism spectrum disorder51,52.
The use of additional screening tools, like SCQ and neurobehavioral observations, helped to reduce the number of SDQ false positives as only six of the fourteen had borderline results on the SCQ and positive (n = 3) or borderline results (n = 3) on neurobehavioral observation. Interestingly the diagnosis of autism spectrum disorder on CARS2 and DSM-5 was confirmed only in the three who also had positive results on neurobehavioral observation and borderline results on SCQ.
While there has been suggestion that neurodevelopmental difficulties are more likely to be associated with the more severe clinical phenotypes, in our cohort autism spectrum disorder was also found in children identified with newborn screening and we were unable to show a consistent association with functional abilities.
In this study we were also interested to establish whether other neurodevelopmental disorders and mental disorders were present and if and to which extent they could be detected by screening tests. Behavioral difficulties, confirmed by DSM-5, were found in another four subjects (1 anxiety, 3 ODD) and they had all been previously suspected by the observation during clinical assessment. The SDQ only partially contributed to the identification of these subjects, as there were both false positive and false negatives results. Not surprisingly, the SCQ and CARS2, which are specifically designed to identify autism spectrum disorder, did not contribute to the detection of other neurobehavioral difficulties53.
The percentage of autism spectrum disorder was slightly raised in our cohort (10%) compared to general population (1.34%)42.
In contrast, the percentage of anxiety, ODD and ADHD was in line or even lower than the values reported in literature (4% anxiety disorder in general population vs 3% in our cohort, ODD 3–15% in general population vs 10% in our cohort, ADHD 5–10% in general population vs. 3% in our cohort)54. These percentages are low, expecially if we consider that other possible risk factors, such as social and material vulnerability index55,56, or the diagnosis of a chronic illness57, the frequent hospitalizations and the caregivers’ burden58 may have potentially also contributed to their development.
These results should be interpreted with caution as this was a cross sectional study and the age and the duration of the follow up in our cohort was variable. While the children with a confirmed diagnosis were relatively few, we cannot exclude that children with minor signs such as stereotyped movements or reduced eye contact, that were not enough to reach the threshold for autism spectrum disorder on CARS2 and DSM-5, may develop more severe or additional signs such as restrictive and repetitive behaviors that become more evident at a later age. Moreover, the lack of self-report measures due to the age of most of the participants, may have led to an underestimation of internalizing difficulties (anxiety, depression). A longer follow up would also help to better understand if the signs of emotional dysregulation, not associated with any confirmed diagnosis on DSM-5, will evolve into more structured signs or, as previously reported, may only be transient in relation to temporary coping abilities or other environmental factors, including parental distress59.
In conclusion, our study suggest that autism spectrum disorder can be found in type I infants with a prevalence that is relatively higher than in the general population. The reason of this relatively high percentage may be due to a multifactorial component. If on one hand there is interest to further understand the possible central nervous system involvement as one of the features of a multisystemic involvement in the more severe form of SMA12, other hypothesis, such as the interaction with multiple genetical and environmental factor interact should also be taken into account. Further genetical and omics studies on individuals with SMA and ASD could help to identify possible interactions between SMN gene and other genes related to ASD. Most importantly, social experiential deprivation due to the high number of hospitalization, fewer motor experiences, poor language abilities in the first ages of life, high parental stress due to early diagnosis of SMA, may also play a role, as previously reported in other populations60.
While further studies may better establish the role and interaction of these different aspects, it is equally important acknowledge the need for an appropriate diagnostic pathway for identifying ASD in SMA patients. Our findings suggest that this may be extremely challenging, and the administration of a comprehensive clinical evaluation employing a combination of structured tools, direct observations, and information from parents may be strategic. Even if we performed a selection of the tests to be used, excluding those who had already been reported to be less suitable for infants and children with motor impairment, we and the families observed that some of the tools used in this study did not appear to be fully appropriate for our cohort. As reported by parents, the majority of the items of the SP2 questionnaires and a limited number of items of SCQ were dependent on motor function and not suitable for this cohort. While our study provides additional information on the suitability of the used tests, it is still necessary to conduct further work in this area and design new modalities of observation using environmental elements tailored to the specific difficulties of children with SMA such as a more structured choice of materials and activities for weak children. Further studies are also needed to investigate the impact of low levels of SMN protein during early stages of brain development12.
