
Abstract
Peripheral T-cell lymphomas (PTCLs) represent a heterogeneous group of rare malignancies with poor survival; however, population-based long-term survival data remain limited. We conducted a nationwide study to estimate overall survival (OS) and relative survival (RS) among 915 patients diagnosed with PTCLs from 2002 − 2018 (57% males, median age 67 years) using the Finnish Cancer Registry. The most common subtypes included PTCL not otherwise specified (PTCL NOS; 37%), angioimmunoblastic T-cell lymphoma (AITL; 27%), and ALK-anaplastic large cell lymphoma (ALK-ALCL; 12%). Age > 60 years at diagnosis, advanced stage, and male sex were associated with poorer OS. Five-year OS and RS were better in patients with ALK + ALCL compared with PTCL NOS (5-year OS: 85% vs 30%). Patients with ALK- ALCL had a favorable 5-year OS compared to PTCL NOS (46% vs 30%), while those with enteropathy-associated T-cell lymphoma (EATL) demonstrated worse OS (15%). There was no improvement in RS from 2002 − 2012 to 2013 − 2018. OS was better in patients (excluding ALK + ALCL) receiving high-dose chemotherapy (HDCT) compared to those for whom HDCT was not planned (HR 0.61; 95% CI 0.47 − 0.80). We conclude that RS did not improve during the study period; however, consolidation with HDCT for eligible patients resulted in favorable survival.
Similar content being viewed by others

Introduction
Peripheral T-cell lymphomas (PTCLs) are a heterogeneous group of rare lymphoid malignancies constituting 5–10% of all malignant lymphomas1,2,3. In the recent WHO-HAEM5 classification, mature T-cell and NK-cell neoplasms are grouped into nine families on the basis of their cell of origin, differentiation state, clinical findings, disease localization, and morphology and are further divided into more than 30 distinct subtypes4. This recent WHO revision brings in a new family of nodal T-follicular helper (TFH) cell lymphomas that include angioimmunoblastic T-cell lymphoma (AITL)4,5. The incidence of various subtypes varies geographically1, and in Western countries, the most common subtypes are PTCL not otherwise specified (PTLC NOS), AITL,anaplastic large cell lymphomas (ALCL), either ALK (anaplastic lymphoma kinase) negative (ALK-) or ALK positive (ALK +) and enteropathy-associated T-cell lymphoma (EATL)1,2,6,7.
Compared with B-cell lymphomas, PTCLs have dismal outcomes, with a 5-year overall survival (OS) of 34–48%. An exception is the ALK + ALCL subtype, with a 5-year OS of 58–79%1,2,6,8,9. Treatment of PTCL patients is usually based on cyclophosphamide, doxorubicin, vincristine, and prednisolone (CHOP) combination chemotherapy10. The impact of adding etoposide to the CHOP regimen (CHOEP) is controversial. More complete responses have been achieved with CHOEP than with CHOP2,6, which, however, has not translated to improved OS2,11,12except in ALK + ALCL6,9,13. Various new drugs have been studied to improve survival in PTCL patients, but to date, only brentuximab vedotin combined with a CHP backbone (vincristine omitted) has improved survival in CD30-positive PTCL patients, with 75% of the studied patients having the ALCL subtype14..
Due to the poor survival rates of patients with PTCL, consolidation with high-dose chemotherapy and autologous stem cell transplantation (HDCT/ASCT) is generally included in the treatment recommendations for PTCL, excluding ALK + ALCL, which nevertheless has superior survival10,15. The favorable impact of HDCT/ASCT on the survival of patients with PTCL has only been demonstrated to date in prospective nonrandomized phase II trials with a 5-year OS of approximately 50%16,17. In the COMPLETE study, the survival benefit of HDCT/ASCT was observed in patients with AITL and those with advanced-stage disease or high IPI scores18. Moreover, allogeneic transplantation did not improve survival compared with HDCT/ASCT19..
Population-based long-term data on systemic PTCLs are limited2,8. We conducted a nationwide population-based study in patients diagnosed with systemic PTCLs in Finland between 2002 and 2018 to determine OS and relative survival (RS) rates. We also compared baseline characteristics and the impact of different first-line chemotherapy regimens and consolidation with HDTC/ASCT on total mortality.
