
Abstract
To explore the effects of two-dimensional dosimetric leaf gap (DLG) on the gamma pass rate (GPR) for single-isocenter multi-target (SIMT) stereotactic radiosurgery for patients with brain metastases. Two-dimensional DLG data were measured by an electronic portal imaging device (EPID) with the sweeping gap methods provided by Varian. A total of 56 arc fields from 28 SIMT patients were analyzed, including 19 with multiple targets and 9 with single targets. The leaf gap in patients’ plan were modified using an in-house program, which adjusted the multileaf collimator positions based on the DLG values from the two-dimensional DLG distribution. Dose measurements were performed with EPID for both the original and modified plans. Comparisons were made between the measurements and the predicted dose planes from the treatment planning system using 3%/2 mm gamma criteria. Additionally, factors influencing the improvements in measurement results were analyzed.Compared to the original plan, the GPR for sweep test plans with leaf gaps of 2 mm, 4 mm, 6 mm, 10 mm, 14 mm, 16 mm and 20 mm increased by 12.2%, 17.6%, 25.4%, 58.2%, 83.6%, 84.3%, and 82%, respectively, after modification. For the clinical VMAT fields, GPR improvements fluctuated significantly due to the variations of modulation complexity score, the monitor units, as well as the number and volume of targets. The maximum GPR improvements with 16% and 36.3% were observed for the single-isocenter single-target and SIMT patients respectively. A linear relationship was found between GPR improvement and both modulation complexity score and the number of targets, whereas no significant correlation was found with monitor units or target volume. The two-dimensional DLG significantly impacts treatment plans for SIMT and single-isocenter single-target patients, particularly for SIMT cases. The GPR improvement correlates linearly with increases in modulation complexity score and the number of targets, while the monitor units and target volume show minimal correlation with GPR improvement. This study underscores the importance of accurate beam modeling as a key factor influencing GPR improvement.
Similar content being viewed by others


Background
Stereotactic radiosurgery (SRS) has emerged as a suggested treatment for patients with a limited amount of brain metastases, particularly those with single-isocenter multi-target (SIMT)1,2. This technique ensures high accuracy while conforming closely to the target with large doses in few fractions, resulting in increased local tumor control and lower toxicity compared with whole brain radiation therapy1,3,4. Volumetric modulated arc therapy (VMAT) is widely used in SRS due to its continuous throughput, excellent conformity and homogeneity index, and enhanced protection for organs at risk5,6.
In VMAT, the radiation delivery aperture is modulated through variation in the leaf positions of the multileaf collimator (MLC) 7. However, some leakage radiation occurs due to the rounded leaf ends of MLC8. In the Eclipse treatment planning system (TPS), the MLC leaf ends are modeled as right angles, leading to discrepancies between the light and radiation fields caused by the rounded tips (Fig. 1). This necessitates the introduction of an offset to enhance the calculated dose precision, ensuring closer alignment with the real dose delivered by the linac9. The dosimetric leaf gap (DLG) in Eclipse represents the offsets between opposing leaf banks (bank A and bank B) 8. Given that SRS with VMAT involves more complex MLC leaf motion than other radiotherapy techniques, even small fluctuations in DLG value can result in significant dosimetric deviation8,10. Therefore, accurately determining the DLG is crucial for the TPS commissioning and precise radiotherapy planning, particularly in SRS7,11.

Illustration of irradiation path through the MLC with rounded end and the relationship between the optical field, radiation filed and DLG.
Several studies have examined the dosimetric effects of DLG value and MLC leaf offsets on dose delivery in various radiotherapy contexts. For example, Kim et al. reported that dose calculation errors decreased by 6.2% for 6 MV X-rays and 5.9% for 6 MV flattening filter-free X-rays with each 1 mm increase in DLG value12. Lin et al. found that the differences of DLG value larger than 0.2 mm could lead to dose variation in the PTV exceeding 1%13. Mei et al. observed a 0.5 mm decrease in DLG when measurement position shifted from the central axis to 2.5 mm along the Y-axis 14. Additionally, Rangel et al. demonstrated that a 1 mm position shift of all MLC leaves led to an average increase in the reference equivalent uniform dose of 2.7% for prostate and 5.6% for head and neck clinical target volume, respectively15. These findings demonstrate the critical role of DLG value and corresponding MLC position accuracy in precise dose calculation.
The vendor-recommended sweeping gap method was used to measure the DLG value at the central axis for MLC modeling in Varian TPS. The DLG value exhibited significant variation across the two-dimensional (2D) distribution, with a variation of 0.3 mm observed for the 40 central MLC leaves (0.5 cm width) and 0.65 mm for the 20 peripheral MLC leaves (1.0 cm width) along the central axis and perpendicular to the MLC leaf travel directions16. Additionally, reductions in DLG of 0.1 mm and 0.3 mm were found in the middle 0.5 cm and outer 1 cm width leaves, respectively, when assessed forwards the direction of leaf movement16. The DLG values also showed slight variations with depth13.