Subjects and methods
This prospective cross-sectional study was conducted between November 2023 and April 2024 at Nemo Pediatric Medical Center, part of the Women, children, and Public Health Sciences Department of the Fondazione Policlinico Universitario Agostino Gemelli IRCCS in Rome. Children with genetically confirmed SMA diagnoses prospectively followed at Nemo Center for clinical consultation were enrolled.
Demographic and clinical information were collected, including sex assigned at birth, data on ethnicity and race, SMN2 copy number, SMA I subclassification61, treatment start date, motor function, social and material vulnerability index62, and parental education levels.
Any previous clinical evaluations on developmental and cognitive tests were extracted from the medical record. After the comprehensive clinical assessment, a multidisciplinary team screened each child for neurodevelopmental and mental disorders according to the DSM-5 criteria assessment. All study procedures were approved by the ethics committee of the Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome (Date 26/05/2020, no 1894). Written informed consent was obtained from all the subjects and/or their legal guardians (research consent). All experiments were performed in accordance with relevant guidelines and regulations.
All children were assessed by a multidisciplinary team (a child psychiatrist, a neuro and psychomotor therapist63 a child neurologist, neuroscientist experts on autism, psychologists) with a battery of tests that included both screening questionnaires and dedicated diagnostic tools for neurodevelopmental and mental disorders. This included a semi-structured clinical observation, the Childhood Autism Rating Scale (CARS)64 and the following parental questionnaire: Strengths and Difficulties Questionnaire (SDQ-P)65, Social Communication Questionnaire (SCQ)66, Sensory Profile2 (SP2)67.
Parental questionnaires
Two trained clinicians (BB, CC) instructed parents to fill out three parental questionnaires widely used in mental health care and research settings.
The SDQ-P provides information on children’s behaviors. Its scoring yields five scales: emotional symptoms, conduct problems, hyperactivity/inattention, peer relationship problems, and prosocial behavior. Literature data indicates that the prosocial scale is the strongest indicator of autism spectrum disorder51,52. This study used the two Italian versions of the SDQ-P based on the subject’s age (2–4 years or 4–17 years).
The SCQ is a tool screening for ASD. Two forms are available, “Current”, which looks at the child’s last 3 months and can be completed by two years of age, and “Lifetime”, which looks at the child’s developmental history and can be completed for children from the age of four years. In this study, the Italian version of SCQ was used, and the cut-off of 15 was selected, as it is commonly considered suggestive of ASD presence68. Some studies suggest considering scores between 11 and 15 in high functioning population68.
The SP2 is a norm-referenced questionnaire used to identify sensory processing patterns and assess the effect of different sensory processing patterns on functional performance. SP2 score classify children’s level of sensory abnormality based on score percentiles from a large normative sample. This study used the two Italian versions of SP2 based on the subject’s age (7–36 months or 3–10 years).
Two assessors (BB, CC) scored SDQ-P, SCQ, and SP2 according to existing validated algorithm. Since some activities described in questionnaires may not be performed due to strength issues for children with an SMA diagnosis, parents were instructed to specify any items they deemed unsuitable for their child’s motor ability level.
Neurobehavioral observation
In order to obtain additional information to the parent reported questionnaires, we included a clinical play observation. The neurobehavioral observation69 was conducted by two independent and trained clinicians (BB, CC) and proceeded through two steps:
-
1.
“Observation of the child’s spontaneous behavior” focusing on spontaneous play, spatial exploration, approaches to objects, action patterns used, and the type of play implemented.
-
2.
“Engagement with the play set.” Focusing on the child’s reaction to the changed play scheme or activities introduced by clinicians. Several domains and symptoms were specifically observed: ability to organize his/her own game, engaging/sharing the playset with the caregiver/clinician, content of the playset, eye contact, facial expression, communication and social interaction, patterns of behavior, interests, or restricted and repetitive activities, behavioral issues (irritability, oppositive behavior, hyperactivity, conduct problems, anxiety), emotional dysregulation (inability to regulate the intensity and quality of emotions to generate an appropriate emotional response). As regards emotional dysregulation, which is a trans diagnostic entity, neurobehavioral observation was scored as present if the child presented an impaired regulation of emotional states, including mood lability and instability, severe irritability, low tolerance to frustration, temper outburst, and hyperarousal70 referring to the to characteristic reported in recent literature 71,72,73,74.