Methods
Data sources
The data were obtained from the Finnish Cancer Registry (FCR), which is a statistical and epidemiological research institute in Finland. In accordance with special legislation, physicians, hospitals, and pathology and hematology laboratories are obliged to report new cancer cases to the FCR without the consent of patients. Thus, FCR includes nationwide data on the incidence of all cancers in Finland since 1953. The information on death for cancer patients is received from Statistics Finland once per year and can be linked to the FCR data via a unique personal identity code included in the registries.
Since 2007, the coding of cancer cases has followed the International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3), which is consistent with the World Health Organization (WHO) Classification of Tumors of Haematopoietic and Lymphoid Tissues, 4th edition5. In 2007, former codes based on the Manual of Tumor Nomenclature and Coding were also converted to ICD-O-320,21. The FCR has high overall coverage, the completeness for lymphoid cancers has been estimated to be 94%, and 99% of cases are morphologically verified22..
Patients
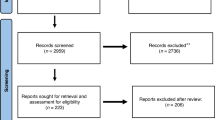
We identified 1123 patients who were diagnosed with PTCL (ICD-O-3 morphology codes 9702, 9705, 9714, 9716, 9717, 9719 9590, 9591) between January 1 st, 2002, and December 31 st, 2018, with follow-up information until December 31 st, 2022, from the FCR. The diagnoses were verified by reviewing pathology and clinical reports linked to the registry, but no new histopathological review was performed. Patients without clear confirmation of systemic PTCL were excluded (n = 49). Patients with only solitary skin involvement who were treated without systemic chemotherapy were considered to have cutaneous T-cell lymphomas (n = 81) and were excluded, as were those with leukemic forms of T-cell lymphomas or other types of cancer (n = 24). In addition, patients were excluded if the diagnosis was confirmed the first time at autopsy or after the patient had died (n = 54). After the exclusions mentioned above, the study population consisted of 915 patients.
Clinical data on stage, extranodal disease involvement, information on first-line treatment, including the given chemotherapy combination, the number of given chemotherapy cycles, and the response to first-line treatment, were retrieved from the electronic medical records (EMR) of the three largest university hospitals in Finland and were reported to the FCR. We grouped the patients according to the treatment data into no treatment groups, which included treatment with corticosteroids and palliative radiation therapy only, CHOP-based, CHOEP-based, and other types of chemotherapy. If a patient had received any number of CHOP cycles without the addition of etoposide, we grouped the patient into the CHOP group. If the patient had received at least one course of the CHOEP, we grouped the patient into a CHOEP group (intention to treat with the CHOEP).
The data on treatments, response to first-line therapy, and the intention to consolidate with HDCT/ASCT were based on data collected from the EMR. If HDTC/ASCT was not mentioned, we grouped the patient as not scheduled for HDCT/ASCT.
This study was performed according to the Declaration of Helsinki. The study was approved by the National Institute for Health and Welfare (Dnro THL/1441/5.05.00/2019), Statistics Finland (Dnro TK-53–1172-19), and Helsinki University Hospital Institutional Review Board. Written informed consent was waived due to the retrospective nature of the study and the de-identification of the patient information. All methods were carried out following the WHO and ICD-O-3 guidelines and recommendations.
Statistical analysis
OS was defined as the time from the date of diagnosis to death from any cause or the last follow-up on December 31th, 2022. OS was estimated with the Kaplan–Meier method, and hazard ratios (HRs) were calculated with a 95% confidence interval (CI) Cox regression model. The log-rank test was applied for group comparisons when appropriate. Patients with missing data were excluded from the analysis. Relative survival (RS) was estimated via the Ederer II method with internal age standardization (age groups: 0 − 44, 45 − 54, 55 − 64, 65 − 74, and ≥ 75 years)23. The follow-up time was split into monthly intervals. Age-specific RS was estimated for three age groups on the basis of the age at diagnosis (0 − 54, 55 − 74, and ≥ 75 years). A complete analysis was based on all person-time and deaths from 1995 − 2018, and period analyses were carried out for 2002 − 2012 and 2013 − 2018, separately, with left-truncated data for the later period24. The baseline demographics of the different subtype groups were compared with the Bonferroni-adjusted Chi-square test or analysis of variance. The statistical analysis was conducted with SPSS version 27 (IBM Armonk) and R, version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria), with the packages survival 3.1–12, rstpm2 1.5.2, Epi 2.44, and popEpi 0.4.8.
