
Abstract
The purpose of this pilot study was to test an adapted childhood obesity prevention intervention called Preventing Obesity Using Digital-Assisted Movement and Eating (ProudMe) in under-resourced schools. Six schools were cluster-randomized to ProudMe (n = 33; at three schools) or waitlist control (n = 46; at three schools) conditions. ProudMe aimed to improve participants’ health behaviors and weight status through interventions in the school cafeteria (i.e., ProudMe Cafeteria), physical education (PE) (i.e., ProudMe PE), and through artificial-intelligence- (AI-) assisted behavioral counseling (i.e., ProudMe Tech), and staff professional development (i.e., ProudMe PD). Two implementation outcomes including penetration and fidelity were captured through mixed methods. We drew upon the Consolidated Framework for Implementation Research (CFIR) to identify facilitators and barriers underlying implementation. The intervention only resulted in highly positive implementation outcomes in the cafeterias, which subsequently resulted in improved cafeteria scores. Implementation outcomes were less desirable in ProudMe PE with moderate penetration and fidelity. ProudMe PD was well attended but ProudMe Tech was under-utilized. The pilot intervention as a whole did not show significant effects on student-level outcomes (p > 0.05). Multiple facilitators and barriers across CFIR domains emerged as influential factors for the pilot intervention’s implementation and preliminary effectiveness. This study generated mixed evidence concerning the ProudMe intervention. The lessons learned inform future intervention refinement.
Similar content being viewed by others
Introduction
Tailored childhood obesity prevention interventions are needed to address health disparities in under-resourced communities. Like other Southern states in the United States, Louisiana faces significant public and community health challenges due to factors such as high poverty, inadequate healthcare, high crime rates, and energy-dense, high-sodium diet4. A recent report from the State of Childhood Obesity indicated that 22.2% of children aged 10–17 years in Louisiana have obesity, notably higher than the national average (%)4. The greater Baton Rouge metropolitan area of Louisiana has one of the highest obesity prevalence estimates in the United States5 and is racially diverse with over two-thirds of the population identifying as African American and Hispanic minorities6. Many Louisianans reside in communities and households with limited resources and poor accessibility to healthcare, therefore putting them at elevated risks for chronic diseases and health conditions (e.g., obesity, diabetes, metabolic syndromes)7,8. Children living in these areas are especially vulnerable to obesity and other health problems, warranting preventive interventions9,10,11.
Prior research has shown that theory-driven, multi-setting, and multi-component obesity prevention interventions can be effective in reducing children’s risk for obesity and chronic diseases1,9,12. Successful interventions have usually targeted modifiable factors that can affect children’s health behaviors such as physical activity, screen time, and diet, to influence energy balance13 and achieve a healthy body weight status14. Meeting the recommended levels of moderate-to-vigorous physical activity (MVPA; ≥ 60 min per day), screen time (≤ 2 h per day), and dietary intake (≥ 5 servings of fruits/vegetables and having balanced meals) contributes to a child’s overall health and significantly lowers their obesity risk15,16,17. However, at the population level, especially for children attending under-resourced schools, meeting the recommended levels of these health behaviors is difficult, which demands tailored and cost-effective interventions18,19,20,21.
Researchers have frequently used schools as a primary setting for obesity prevention and health interventions22as more than 90% of school-aged children attend schools most of the year23. If planned well, schools can simultaneously achieve educational and health promotion goals24. Several opportunities are presented within the school setting, including the cafeteria, physical education (PE), recess, and classrooms, for children to consume healthy meals, engage in physical activity, and acquire knowledge and skills to foster a more active lifestyle25. For children with lower socioeconomic status (SES), in particular, school cafeterias are a critical source of nutritious meals (breakfast and lunch) that help them avoid hunger during school days26,27. Most school-based child nutrition programs in the United States aim to offer nutritious meals by following relevant governmental guidelines (e.g., USDA guidelines), and cafeteria managers and staff may benefit from receiving intentional training and support to exercise best practices in the cafeteria28. Similarly, PE is a major contributor to students’ daily MVPA participation29 and development of physical fitness, skills (motor, sport, and behavioral management skills), and physical literacy29,30,31. However, most PE programs across the United States, particularly in secondary schools, over-emphasize participation and recreation, without clear goals or efforts to teach students to attain the national PE standards32. Offering students with purposeful learning experiences in PE and providing teachers with relevant professional development (PD) are important to avoid missed opportunities for the students and equip themselves with the competence and confidence for healthy and active living33,34.
Furthermore, continual exposure to interventions beyond the school settings may be necessary to render a sustained impact on health behaviors and weight status. Recent research, our pilot work included, has employed artificial intelligence (AI) as a low-cost, tailored strategy to deliver personalized health behavior counseling and support to prevent and control child and adolescent obesity35,36. Across the United States, more than 90% of teens regularly use or own a smartphone, and minority youths from lower-income households often rely solely on mobile devices for communication and Internet access37. The prevalent use of electronic devices has generated significant research interest in using modern technology38 for obesity prevention and health promotion39,40 for this population. The AI technology (e.g., ChatGPT) has been revolutionizing modern societies. AI offers great opportunities for adolescents to receive cost-effective, tailored behavioral counseling, which is crucial for them to live healthfully and lower the risk of obesity41. Integrating AI-based technologies into a multi-component, multi-setting intervention to prevent adolescent obesity is innovative and warrants empirical testing.
Preventing Obesity using Digital-assisted Movement and Eating (ProudMe) is a theory-driven, multi-setting, multi-component obesity prevention intervention for middle school students attending under-resourced schools. It was adapted from the evidence-based intervention School Wellness Integration toward Child Health ─ Middle School (SWITCH─MS). SWITCH─MS encompassed (a) a 12-lesson PE unit focused on energy balance, (b) a static website that enabled students to track their health behaviors, and (c) a set of strategies to make environmental and policy changes in the cafeteria following the Smarter Lunchrooms Movement guidelines42. SWITCH─MS was originally field-tested in Iowa schools, and demonstrated moderate effects on improving students’ physical activity and reducing screen time43,44,45,46,47. Given the sociocultural differences between Iowa and Louisiana, SWITCH─MS was adapted for dissemination to under-resourced schools in Louisiana, re-branded as ProudMe. ProudMe has implemented notable modifications including: (a) Refined PE lessons; (b) Integrated artificial intelligence (AI) for behavioral counseling; and (c) Simplified Smarter Lunchrooms Movement guidelines for easier implementation. ProudMe has not been field-tested; therefore, pilot testing its implementation and effectiveness at a small scale is necessary to determine long-term suitability for dissemination to broader settings.
This study aimed to assess the feasibility of the pilot ProudMe intervention (i.e., registered trial: NCT06335056, 28/03/2024) resolving uncertainties regarding its implementation and potential impact in Louisiana. Our study was guided by three relevant theoretical underpinnings in implementation science. First, we followed Curran et al.’s type II hybrid effectiveness-implementation design, to simultaneously evaluate the implementation and preliminary effectiveness of the ProudMe intervention48. The dual focus on implementation and preliminary effectiveness in this pilot clinical trial can generate useful evidence informing the impact of the ProudMe intervention. The type II hybrid design is a pragmatic design that can effectively and efficiently generate evidence for health interventions and shorten the time span needed for translating science to practice, making a timely impact on public health. Secondly, we followed Proctor and Brownson’s taxonomy to examine two implementation outcomes of the intervention: penetration (i.e., integration of a practice within a setting) and fidelity (i.e., the degree to which an intervention was implemented as prescribed)49. Thirdly, we drew upon the Consolidated Framework for Implementation Research (CFIR) as the theoretical framework1,2 to engage in a reflective process to identify influential facilitators and barriers underlying implementation. CFIR allows researchers to systematically study five major domains of an intervention: intervention characteristics, outer setting, inner setting, characteristics of the individuals involved, and the process of implementation. A recent systematic review found that most of prior studies used complex (vs. simple) interventions and the aspects of inner setting were most frequently examined (outer setting least examined50. Categorizing factors by the five CFIR domains allows researchers to systematically understand facilitators and barriers that would lead to the success or failure of an intervention. The lessons learned from this pilot study will inform future intervention refinement and full-scale effectiveness evaluation.
