
Abstract
The study aimed to analyze the predictive value of the vasoactive inotropic score (VIS) in the postoperative treatment of patients undergoing valve surgery for infective endocarditis (IE). At our institution, 334 patients underwent valve surgery for IE from 01/2016 to 12/2022. Patients with postoperative MCS device were excluded from this study. Data are presented as medians and 25th – 75th percentiles, or absolute numbers and percentages. Non-survivors had a significantly higher EuroSCORE II preoperatively (4.5 (2.3–9.8)% vs. 12.6 (5.7–20.9)%, p < 0.001). In non-survivors, Staphylococcus (89 (32.1%) vs. 20 (54.1%), p = 0.01) and Staphylococcus aureus (62 (22.4%) vs. 14(37.8%), p = 0.064) were significantly more frequently identified as causative pathogens. Non-survivors had significantly higher IL-6 levels at POD 1, 2 and 4 compared to survivors (p < 0.021). Non survivor had significantly higher VIS immediately postoperatively as well as 6 h, 12 h, 24 h, 36 h and 48 h after surgery. In addition, VIS at 48 h was identified as an independent variable associated with non-survival at values > 4.1. When comparing the ROC of lactate, ScvO2 and VIS after 48 h, VIS showed the highest AUC. The VIS is particularly suitable for patients with infective endocarditis due to combined assessment of postoperative cardiovascular dysfunction and IE related inflammatory response. We provided suggestive evidence that the amount of cardiovascular support represented as the VIS has a predictive value regarding mortality in patients undergoing valve replacement for IE. In addition, VIS showed superiority compared to conventional scoring systems for predicting outcome in the intensive care of postoperative IE patients.
Similar content being viewed by others
Introduction
Patients suffering from infective endocarditis (IE) are prone to excessive release of cytokines and other inflammatory mediators during surgery as they are exposed to infected material during the removal of vegetations and resection of infected tissue. In addition, surgical trauma, cardiopulmonary bypass, ischemia-reperfusion phenomena, and the effects of general anesthesia can lead to a generalized inflammatory response, vasoplegic reaction and therefore multiorgan failure in patients undergoing cardiac surgery1,2. Common ICU scoring systems were not primarily developed for postoperative cardiac surgery patients so that patients’ reactions to the surgery, cardiopulmonary bypass and inflammatory release especially in IE patients are hardly taken into account3,4,5,6.
The vasoactive-inotropic score (VIS) is calculated from the weighted sum of all administered inotropes and vasoconstrictors and thus reflects the extent of pharmacological support of the cardiovascular system6,7. Originally developed for the treatment of septic patients, in recent years it has been shown that a higher VIS value predicts unfavorable outcomes after pediatric cardiac surgery6,7,8,9,10. The use of the VIS in postoperative IE patients is supported by its role in assessing the severity of the need for circulatory support, which correlates with morbidity and mortality. While the VIS has traditionally been used as a preoperative indicator, its usefulness in the postoperative setting has been confirmed by studies indicating its prognostic value in critical care, particularly in relation to the intensity of inotropic and vasopressor support, which may indicate the risk of adverse outcomes (e.g. mortality, prolonged ICU stay)6,7,8. In particular, maximum VIS within 24 h of ICU admission (VISmax) has been repeatedly evaluated as a good predictor of adverse outcomes in these patients6,7,8. Although several studies have investigated the predictive value of VIS in pediatric cardiac surgery, there are few studies in adult cardiac surgery patients and no study investigating patients suffering from IE5,6,8,10,11.
The aim of the present study was to investigate the predictive value of the VIS in postoperative cardiac surgery patients suffering from IE by a combined assessment of postoperative cardiovascular dysfunction and IE-related inflammatory response.
Methods
Study design
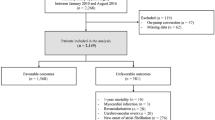
All methods were carried out in accordance with relevant guidelines and regulations. This study was approved by the institutional ethics committee of the Ludwig Maximilian University (22–0612). Due to the retrospective nature of the study, the need to obtain the informed consent was waived by the institutional ethics committee of the Ludwig Maximilian University (22–0612). Postoperative treatment and data collection was performed as part of routine patient care. Data acquisition was based on institutional databases and was subsequently anonymized. All data processing described in this study was in accordance with the institutional ethics board and national data safety regulations. Between January 2016 and December 2022, 334 consecutive patients underwent valve surgery for IE at our institution. Patients with postoperative mechanical circulatory support (MCS) devices were excluded from this study.