Results
Patient characteristics
Altogether, 915 patients were identified with newly diagnosed PTCLs in Finland between 2002 and 2018 with follow-up information until the end of 2022; the median follow-up for surviving patients was 11.6 years (interquartile range (IQR) 8.0–14.9 years).
The clinical characteristics and distributions of the different subtypes are presented in Table 1. PTCL NOS was the most common entity (37%), followed by AITL (27%), ALK- ALCL (12%), and EATL (10%). In 38 (19%) patients with ALCL, the ALK status was unknown (ALCL ALKu).
The median age for the whole cohort was 67 years (IQR 57–77, range 4.3–94.5), with patients with ALK + ALCL being significantly younger (median 36 years at diagnosis, IQR 20–51, range 4.3–81.4), except when compared with hepatosplenic T-cell lymphoma patients (HSTCL). On the other hand, patients with AITL were significantly older than patients with ALK-ALCL and extranodal NK/T-cell lymphoma (ENKTL).
There was a slight male predominance (57%) present in all the subgroups. Overall, 75% of the patients had advanced-stage disease (Ann Arbor stages III–IV), with a significantly greater proportion of PTCL NOS (82%) and AITL (90%) patients than ALCL patients. Extranodal disease was present in 73% of the patients. Bone marrow, spleen, gastrointestinal, skin, and lung involvement were present in 20%, 20%, 14%, 14%, and 9% of the patients, respectively. B-symptoms were present in 52% of the patients. Data on lactate dehydrogenase (LDH) levels and performance statuses were not available; therefore, the International Prognostic Index (IPI) could not be calculated.
Overall survival by different subtypes and clinical characteristics
We recorded 679 deaths during the follow-up period (74%). The median overall survival (mOS) for the whole cohort was 1.6 years, and the 5-year OS was 36% (Table 1). Survival was significantly longer in patients with ALK + ALCL than in those with all other entities, with a 5-year OS of 85%. This superior survival was also observed in the Cox multivariable analysis (Table 2). In addition, survival in patients with ALK-ALCL was significantly longer than that in patients with PTCL NOS and AITL. Survival was significantly shorter in patients with EATL and AITL than in those with PTCL NOS (Fig. 1 and Table 2). However, in the Cox multivariable analysis, survival was significantly longer in patients with the AITL subtype than in those with the PTCL NOS when sex and age were also considered.

Overall and relative survival according to different T-cell lymphoma subtypes. A OS according to histological subtypes of PTLC NOS, AITL, ALCL ALK +, and ALCL ALK- patients; B OS according to histological subtypes of HSCTL, EATL, NKTCL, and ALCL ALKu patients;C RS according to the main subtypes of PTCL NOS, AITL, ALCL ALK +, ALCL ALK- and EATL.
Cox regression analyses of the effects of clinical characteristics and subtypes on survival are shown in Table 2. B-symptoms and extranodal disease were associated with inferior survival, although in the multivariable analysis, age and advanced-stage disease were the only variables significantly associated with inferior survival (HR 1.06; 95% CI 1.04–1.07 and HR 1.85; 95% CI 1.34–2.56, respectively). In addition, in the RS (Fig. 2) and Cox multivariable models, male sex had an inferior impact on survival (HR 1.27; 95% CI 1.01–1.6). Kidney involvement was associated with inferior survival (HR 2.77, 95% CI 1.01–7.56), although it was present in only five patients.

Relative survival in patients diagnosed with systemic T-cell lymphoma in Finland from 2002–2018. A Ten-year age-standardized relative survival (RS) for 2002–2018; B Ten-year age-standardized RS for 2002–2012 and 2013–2018; C Ten-year age-specific RS; D Ten-year age-standardized RS by sex.
Relative survival
The 5-year RS for the entire cohort was 39% (95% CI, 36–42). The RS decreased with age; the 5-year RS for patients aged 0‒54 years at diagnosis was 62% (95% CI, 55–68), that for patients aged 55‒74 years was 36% (95% CI, 32‒41), and that for patients aged 75 years or older was 24% (95% CI, 17‒31). The RS was superior for the ALK + ALCL subgroup, at 79% (95% CI, 49–93). There was no improvement in the RS of patients diagnosed in the later calendar period of 2013‒2018 compared with 2002‒2012 (Table 1 and Fig. 2).