Materials and methods
Setting and participants
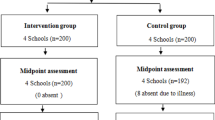
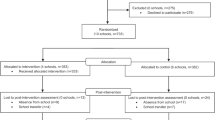
This pilot study was conducted at six schools with middle school grades (6th, 7th, and/or 8th grades) recruited from one Louisiana school district near the metropolitan area of Baton Rouge, Louisiana. Upon the school district’s approval and the permission of the participating schools, we divided the six schools into three sampling brackets by pairing two most similar schools in each bracket. Four factors were considered: enrollment size (small, medium, large), racial diversity (diverse vs. very diverse based on % of racial minorities vs. non-Hispanic White), student to teacher ratio (high vs. low), and free and reduced-price meal (FARM) eligibility percentage (FARM%; medium vs. high percentages). We subsequently randomized the two similar schools within each sampling bracket into the ProudMe or waitlist control conditions. Table 1 shows the characteristics of the schools in the two groups. Although across the six schools, there were 631 students enrolled in 6th, 7th, and 8th grades, only 79 students participated and completed both pre- and post-test assessments (ProudMe: n = 33; control: n = 46). The sample size ranged from five (school 5) to 22 (school 3) students per school. Despite the incentives, a large number of students (mostly their parents) declined participation or did not complete both pre- and post-test assessments due to reasons unwilling to report. Furthermore, two PE teachers at the experimental stage withdrew from the study; therefore, students in those two classes also withdrew as they were no longer receiving the intervention. The Louisiana State University Institutional Review Board approved the study protocol (IRBAM-21-0702). Parental informed consent and child assent were obtained in writing for study participation.
The ProudMe intervention
The ProudMe intervention consisted of four components: ProudMe Cafeteria, ProudMe PE, ProudMe Tech (implemented within PE), and ProudMe Professional Development (PD). ProudMe Cafeteria, ProudMe PE, and ProudMe Tech were implemented in late February through early May 2024, immediately after the ProudMe PD which occurred in early February of 2024. We describe each of these components below.
ProudMe Cafeteria was designed to improve the school food environment and promote healthy eating behaviors among students. This component involved empowering leaders and staff in the district’s child nutrition program and cafeterias to implement simplified Smarter Lunchrooms Movement strategies42 over eight weeks. A total of 60 strategies across eight focus areas were observed, addressed, promoted, and then re-observed (e.g. Focus on Fruits, Vary the Vegetables, Move More White Milk, Boost Reimbursable Meals, Lunchroom Atmosphere, Student Involvement, and School Community Involvement). For example, an item within the Focus on Fruits area is phrased as “At least two kinds of fruit were offered”. These strategies and focus areas are described in detail in the ProudMe Cafeteria booklet, which was shared and discussed with each cafeteria in the beginning of the project and then explained and reiterated in subsequent check-in sessions. Specifically, the cafeteria intervention began with a discussion of the Smarter Lunchrooms Scorecard baseline results. The purpose of this discussion was to identify strengths and weaknesses within each cafeteria, increase staff awareness, elicit desire for change, set goals and make action plans for the upcoming implementation. The head researcher empowered the cafeteria managers to lead their team to set up objectives and select changes based upon the strengths, weaknesses, and available resources at each school. Regular check-in and continual support were provided throughout the implementation period. After each meeting, each cafeteria manager returned to their school, shared the training to their cafeteria staff team, and worked with their team to implement the ProudMe Cafeteria. We provided constructive feedback and encouragement to each cafeteria manager, to (1) sustain staff motivation and (2) help each cafeteria make progressive changes.
The ProudMe PE component included 12 PE lessons that taught students about healthy living related to physical activity (four lessons), screen time (four lessons), and fruit and vegetable consumption (four lessons). These lessons were developed by master PE teachers, teacher educators, and researchers; and were field-tested and adapted for the Louisiana context. These lessons were designed to be physically engaging, and to help middle school students to meet the recommended levels of the three health behaviors related to obesity prevention. All 12 lessons included scripted lesson plans within the ProudMe PE teacher’s manual. The lessons required minimal equipment and space to accommodate under-resourced schools. For implementation, PE teachers were told to preview the lesson plans, set up the instructional space following the illustrated diagram, and teach the lessons following the lesson plans (1–2 lessons per week). They were allowed to make planned or improvised changes to the lessons. If modifications were made, they were instructed to document them in writing and share with the researchers.
ProudMe Tech is a separate intervention component but was implemented within PE lessons as an in-class activity. ProudMe Tech successfully embedded a set of tailored prompt algorithms (upon over a year of development and iterative testing) into our project’s website, which enabled the student users to set individualized daily goals and record their behaviors onto the ProudMe Tech journal. Data input into the journal were transmitted to ChatGPT, which provides instant feedback as behavioral counseling to each user. The chatbots provided users with counseling, which helps them (1) set specific, measurable, attainable, realistic, and timely (SMART) goals51 for physical activity52sedentary time, fruit and vegetable intake and sleep; (2) track and monitor these behaviors; (3) record self-reflective thoughts about their goal attainments; and (4) receive and process AI-assisted feedback. To use ProudMe Tech, each user had to register an account with a username and password, and then regularly interact with the technology on their school-assigned laptops during PE classes and on their private computers at home to receive behavioral counseling at least three days per week.
ProudMe PD provided implementation staff, including cafeteria managers, PE teachers, administrators, and support staff with the necessary training before launching the ProudMe intervention. ProudMe PD included a half-day wellness conference (i.e., four hours) followed by regular check-ins and continual support by the research team. The wellness conference began with welcome remarks from a district administrator, followed by introductions and greetings, and then proceeded to four short presentations that provided overviews of the ProudMe project, the relationship between food environment and healthy eating, the importance of quality PE, and pre- and post-test assessments for all attendees. Upon a short break, the attendees split into two breakout rooms to receive different trainings. The teachers and staff at the ProudMe schools received training related to ProudMe Cafeteria, ProudMe PE (including a PPT presentation and a demo lesson in the gymnasium), and ProudMe Tech. The teachers and staff at the control schools learned several instructional drills to teach ultimate frisbee in an open space outside of the gymnasium. The conference concluded with teachers and staff from each school gathering to summarize, reflect, and make action plans for implementation in the next few weeks.
Implementation evaluation
The evaluation of the pilot ProudMe intervention simultaneously examined its implementation and preliminary effectiveness. For implementation evaluation, we gathered mixed methods data by using field observations, teacher log, teacher interviews, and written records to inform two implementation outcomes selected from Proctor and Brownson’s taxonomy: penetration and fidelity49.