Each neurobehavioral observation was independently labeled as negative, borderline, or positive according to the clinical judgment of the two assessors. Conflicts were solved with the intervention of senior clinicians employed at the Nemo Pediatric Medical Center. Concordance between raters was 93%.
Childhood autism rating scale, 2nd edition
The CARS2 is a well-validated clinical tool to explore ASD symptoms through direct observation of children. CARS2 comprises 15 items that assess a child’s behavior across various domains, including verbal and nonverbal communication, socialization, stereotyped and repetitive behavior, and adaptability to change. Each item is rated on a scale from 1 to 4, with 1 indicating typical behavior and 4 indicating highly atypical behavior. Total scores on CARS2 range from 15 to 60, with higher scores indicating greater severity of symptoms. Two trained clinicians administered the Italian adaptation of the CARS2 (BB, CC) and rated the total score according to existing validated algorithms (a score of < 30 indicates non-autism, a score of 30–36.5 indicates mild to moderate autism spectrum disorder, a score of ≥ 37 indicates severe autism spectrum disorder).
Statistical analysis
Participant characteristics were described using proportions (percentages) for categorical variables, mean with standard deviations (SD), and/or medians with ranges for continuous variables. Parental education levels were classified according to the highest degree obtained (middle school, high school, university). The social and material vulnerability was assessed using the social and material vulnerability index which is a composite score reflecting the risk of adverse social and economic conditions, based on factors such as educational level, family structure, housing conditions, labor market participation, and economic conditions within a specific geographic area75. This index measures varying degrees of exposure to vulnerability, which do not necessarily indicate an actual situation of material and social distress. The index was classified into four levels: low risk (91.12–97.27), medium–low risk (97.28–98.65), medium–high risk (98.6–100.29), and high risk (100.30–119.64).
Fisher’s Exact Test for variable data and Kruskal Wallis for continuous variables were employed to investigate the association between the results from different tools and the variables describing subject characteristics. Due to the small sample size, no association test was conducted between CARS2 and the variables describing subject characteristics. Sensitivity and specificity tests were employed to evaluate the ability of each screening tool (SDQ, SCQ, neurobehavioral observation) to identify a diagnosis coded via DSM-5 and CARS2.
Data availability
Individual participant data that underlie the results reported in this article will be shared, after de-identification beginning 3 months and ending 5 years following article publication, with Researchers who provide a methodologically sound proposal. Proposals should be directed to eugeniomaria.mercuri@unicatt.it; to gain access, data requestors will need to sign a data access agreement.
References
Mercuri, E., Sumner, C. J., Muntoni, F., Darras, B. T. & Finkel, R. S. Spinal muscular atrophy. Nat. Rev. Dis. Primers. 8, 52. https://doi.org/10.1038/s41572-022-00380-8 (2022).
Dubowitz, V. Chaos in classification of the spinal muscular atrophies of childhood. Neuromuscul. Disord. 1, 77–80. https://doi.org/10.1016/0960-8966(91)90051-s (1991).
Al-Zaidy, S. et al. Health outcomes in spinal muscular atrophy type 1 following AVXS-101 gene replacement therapy. Pediatr. Pulmonol. 54, 179–185. https://doi.org/10.1002/ppul.24203 (2019).
Pane, M. et al. Nusinersen in type 1 spinal muscular atrophy: Twelve-month real-world data. Ann. Neurol. 86, 443–451. https://doi.org/10.1002/ana.25533 (2019).
Bitetti, I., Manna, M. R., Stella, R. & Varone, A. Motor and neurocognitive profiles of children with symptomatic spinal muscular atrophy type 1 with two copies of SMN2 before and after treatment: A longitudinal observational study. Front. Neurol. 15, 1326528. https://doi.org/10.3389/fneur.2024.1326528 (2024).
Buchignani, B. et al. Communicative development inventory in type 1 and presymptomatic infants with spinal muscular atrophy: A cohort study. Arch. Dis. Child 109, 395–401. https://doi.org/10.1136/archdischild-2023-326613 (2024).
Tosi, M. et al. Neurocognitive profile of a cohort of SMA type 1 pediatric patients and emotional aspects, resilience and coping strategies of their caregivers. Eur. J. Paediatr. Neurol. 43, 36–43. https://doi.org/10.1016/j.ejpn.2023.02.004 (2023).