Prior research demonstrated that in cases of whole brain metastases, where radiation areas are extensive, variations in the DLG have dramatic impact on the agreement between calculated and delivered doses, particularly for the maximum dose17. Due to the multiple targets optimization and delivery simultaneously by the SRS with VMAT technique, individual PTVs may be positioned up to 7 cm away from the radiation isocenter4. Thus, any geometric or dosimetric discrepancies can adversely impact local tumor control in accurate SRS4,18. According to the Han et al., the DLG values varying from 0.3 to 1.4 mm can result in 20% increase between the measured and calculated dose4. Furthermore, Prentou et al. observed that a reduction of 0.19 mm in MLC leaf offset could result in over 5% loss of target coverage for patients10. Thus, DLG value is critical for ensuring consistency in dose calculation and delivery.
The electronic portal imaging device (EPID) offers advantages such as a high density of measurement point, robust performance, good temperature stability, and ease of use, making it suitable for detecting 2D DLG distributions19. However, to the best of our knowledge, there has been no publication that investigate the effect of 2D DLG distributions on SRS plans delivered using the SIMT VMAT technique via EPID verification, or analyzing the associated factors influencing GPR improvement.
In this study, we proposed an MLC leaf position adjust approach to measure and evaluate the impact of 2D DLG on patient plans with SIMT for brain with multiple metastases, which are particularly sensitive to DLG fluctuations. Dose was delivered by a 6MV flattening-filter-free photon beam. The 2D DLG distribution map was obtained from the EPID of the Varian linear accelerator (LINAC), and the leaf positions in the SIMT VMAT treatment plans were adjusted according to this 2D DLG map using an in-house software. Gamma pass rate (GPR) improvements and the influencing factors for SIMT brain metastases in SRS-VMAT were explored.
Methods and materials
LINAC, MLC, and EPID
A Varian Vital Beam LINAC (Varian Medical Systems, Palo Alto, CA) mounted with a Millennium 120 MLC system and an amorphous silicon (aSi-1200) EPID was used in this study20. This setup facilitated the delivery and measurement of 2D DLG distribution maps for a 6 MV flattening-filter-free photon beam. The Eclipse TPS (V15.1, Varian Medical Systems, Palo Alto, CA) was employed to optimize and calculate VMAT plans.
The Millennium 120-leaf MLC is composed of 40 pairs of central leaves (spanning from the central axis to 20 cm off axis), and 20 pairs of outer leaves. The leaf widths are 0.5 cm for the central leaves and 1.0 cm for the outer leaves at the isocenter13. The aSi-1200 EPID features a 43*43 cm2 sensitive area consisting of 1190*1190 detector pixels, each one with a size of 0.33*0.33 mm2. Calibration of the EPID involved acquiring both dark filed and flood field images. Dark field images were acquired by averaging a series of measurements taken without radiation, providing pixel offsets. Flood field images were acquired by exposing the EPID to a large, uniform open field that covered the whole active area. Dose normalization was performed by adjusting the dose response to the clinical dose unit. Lastly, pixel corrections were applied using the dark field and flood field data for the Vital Beam 21,22.
Sliding window MLC gap plan
Several sliding window MLC gap plans, provided by Varian through the sweeping gap method, were used to acquire the DLG 2D distribution. The MLC gaps were symmetric about the central axis., with sizes of 2, 4, 6, 10, 14, 16 and 20 mm. The field size was expanded from 10×10 to 15×30 cm2. A fixed speed was set to move the gap from -85 mm to 85 mm, with each field receiving an exposure of 100 monitor units (MU). Different gap sizes represented varying modulation scores, with the 2 mm gap indicating high modulation and the 10 mm gap representing minimally modulation. All gap plans were performed on a Vital Beam LINAC and measured using its integrated EPID.
2D DLG map generation by EPID
The sweeping gap method was used with an amorphous Si EPID (a-Si 1200) as described in Section “LINAC, MLC, and EPID”, replacing the ion chamber. The EPID was treated as a grid of point detectors, where each pixel serves as a sensing element. The portal dosimetry mode was selected for the EPID measurements. The source-to-detector distance of 105 cm was used, with an inherent buildup of about 0.8 cm and the gantry angle at 0◦. A dose of 100 MU with 6MV FFF photon beams were delivered for each field. Customized MATLAB software was developed to generate 2D DLG map based on the results measured by the EPID portal dosimetry.
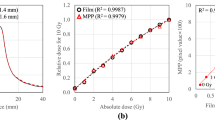
For a specific spatial point (i, j) in the map, the corresponding DLG value, denoted as DLG (i, j), represents the absolute intercept value obtained from linear extrapolation. The linear extrapolation was performed by analyzing corrected gap reading (Rg') as a function of the width in sliding window fields. \({R}_{g{\prime}}\) was calculated as follows:
Here, \({R}_{g}\) accounts for the direct measured dosimetry value of the sweeping gap fields, and \({R}_{T}\) was calculated by averaging the leaf transmission of MLC bank A and bank B. The variable g(mm) denoted the gap width in the sliding window fields. The sweeping gap movement ranges from 2 to 120 mm 23. The measurement fields and the generated DLG map are shown in Fig. 2.