Penetration (i.e., integration of a practice within a setting) was measured using our written data records that recorded the names of the individuals who implemented the ProudMe intervention and those who did not. The penetration index was calculated as the number of implementers who delivered an intervention divided by the total number of persons eligible for the delivery53. Fidelity (i.e., the degree to which an intervention was implemented as prescribed) in the PE setting was measured using three methods: field observations, teacher logs, and teacher interviews. First, trained observers visited each experimental school every two weeks (monthly to control schools) to observe implementation of the ProudMe PE lessons. Observers completed a standardized checklist with 10 questions that recorded the extent to which a PE teacher made modifications to the lessons. If a modification was made, the trained observer described them in detail. Observation-based fidelity index was calculated by dividing the sum scores of 1s (i.e., no modification) by eight (i.e., eight scorable checklist items). Descriptive notes recorded by the trained observers were analyzed to describe the timing, location, nature, extent, rationale, and perimeters of the modifications made. Second, the PE teachers were asked to complete a log sheet immediately after teaching each lesson. The log had six questions regarding which lesson was taught (open-ended), lesson length (0–15 min; 16–30 min; 31–45 min; 46–60 min; 61–75 min; >75 min), modifications made (yes, describe; or no), level of student focus (1 = far below average; 5 = far above average), perception of the level of student enjoyment (1 = not at all; 3 = very), and changes and thoughts (open-ended). Third, PE teachers were invited to attend semi-structured interviews twice: early and late stages of intervention, respectively. These interviews were conducted following an interview guide. Each interview asked teachers about their implementation of ProudMe PE, progress made, positive experiences, difficulties or barriers, modifications made, student response to the instruction, and support needed. Fidelity level in the cafeteria setting was measured using conversational interviews that occurred during regular training sessions. Fidelity of the ProudMe Cafeteria implementation was captured through conversational interviews between the head researcher and cafeteria managers. Objectives and changes at each cafeteria were discussed and recorded as notes. These were also recorded in the ProudMe Cafeteria booklet, which was subsequently used as artifact data for the implementation evaluation. Fidelity of the ProudMe Tech implementation was captured by human/computer interaction records, which were automatically saved on the server and the data base and monitored by our website developer daily.
Preliminary effectiveness evaluation
Trained observers conducted objective observations of all six cafeterias, using the Smarter Lunchrooms Scorecard, to assess the environmental and policy changes in the cafeterias54. The Smarter Lunchrooms Scorecard22 contains 60 questions measuring eight focused areas. The sum scores from these questions determined a cafeteria’s medal status: gold (46–60), silver (26–45), or bronze (15–25).
Participant’s weight, height, and waist circumference were pre- and post-assessed by trained data collectors. Weight and height were measured using the Seca 777 Digital Physician Scale (Seca GmbH & Co. KG, Hamburg, Germany). Body mass index (BMI) was calculated based on weight and height and converted to BMI z-scores (BMIz) and BMI percentile scores taking into account the age- and sex-specific CDC growth charts and standards55. Waist circumference was measured using the Seca 201 Ergonomic Circumference Measuring Tape (Seca GmbH & Co. KG, Hamburg, Germany). We asked each participant to stand up tall and placed the constant-tension Seca tape measure horizontally around the waist through the anterior superior iliac spine and then recorded the measurement.
Participants’ health behaviors including physical activity, screen time, and diet were measured using a Qualtrics survey56. We adopted both self-report and accelerometer-based measurements of physical activity. First, participants were asked to report the number of days they were active for at least 60 min in the past week, with choices ranging from 0 to 7 days. This question was adopted from the National Health and Nutritional Examination Survey (NHANES), which has been used in similar research. Secondly, Screen time questions asked about their time spent playing video games, using social media, watching shows or movies, and other screen activities, with answers categorized from 1 (0–30 min) to 5 (more than 3.5 h)57. The survey also asked about servings of fruit and vegetables consumed with answers ranging from 0 (0 serving) to 5 (5 or more servings). Additionally, a subsample from each school was asked to wear the ActiGraph GT3X+ (ActiGraph, LLC., Pensacola, Florida, USA) accelerometers on their waist for seven days to provide objective measurement of physical activity and sedentary behavior58. The accelerometer data (15-s epoch) were processed using the critical cut-point standard by Freedson59to estimate metabolic equivalent (MET). The MET rate was calculated using the following formula: MET = 2.757 + (0.0015 * CPM) - (0.08957 * age) - (0.000038 * CPM * age), where CPM refers to count per minute. We categorized activity data into MVPA (≥ 3 METs), light PA (LPA; 1.5–2.99 METs), and sedentary behavior (SB; <1.5 METs) and calculated the time (in minutes) and time percentage for subsequent data analysis.
Data collection
We gathered mixed methods data throughout the implementation process using observations (every two weeks in ProudMe schools; monthly in control schools), teachers’ logs (immediately after teaching each lesson), teacher interviews (early and late phases of implementation), and written record (throughout the study). All data collectors received two hours of ethics online training and two hours of specific research training. They were required to pass the competency test prior to data collection. Upon training, data collectors were sent to ProudMe schools in every two weeks to observe the implementation of ProudMe PE lessons following a pre-established observation protocol. They completed the observation checklist and recorded any deviations from the ProudMe lesson plans along with reflective thoughts. Data collectors also observed the control schools monthly, to capture teaching and learning activities that took place in those PE classes. For teachers’ logs, we delivered the hard-copy log sheets to each school and instructed the teachers to report their implementation as soon as they finish teaching each lesson. Completed logs were picked up at end of the project and progresses were also discussed during the teacher interviews. The head researcher conducted teacher interviews on Microsoft Teams, following the interview guide. Interview conversations were recorded upon participants’ permission and transcribed to verbatim for subsequent data analysis. Each interview lasted for 17–25 min. Written records including school schedules, attendance records, data collection journals, and data records were kept and organized daily in the lab.
To determine preliminary effectiveness, participants were pre- and post-assessed in February and May, respectively, for anthropometric outcomes and health behavior. Following the data collection protocol, each round of assessment took two days with day one gathering consent and measuring weight, height, and waist circumference (in private), and day two involved distributing the accelerometers (individually configured for participants) and administering the survey. To measure environmental and policy changes in the cafeteria, two trained observers conducted cafeteria observations in November–December 2023 and again in April–May 2024. The training consisted of reviewing the Smarter Lunchrooms Scorecard and familiarizing with the measure (background, rationale, content, and scoring) in the lab, followed by conducting a real-time observation at a convenience school’s cafeteria (not a participating school in the study). The student observers’ observation scores were compared with the head researcher’s scores, which reached > 90% agreement. Disagreements were discussed and reconciled with agreements.
Data analysis
Mixed-method data from teacher logs, teacher interviews, observation notes, and written records were analyzed using thematic coding to identify common categories and patterns to describe the implementation process and outcomes. Quantitative data from surveys, checklists, and objective measurements (accelerometer data and anthropometric measures) were analyzed using descriptive and inferential statistical analyses. Repeated-measures analyses of variance (RM-ANOVA) were employed to compare baseline and post-test scores for anthropometric outcomes, health behaviors, and physical activity self-efficacy within and between groups. For accelerometer data analysis, we compared MVPA, LPA, and SB in terms of time and time percentage by time (baseline vs. post) and group (treatment vs. control). To identify influential facilitators and barriers underlying the pilot ProudMe intervention, we drew upon CFIR as our theoretical framework and categorized these factors by five domains: intervention characteristics, outer setting, inner setting, characteristics of individuals, and implementation process.