Scoring systems and definitions
The European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) was used to predict the risk of perioperative mortality12. VIS was calculated according to the following formula: [Dopamine dose (µg/kg/min)] + [Dobutamine dose (µg/kg/min)] + [50*Levosimendan dose (µg/kg/min)] + [100*Noradrenaline dose (µg/kg/min)] + [100*Adrenaline dose (µg/kg/min)] + [10000*Vasopressin dose (U/kg/min)] + [10*Milrinone dose (µg/kg/min)]13. Cardiac output was calculated according to modified Fick formula: CO (l/min) = [VO2] / [13,4*Hb*(SaO2-ScvO2)]. Cardiac index was calculated by the following formula: CI(l/min/m2) = CO / BSA14,15,16.
Statistical analysis
Data were analyzed using the IBM SPSS Statistics Data Editor® version 29 (IBM Corp. Released 2022. IBM SPSS Statistics, Version 29.0. Armonk, NY: IBM Corp.). Data were tested for normal distribution using the Kolmogorov-Smirnov test with Lillefors correction. Categorical variables were analyzed using the Chi-Squared and Fisher‘s exact test and continuous variables using the Mann-Whitney-U test. Multivariable analysis included logistic regression using a forward stepwise (conditional) model, where significance for entry was set at p < 0.05 and significance for exit was p < 0.10. The regression model was verified using the goodness of fit test as well as tests for autocorrelation, multicollinearity, and heteroscedasticity. Illustrations were prepared using GraphPad Prism (GraphPad Software Inc., San Diego, CA, USA). Data are presented as medians (25–75th quartiles) or as absolute numbers (percentages) unless otherwise specified.
Results
Patient characteristics, comorbidities and preoperative condition
Patient characteristics and comorbidities are listed in Table 1. There were no differences in age and gender distribution between survivors and non-survivors. Non-survivors had a significantly higher EuroSCORE II preoperatively (4.5 (2.3–9.8) vs. 12.6% (5.7–20.9), p < 0.001). Non-survivors were significantly more likely to have IDDM (61 (20.6%) vs. 18 (45.0%), p < 0.001), PAD (17 (5.8%) vs. 7 (17.5%), p = 0.015) and CKD (74 (25.0%) vs. 22 (55.0%), p < 0.001). Non-survivors were significantly more frequently ventilated preoperatively (13 (4.4%) vs. 7 (17.5%), p = 0.005).
IE specific data
IE-specific data and the preoperative status are listed in Table 1. There was no statistically significant difference between the cohorts in terms of the affected heart valves. In non-survivors, Staphylococcus sp. (89 (32.1%) vs. 20 (54.1%), p = 0.01) and Staphylococcus aureus (62 (22.4%) vs. 14 (37.8%), p = 0.064) were significantly more frequently identified as causative pathogens. Conversely, survivors suffered statistically significant more frequently from streptococcal endocarditis (95 (34.4%) vs. 6 (16.2%), p = 0.038).
Pre- and postoperative laboratory results
Detailed pre- and postoperative laboratory results are listed in Table 2. Non-survivors had statistically significant higher bilirubin levels (mg/dl) preoperative and on POD 0 to 4, statistically significant higher thrombocyte levels (G/l) on POD 0, 1 and 4, statistically significant higher leukocyte levels (G/l) preoperative and on POD 2, 3 and 4, statistically significant higher IL-6 levels (pg/ml) preoperative and on POD 1, 2 and 4 and statistically significant higher C-reactive protein (mg/dl) preoperative compared to survivors.
Postoperative morbidities
Postoperative morbidities are listed in Table 3. Non-survivors had a significantly longer duration of ventilation (19 (13–25) vs. 44 h (19–100), p < 0.001), had a significantly higher rate of cerebrovascular events (50 (17.1%) vs. 13 (35.1%), p = 0.014) and were significantly more likely to require dialysis (28 (9.5%) vs. 11 (29.7%), p < 0.001). Non-survivors were significantly more likely to require red blood cell concentrates (3 (1–4) vs. 4 units (2–7), p < 0.001), platelet concentrates (0 (0–1) vs. 3 units (1–4), p < 0.001) and fresh frozen plasma (0 (0–4) vs. 12 units (7–18), p < 0.001).