First-line treatment
Data on first-line treatment were available for 66% of the patients (n = 608). Of them, 48% (n = 292) received CHOP, 24% (n = 147) received CHOEP, and 14% received other chemotherapies (n = 86). Eighty-three patients (14%) received only corticosteroids or palliative radiotherapy (n = 10) as best supportive care (Supplementary Table S1). The median OS for patients receiving best supportive care was 1.5 months (range 0–120 months).
Of the patients receiving chemotherapy, 76% (n = 321) completed at least four cycles and 24% (n = 99) 1–3 cycles. Data on responses to first-line therapy were available for 78% of the patients showing the overall response rate (ORR) of 78%.
CHOEP is generally recommended only for fit patients, who are usually aged less than 65 years at diagnosis. In our cohort, 20 patients aged over 65 years received CHOEP. Overall, median OS was longer for patients treated with CHOEP compared to CHOP (5-y OS 53% vs 43%, HR 0.64; 95% CI 0.50–0.83), but when considering only patients under 65 years, the difference was not significant (5-y OS 54% vs 50%, HR 0.78; 95% CI 0.56–1.08). The complete response rate (CRR) was higher with CHOEP (59% vs 49%, p = 0.006), but no significant difference in CRR rate was seen in patients under 65 years (61% vs 54%, p = 0.11).
Twelve percent (n = 62) of the patients received radiation therapy as part of their first-line therapy, and 65% of these patients had stage I or II disease (n = 40).
Consolidation with autologous stem cell transplantation
HDCT/ASCT was planned as consolidation in the first-line therapy for 195 patients (56%) under 70 years at diagnosis with 135 (70%) completing it. For the remaining 60 (30%) patients consolidation was not given due to progression (n = 29), infections or other comorbidities (n = 16), mobilization failures (n = 7), patient choice (n = 7), or unknown reasons (n = 1). HDCT/ASCT was not planned in 44% (n = 155) of the patients less than 70 years.
When analyzing the impact of HDCT/ASCT on survival, patients with ALK + ALCL were excluded as only 15% (n = 5) of them received HDCT/ASCT and they nevertheless had superior survival. HDCT/ASCT recipients (n = 130) had better survival (5-y OS 60%) than patients for whom HDCT/ASCT was not planned (n = 130) (5-y OS 32%, HR 0.42; 95% CI 0.31–0.58). Patients for whom HDCT/ASCT was planned but not completed, had the poorest survival (5-y OS 20%, HR 2.36; 95% CI 1.72–3.25), even compared to those patients who never intended to proceed to HDCT/ASCT (HR 1.41; 95% CI 1.0–1.98) (Fig. 3).

Survival according to HDCT/ASCT consolidation.
We then excluded patients with OS < 6 months, no induction chemotherapy, or if HDCT/ASCT was not performed although planned. In the remaining 114 patients, the favorable impact of HDCT/ASCT consolidation on survival was maintained compared to 85 patients not receiving HDCT/ASCT consolidation (HR 0.57; 95% CI 0.40–0.82). This was confirmed in multivariable Cox regression analysis (HR 0.53; 95% CI 0.34–0.83) adjusted with age, advanced stage, extranodal disease, and addition of etoposide to the CHOP-backbone (Table 3).
Among the 260 patients who achieved CR after first line treatment, 117 were intended for HDCT/ASCT. There was a trend toward improved survival in the HDCT/ASCT group (HR 0.73; 95% CI 0.51–1.05). When restricting the analysis to patients who actually underwent HSCT (n = 95), the survival benefit reached statistical significance (HR 0.58; 95% CI 0.40–0.87). There was no significant difference in overall survival (OS) among patients who underwent HDCT/ASCT between the early study period (2002–2012) and the later period (2013–2018).