Pechmann, A. et al. Effect of nusinersen on motor, respiratory and bulbar function in early-onset spinal muscular atrophy. Brain 146, 668–677. https://doi.org/10.1093/brain/awac252 (2023).
Darras, B. T. et al. Risdiplam-treated infants with type 1 spinal muscular atrophy versus historical controls. N. Engl. J. Med. 385, 427–435. https://doi.org/10.1056/NEJMoa2102047 (2021).
Al-Zaidy, S. A. et al. AVXS-101 (Onasemnogene Abeparvovec) for SMA1: Comparative study with a prospective natural history cohort. J. Neuromuscul. Dis. 6, 307–317. https://doi.org/10.3233/JND-190403 (2019).
Erdos, J. & Wild, C. Mid- and long-term (at least 12 months) follow-up of patients with spinal muscular atrophy (SMA) treated with nusinersen, onasemnogene abeparvovec, risdiplam or combination therapies: A systematic review of real-world study data. Eur. J. Paediatr. Neurol. 39, 1–10. https://doi.org/10.1016/j.ejpn.2022.04.006 (2022).
Masson, R., Brusa, C., Scoto, M. & Baranello, G. Brain, cognition, and language development in spinal muscular atrophy type 1: A scoping review. Dev. Med. Child Neurol. 63, 527–536. https://doi.org/10.1111/dmcn.14798 (2021).
Lipnick, S. L. et al. Systemic nature of spinal muscular atrophy revealed by studying insurance claims. PLoS ONE 14, e0213680. https://doi.org/10.1371/journal.pone.0213680 (2019).
Finkel, R. S. et al. Diagnosis and management of spinal muscular atrophy: Part 2: Pulmonary and acute care; medications, supplements and immunizations; other organ systems; and ethics. Neuromuscul. Disord. https://doi.org/10.1016/j.nmd.2017.11.004 (2017).
Mercuri, E. et al. Diagnosis and management of spinal muscular atrophy: Part 1: Recommendations for diagnosis, rehabilitation, orthopedic and nutritional care. Neuromuscul. Disord. https://doi.org/10.1016/j.nmd.2017.11.005 (2017).
Salmin, F. et al. Resolution of skin necrosis after nusinersen treatment in an infant with spinal muscular atrophy. Muscle Nerve 59, E42–E44. https://doi.org/10.1002/mus.26457 (2019).
Oskoui, M. et al. The changing natural history of spinal muscular atrophy type 1. Neurology 69, 1931–1936. https://doi.org/10.1212/01.wnl.0000290830.40544.b9 (2007).
Battaglia, G., Princivalle, A., Forti, F., Lizier, C. & Zeviani, M. Expression of the SMN gene, the spinal muscular atrophy determining gene, in the mammalian central nervous system. Hum. Mol. Genet. 6, 1961–1971. https://doi.org/10.1093/hmg/6.11.1961 (1997).
Tizzano, E. F., Cabot, C. & Baiget, M. Cell-specific survival motor neuron gene expression during human development of the central nervous system: Implications for the pathogenesis of spinal muscular atrophy. Am. J. Pathol. 153, 355–361. https://doi.org/10.1016/S0002-9440(10)65578-2 (1998).
Devriendt, K. et al. Clinical and molecular genetic features of congenital spinal muscular atrophy. Ann. Neurol. 40, 731–738. https://doi.org/10.1002/ana.410400509 (1996).
Harding, B. N. et al. Spectrum of neuropathophysiology in spinal muscular atrophy type I. J. Neuropathol. Exp. Neurol. 74, 15–24. https://doi.org/10.1097/NEN.0000000000000144 (2015).
Araki, S. et al. Neuropathological analysis in spinal muscular atrophy type II. Acta. Neuropathol. 106, 441–448. https://doi.org/10.1007/s00401-003-0743-9 (2003).
Ito, Y. et al. Thalamic lesions in a long-surviving child with spinal muscular atrophy type I: MRI and EEG findings. Brain Dev. 26, 53–56. https://doi.org/10.1016/s0387-7604(03)00075-5 (2004).
Mendonca, R. H. et al. Severe brain involvement in 5q spinal muscular atrophy type 0. Ann. Neurol. 86, 458–462. https://doi.org/10.1002/ana.25549 (2019).
Maeda, K. et al. Global central nervous system atrophy in spinal muscular atrophy type 0. Ann. Neurol. 86, 801–802. https://doi.org/10.1002/ana.25596 (2019).