Results
Implementation outcomes
The results below are related to two implementation outcomes including penetration and fidelity of the pilot ProudMe intervention. The intervention showed a moderate penetration index (50–67%) in PE classes and a perfect penetration index (100%) in the cafeterias. At least half of the eligible PE teachers and all cafeteria managers delivered the intervention. Table 2 below presents the detailed penetration index scores by school (#4, #5, and #6) and implementation setting (PE and cafeteria).
Implementation fidelity in PE was measured using field observations, teacher logs, and teacher interviews. Table 3 reports the fidelity index values by class, teacher, and school, based upon the field observations. The number of lessons observed ranged from two to five (Median = 3); and fidelity index ranged from 50 to 68.8% (Median = 62.5%). Table 4 reports the results based on teachers’ log data. Of the five classes across three schools, only two classes at school 5 and school 6 (joint-taught by two teachers), respectively, completed the teacher logs. The teachers reported that they made some modifications to 80–91% of the lessons within the curriculum unit. The median duration of the ProudMe PE lessons taught was 16–30 min (67%) at school 5 and 31–45 min (91%) at school 6, respectively. Teacher logs from school 4 were reported missing by both teachers. The teachers reported that their students’ level of focus was relatively low to moderate (5-point scale), and the students’ level of enjoyment was moderate to high (3-point scale). Based on open-ended responses from the teachers’ logs and interviews, the most common modifications made were related to equipment substitution and time allocation. For example, one teacher at school 3 stated: “Sometimes equipment is a challenge. We kind of have to work around that, so I just use simple stuff.” Similarly, another teacher at school 6 explained her rationale for making modifications related to time and equipment saying: “the biggest one is just time constraints cutting everything down……Kicking soccer balls is not the safest option, so we have substituted soccer balls with those alligator dodge balls.” The implementation of ProudMe Tech within the PE classes largely failed due to unsolved technical problems that resulted in unsuccessful user account registrations. Less than a quarter of the students were able to register an account, and they only engaged in AI-assisted behavioral counseling for 0–3 times. The teachers and students discontinued use, after several failed registration attempts.
Implementation fidelity at the three school cafeterias was outstanding. Based on conversational interviews with the cafeteria managers and the Supervisor of Child Nutrition in the district, the cafeterias fully endorsed ProudMe Cafeteria, set goals, put forth actions, and even implemented innovative strategies beyond the lesson plan to make changes. For example, the cafeteria manager at school 4 shared in a regular team meeting with the head researcher and other cafeteria managers the changes made in her school: “We removed the cleaning supplies and moved the trashcans. We rearranged the salad and fruit stations and came up with creative names for the foods. We also offered mixed fruits in two different locations to give students more choices.” Similarly, at school 5, the cafeteria manager said: “We started offering fresh fruits and introduced salad. We put up food signs to guide the kids. We also got students involved in making paper Mache and artwork for the cafeteria.” Lastly, the cafeteria manager at school 6 shared the changes her team made in the lunchroom: “We made sure to post the featured food items on our board. I convinced the principal to display pictures of fruits and vegetables. We also organized a food-tasting event to get the students excited.” Supported by their supervisor and the head researcher, cafeteria managers and their lunchroom staff demonstrated strong motivation to make positive changes to improve their scores. They followed the ProudMe Cafeteria booklet, applied the recommended strategies as well as creative strategies through their own grassroots effort, and regularly reflected upon their actions. Meetings with the head researcher were full of positive energy and social support.
Preliminary effectiveness
To evaluate the preliminary effectiveness of the pilot ProudMe intervention, we examined the setting- and student-level outcomes by time (pre vs. post) and condition (ProudMe vs. control). These outcomes included the Smarter Lunchrooms Scorecard scores (i.e., overall and by scoring categories), anthropometric outcomes (i.e., BMI, BMIz, BMI percentile, and waist circumference), and health behaviors (i.e., physical activity, screen time, and fruits and vegetable intake). These results are reported below.

Cafeterias’ mean scores by time and condition. Solid line: ProudMe; broken line = control.
The successful implementation of ProudMe Cafeteria led to positive policy and environmental changes in the three cafeterias. Figures 1 and 2 illustrate the improved scorecard scores. Without intervention, the overall scorecard score at the three control schools decreased by 9.8% (ΔM = − 3.0). Two of the three schools maintained the silver medal status (24–45 points out of 60), while the third school dropped to bronze medal status (15–25 points) at post-test. In comparison, ProudMe cafeterias (over 10–12 weeks) increased by 13.4% (ΔM = 4.7). All three ProudMe schools improved their scorecard scores (by 4–7 points), maintaining the silver medal status. Of these three ProudMe schools, school 5 was only three points away from gold medal status (46–60 points). The scoring categories with most notable improvement in the ProudMe cafeterias were “Focus on fruit”, “Vary the Vegetables”, “Boost Reimbursable Meals”, “Lunchroom Atmosphere”, “Student Involvement”, and “School Community Involvement”. “Highlight the Salad” and “Move More White Milk” were the only two areas that declined. No inferential statistical analyses were performed due to the small number of cafeterias involved.
We also examined intervention effects of ProudMe on student-level outcomes including anthropometric outcomes and health behaviors. For anthropometric outcomes, RM-ANOVAs did not find statistically significant time-by-condition interaction effects for BMI, BMIz, BMI percentile, and waist circumference (ps > 0.05). Figure 3 illustrates the gain scores (posttest – pretests scores) in these outcomes by condition. Compared to the control group, the ProudMe group experienced minimal to no changes in BMI and BMIz, a small increase in BMI percentile (small decrease in control), and a small decrease in waist circumference (less decrease in control). Further moderation analyses did not detect clear, significant change patterns in these anthropometric outcomes by grade, gender, or teacher (ps > 0.05).

Cafeterias scores in the eight scoring categories by time and condition. Solid line: ProudMe; broken line = control.

Changes for ProudMe (n = 33) and Control (n = 46) in anthropometric outcomes (BMI, BMIz, BMI percentile = BMIp, WC) by condition. BMI = body mass index; WC = waist circumference; dif = posttest – pretest difference.
RM-ANOVAs did not find significant condition-by-time interaction effects for the health behaviors including physical activity, fruit and vegetable intake, and screen time, regardless of their measurement methods (self-report or accelerometer-measured) (ps > 0.05). Tables 5 and 6 below report the estimated marginal means and standard errors of these health behaviors by condition and time. For activity, we separately report duration (minute) and percentage of sedentary behavior (SB), light physical activity (LPA), and moderate-to-vigorous physical activity (MVPA).
Facilitators and barriers
Our mixed methods data analysis identified 31 factors, including 15 facilitators and 16 barriers, which have influenced the implementation and preliminary effectiveness of the ProudMe pilot intervention. These factors are organized by the five CFIR domains in Table 7. For the Intervention Characteristics domain, facilitators such as the use of theory-driven and field-tested intervention, simplified cafeteria strategies, and supportive training sessions contributed to the intervention processes and outcomes. However, barriers such as perceived misalignment between ProudMe PE and the district’s existing PE curriculum, equipment shortages, and technical issues with ProudMe Tech limited implementation limited success. For the Outer Setting, district-level leadership and alignment with USDA guidelines supported the project implementation; whereas limited resources, restricted access to technology, and low parental consent posed significant challenges. Furthermore, for Inner Setting, the schools offered supportive leadership from principals and autonomy for cafeteria operations, but barriers such as scheduling disruptions, spatial constraints, and weak communication with PE teachers hindered progress. As for the Individuals Characteristics, notable facilitators included having licensed physical educators and engaging cafeteria staff, which were in contrast with issues such as over-burdened teachers who demonstrated undesirable class management and reluctance to use technology in instruction. Finally, for the Implementation Process, we found that cafeteria teams actively implemented the ProudMe Cafeteria intervention and both teachers and cafeteria managers showed increased engagement due to our financial incentives as facilitators. We also observed significant teacher-initiated" modifications to the intervention throughout the process (for various reasons) and participant attrition (e.g., reduced participation in post-test), which hampered the reach and fidelity of the intervention implementation.