Vasoactive inotropic score and postoperative vasopressor therapy
The VIS course in the first 48 h after surgery is shown in Fig. 1; Table 4. Non-survivors had a statistically significant higher vasoactive inotropic score compared to survivors immediately postoperatively as well as 6 h, 12 h, 24 h, 36 h, and 48 h after surgery. Postoperative freedom from vasopressor therapy in the first 48 h after surgery is shown in Fig. 2; Table 4. Survivors were significantly more likely to be free from vasopressors at 6 h, 12 h, 24 h, 36 h, and 48 h compared to non-survivors.

Vasoactive inotropic score. Vasoactive inotropic score was calculated postoperative (= admission on ICU), 6 h, 12 h, 24 h, 36 h, and 48 h after surgery. Data are presented as medians (25–75th quartiles) or as absolute numbers (percentages). Marked p-values are two-sided significant at least at the 0.05 level.

Freedom from vasopressors. Survivors and Non-survivors compared in terms of freedom from vasopressors postoperative (= admission on ICU), 6 h, 12 h, 24 h, 36 h, and 48 h after surgery. Data are presented as medians (25–75th quartiles) or as absolute numbers (percentages). Marked p-values are two-sided significant at least at the 0.05 level.
Hemodynamic course
The hemodynamic course including cardiac output, cardiac index and ScvO2 (%) in the first 48 h after surgery is shown in Figs. 3 and 4; Table 4. There was no significant difference in cardiac output and cardiac index between survivors and non-survivors. At 48 h after surgery, non-survivors had a significantly higher ScvO2 (64 (59–70) % vs. 68 (60–73) %, p = 0.026).

Central venous saturation. Central venous saturation (ScvO2) was measured postoperative (= admission on ICU), 6 h, 12 h, 24 h, 36 h, and 48 h after surgery. Data are presented as medians or as absolute numbers (percentages). Marked p-values are two-sided significant at least at the 0.05 level.

Cardiac Index. Cardiac index was calculated postoperative (= admission on ICU), 6 h, 12 h, 24 h, 36 h, and 48 h after surgery. Data are presented as medians or as absolute numbers (percentages). Marked p-values are two-sided significant at least at the 0.05 level.
Lactate
The lactate levels in the first 48 h after surgery are shown in Fig. 5; Table 4. Non-survivors had significantly higher lactate levels (mmol/l) compared to survivors immediately postoperatively and 6 h, 12 h, 24 h, 36 h and 48 h after surgery.

Serum lactate. Serum lactate levels were measured postoperative (= admission on ICU), 6 h, 12 h, 24 h, 36 h, and 48 h after surgery. Data are presented as medians or as absolute numbers (percentages). Marked p-values are two-sided significant at least at the 0.05 level.
ROC analysis
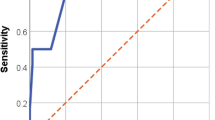
ROC analysis is shown in Fig. 6A and B. In a sensitivity analysis the ability of EuroSCORE II for predicting non-survival was poor (AUC 0.541; 95% CI 0.424–0.658) (Fig. 6A). VIS after 48 h (AUC: 0.749, 95%CI: 0.637–0.860, p < 0.001); ScvO2 after 48 h (AUC: 0.636, 95%CI: 0.516–0.756, p = 0.021) and lactate after 48 h (AUC: 0.639, 95%CI: 0.536–0.742, p = 0.018) independently predicted non-survival. VIS at 48 h had the highest AUC (Fig. 6B).

(A) ROC sensitivity analysis. Receiver operating characteristic analysis. AUC: Area under the curve; CI: Confidence interval; VIS: Vasoactive inotropic score. (B) ROC analysis. Receiver operating characteristic analysis. AUC: Area under the curve; CI: Confidence interval; ScvO2: Central venous saturation; VIS: Vasoactive inotropic score; Marked p-values are two-sided significant at least at the 0.05 level.
Multivariate models
The variables that were independently associated with non-survival in the multivariate analysis are shown in Fig. 7. CKD (OR: 3.416, 95% CI: 1.208–9.658, p = 0.021), lactate at 48 h > 1.5 (OR: 3.051, 95% CI: 1.036–8.986, p = 0.043) and VIS at 48 h > 4.1 (OR: 3.430, 95% CI: 1.212–9.710, p = 0.020) were independently associated with non-survival.

Prediction of mortality. Multivariate analysis: CI: Confidence interval; CKD: Chronic kidney disease; IDDM: Insulin dependent diabetes mellitus; VIS: Vasoactive inotropic score; ScvO2: Central venous saturation; Marked p-values are two-sided significant at least at the 0.05 level.