Baranello, G. & Neurodevelopment in, S. M. A. W. G. The emerging spectrum of neurodevelopmental comorbidities in early-onset Spinal Muscular Atrophy. Eur. J. Paediatr. Neurol. 48, 67–68. https://doi.org/10.1016/j.ejpn.2023.11.006 (2024).
Alıcı, N. et al. P213 Beneath the iceberg: spinal muscular atrophy (SMA) and autistic spectrum disorder. Neuromuscul. Disord. 33, S88. https://doi.org/10.1016/j.nmd.2023.07.095 (2023).
Abdul Hamid, O. et al. Rate of autism or cognitive delay in spinal muscular atrophy; A single center 1 Year experience. Muscular Dystrophy Association Clinical and Scientific Conference. Poster Number: T390. https://www.mdaconference.org/abstract-library/rate-of-autism-or-cognitive-delay-in-spinal-muscular-atrophy-a-single-center-1-year-experience/ (2025).
Polido, G. J. et al. Cognitive performance of children with spinal muscular atrophy: A systematic review. Dement Neuropsychol. 13, 436–443. https://doi.org/10.1590/1980-57642018dn13-040011 (2019).
Giannotta, G., Ruggiero, M., De Rinaldis, M. & Trabacca, A. Exploring variability in cognitive functioning in patients with spinal muscular atrophy: A scoping review. Neurol. Sci. 45, 3699–3710. https://doi.org/10.1007/s10072-024-07503-x (2024).
Diagnostic and statistical manual of mental disorders: DSM-5™. 5th edn. (American Psychiatric Publishing, a division of American Psychiatric Association, 2013).
International classification of diseases. 11th revision. (World Health Organization, 2018).
Yu, Y., Ozonoff, S. & Miller, M. Assessment of autism spectrum disorder. Assessment 31, 24–41. https://doi.org/10.1177/10731911231173089 (2024).
Greene, R. K., Vasile, I., Bradbury, K. R., Olsen, A. & Duvall, S. W. Autism diagnostic observation schedule (ADOS-2) elevations in a clinical sample of children and adolescents who do not have autism: Phenotypic profiles of false positives. Clin. Neuropsychol. 36, 943–959. https://doi.org/10.1080/13854046.2021.1942220 (2022).
Colombi, C., Fish, A. & Ghaziuddin, M. Utility of the ADOS-2 in children with psychiatric disorders. Eur. Child Adolesc. Psychiatry 29, 989–992. https://doi.org/10.1007/s00787-019-01411-8 (2020).
Maddox, B. B. et al. The accuracy of the ADOS-2 in identifying autism among adults with complex psychiatric conditions. J. Autism. Dev. Disord. 47, 2703–2709. https://doi.org/10.1007/s10803-017-3188-z (2017).
Colombo, P. et al. Assessing mental health in boys with Duchenne muscular dystrophy: Emotional, behavioural and neurodevelopmental profile in an Italian clinical sample. Eur. J. Paediatr. Neurol. 21, 639–647. https://doi.org/10.1016/j.ejpn.2017.02.007 (2017).
Simone, M. et al. Autism spectrum disorder and Duchenne muscular dystrophy: A clinical case on the potential role of the dystrophin in autism neurobiology. J. Clin. Med. https://doi.org/10.3390/jcm10194370 (2021).
Parravicini, S., Quaranta, C. A., Dainesi, M. I. & Berardinelli, A. The hidden face of Duchenne (neuro) muscular dystrophy. Preliminary evidence of social cognition impairment as a feature of the neuropsychological phenotype of DMD. Front. Psychol. 15, 1504174. https://doi.org/10.3389/fpsyg.2024.1504174 (2024).
Passos-Bueno, M. R., Costa, C. I. S. & Zatz, M. Dystrophin genetic variants and autism. Discov. Ment. Health 2, 4. https://doi.org/10.1007/s44192-022-00008-z (2022).
Ekström, A., Lindeblad, G. & Sofou, K. P. 25A longitudinal study of autism spectrum disorders in children, adolescents and young adults with congenital and childhood myotonic dystrophy type 1. Neuromusc. Disord. 29, S48–S49. https://doi.org/10.1016/j.nmd.2019.06.054 (2019).
Wechsler, D. Wechsler Intelligence Scale for Children. Psychological Corporation. (1949)
Farmer, C. in Encyclopedia of Autism Spectrum Disorders (ed Fred R. Volkmar) 1732–1735 (Springer, 2013).