Discussion
This is a large, population-based study showing the prevalence of PTCL patients in the entire Finnish population over a 17-year time period. The largest subtypes in this cohort were PTCL NOS (37%) and AITL (27%), which is in concordance with the results from the International Peripheral T-cell Lymphoma Project (ITLP) from Europe1. A previous similar cohort from Sweden2 reported a lower proportion of AITL patients (only 14%), but otherwise, the frequencies of different PTCL subtypes were reported to be similar in both Nordic countries.
The median age of all patients was 67 years, with the exception of ALK + ALCL patients, who presented with a significantly lower median age at diagnosis. As previously shown2,16, male sex was also associated with inferior OS and RS in our population (Fig. 2). The IPI score has also been shown to predict survival in patients with PTCL1,2,6,8. Unfortunately, we were not able to calculate the IPI scores of the patients due to a lack of information on performance status and LDH. However, we show that advanced stage disease, age over 60 years at diagnosis, and extranodal disease, which are factors associated with the IPI score, have unfavorable impacts on survival.
The 5-y OS in the whole group was 36%, similar to that reported in the Swedish population (34%)2. The outcome of the ALK + ALCL subtype, with respect to both OS and RS, was superior to that of the other subtypes, as also shown previously1,2,6,825. In addition, the survival of patients with the ALK-ALCL subtype was significantly better than that of PTCL NOS patients, as suggested previously1,16. In our cohort, the AITL subtype also seemed to translate to better outcomes than PTCL NOS when adjusted for age, stage, and extranodal disease, as the patients with AITL were mostly older and had advanced-stage disease more often (Tables 1 and 2).
In our cohort, 14% of the patients never received any chemotherapy, which is comparable to the 16% reported in the Swedish study2. These patients naturally had a detrimental median survival of only 1.5 months. CHOEP is generally recommended in Finland as a treatment for nodal PTCLs in fit patients, who are usually aged less than 60–65 years and have advanced-stage disease. The positive effect of CHOEP has been mostly shown in ALK + ALCL patients2,6,9,11,12. Unlike in a recent Dutch study6, we did not record differences in ORR or survival in favor of the addition of etoposide when focusing only on patients aged less than 65 years or those with the ALK + ALCL subtype alone, which might be due to a more liberal definition of CHOEP-based treatment, as we included in this group any patient receiving at least one cycle of CHOEP, whereas in the Dutch study, the patients were excluded from the CHOEP group if they had received both CHOP and CHOEP courses.
In patients aged less than 70 years at diagnosis, HDCT/ASCT was planned as part of their first-line therapy for 56% of the patients, which is similar to the Swedish cohort (51%). In our study, 70% of the patients actually received HDCT/ASCT, which is in line with the data from the NLG T-01 trial and the Swedish cohort2,16. The main reasons for omitting HDCT/ASCT were progressive disease, serious infection, or other comorbidity-related problems, resulting in overall dismal survival for this group of patients (intended but not receiving HDCT/ASCT). Consolidation with HDCT/ASCT is not generally recommended for patients with ALK + ALCL, because they have superior survival even without it, and this group was also excluded from our analysis regarding the impact of HDCT/ASCT on survival. In this cohort, only five patients (15%) with ALK + ALCL received HDCT/ASCT as consolidation, whereas 35–46% of the patients with other nodal PTCLs had HDCT/ASCT consolidation (Supplementary Table S1). When ALK + ALCL patients were excluded, consolidation with HDCT/ASCT translated to superior survival, also in the intention to treat with HDCT/ASCT group compared to the group with no consolidation planned. As the clinical data were collected retrospectively from the medical records, documentation on the intention to consolidate with HDCT/ASCT may be missing in some cases, especially in patients who are highly symptomatic with rapidly progressing PTCL, causing potential bias in this study.
In the most recent Dutch study6, which evaluated the impact of HDCT/ASCT on the outcome of PTCL patients, a landmark analysis of 9 months was used. On the other hand, we speculated that induction therapy and consolidation with HDCT/ASCT are mostly completed within 6 months of diagnosis. Therefore, we excluded patients with a dismal prognosis, namely, patients with an OS of less than 6 months, patients who received no chemotherapy at all, and patients who intended to be consolidated with HDT/ASCT but failed to receive it. In this cohort, the positive effect of HDCT/ASCT consolidation on survival also remained significant in the multivariate model with age at diagnosis, advanced-stage disease, and the addition of etoposide to the treatment regimen.