Acquisition process of 2D DLG distribution map. (a) The EPID detection results of the sliding window gap MLC gap plans with gap of 2 mm to 20 mm. (b) Extrapolation graph to calculate the DLG value of each pixel. (c) 2D DLG distribution map.
DLG value evaluation by ionization chamber
A 0.6 cc PTW 30013 Farmer ion chamber (PTW Freiburg, Germany) was utilized for the evaluation of DLG values. A PTW UNIDOS®E electrometer was connected to the ionization chamber placed within a PTW MP1 water phantom to measure DLGion. The chamber was placed underwater at depth of 1.5 cm, with a source to surface distance of 103.5 cm to facilitate comparison with DLG measured by the EPID. DLGEPID was obtained with the source-to-detector distance of 105 cm. The ionization chamber was positioned at distances of 0, ±3 cm, and ±5 cm from the isocenter, in both parallel and perpendicular orientations along the direction of MLC leaf motion, allowing for the detection of the DLGion distribution, marked as ‘⊥’ or ‘∥’. The positive direction is defined as forward and to the right. The corresponding DLGEPID were calculated according to the DLGion position. Both DLGEPID and DLGion values are shown in Table 1.
Patient original and adjusted plan
Nineteen patients with 2–14 targets of brain metastases (ranging from 0.90 to 15.20 cc) and 9 patients with a single target (ranging from 0.20 to 8.60 cc) with SIMT VMAT were selected. The central point of all targets was designated as the isocenter. Two full coplanar arcs with collimator angles set to 5◦ and 355◦ were applied. For all plans, the prescription was set to 30 Gy in five fractions. The Progressive Resolution Optimizer (version 13.5) and Anisotropic Analytical Algorithm in Varian Eclipse TPS were used to the optimization and calculation, respectively. The leaf sequence variability and the aperture area variability were defined to calculate the modulation complexity score (MCS) for each plan fields, following the approach proposed by Masi et al24.
All VMAT plans were calculated with a constant DLG value of 0.21 cm. The original plans (Planorg) were obtained by exporting the plans directly from TPS.
Given the potential variability in DLG values between leaf pairs, discrepancies may arise between the delivered and planned dose distributions, which can be attributed to leaf positioning. To enhance the calculation accuracy, the MLC leaf positions in the Planorg were adjusted based on the corresponding DLG values in the 2D DLG map. An in-house Matlab software (DLGTuner) was customized to integrate the 2D variations of DLG value into the delivery plan. The 2D DLG map was used to adjust every MLC leaf position in the Planorg.
For example, consider leaf pair 58, which has a measured value of 0.25 cm in the 2D DLG map, while the value in the TPS is 0.21 cm. DLGTuner will adjust the gap between leaf 58A and leaf 58B by 0.04 cm. Similarly, each MLC leaf position in all control points from Planorg can be modified. The adjusted plan (denoted as Planadj) was exported from DLGTuner as a DICOM file, ready for delivery to the treatment linac. The running process of the code is illustrated in Fig. 3.

The flowchart of in-house developed software-DLGTuner to adjust the MLC position according to the 2D DLG map.
The performance of DLGTuner was assessed on two key metrics: efficiency and robustness. Efficiency was quantified by measuring the computational time required to generate adjusted plans. Robustness was evaluated by determining the success rate across 10 independent repetitions of the plan generation process.
Patient specific quality assurance using EPID
Criteria of 3% and 2% dose differences with a 2 mm distance to agreement were applied to both the original plans (Planorg) and the adjusted plans (Planadj).
To eliminate the effect of the measurement device variability, patient-specific quality assurance was performed via the same device—an EPID—equipped in the linac, which was also used for DLG measurement as described above. The GPR for the patient plans were calculated by the Varian portal dosimetry system. This was done by comparing the delivered fluence of Planorg and Planadj measured by the EPID with predictions of Planorg calculated by the Portal Dosimetry Image Prediction algorithm of Varian.
Results
DLGEPID vs DLGion
As shown in Table 1, the DLG values measured by EPID (DLGEPID) were generally lower than those measured by the ionization chamber (DLGion). At the isocenter, DLGEPID was 0.95 mm, which is 0.27 mm lower than DLGion. At positions ±3 cm∥ and ±5 cm∥, DLGEPID consistently measured around 0.95 mm, while DLGion was approximately 1.30 mm and 1.40 mm, respectively. For the perpendicular positions at ±3 cm⊥ and ±5 cm⊥, DLGion values were 1.08 mm, 1.20 mm, and 1.21 mm for both, whereas the DLGEPID values were 0.65 mm, 0.58 mm and 0.71 mm, 0.61 mm.