Discussion
Our primary goal of this pilot study was to test the intervention components, implementation strategies, instrumentation, and project operation to assess the likelihood of success in a future full-scale effectiveness trial. The pilot ProudMe intervention demonstrated mixed results regarding implementation outcomes and preliminary effectiveness. These results as well as the attributable factors (facilitators and barriers) are discussed below.
Our pilot intervention demonstrated varying levels of implementation fidelity across settings and components. Implementation outcomes were particularly strong in the cafeteria setting, where we achieved full penetration and excellent fidelity. In contrast, PE classes showed only moderate levels of implementation. Although the ProudMe PD sessions were generally well attended, with only two PE teachers absent. AI-assisted behavioral counseling was under-utilized due to technical failures and logistical challenges. The two teachers who missed PD sessions were provided with the curriculum handbook and brief training prior to implementing the intervention.
Regarding preliminary effectiveness, the pilot ProudMe intervention, as a whole, showed a notable setting-level impact as evidenced by improved policy and environmental changes in the cafeterias although it did not yield significant effects on student-level outcomes including anthropometric outcomes and health behaviors. The improved cafeteria scores observed in this study are consistent with previous research that substantiated the impact of applying the Smarter Lunchrooms Movement strategies in school cafeterias3,60. Specifically, Drzal et al.’s study involved 67 Michigan schools in Smarter Lunchroom programming by applying strategies related to fruits and vegetables. That study showed improved scorecard scores (pre to post; no control group) but not statistically significant improvement in consumption of fruits or vegetables3. Furthermore, Mumby et al.’s systematic review concluded that Smarter Lunchrooms Strategies were associated with school children’s healthy food selection, and strategies that involved children in naming food products, in taste-testing, and/or in creating marketing materials were associated with consumption of healthier food items60.
In addition, our pilot ProudMe intervention did not result in a statistically significant effect on adolescents’ anthropometric outcomes and health behaviors (either self-reported or objectively measured). The lack of preliminary effectiveness is somewhat consistent with observations made in previous systematic reviews, including Jacob et al. (2021), which reported mixed and generally small effect sizes of school-based obesity prevention interventions on anthropometric and behavioral outcomes61.
The lack of significant individual-level changes in the current study may be attributable to several interrelated barriers, as supported by our mixed-methods evidence (as discussed later in detail). In addition, challenges such as a small sample size—partly due to low parental consent rates—and limited teacher buy-in, along with participant attrition, may have further constrained the pilot ProudMe intervention’s potential to drive measurable changes in BMI or waist circumference and health-related behaviors61,62,63. However, the predecessor version of the ProudMe, namely, the Iowa-based SWITCH MS intervention showed relative effectiveness on health behaviors (self-reported PA and screen time) and acceptable implementation outcomes in Iowan students43. These results suggest the need to further tailor the ProudMe intervention and implementation strategies (by considering and addressing influential factors including both facilitators and barriers) through a robust implementation science framework such as CFIR. Further adaptation of the ProudMe intervention as well as the implementation should address the unique sociocultural and demographic characteristics of adolescents, parents, schools, and communities in under-resourced Louisiana areas (e.g., high poverty, hot and humid climate, palatable but unhealthy food culture, large school district, limited PE space and resources).
To fully understand the reasons that have led to the mixed evidence of this pilot intervention, we have drawn upon the CFIR as the implementation science framework, to identify and discuss influential facilitators and barriers, which have affected the implementation outcomes and preliminary effectiveness.
Intervention characteristics
The ProudMe intervention was recently adapted from an evidence-based intervention called SWITCH─MS43,44,45,46,47. To fit the characteristics of the local schools in Louisiana, we made deliberate adaptations (in consultation with content experts) to all of the four components: Cafeteria, PE, technology, and professional development. We anticipated positive implementation outcomes and preliminary effectiveness. However, we observed mixed results in this pilot trial. We found positive outcomes for ProudMe Cafeteria including outstanding penetration and fidelity data thanks to the strong district leadership, a collegial work environment, and engaging cafeteria managers. In comparison, we observed less desirable implementation outcomes in the other three ProudMe components including moderate attendance to the PD, significant modifications in PE, low usage of the ProudMe Tech. Future efforts should further refine the ProudMe PE lesson plans to be more user-friendly (e.g., make equipment optional rather than required). Participants’ usage of the technology during the intervention was halted due to a lingering technical error that limited user registration. This failure largely constrained the impact of the entire ProudMe intervention on student-level outcomes. Prior research has shown that self-monitoring is an effective behavioral management skill for behavior change and health promotion41,64. ProudMe Tech was designed to continually engaged participants in behavioral counseling (e.g., SMART goal-setting). Without this feature, the intervention exposure was greatly reduced (e.g., 12 ProudMe PE lessons over 3–4 months, indirect intervention from gradual policy and environmental changes in cafeterias). Future emphasis should also be placed to ensure that all implementers receive ProudMe PD, receive continual support, and make concerted efforts to implement ProudMe in their respective settings.
Outer setting
The outer setting of ProudMe played a crucial role in the implementation of the pilot ProudMe intervention, although such factors had been less studied according to a recent systematic review study50. Prior research has shown that top-down political and administrative support (along with bottom-up intervention development) may offer immense influence on implementation outcomes of externally introduced health interventions in schools65. Having administrative approval and support from the school district and school principals throughout the project was the most prominent facilitator of powerful influence on the inner setting, individuals (e.g., teachers, cafeteria managers and staff), and the implementation process. Such support from both the district and school leaderships not only enabled logistical coordination and staff engagement, but also created a top-down climate that legitimized the intervention across settings. This aligns with existing literature suggesting that high-level administrative endorsement is a critical determinant of implementation success in school-based health interventions66. Without such supports, it would have been impossible to conduct the project; let al.one have positive outcomes. Another facilitator in the outer setting was related to the positive leadership and collegial social culture within the district’s Child Nutrition program. The supervisor and cafeteria managers were welcoming, kind, diligent, and receptive to new ideas and changes. These district-level leaders acquired knowledge and skills from our meetings, and then led their lunchroom staff to make specific changes. The meetings, held in every two to three weeks, were characterized as having positive energy and social support. On the contrary, limited resources in the school district and surrounding communities (and within families) constrained the implementation of the pilot ProudMe intervention at these schools. Due to the lower SES, many students within the district received minimal parental supervision at home67resulting in this study’s low participation rate. An additional barrier at the district that limited the intervention was the censorship of external websites. The ProudMe Tech and survey data collection both required students to access to external websites. Not knowing this policy at the district, we experienced project delay that eventually strained our implementation schedule and should be investigated thoroughly prior in future study.