On the basis of data from the ECHELON-2 trial14, brentuximab vedotin has been the first-line treatment option for CD30-positive ALCL patients in Finland for only a few recent years. In our cohort, with the data collected up to 2018, there were naturally no brentuximab-based first-line treatment regimens used, and no significant improvement in RS during the study period was recorded (Fig. 2). In the ECHELON-2 trial, 70% of the patients were diagnosed with the ALCL subtype, and both the ALK + and ALCL- ALCL patients had superior OS compared with the other subtypes. Thus, new therapeutic approaches for PTCL subtypes other than ALCL are urgently needed.
The strengths of this study include its population-based design and the use of high-quality nationwide cancer registry data spanning an extensive period of 17 years. Furthermore, all diagnoses were reviewed from the original pathology reports at the Finnish Cancer Registry, with most cases diagnosed in one of Finland’s five university hospitals or reviewed by an expert hematopathologist. However, some limitations require careful consideration. First, we could not perform a central pathology review to confirm the diagnosis. Second, clinical data were collected retrospectively from medical records and were not available for all patients. Consequently, data on frontline therapy and responses were available for 66% and 78% of patients, respectively, while ALK status was unknown for 19% of patients with ALCL. Additionally, the information on HDCT/ASCT consolidation was obtained from electronic medical records, and there were no standardized criteria for proceeding with consolidation. This lack of harmonization may have introduced selection bias, potentially favoring patients with a better initial prognosis.
In conclusion, this large nationwide population-based cohort study with long-term follow-up demonstrated similar incidences of different PTCL subtypes and survival rates, as previously reported, including superior survival of ALCL subtypes, especially ALK + cases. Consolidation with HDCT/ASCT was associated with improved survival and remains a feasible approach when treating PTCL patients, apart from those with ALK + ALCL. However, we recognise that a randomised trial is required to establish the benefit of HDCT/ASCT for PTCL patients. No significant positive effect was observed with the addition of etoposide to the CHOP regimen, leaving the benefit of adding etoposide questionable. Furthermore, overall RS did not improve during the study period, underscoring the urgent need for more effective and innovative therapies for patients with PTCL as well as integrative studies that combine clinical and molecular data to better understand survival disparities in PTCL patients.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Vose, J. M., Neumann, M. & Harris, M. E. International peripheral T-cell and natural killer/T-cell lymphoma study: Pathology findings and clinical outcomes international T-cell lymphoma project. J Clin Oncol. 26(25), 4124–4130 (2008).
Ellin, F., Landström, J., Jerkeman, M. & Relander, T. Real-world data on prognostic factors and treatment in peripheral T-cell lymphomas: A study from the swedish lymphoma registry. Blood 124(10), 1570–1577 (2014).
Rüdiger, T. et al. Peripheral T-cell lymphoma (excluding anaplastic large-cell lymphoma): Results from the non-Hodgkin’s lymphoma classification project. Ann. Oncol. 13(1), 140–149 (2002).
Alaggio, R. et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: Lymphoid neoplasms. Leukemia 36(7), 1720–1748 (2022).
Swerdlow, S. H. et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 127(20), 2391–2405 (2016).
Brink, M. et al. Impact of etoposide and ASCT on survival among patients aged 65 years with stage II to IV PTCL: a population-based cohort study. Blood 140(9), 1009–2132 (2022).
Wang, S. S. et al. Medical history, lifestyle, family history, and occupational risk factors for peripheral T-cell lymphomas: The interlymph non-hodgkin lymphoma subtypes project. J. Natl. Cancer Inst. Monogr. 48(66), 75 (2014).
Savage, K. J., Chhanabhai, M., Gascoyne, R. D. & Connors, J. M. Characterization of peripheral T-cell lymphomas in a single North American institution by the WHO classification. Ann. Oncol. 15(10), 1467–1475 (2004).
Cederleuf, H. et al. The addition of etoposide to CHOP is associated with improved outcome in ALK+ adult anaplastic large cell lymphoma: A nordic lymphoma group study. Br. J. Haematol. 178(5), 739–746 (2017).
d’Amore, F. et al. Peripheral T- and natural killer-cell lymphomas: ESMO-EHA clinical practice guideline for diagnosis, treatment, and follow-up. Ann. Oncol. 36(6), 626–644 (2025).