DLGion values at the −3 cm⊥ and –5 cm⊥ remained consistent, with a maximum difference of 0.62 mm at the –3 cm⊥ position and a minimum difference of 0.27 mm at the isocenter. As the distance from the detection point to isocenter increased, the difference also increased. DLGEPID at the isocenter and at ±3 cm∥, ±5 cm∥remained nearly constant, while DLGion values varied. The points at ±3 cm∥ and ±5 cm∥ were consistently higher than at the isocenter. Notably, both DLGEPID and DLGion values at these perpendicular detection points were lower than those in the parallel orientation, except at the +3 cm⊥ position.
Sliding window MLC gap plan
The original plan and the 2D DLG-based adjusted plan for the sliding window MLC gap plan were measured using the EPID device. A comparison between the measured results and the TPS calculated dose was made. Table 2 shows the GPR results with absolute dose criteria of 3%/2 mm and 2%/2 mm, a dose threshold of 10%. For the criterion of 3%/2 mm, the fields with small gaps (2 mm, 4 mm, 6 mm, 10 mm), GPR of Planadj improved by 12.2%, 17.6%, 25.4%, and 58.2%, respectively, compared to Planorg; the larger dynamic gap fields (14 mm, 16 mm, 20 mm), the GPR improvements were even more substantial, with increases of 83.6%, 84.3% and 82%, respectively. As to the criterion of 2%/2 mm, GPR improvements were consistently smaller than those with the criterion of 3%/2 mm across all gap fields, though the same improvement trend was maintained. For the fields with small gap (2 mm, 4 mm, 6 mm, 10 mm), GPR improvements were 8.5%, 11.6%, 17.6%, 33.2% respectively. In contrast, larger fields (14 mm, 16 mm, 20 mm) showed larger improvements of 59.5%, 70.3%, 78.9%.
As the gap increased from 2 to 10 mm, the GPR improvement accordingly increased for both criterion of 3%/2 mm and 2%/2 mm. Beyond a gap of 10 mm, the GPR improvement stabilized with minimal fluctuations for 3%/2 mm and stay increased for 2%/2 mm. (a) For the criterion of 3%/2 mm, both the GPRs for the planorg and planadj were notably low for small gap fields, indicating a significant difference between the measured and predicted planar dose. In contrast, for large gap fields, GPR for the planorg remained low, whereas the planadj showed a significant improvement, with values exceeding 90%. (b) For the criterion of 2%/2 mm, the GPRs of the original plans remained the same as those of 3%/2 mm for fields with gap ranges of 2 mm to 10 mm. However, the GPRs of the adjusted plans were lower for all gap fields. Notably, the GPR improvement values of 2%/2 mm continued to increase across all fields, including the larger gap fields, which differs from the trend observed under 3%/2 mm criterion. As a result, the 2D DLG correction had a substantial impact on GPR for the constant gap dynamic MLC plan.
Patient plan
The DLGTuner exhibited excellent performance in the plan adjustment process. The time of generating the adjusted plan was within 10 to 15 seconds, which depends on the complexity of original plans. Ten consecutive generating processes were performed without any instability for DLGTuner, with complete consistency observed across all generated plans. Besides, DLGTuner demonstrated strong effectiveness in clinic practice. The original plan exported from TPS was modified using DLGTuner, and the resulting plan could be delivered directly on the LINAC after specific patient quality assurance. Therefore, these results confirm the DLGTuner’s reliability and suggest strong potential for clinical implementation.
Both planorg and planadj were measured with EPID. Measured results were compared with the calculated dose of TPS. Absolute dose criteria of 3%/2 mm and 2%/2 mm, global dose normalization, and a dose threshold of 10% were used to calculate the GPR.
Figures. 4 and 5 were the comparisons of distribution and profile between the delivered fluence measured by EPID and patient plans calculated by TPS for both planorg and planadj. The two figures display a multiple target patient with 14 targets and 5.4cc volumes that passed 3%/2 mm criteria at 67.1% for planorg and 99% for planadj. As shown in the figures, the measured dose was higher than the calculated dose for both planorg and planadj in both X and Y directions, especially in the tumor region. For both planorg and planadj, measured dose was aligned with calculated in the low dose region. Compared with the planorg, the dose differences between the measured and calculated were decreased, and the alignment was increased, especially in the Y direction for the planadj. For both planorg and planadj, in the Y direction, the dose fluctuated due to the MLC inter and intra dose variation. Fig. 6a displays the 3%/2 mm GPR for all clinical multi-target VMAT plan fields in relation to the level of modulation, indicated by the MCS. The figure shows that GPR improvements were consistently positive, with GPR for the planadj higher than that for planorg across all cases. The most significant improvements in GPR occurred in highly modulated plans (with low MCS score), with the largest improvement exceeding 35% and the smallest around 5%. This suggests that the 2D DLG correction enhances deliverability and accuracy, especially for highly modulated plans, resulting in better alignment between calculated and delivered doses.