Discussion
This is the first study to assess the predictive value of VIS calculated in the postoperative care of patients suffering from infective endocarditis. The VIS, primarily used in the intensive care treatment of septic patients, has been shown to be a good predictor for poor clinical outcome after cardiac surgery in various patient groups5,6,7,8,11,17. Studies repeatedly described, that an increased requirement for vasoactive and inotropic agents during the first 48 h after cardiac surgery can successfully predict the risk of postoperative complications, including mortality up to one year5,6,11,17.
The principal findings of the present study are as followed: (1) The VIS at 48 h independently predicted mortality after cardiac surgery in IE patients and (2), the VIS is particularly suitable for patients with infective endocarditis due to combined assessment of postoperative cardiovascular dysfunction and IE related inflammatory response.
The present study showed that an increased need for vasoactive and inotropic agents, quantified by the VIS, was significantly associated with non-survival after surgical treatment of IE. The VIS was significantly increased in patients expiring during hospital stay at almost any time within the first 48 h and a score above 4.1 was identified as independent threshold of mortality. When comparing lactate levels, SvO2, and VIS after 48 h, VIS showed the highest predictive value in terms of mortality.
Surgical trauma, cardiopulmonary bypass, ischemia-reperfusion phenomena, and the effects of general anesthesia cause a vasoplegic reaction that can lead to a generalized inflammatory response and multiorgan failure1,2. Acute cardiovascular dysfunction is anticipated in 20% or even more patients in the perioperative period of cardiac surgery18. At the same time variable degrees of left ventricular dysfunction have been observed in 25–50% of septic shock patients18. The combination of all these effects makes the postoperative treatment of IE patients challenging. IE patients are prone to excessive release of cytokines and other inflammatory mediators during surgery as they are exposed to infected material during the removal of vegetations and resection of infected tissue. There is ample evidence that the following increase in cytokine levels correlates with the severity of postoperative organ dysfunction in IE patients19,20,21. In sepsis, high levels of proinflammatory cytokines (i.e., IL-6, IL-8, IL-18, and IL-1β) have been associated with higher mortality, a similar correlation in IE patients can be assumed19,20,21. The present study confirms this correlation. There was a significant association between preoperative as well as POD 1, POD 2 and POD 4 elevated IL6 levels and non-survivors. The combination of cardiovascular dysfunction as well as CPB- and IE-associated inflammation in the postoperative assessment of IE patients is not yet addressed by conventional ICU scoring systems. The analysis of vasoactive and inotropic support using the VIS, which reflects both cardiac dysfunction and inflammation-related vasoplegia, can close this gap.
Patients with critical cardiovascular dysfunction often require a combination of vasoactive and inotropic agents. However, the underlying cause of this dysfunction can vary, particularly in postoperative IE patients. As previously described, the condition may also has an inflammatory or surgical etiology in addition to purely cardiovascular causes. The VIS reflects the extent of hemodynamic support required, with a negative correlation between VIS and clinical outcomes13. In the present study, there was no significant correlation between non-survival and a median cardiac index of > 3 l/min/m2 for all measurements, so therapeutic success in terms of guideline directed postoperative hemodynamic management (MAP > 65mmHg; CI > 2.1 l/min/m2) can be assumed but did not prevent non-survivors from having poor outcome22. Other studies already confirmed that myocardial function is depressed in sepsis despite hemodynamic measurements showing increased cardiac output18. Furthermore, not only macro- but also microcirculatory dysfunction may contribute to poor outcome in septic patients. Even if increased CO initially compensates for vasodilation and fluid shifts, it does not ensure adequate tissue perfusion. Microcirculatory disorders, such as endothelial dysfunction, leukocyte adhesion and microthrombosis, impair blood flow at the capillary level and prevent adequate tissue oxygenation23,24.
Several mechanisms may explain the increased mortality in postoperative patients caused by a high amount of vasoactive support in a vicious circle. This includes increased myocardial oxygen consumption induced by inotropic support and an increased risk for cardiac arrhythmias18,25. In addition, low cardiac output may be a result of cardiac tamponade, so inotropes may mask this by initially improving hemodynamics and therefore delaying early surgical intervention25. In addition, catecholamines are associated with reduced metabolic efficiency as they promote the oxidation of fatty acids over glucose25. This may be a further barrier to optimal cardiac performance. Studies have also found an association with increased bacterial growth, increased bacterial virulence, biofilm formation, insulin resistance and hyperglycemia25,26. If this vicious circle is not broken within the first 48 h, the outcome will be poor.