Raven, J. The raven progressive matrices tests: Their theoretical basis and measurement model. Uses and Abuses of Intelligence: Studies Advancing Spearman and Raven’s Quest for Non-arbitrary Metrics (2008).
Luiz, D. M., Foxcroft, C. D. & Stewart, R. The construct validity of the Griffiths scales of mental development. Child Care Health Dev. 27, 73–83. https://doi.org/10.1046/j.1365-2214.2001.00158.x (2001).
Lennon, E. M., Gardner, J. M., Karmel, B. Z. & Flory, M. J. in Encyclopedia of Infant and Early Childhood Development (eds Haith, M. M. & Benson, J. B.) 145–156 (Academic Press, 2008).
Esler, A. N. et al. The autism diagnostic observation schedule, toddler module: Standardized severity scores. J. Autism. Dev. Disord. 45, 2704–2720. https://doi.org/10.1007/s10803-015-2432-7 (2015).
Kuban, K. C. et al. An algorithm for identifying and classifying cerebral palsy in young children. J. Pediatr. 153, 466–472. https://doi.org/10.1016/j.jpeds.2008.04.013 (2008).
Bal, V. H. et al. The adapted ADOS: A new module set for the assessment of minimally verbal adolescents and adults. J. Autism. Dev. Disord. 50, 719–729. https://doi.org/10.1007/s10803-019-04302-8 (2020).
Cordis, C. E. E. Evaluation of Autism SpEctrum Disorder in children with Cerebral Palsy (EASED-CP, 2022).
Russell, G., Rodgers, L. R. & Ford, T. The strengths and difficulties questionnaire as a predictor of parent-reported diagnosis of autism spectrum disorder and attention deficit hyperactivity disorder. PLoS ONE 8, e80247. https://doi.org/10.1371/journal.pone.0080247 (2013).
Grasso, M., Lazzaro, G., Demaria, F., Menghini, D. & Vicari, S. The strengths and difficulties questionnaire as a valuable screening tool for identifying core symptoms and behavioural and emotional problems in children with neuropsychiatric disorders. Int. J. Environ. Res. Publ. Health. https://doi.org/10.3390/ijerph19137731 (2022).
Janssens, A. & Deboutte, D. Screening for psychopathology in child welfare: The strengths and difficulties questionnaire (SDQ) compared with the Achenbach system of empirically based assessment (ASEBA). Eur. Child Adolesc. Psychiatry 18, 691–700. https://doi.org/10.1007/s00787-009-0030-y (2009).
Global Burden of Disease (GBD) network. GBD study. (Website, 2021).
World Health, O. Depression and other common mental disorders: global health estimates. (World Health Organization, 2017).
Lin, X., He, T., Heath, M., Chi, P. & Hinshaw, S. A systematic review of multiple family factors associated with oppositional defiant disorder. Int. J. Environ. Res. Publ. Health https://doi.org/10.3390/ijerph191710866 (2022).
Delamater, A. M., Guzman, A. & Aparicio, K. Mental health issues in children and adolescents with chronic illness. Int. J. Human Rights Healthc. 10, 163–173. https://doi.org/10.1108/IJHRH-05-2017-0020 (2017).
Landfeldt, E. et al. Caregiver burden of spinal muscular atrophy: A systematic review. Pharmacoeconomics 41, 275–293. https://doi.org/10.1007/s40273-022-01197-9 (2023).
Du, L., Dong, H., Miao, C., Jia, F. & Shan, L. Analysis of scores of symptom checklist 90 (SCL-90) questionnaire of 182 parents of children with spinal muscular atrophy: A cross-sectional study. Transl. Pediatr. 11, 1776–1786. https://doi.org/10.21037/tp-22-464 (2022).
Kaku, S. M. et al. Social experiential deprivation in autism spectrum disorders: A possible prognostic factor?. Asian J. Psychiatr. 26, 44–45. https://doi.org/10.1016/j.ajp.2017.01.021 (2017).
Finkel, R., Bertini, E., Muntoni, F., Mercuri, E. & Group, E. S. W. S. 209th ENMC international workshop: Outcome measures and clinical trial readiness in spinal muscular atrophy 7-9 November 2014, Heemskerk, The Netherlands. Neuromuscul. Disord. 25, 593–602. https://doi.org/10.1016/j.nmd.2015.04.009 (2015)
Istituto Nazionale di Statistica. Le misure della vulnerabilità: un’applicazione a diversi ambiti terrioriali. (2020).