The comparison between the measured and calculated dose for Planorg. (a) dose distribution calculated by TPS. (b) dose distribution measured by EPID. (c) dose profile comparison between measured and calculated in X direction. (d) dose profile comparison between measured and calculated in Y direction.

The comparison between the measured and calculated dose for Plannew. (a) dose distribution calculated by TPS. (b) dose distribution measured by EPID. (c) dose profile comparison between measured and calculated in X direction. (d) dose profile comparison between measured and calculated in Y direction.

The relationship between the GPR improvements and (a) MCS, (b) target number, (c) number of MUs and (d) target volumes for the multiple targets brain metastasis.
Fig. 6b illustrates the relationship between GPR improvement and the number of targets. It is evident that when the target number increases, the GPR improvement becomes more pronounced. For cases with 2 or 4 targets, GPR improvements varied significantly, likely due to additional influencing factors, which is discussed in the following section.
The number of MUs shows a slight correlation with GPR improvement. Plans with a higher number of MUs were prone to show greater GPR improvement (Fig. 6c). However, no significant relationship was observed between GPR improvement and target volume (Fig. 6d).
As shown in Table 3, the mean GPRs of the original plans were 82.8% and 78.7% for multiple targets, 97.2% and 96.5% for single target under the 3%/2 mm and 2%/2 mm criterion, respectively. After applying the 2D DLG correction, the GPR for both multiple and single targets improved to nearly 100% under the 3%/2 mm criterion. However, under the stricter 2%/2 mm criterion, the GPRs were slightly lower for both multiple and single targets. The average GPR improvements for single target plans were 2.59% and 3.07% (standard deviation: 4.29% and 3.21%), while for multi-target plans, the average GPR improvements were 16.52% and 19.77% (standard deviation: 9.37% and 9.71%), under the 3%/2 mm and 2%/2 mm criteria, respectively. Notably, the GPR improvements under the 2%/2 mm criterion were greater than that under the 3%/2 mm criterion for both single and multiple targets, suggesting that the 2D DLG correction is more impactful under stricter evaluation criterion. Furthermore, the GPR improvements for multi-target plans were significantly larger than that for single-target plans for both 3%/2 mm and 2%/2 mm, indicating that the 2D DLG correction has a more substantial impact on dose delivery for patients with multiple targets compared to those with a single target.
Discussion
The values of DLGEPID were approximately 0.3 mm lower than those of DLGion, consistent with findings reported by Mei et al. 14. The under-response of the EPID to smaller doses result in the lower DLG value25. Consequently, a correction of 0.3 mm was applied to each DLG value in the 2D distribution map measured by the EPID to align it with the ionization chamber measurements in TPS.
For 10 MV FFF beams, the dose measured by EPID exhibits distinct characteristics compared to 6 MV FFF beams, primarily attributed to the filtering of low energy and attenuation of MLC-transmitted process26. Furthermore, MLC types variations, such as Millennium MLC and High-definition with different MLC widths, may lead to different transmission dose and DLG values. The EPID’s dose response maintains within 1% deviation from ionization chamber references at low MU (2-4), and 0.4% in the range 4-600 MU for both 6 and 10 MV FFF beams27. Therefore, various energies and MLC types may cause different dose achieved by EPID. The correction value of 0.3 mm was not suitable for beams with different energies and MLC types.
EPID was used to acquire data and measure the patient specific quality assurance in the study. All the results presented were limited to those obtained using the EPID. A limitation of this study is that the performance of other devices, such as ionization chamber array, diode array, film, were not investigated, preventing a comprehensive characterization of each device.
As shown in Table 1, the DLGEPID at the isocenter, ±3cm∥ and ±5cm∥ were approximately 0.95. However, both DLGEPID and DLGion in the perpendicular orientation were lower than those in the parallel orientation. This variation can be contributed to inter- and intra-leaf position discrepancies. As shown in Fig. 7, the dose profile in the parallel orientation across the interleaf region was higher than that in the intra-leaf region. The DLG values for both inter- and intra-leaf positions in the parallel orientation remained consistent, resulting in similar DLG values in the parallel orientation. Sinusoidal patterns with similar amplitudes were observed for inter- and intra-leaf positions in the perpendicular orientation. In addition, the sensitive area of ionization chamber exposed to radiation fields is another factor that can affect the DLG value28. These factors contribute to the observed discrepancies, with the difference between DLGEPID and DLGion being more pronounced in the perpendicular orientation than in the parallel orientation.

Dose profiles of sweeping gap field (2 mm width) acquired by the EPID.