Inner setting
Several factors within a school setting were identified and categorized as facilitators or barriers of the inner setting for ProudMe. Inner setting was previously found as the most frequently examined CFIR domain in school-based obesity prevention interventions50. Under the leadership of each cafeteria manager, the cafeteria staff were able to make changes to improve their scorecard scores. We found that all cafeterias in the district had control over meal preparation and offering (e.g., menu, food selection, vendor selection, food presentation, etc.), as long as these practices complied with the USDA guidelines and their district’s wellness policy. These inner setting characteristics afforded the cafeteria staff with autonomy to make short-term and medium-term changes within a few short weeks68. Further, changes within the cafeteria were easier with the support of the principal. All principals involved in the intervention showed positive support for the ProudMe project. One principal voluntarily assisted in implementing ProudMe Cafeteria. In contrast with the facilitators within the cafeterias, we observed barriers that hampered the implementation of ProudMe PE. Implementing 12 lessons during a hectic and sometimes unpredictable spring semester was a significant challenge. Our implementation schedule was frequently interrupted by inclement weather (storms) followed by power outage, and temporary events (e.g., field trips and standardized testing). Additionally, PE teachers had other curriculum competing priorities along with time needed to implement ProudMe PE, and limited space and resources. Sharing the same gymnasium with another class means a noisy and chaotic atmosphere. These above facilitators and barriers observed at the inner setting domain somewhat overlap with what are observed in the existing literature where the most frequently reported barriers including weather, characteristics of the school, lesson scheduling and program coordination69. These inner setting issues contributed to success as well as added challenges to our pilot ProudMe intervention.
Individual characteristics
The success of a school-based intervention is largely influenced by characteristics of the individuals who are involved in the implementation70. The cafeteria managers and the Supervisor of the Child Nutrition program from the school district exhibited positive intention, effort, and morale throughout the project, which facilitated the successful implementation outcomes in the cafeterias (i.e., outstanding penetration, fidelity, and sustainability). Another facilitator related to this domain was the presence of our trained researchers in training meetings with the cafeteria managers and in the gymnasia to provide support when needed. Despite the facilitators, the ProudMe PE implementation was stifled with moderate to low levels of outcomes. Prior research suggests that teachers’ delivery of an externally introduced curriculum was negatively affected by the limited school resource, time constraint, workload, and lack of motivation (sometimes burnout)69. In this study, only six of the nine PE teachers who were invited to implement ProudMe PE agreed to teach the curriculum, and two of the six implementers were not licensed or were novice teachers who were assigned by their principal to cover the instructional needs (limited by school budget). The teachers were reluctant to implement ProudMe PE and ProudMe Tech, which were regarded as additional tasks on top of their hectic work schedules. As a result, we observed low teacher motivation and effort as well as significant student misbehaviors during daily lessons. These individual characteristics posed immense challenges to the project, and schooling in general.
Implementation process
The implementation process of the pilot ProudMe intervention was marked by success in the cafeterias but challenges in the PE programs. Factors in the other four CFIR domains (intervention characteristics, outer setting, inner setting, and individual characteristics) collectively affected the process and outcomes of the implementation. Overall, our data indicate smooth and, in some cases, creative implementations of the ProudMe Cafeteria (e.g., involving students to make creative paper mache and artwork for the cafeteria). However, the implementation of ProudMe PE saw significant deviations (50–69% fidelity index) from the lesson plans and modifications (80–91% lessons modified) to the equipment and time. Throughout the curriculum unit, the teachers reported that the students maintained low to moderate levels of focus and moderate to high levels of enjoyment when participating in ProudMe PE lessons. Similar to our findings, previous studies have shown that in school-based interventions, teachers often adapt or modify lesson plans due to constraints such as limited time, competing demands, and low perceived relevance—factors that reduce fidelity and impact69. The quality of the implementation process ultimately determined the implementation outcomes and impacted students’ anthropometric outcomes and health behaviors. Continually engaging teachers and students in school-based interventions is proven challenging71. In fact, our study experienced significant participant attribution throughout the intervention period due to low parental consent, high student absence, and significant non-participation in the posttest.
Conclusions
The pilot ProudMe intervention led to mixed results for implementation outcomes and preliminary effectiveness. The positive implementation outcomes (and improved scorecard scores) in the cafeterias, less desirable implementation outcomes elsewhere, and non-significant effects on students’ anthropometric outcomes and health behaviors will inform our future intervention refinement and effectiveness evaluation. The facilitators and barriers across five CFIR domains identified in this pilot study have not only enabled us to fully understand the reasons for our limited success observed in this pilot trial, but also will guide future systematic revision efforts to improve the implementation and effectiveness outcomes of ProudMe or other school-based obesity prevention interventions.
Data availability
The datasets generated and analyzed during this study are not publicly available due to confidentiality concerns and ethical restrictions. However, data may be made available from the corresponding author on reasonable request and after approval by the Institutional Review Board.
References
Damschroder, L. J. et al. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement. Sci. 4, 1–15 (2009).
Damschroder, L. J., Reardon, C. M., Widerquist, M. A. O. & Lowery, J. The updated consolidated framework for implementation research based on user feedback. Implement. Sci. 17, 75 (2022).
Drzal, N. & Henne, R. The impact of A smarter lunchroom program on selection of fruits and vegetables by children in school cafeterias. J Child. Nutr. Manag 44 (2020).
State of Childhood Obesity. (Robert Wood Johnson Foudation, 2021).
Bernardo, R. Fattest Cities in America (2024). https://wallethub.com/edu/fattest-cities-in-america/10532.
Bureau, U. S. C. Hispanic or Latino, and Not Hispanic or Latino by Race – 2020: DEC Redistricting Data (PL 94-171) – Baton Rouge637 city, Arkansas. Report No. PL 94-171 (2021).
Vilar-Compte, M. et al. Urban poverty and nutrition challenges associated with accessibility to a healthy diet: A global systematic literature review. Int. J. Equity Health 20, 40. https://doi.org/10.1186/s12939-020-01330-0 (2021).
Schwarz, T., Schmidt, A. E., Bobek, J. & Ladurner, J. Barriers to accessing health care for people with chronic conditions: A qualitative interview study. BMC Health Serv. Res. 22, 1037 (2022).
Angawi, K. & Gaissi, A. Systematic review of Setting-Based interventions for preventing childhood obesity. Biomed. Res. Int. 2021, 4477534. https://doi.org/10.1155/2021/4477534 (2021).
Bahia, L. et al. Overview of meta-analysis on prevention and treatment of childhood obesity. J. Pediatr. (Rio J). 95, 385–400. https://doi.org/10.1016/j.jped.2018.07.009 (2019).
Dugravot, A. et al. Social inequalities in multimorbidity, frailty, disability, and transitions to mortality: A 24-year follow-up of the Whitehall II cohort study. Lancet Public. Health. 5, e42–e50. https://doi.org/10.1016/s2468-2667(19)30226-9 (2020).
Korn, A. R. et al. Engaging coalitions in community-based childhood obesity prevention interventions: A mixed methods assessment. Child. Obes. 14, 537–552. https://doi.org/10.1089/chi.2018.0032 (2018).
NHLBI. Balance Food and Activity (2013). https://www.nhlbi.nih.gov/health/educational/wecan/healthy-weight-basics/balance.htm.
Knell, G., Durand, C. P., Kohl, H. W., Wu, I. H. C., Pettee Gabriel, K. & rd, & Prevalence and likelihood of meeting sleep, physical activity, and screen-time guidelines among US youth. JAMA Pediatr. 173, 387–389. https://doi.org/10.1001/jamapediatrics.2018.4847 (2019).