Deng, S., Lin, S., Shen, J. & Zeng, Y. Comparison of CHOP vs CHOPE for treatment of peripheral T-cell lymphoma: A meta-analysis. Onco. Targets Ther. 12, 2335–2342 (2019).
Kim, Y. A. et al. Redefining the role of etoposide in first-line treatment of peripheral T-cell lymphoma. Blood Adv. 1(24), 2138–2146 (2017).
Schmitz, N. et al. Treatment and prognosis of mature T-cell and NK-cell lymphoma: An analysis of patients with T-cell lymphoma treated in studies of the german high-grade non-hodgkin lymphoma study group. Blood 116(18), 3418–3425 (2010).
Horwitz, S. et al. Brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma (ECHELON-2): a global, double-blind, randomised, phase 3 trial. Lancet 393(10168), 229–240 (2019).
Horwitz, S. M. et al. Cell Lymphomas, Version 2.2022, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 20(3), 285–308 (2022).
d’Amore, F. et al. Up-front autologous stem-cell transplantation in peripheral T-cell lymphoma: NLG-T-01. J. Clin. Oncol. 30(25), 3093–3099 (2012).
Reimer, P. et al. Autologous stem-cell transplantation as first-line therapy in peripheral t-cell lymphomas: Results of a prospective multicenter study. J. Clin. Oncol. 27(1), 106–113 (2009).
Park, S. I. et al. The role of autologous stem cell transplantation in patients with nodal peripheral T-cell lymphomas in first complete remission: Report from COMPLETE, a prospective, multicenter cohort study. Cancer 125(9), 1507–1517 (2019).
Schmitz, N. et al. A randomized phase 3 trial of autologous vs allogeneic transplantation as part of first-line therapy in poor-risk peripheral T-NHL. Blood 137(19), 2646–2656 (2021).
World Health Organization. Manual of the international statistical classification of diseases, injuries, and causes of death based on the recommendations of the seventh revision Conference, 1955, and adopted by the ninth World Health Assembly under the WHO Nomenclature Regulations. (1957). https:// apps.who.int/iris/handle/10665/42900. 1955
American Cancer Society. Manual of tumor nomenclature and coding (American Cancer Society, 1951).
Leinonen, M. K., Miettinen, J., Heikkinen, S., Pitkäniemi, J. & Malila, N. Quality measures of the population-based finnish cancer registry indicate sound data quality for solid malignant tumours. Eur. J. Cancer Oxf. Engl. 77, 31–39 (2017).
Ederer F., Heise H . Instructions to IBM 650 programmers in processing survival computations. Methodological note no. 10. Bethesda: National Cancer Institute; 1959.
Brenner, H. & Gefeller, O. An alternative approach to monitoring cancer patient survival. Cancer 78, 2004–2010 (1996).
Cederleuf, H. et al. Outcome of peripheral T-cell lymphoma in first complete remission: A Danish-Swedish population-based study. Leuk Lymphoma. 58(12), 2815–2823 (2017).
Acknowledgements
This research was funded by grants from the Academy of Finland (SL), Finnish Cancer Organizations (SL), Sigrid Juselius Foundation (SL), University of Helsinki (SL), Helsinki University Hospital (SL), and Finnish Society for Oncology (TR). Open access is funded by the Helsinki University Library.
Funding
Suomen Onkologiayhdistys,Academy of Finland,Finnish Cancer Institute,Sigrid Juséliuksen Säätiö,Helsingin ja Uudenmaan Sairaanhoitopiiri,Helsingin yliopisto
Author information
Authors and Affiliations
Contributions
T.R., I.K., S.J., and S.L. designed and conceived the study. T.R., I.K., K.L., M.P., L.V., and S.M. collected the data. T.R. and I.K. analyzed the data. S.J. and S.L. supervised the study. T.R. wrote the original draft of the manuscript. All the authors interpreted the data, critically reviewed and revised the manuscript, and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Reunamo, T., Kalashnikov, I., Lahtela, K. et al. A Finnish nationwide population-based study on the survival of patients with peripheral T-cell lymphoma. Sci Rep 15, 27077 (2025). https://doi.org/10.1038/s41598-025-12596-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-12596-1