Sait et al29 reported that the GPR declined gradually with the decline of the field size, beginning with a GPR of 99% for a 10×10 cm2 field and decreasing to 43% for a 0.5×0.5 cm2 field, which aligns with our findings shown in Table 2. For sweeping gap fields, varying from 2 to 20 mm, the GPR for the original plan varied between 7.4 and 15.4% for 3%/2 mm, 7.4% and 11.0% for 2%/2 mm. This suggests that the EPID dosimetry response improves with increasing field size30. In smaller fields, the EPID under-response may lead to a lower GPR. Additionally, the accuracy of MLC positioning is critical, as smaller fields are more sensitive to MLC positional errors31. Random fluctuations in MLC position can result in significant dose differences. Furthermore, calibration of the beam for the smallest fields (3×3 cm2) during commissioning may also contribute to the lower GPR.
The GPR improvements fluctuated slightly when the gap ranged from 14 mm to 20 mm under the 3%/2 mm criterion. This suggests that the number of the points of dose differences exceeding 3% could not be reduced below 3% by 2D DLG correction. Factors such as MLC positioning errors, system errors may have contributed to those dose differences. However, dose differences between 2 and 3% could be effectively reduced below 2% with 2D DLG correction. As a result, the GPR improvements increased as the field gap widened under the 2%/2 mm criterion.
As Table 2 shown, the GPR improvements of the 2%/2 mm criterion were smaller than those of 3%/3 mm, likely due to the dose-response characteristics of EPID and the impact of MCS. The GPR improvements increased with the MCS as shown in Fig. 6a. Therefore, we hypothesized that the GPR improvements would continue to rise for the gap larger than 20 mm. This is consistent with the results in Table 3, which indicate that the GPR improvements under the 2%/2mm criterion were greater than those under 3%/2 mm criterion for both multiple and single targets.
The comparison of dose distribution and profile were shown in Fig. 4 and Fig. 5. The GPRs for planorg and planadj were calculated by dose differences and distance to agreement of Figs. 4a and b and 5a and b shown respectively. The alignment between the calculated and measured dose profile out of the tumor in the low dose region means that there is no problem in MLC transmitted factor in Varian TPS MLC modelling. In the tumor region, the great differences arose primarily from DLG deviations, which introduced errors in dose calculations associated with MLC. After the 2D DLG correction, differences between the calculated and measured dose decreased and the gamma pass rate increased from 67.1 to 99%, which indicated that 2D DLG is significant for precise dose calculation.
Fig. 6a illustrates that the GPR for two fields with smaller MCS values (indicating more complex modulation) showed less improvement compared to those with larger MCS values. This is contrary to what we discussed earlier. A possible explanation is that the smallest target volumes in these two fields are only 0.2 cc, where the small segment size and sharp dose fall off contribute to a lower MCS32. The MCS value is calculated based on two parameters: aperture area variability (AAV) and leaf sequence variability (LSV). AAV measures the difference between leaf pair aperture for each segment compared to the maximum leaf separation of the beam24. However, for small targets, each segment is small to achieve adequate dose coverage and sharp dose fall-off outside the target, resulting in inherently small AAV values. These low values do not necessarily reflect real plan complexity since they primarily indicate constrained aperture dimensions rather than complex leaf arrangements.
Similarly, LSV quantifies the variation between adjacent leaves within the same leaf bank24. In small-target plans, only a limited number of leaves (typically 2–3) may be used to shape the target, and the rounded contour of small target further reduces leaf position variations, leading to lower LSV values. Consequently, the low MCS for small targets plans does not accurately represent higher modulation complexity in some cases.
Additionally, MLC position accuracy is also another factor contributes to this phenomenon. Take Vital Beam for example, the MLC position tolerance is 2 mm, which significantly impacts dose delivery accuracy. Thus, MLC accuracy may become the primary factor affecting the GPR for small-volume targets, indicating that 2D DLG correction might not yield substantial GPR improvements in these cases.
As shown in Fig. 6b, the improvement in GPR rises with the targets number, aligning with the results in Table 3. The average GPR improvement for single-target plans was lower than for multi-target plans. More targets necessitate the use of additional 1 cm MLC leaf pairs (those positioned beyond 10.0 mm superior and inferior to the central axis). In the TPS, a constant DLG, typically 0.3–0.6 mm higher than that of the peripheral leaves with 1 cm width, is used 33. For fields with small gap or highly complex plan utilizing leaves of 1 cm width, the DLG value variations between leaf pairs is significant for accurate dose calculation.
The relationship between MCS and the number of MUs is not clearly defined34. However, more complex plans typically require a higher number of MUs to accurately shape beam segments. As shown in Fig. 6d, a weak correlation between GPR improvements and the number of MUs was observed, with a trend suggesting that a higher number of MUs is associated with greater GPR improvement. In some cases with lower complexity, a higher number of MUs may be attributed to the large target volumes.
No clear correlation between target volume and GPR improvements was observed, likely because target volume is affected by both the targets number and the volume of every individual target. These two factors interact in a way that obscures any direction correlation.