VIS represents the extent of medical inotropic and vasoactive support as a therapeutic necessity in the complex treatment of postoperative and IE-associated circulatory insufficiency as well as the side effects caused by this amount of support, which explains its particular suitability for this special patient group.
Compared to postoperative lactate levels and ScvO2, which are commonly used in postoperative monitoring of cardiac surgery patients, the VIS showed superiority in predicting mortality after 48 h. In the present study, lactate, which can be elevated postoperatively due to a transient decrease in systemic organ perfusion, e.g. due to high vasopressor demand, consistently showed a significant correlation with mortality, albeit with a pronounced range of variation and is considered a comparatively unspecific outcome parameter11,27,28. ScvO2 levels only showed a significant correlation with non-survival after 48 h and surprisingly they were significantly increased compared to survivors. Studies have shown that ScvO2 levels can be elevated in septic patients due to microcirculatory dysfunction and insufficient tissue oxygen consumption29,30. This confirms, that ScvO2 levels especially in septic patients may not always be a reliable indicator for tissue perfusion or outcome and a comprehensive assessment of macro- and microcirculatory parameters is warranted29,30. In addition, ScvO2 levels are considered susceptible to disturbances caused by circulatory stress and analgosedation, which preferentially redistribute the blood towards the heart muscle and brain31.
EuroSCORE II was significantly associated with non-survival in the univariate analysis. However, evaluating its predictive performance in the ROC analysis revealed only limited discriminatory ability, especially when compared to VIS at 48 h. We therefore decided to include key components of EuroSCORE II such as CKD, IDDM and preoperative mechanical ventilation as individual variables. Including both the composite score and its components would have introduced substantial collinearity and impaired model stability. These findings suggest that the VIS provides superior predictive accuracy in this clinical context.
Unlike traditional outcome-based parameters which are more general and consider different organ systems, the VIS focuses specifically on the severity of circulatory support. The VIS captures changes in circulatory support in real time, may providing an early and specific indicator of adverse outcomes such as mortality, prolonged ICU stay or the need for additional interventions. Further studies comparing the VIS with other outcome markers such as SOFA or SAPS II could provide additional insight into its role as a complementary tool in predicting postoperative outcomes.
Conclusion
The VIS is particularly suitable for patients with infective endocarditis due to combined assessment of postoperative cardiovascular dysfunction and IE related inflammatory response. We provided suggestive evidence that the amount of cardiovascular support represented by the VIS has a strong predictive value regarding mortality in patients undergoing valve replacement for infective endocarditis. In addition, VIS showed superiority over conventional scoring systems for monitoring hemodynamics in the intensive care unit for postoperative IE patients.
Limitations
This is a retrospective single-center study with the inherent limitation of such an analysis. The small number of patients is associated with a low power of statistical analyses. The VIS was calculated as the sum of the maximum dose of all inotropes or vasopressors administered during the study period. Consequently, the VIS is not a suitable method for assessing the individual impact of each drug on the outcome.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to national data safety regulations and are available from the corresponding author upon reasonable request.
Abbreviations
- AUC:
-
Area under the curve
- BCNIE:
-
Blood culture negative infective endocarditis
- BSA:
-
Body surface area
- CI:
-
Cardiac index
- CKD:
-
Chronic kidney disease
- CO:
-
Cardiac output
- COPD:
-
Chronic obstructive pulmonary disease
- CPB:
-
Cardio pulmonal bypass
- DAPT:
-
Dual antiplatelet therapy
- EuroSCORE II:
-
European System for Cardiac Operative Risk Evaluation II
- FFP:
-
Fresh frozen plasma
- Hb:
-
Hemoglobin
- ICU:
-
Intensive care unit
- IDDM:
-
Insulin dependent diabetes mellitus
- IE:
-
Infective endocarditis
- MCS:
-
Mechanical circulatory support
- NOAC:
-
Novel oral anticoagulants
- PAD:
-
Peripheral arterial disease
- PCI:
-
Percutaneous coronary intervention
- POD:
-
Postoperative day
- PRBC:
-
Packed red blood cells
- PTCA:
-
Percutaneous transluminal coronary angioplasty
- ROC analysis:
-
Receiver operating characteristic analysis
- SaO2 :
-
Arterial oxygen saturation
- SAPT:
-
Single antiplatelet therapy
- ScvO2 :
-
Central venous oxygen saturation
- TAVR:
-
Trans-aortic valve replacement
- VIS:
-
Vasoactive inotropic score
- VISmax:
-
Vasoactive inotropic score maximum
References
Kilger, E. et al. Stress doses of hydrocortisone reduce severe systemic inflammatory response syndrome and improve early outcome in a risk group of patients after cardiac surgery. Crit. Care Med. 31, 1068–1074 (2003).