Purpura, G. & Coratti, G. Neuro and psychomotor therapist of developmental age professional in Italy: An anomaly or an opportunity?. Archiv. Rehabil. Res. Clin. Trans. 6, 100372. https://doi.org/10.1016/j.arrct.2024.100372 (2024).
Kaat, A. & Lecavalier, L. in Encyclopedia of Autism Spectrum Disorders (ed Volkmar, F. R.) 590–593 (Springer, 2013).
Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatr. 38, 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x (1997).
Snow, A. in Encyclopedia of Autism Spectrum Disorders (eds Volkmar, F. R.) 2893–2895 (Springer, 2013).
Dunn, W. Sensory Profile: User’s Manual. xiv, 146: illustrations; 28 cm (Psychological Corp., 1999).
Scattoni, M. L. et al. Autism spectrum disorder prevalence in Italy: A nationwide study promoted by the Ministry of Health. Child Adolesc Psychiatry Ment. Health 17, 125. https://doi.org/10.1186/s13034-023-00673-0 (2023).
Coulehan, K. & Baron, I. S. in Encyclopedia of the Neurological Sciences (Second Edition) (eds Aminoff, M. A. & Daroff, R. B.) 528–531 (Academic Press, 2014).
Masi, G. et al. An exploratory study of emotional dysregulation dimensions in youth with attention deficit hyperactivity disorder and/or bipolar spectrum disorders. Front Psychiatry 12, 619037. https://doi.org/10.3389/fpsyt.2021.619037 (2021).
Paulus, F. W., Ohmann, S., Mohler, E., Plener, P. & Popow, C. Emotional dysregulation in children and adolescents with psychiatric disorders. A narrative review. Front Psychiatry 12, 628252. https://doi.org/10.3389/fpsyt.2021.628252 (2021).
Marques, S., Correia-de-Sa, T., Guardiano, M., Sampaio-Maia, B. & Ferreira-Gomes, J. Emotion dysregulation and depressive symptoms mediate the association between inhibitory control difficulties and aggressive behaviour in children with ADHD. Front Psychiatry 15, 1329401. https://doi.org/10.3389/fpsyt.2024.1329401 (2024).
Brown, M. A. et al. Understanding emotion dysregulation from infancy to toddlerhood with a multilevel perspective: The buffering effect of maternal sensitivity. Dev. Psychopathol. https://doi.org/10.1017/S0954579424000774 (2024).
Saccaro, L. F., Giff, A., De Rossi, M. M. & Piguet, C. Interventions targeting emotion regulation: A systematic umbrella review. J. Psychiatr. Res. 174, 263–274. https://doi.org/10.1016/j.jpsychires.2024.04.025 (2024).
Tronu, D., Istat. Le misure della vulnerabilità: un’applicazione a diversi ambiti territoriali. Istat. https://www.istat.it/it/files/2020/12/Le-misure-della-vulnerabilita.pdf (2020).
Acknowledgements
We thank Caterina Fedi MD, for her precious contribution in the discussion of some of the reported cases.
Funding
There was no role of the funding sources in the study design, collection, analysis and interpretation of data, and in the decision to submit the paper for publication. GCor: Italian Ministry of Health (GR-2021-12374579). BB and PC are partially supported by the Italian Ministry of Health Grant RC 2024 to IRCCS Stella Maris Foundation. MCP: Italian Ministry of Health (GR-2018-12365706). EM: Italian Ministry of Health (RF-2019-12370334).
Author information
Authors and Affiliations
Contributions
BB, GC, CC, EM, had a major role in conception and design of the study, acquisition and analysis of data and drafting a significant portion of the manuscript or figures. MP, MLS, FF, GB, participated in drafting a significant portion of the manuscript or figures and acquisition and analysis of data. CP, DL, MCP, CoC, CB, PC participated in the conception and design of the study and acquisition and analysis of data. RDS, GS, LA participated in the acquisition and analysis of data.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Buchignani, B., Coratti, G., Cutrì, C. et al. Neurodevelopmental and mental disorders in children with type I and presymptomatic spinal muscular atrophy. Sci Rep 15, 26984 (2025). https://doi.org/10.1038/s41598-025-12484-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-12484-8