Conclusion
The DLG is incorporated for MLC modeling in the Varian TPS. However, the DLG value used in the TPS is measured at the central axis, which differs from the 2D spatial DLG value distribution. With advancements in SRS radiotherapy techniques, highly accurate dose calculations are essential. Thus, we developed a method for adjusting 2D DLG map for SIMT patients undergoing SBRT-VMAT and investigated the factors influencing GPR improvements as measured by EPID. The results show a linear relationship between GPR improvements and both the MCS and number of targets. Specially, GPR improvements increased as MCS decreased and as the target number increased. Notably, the improvements were more significant for multi-target plans compared to single-target plans, though both showed substantial enhancement. The variation in DLG across two dimensions play a critical role in ensuring accurate dose calculations and delivery, especially for SIMT patients.
Data availability
Research data are available on request to the corresponding authors.
Abbreviations
- SRS:
-
Stereotactic radiosurgery
- SIMT:
-
Single-isocenter multi-target
- VMAT:
-
Volumetric modulated arc therapy
- MLC:
-
Multileaf collimator
- TPS:
-
Treatment planning system
- DLG:
-
Dosimetric leaf gap
- EPID:
-
Electronic portal imaging device
- LINAC:
-
Linear accelerator
- GPR:
-
Gamma pass rate
- MU:
-
Monitor units
- MCS:
-
Modulation complexity score
- DLGEPID :
-
DLG values measured by EPID
- DLGion :
-
DLG values measured by ionization chamber
References
Raza, G. H. et al. Single-isocenter multiple-target stereotactic radiosurgery for multiple brain metastases: Dosimetric evaluation of two automated treatment planning systems. Radiat. Oncol. 17(1), 116 (2022).
Kraft, J. et al. Distance to isocenter is not associated with an increased risk for local failure in LINAC-based single-isocenter SRS or SRT for multiple brain metastases. Radiother. Oncol. 159, 168–175 (2021).
Shaaer, A., Osei, E., Darko, J. & Gopaul, D. Dosimetric evaluation of VMAT treatment plans for patients with stage IIB or III non-small cell lung carcinomas. J. Radiother. Pract. 22, e100 (2023).
Han, Z. et al. Optimization of MLC parameters for TPS calculation and dosimetric verification: Application to single isocenter radiosurgery of multiple brain lesions using VMAT. Biomed. Phys. Eng. Exp. 6(1), 015004 (2019).
Saito, M. et al. Dosimetric effects of differences in multi-leaf collimator speed on SBRT-VMAT for central lung cancer patients. Technol. Cancer Res. Treat. 21, 15330338221119752 (2022).
Hanna, S. A., Mancini, A., Dal Col, A. H., Asso, R. N. & Neves-Junior, W. F. P. Frameless image-guided radiosurgery for multiple brain metastasis using VMAT: A review and an institutional experience. Front. Oncol. 9, 703 (2019).
Rahman M, Rabby F, Ahmed R, Bhuiyan MH, Khan KA. Multi Leaf Collimator Transmission Factor and Dosimetric Leaf Gap Measurements Using Calibration Unit Values from Integrated Images. Cureus J. Med. Sci. 2023; 15(4).
Giannakitsas P. Determination and Validation of Dosimetric Leaf Gap (DLG) for IMRT/VMAT and stereotactic treatment plans: University of Patras; 2022.
Rostami, A. et al. Investigating of dosimetric leaf gap and leaf transmission factor variations across gantry and collimator angles in volumetric modulation arc therapy. J. Appl. Clin. Med. Phys. 25, e14523 (2024).
Prentou, G. et al. Impact of systematic MLC positional uncertainties on the quality of single-isocenter multi-target VMAT-SRS treatment plans. J. Appl. Clin. Med. Phys. 23(8), e13708 (2022).
Koger, B. et al. Impact of the MLC leaf-tip model in a commercial TPS: Dose calculation limitations and IROC-H phantom failures. J. Appl. Clin. Med. Phys. 21(2), 82–88 (2020).
Kim, J. et al. Relationship between dosimetric leaf gap and dose calculation errors for high definition multi-leaf collimators in radiotherapy. Phys. Imag. Radiat. Oncol. 5, 31–36 (2018).
Lin, C.-Y. et al. A simple method for determining dosimetric leaf gap with cross-field dose width for rounded leaf-end multileaf collimator systems. Radiat. Oncol. 13(1), 222 (2018).
Mei, X., Nygren, I. & Villarreal-Barajas, J. E. On the use of the MLC dosimetric leaf gap as a quality control tool for accurate dynamic IMRT delivery. Med. Phys. 38(4), 2246–2255 (2011).
Rangel, A. & Dunscombe, P. Tolerances on MLC leaf position accuracy for IMRT delivery with a dynamic MLC. Med. Phys. 36(7), 3304–3309 (2009).
Kumaraswamy, L. K., Schmitt, J. D., Bailey, D. W., Xu, Z. Z. & Podgorsak, M. B. Spatial variation of dosimetric leaf gap and its impact on dose delivery. Med. Phys. 41(11), 111711 (2014).