USDH. Physical Activity Guidelines for Americans, 2nd Edn. (2018).
Haughton, C. F., Wang, M. L. & Lemon, S. C. Racial/ethnic disparities in meeting 5-2-1-0 recommendations among children and adolescents in the United States. J Pediatr 175, 188–194 e181. https://doi.org/10.1016/j.jpeds.2016.03.055 (2016).
Tremblay, M. S. et al. Canadian 24-hour movement guidelines for children and youth: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 41, 311–327. https://doi.org/10.1139/apnm-2016-0151 (2016).
Chaput, J. P. et al. Proportion of preschool-aged children meeting the Canadian 24-hour movement guidelines and associations with adiposity: results from the Canadian health measures survey. BMC Public. Health. 17, 147–154 (2017).
Eiraldi, R. et al. Implementation of targeted mental health interventions in urban schools: Preliminary findings on the impact of training strategy on program fidelity. Evid. Based Pract. Child. Adolesc. Ment. Health. 5, 437–451 (2020).
Prochnow, T., Delgado, H., Patterson, M. S. & Umstattd Meyer, M. R. Social network analysis in child and adolescent physical activity research: A systematic literature review. J. Phys. Act. Health. 17, 250–260. https://doi.org/10.1123/jpah.2019-0350 (2020).
Wang, Y. et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 16, 547–565. https://doi.org/10.1111/obr.12277 (2015).
Education, C. D. o. Smarter Lunchrooms Movement (2024). https://www.cde.ca.gov/ls/nu/he/smarterlunchrooms.asp.
van Sluijs, E. M. et al. Physical activity behaviours in adolescence: Current evidence and opportunities for intervention. Lancet 398, 429–442 (2021).
CDC. Whole School, Whole Community, Whole Child (WSCC) (2023). https://www.cdc.gov/healthyschools/wscc/index.htm.
Acciai, F., Yedidia, M. J., DeWeese, R. S., Martinelli, S. & Ohri-Vachaspati, P. School food and physical activity environment: a longitudinal analysis of four school districts in new Jersey. J. Adolesc. Health. 65, 216–223 (2019).
Krukowski, R. A. et al. Development and evaluation of the school cafeteria nutrition assessment measures. J. Sch. Health 81, 431–436. https://doi.org/10.1111/j.1746-1561.2011.00612.x (2011).
Poulsen, P. H., Biering, K., Winding, T. N., Nohr, E. A. & Andersen, J. H. How does childhood socioeconomic position affect overweight and obesity in adolescence and early adulthood: A longitudinal study. BMC Obes. 5, 1–14 (2018).
USDA. Dietary Guidelines for Americans, 2020–2025 (2020). https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf.
Chen, S., Kim, Y. & Gao, Z. The contributing role of physical education in youth’s daily physical activity and sedentary behavior. BMC Public. Health. 14, 110. https://doi.org/10.1186/1471-2458-14-110 (2014).
Bassett, D. R. et al. Estimated energy expenditures for school-based policies and active living. Am. J. Prev. Med. 44, 108–113. https://doi.org/10.1016/j.amepre.2012.10.017 (2013). https://doi.org:.
Liu, Y. & Chen, S. Physical literacy in children and adolescents: Definitions, assessments, and interventions. Eur. Phy Educ. Rev. 27, 96–112. https://doi.org/10.1177/1356336x20925502 (2020).
Hastie, P. A., Chen, S. & Guarino, A. J. Health-Related fitness knowledge development through project-based learning. J. Teach. Phys. Educ. 36, 119–125. https://doi.org/10.1123/jtpe.2016-0151 (2017).
Chen, S. & Garn, A. Student learning in physical education through the lens of a curriculum specialist. Kinesiol. Rev. 7, 226–232. https://doi.org/10.1123/kr.2018-0017 (2018).
Wang, B. & Chen, S. Physical education curriculum interventions: A review of research patterns and intervention efficacy. Quest 74, 205–220. https://doi.org/10.1080/00336297.2022.2032774 (2022).
Alghalyini, B. Applications of artificial intelligence in the management of childhood obesity. J. Family Med. Prim. Care. 12, 2558–2564. https://doi.org/10.4103/jfmpc.jfmpc_469_23 (2023).
Colmenarejo, G. Machine learning models to predict childhood and adolescent obesity: A review. Nutrients 12, 2466 (2020).
Schaeffer, K. Most U.S. teens who use cellphones do it to pass time, connect with others, learn new things (2019). https://www.pewresearch.org/fact-tank/2019/08/23/most-u-s-teens-who-use-cellphones-do-it-to-pass-time-connect-with-others-learn-new-things/.
Lyons, E. J. & Swartz, M. C. Motivational dynamics of wearable activity monitors. ACSMs Health Fit. J. 21, 21–26 (2017).
Gao, Z., Chen, S., Pasco, D. & Pope, Z. A meta-analysis of active video games on health outcomes among children and adolescents. Obes. Rev. 16, 783–794. https://doi.org/10.1111/obr.12287 (2015).
Gao, Z., Zeng, N., McDonough, D. J. & Su, X. A. Systematic review of active video games on youth’s body composition and physical activity. Int. J. Sports Med. 41, 561–573. https://doi.org/10.1055/a-1152-4959 (2020).
Chen, S. Empower your wellness: Setting SMART goals to live healthy in the digital age. J. Dis. Prev. Health Promot. 8, 5–8. https://doi.org/10.5283/jdphp.46 (2024).
Hanks, A. S., Just, D. R. & Wansink, B. Smarter lunchrooms can address new school lunchroom guidelines and childhood obesity. J. Pediatr. 162, 867–869. https://doi.org/10.1016/j.jpeds.2012.12.031 (2013).
Chen, S. et al. Feasibility study of the SWITCH implementation process for enhancing school wellness. BMC Public. Health. 18, 1119. https://doi.org/10.1186/s12889-018-6024-2 (2018).
Chen, S. et al. Evaluating the implementation and effectiveness of the SWITCH-MS: an ecological, Multi-Component adolescent obesity prevention intervention. Int. J. Environ. Res. Public. Health. 17 https://doi.org/10.3390/ijerph17155401 (2020).
Gentile, D. A. et al. Evaluation of a multiple ecological level child obesity prevention program: switch what you do, view, and chew. BMC Med. 7, 49. https://doi.org/10.1186/1741-7015-7-49 (2009).
Rosenkranz, R. R. et al. A cluster-randomized trial comparing two SWITCH implementation support strategies for school wellness intervention effectiveness. J. Sport Health Sci. 12, 87–96. https://doi.org/10.1016/j.jshs.2021.12.001 (2023).
Welk, G. J., Chen, S., Nam, Y. H. & Weber, T. E. A formative evaluation of the SWITCH(R) obesity prevention program: Print versus online programming. BMC Obes. 2, 20. https://doi.org/10.1186/s40608-015-0049-1 (2015).
Curran, G. M., Bauer, M., Mittman, B., Pyne, J. M. & Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care. 50, 217–226. https://doi.org/10.1097/MLR.0b013e3182408812 (2012).
Proctor, E. K. & Brownson, R. C. in Dissemination and Implementation Research in Health: Translating Science to Practice (eds Ross C. Brownson, Graham A. Colditz, & Enola K. Proctor)Oxford University Press, 2012).