Szpala, S., Cao, F. & Kohli, K. On using the dosimetric leaf gap to model the rounded leaf ends in VMAT/RapidArc plans. J. Appl. Clin. Med. Phys. 15(2), 67–84 (2014).
Mukwada, G., Chamunyonga, C., Rowshanfarzad, P., Gill, S. & Ebert, M. A. Insights into the dosimetric and geometric characteristics of stereotactic radiosurgery for multiple brain metastases: A systematic review. PLoS ONE 19(8), e0307088 (2024).
Dogan, N. et al. AAPM task group report 307: Use of EPIDs for patient-specific IMRT and VMAT QA. Med. Phys. 50(8), e865–e903 (2023).
Yazdani, S., Takabi, F. S. & Nickfarjam, A. The commissioning and validation of eclipseTM treatment planning system on a varian vitalbeamTM medical linear accelerator for photon and electron beams. Front. Biomed. Technol. 8(2), 102–114 (2021).
Systems VM. TrueBeam Technical Reference Guide—Volume 2: Imaging. 2013.
Ma, Y. et al. An electronic portal image device (EPID)-based multiplatform rapid daily LINAC QA tool. J. Appl. Clin. Med. Phys. 22(1), 45–58 (2021).
Ritter, T. et al. Automated EPID-based measurement of MLC leaf offset as a quality control tool. Biomed. Phys. Eng. Exp. 4(2), 027008 (2018).
Masi, L., Doro, R., Favuzza, V., Cipressi, S. & Livi, L. Impact of plan parameters on the dosimetric accuracy of volumetric modulated arc therapy. Med. Phys. 40(7), 071718 (2013).
Divyalakshmi, J. et al. A strategy to determine off-axis dosimetric leaf gap using OSLD and EPID. Rep Pract Oncol Radiother. 26(6), 1019–1028 (2021).
Greer, P. B., Vial, P., Oliver, L. & Baldock, C. Experimental investigation of the response of an amorphous silicon EPID to intensity modulated radiotherapy beams. Med. Phys. 34(11), 4389–4398 (2007).
De Freitas, N. L. & Gasparini, A. Review of real time 2D dosimetry in external radiotherapy: Advancements and techniques. Radiat. Measure. 180, 107344 (2024).
Delfs, B. et al. The role of the construction and sensitive volume of compact ionization chambers on the magnetic field-dependent dose response. Med. Phys. 48(8), 4572–4585 (2021).
Sait AA, Yoganathan S, Jones GW, Patel T, Rastogi N, Pandey S, et al. Small field measurements using electronic portal imaging device. Biomed. Phys. Eng. Exp. 2024.
Parent, L., Seco, J., Evans, P. M., Fielding, A. & Dance, D. R. Monte Carlo modelling of a-Si EPID response: the effect of spectral variations with field size and position. Med. Phys. 33(12), 4527–4540 (2006).
Yousif, A. E., Abdelgawad, M. H., Eldib, A. A., El-Sayed, S. M. & Talaat, M. Investigating a correlation between MLC positional errors and IMRT QA passing rate. Radiat. Phys. Chem. 209, 111001 (2023).
Jubbier ON, Abdullah SS, Alabedi HH, Alazawy NM, Al-Musawi MJ, editors. The effect of modulation complexity score (MCS) on the IMRT treatment planning delivery accuracy. Journal of physics: conference series; 2021: IOP Publishing.
Kumaraswamy, L. K., Xu, Z., Bailey, D. W., Schmitt, J. D. & Podgorsak, M. B. Evaluation of fluence-based dose delivery incorporating the spatial variation of dosimetric leaf gap (DLG). J. Appl. Clin. Med. Phys. 17(1), 12–21 (2016).
McNiven, A. L., Sharpe, M. B. & Purdie, T. G. A new metric for assessing IMRT modulation complexity and plan deliverability. Med. Phys. 37(2), 505–515 (2010).
Acknowledgements
Great thanks to Dr. Ke Li for his efforts on manuscript writing. We also like to thank Dr. Jie Hu for his professional assistance.
Funding
This project is supported by Shaanxi Provincial Cancer Hospital National Science Foundation Incubation Project (SC23A01).
Author information
Authors and Affiliations
Contributions
X. Wang conceived the project and wrote the manuscript. C. Ma and X. Wang coded the software. T. Zhang and X. Chang collected data. J. Liang and L. Lin analyzed the data. The manuscript was reviewed by all the authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and informed consent
The study was approved by the Medical Ethics Committee of the Shaanxi Provincial Cancer Hospital. All relative guidelines and regulations were followed in the methods. Due to the retrospective nature of the study, the Medical Ethics Committee of the Shaanxi Provincial Cancer Hospital waived the need for obtaining informed consent.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, X., Ma, C., Zhang, T. et al. Impact of two-dimensional dosimetric leaf gap on SRS-VMAT for single-isocenter multi-target brain metastases. Sci Rep 15, 29627 (2025). https://doi.org/10.1038/s41598-025-14300-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-14300-9