Butscher, F., Ellinger, J., Singer, M. & Mall, C. Influencing factors for the implementation of school-based interventions promoting obesity prevention behaviors in children with low socioeconomic status: A systematic review. Implement. Sci. Commun. 5, 12. https://doi.org/10.1186/s43058-024-00548-1 (2024).
Corbin, C. B., McConnell, K., Le Masurier, G., Corbin, D. & Farrar, T. Health Opportunities Through Physical Education (Human Kinetics, 2014).
Swann, C. et al. The (over)use of SMART goals for physical activity promotion: A narrative review and critique. Health Psychol. Rev. 17, 211–226. https://doi.org/10.1080/17437199.2021.2023608 (2023).
Proctor, E. K. & Brownson, R. C. Measurement issues in dissemination and implementation research. Vol. 261 (2012).
USDA. Smarter Lunchrooms Movement (2017). https://snaped.fns.usda.gov/library/success-stories/smarter-lunchrooms-movement.
CDC. Extended BMI-for-age growth charts. (2024).
Miller, C. A., Guidry, J. P. D., Dahman, B. & Thomson, M. D. A tale of two diverse qualtrics samples: Information for online survey researchers. Cancer Epidemiol. Biomarkers Prev. 29, 731–735. https://doi.org/10.1158/1055-9965.Epi-19-0846 (2020).
Motl, R. W. et al. Factorial validity and invariance of questionnaires measuring social-cognitive determinants of physical activity among adolescent girls. Prev. Med. 31, 584–594. https://doi.org/10.1006/pmed.2000.0735 (2000).
Carr, L. J. & Mahar, M. T. Accuracy of intensity and inclinometer output of three activity monitors for identification of sedentary behavior and light-intensity activity. J Obes 2012, 460271. (2012). https://doi.org/10.1155/2012/460271
Freedson, P., Pober, D., Janz, K. F. & S523-S530. Calibration of accelerometer output for children. Med. Sci. Sports Exerc. 37 https://doi.org/10.1249/01.mss.0000185658.28284.ba (2005).
Mumby, S. L. & Andrade, M. The impact the smarter lunchroom movement strategies have on school children’s healthy food selection and consumption: A systematic review. J. Child. Nutr. Manag. 42, 19 (2018).
Jacob, C. M. et al. A systematic review and meta-analysis of school-based interventions with health education to reduce body mass index in adolescents aged 10 to 19 years. Int. J. Behav. Nutr. Phys. Act. 18, 1. https://doi.org/10.1186/s12966-020-01065-9 (2021).
Liu, Z. et al. A systematic review and meta-analysis of the overall effects of school-based obesity prevention interventions and effect differences by intervention components. Int. J. Behav. Nutr. Phys. Act. 16, 95. https://doi.org/10.1186/s12966-019-0848-8 (2019).
Singhal, J., Herd, C., Adab, P. & Pallan, M. Effectiveness of school-based interventions to prevent obesity among children aged 4 to 12 years old in middle-income countries: A systematic review and meta-analysis. Obes. Rev. 22, e13105. https://doi.org/10.1111/obr.13105 (2021).
McLoughlin, G. M. et al. The importance of Self-Monitoring for behavior change in youth: findings from the SWITCH((R)) school wellness feasibility study. Int. J. Environ. Res. Public. Health. 16 https://doi.org/10.3390/ijerph16203806 (2019).
Vansteenkiste, M., Williams, G. C. & Ken, R. Toward systematic integration between self-determination theory and motivational interviewing as examples of top-down and bottom-up intervention development: autonomy or volition as a fundamental theoretical principle. Int. J. Behav. Nutr. Phys. Act. 9 https://doi.org/10.1186/1479-5868-9-23 (2012).
Schäfer, S. K. et al. Barriers and facilitators for the implementation of preventative mental health interventions among secondary schools in high-income countries: a systematic review. Eur. Child Adolesc. Psychiatry. 1–19. https://doi.org/10.1007/s00787-025-02796-5 (2025).
Scrimin, S. et al. Effects of socioeconomic status, parental stress, and family support on children’s physical and emotional health during the COVID-19 pandemic. J. Child. Fam Stud. 31, 2215–2228 (2022).
Hamdi, N. et al. Implementation of a Multi-Component school lunch environmental change intervention to improve child fruit and vegetable intake: A mixed-methods study. Int. J. Environ. Res. Public. Health 17 https://doi.org/10.3390/ijerph17113971 (2020).
Naylor, P. J. et al. Implementation of school based physical activity interventions: A systematic review. Prev. Med. 72, 95–115. https://doi.org/10.1016/j.ypmed.2014.12.034 (2015).
Ramos-Vidal, I., Palacio, J., Villamil, I. & Uribe, A. Examining the effect of the individual characteristics of implementers and the interaction of multiple relationships on the structure of psychosocial intervention teams. Implement. Sci. 15, 69. https://doi.org/10.1186/s13012-020-01032-9 (2020).
de Leeuw, R. R., de Boer, A. A. & Minnaert, A. E. M. G. The proof of the intervention is in the implementation; a systematic review about implementation fidelity of classroom-based interventions facilitating social participation of students with social-emotional problems or behavioural difficulties. Int. J. Educational Res. Open. 1, 100002. https://doi.org/10.1016/j.ijedro.2020.100002 (2020).
Acknowledgements
We would like to thank the schools (i.e., the district and schools administrators), cafeteria managers and crews, teachers, students, and families who participated in the ProudMe project. We acknowledge the following former or current undergraduate and graduate students who contributed to various aspects of the project: Virginia Bordelon, Kayla Drummond, Rachel Hunter, Gracie Chen, Katherine Christie, and Anna Whitfield for assisting with data collection; Bruce Quach for web development; Dino A. Pellisier, Madeline Yi, and Madison E. Lewis for designing art assets for the project; Dr. Stacy Imagbe, Dr. Weidong Li, Jared Smith, and Jordan Mathews for being involved in the intervention development. We further acknowledge Dr. Xin Li and Dr. Beibei Guo for collaborating in grants application.
Funding
This research was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health (1R15HD108765-01A1) and the Louisiana Board of Regents Research Competitiveness Subprogram [LEQSF(2022-24)-RD-A-03]). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Author information
Authors and Affiliations
Contributions
S.C. and A.E.S. conceptualized the study. Methodology was developed by A.E.S. and S.C. Formal analy-sis was conducted by S.C. and Y.N. Investigation was carried out by Y.N., P.S., Q.T., and S.C. Resources were provided by A.E.S. and S.C. Data curation was performed by Y.N., P.S., Q.T., and S.C. Y.N., P.S., Q.T., and S.C. prepared the original draft. Y.N., Q.T., P.S., A.E.S., R.R.R., R.A.U., K.E.S., M.S.R., J.N.A., F.W., and S.C. reviewed and edited the manuscript. Visualization was performed by Y.N. and S.C. Super-vision and project administration were led by S.C. Funding acquisition was managed by A.E.S., R.R.R., and S.C. All authors have reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Informed consent
All authors provided consent to the publication of this manuscript. Participants provided consent for the publication of anonymized data collected from the study.
Institutional review board statement
his study was conducted in accordance with the Declaration of Helsinki and was approved by the Louisiana State University Institutional Review Board (protocol code IRBAM-21-0702). Written informed consent was obtained from each of the participants involved in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Nie, Y., Tan, Q., Son, P. et al. Testing an adapted obesity prevention intervention in under resourced schools: a pilot clustered randomized controlled trial. Sci Rep 15, 31678 (2025). https://doi.org/10.1038/s41598-025-16754-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-16754-3