Datt, V. et al. Vasoplegic syndrome after cardiovascular surgery: A review of pathophysiology and outcome-oriented therapeutic management. J. Card Surg. 36, 3749–3760 (2021).
Vincent, J. L. et al. The SOFA (Sepsis-related organ failure Assessment) score to describe organ dysfunction/failure. On behalf of the working group on sepsis-related problems of the European society of intensive care medicine. Intensive Care Med. 22, 707–710 (1996).
Knaus, W. A., Draper, E. A., Wagner, D. P. & Zimmerman, J. E. APACHE II: a severity of disease classification system. Crit. Care Med. 13, 818–829 (1985).
Chang, C. H. et al. Sequential organ failure assessment score predicts mortality after coronary artery bypass grafting. BMC Surg. 17, 22 (2017).
Koponen, T. et al. Vasoactive-inotropic score and the prediction of morbidity and mortality after cardiac surgery. Br. J. Anaesth. 122, 428–436 (2019).
Gaies, M. G. et al. Vasoactive-inotropic score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass. Pediatr. Crit. Care Med. 11, 234–238 (2010).
Gaies, M. G. et al. Vasoactive-inotropic score is associated with outcome after infant cardiac surgery: an analysis from the pediatric cardiac critical care consortium and virtual PICU system registries. Pediatr. Crit. Care Med. 15, 529–537 (2014).
Favia, I., Vitale, V. & Ricci, Z. The vasoactive-inotropic score and levosimendan: time for LVIS? J. Cardiothorac. Vasc Anesth. 27, e15–16 (2013).
Davidson, J. et al. Prospective validation of the vasoactive-inotropic score and correlation to short-term outcomes in neonates and infants after cardiothoracic surgery. Intensive Care Med. 38, 1184–1190 (2012).
Kwon, J. H. et al. Vasoactive inotropic score as a predictor of long-term mortality in patients after off-pump coronary artery bypass grafting. Sci. Rep. 12, 12863 (2022).
Nashef, S. A. M. et al. EuroSCORE II. Eur. J. Cardiothorac. Surg. 41, 734–744 (2012). discussion 744–745.
Belletti, A., Lerose, C. C., Zangrillo, A. & Landoni, G. Vasoactive-inotropic score: evolution, clinical utility, and pitfalls. J. Cardiothorac. Vasc. Anesth. 35, 3067–3077 (2021).
Dehmer, G. J., Firth, B. G. & Hillis, L. D. Oxygen consumption in adult patients during cardiac catheterization. Clin. Cardiol. 5, 436–440 (1982).
Ragosta, M. Textbook of Clinical Hemodynamics E-Book: Textbook of Clinical Hemodynamics E-Book (Elsevier Health Sciences, 2017).
Alkhouli, M. et al. Clinical utility of central venous saturation for the calculation of cardiac index in cardiac patients. J. Card Fail. 20, 716–722 (2014).
Barge-Caballero, E. et al. Evaluation of the preoperative vasoactive-inotropic score as a predictor of postoperative outcomes in patients undergoing heart transplantation. Int. J. Cardiol. 185, 192–194 (2015).
Parissis, J. T., Rafouli-Stergiou, P., Stasinos, V., Psarogiannakopoulos, P. & Mebazaa, A. Inotropes in cardiac patients: update 2011. Curr. Opin. Crit. Care. 16, 432–441 (2010).
Diab, M. et al. Cytokine hemoadsorption during cardiac surgery versus standard surgical care for infective endocarditis (REMOVE): results from a multicenter randomized controlled trial. Circulation 145, 959–968 (2022).
Diab, M. et al. Changes in inflammatory and vasoactive mediator profiles during valvular surgery with or without infective endocarditis: A case control pilot study. PLoS One. 15, e0228286 (2020).
Hotchkiss, R. S., Monneret, G. & Payen, D. Sepsis-induced immunosuppression: from cellular dysfunctions to immunotherapy. Nat. Rev. Immunol. 13, 862–874 (2013).
Delgado, V. et al. 2023 ESC guidelines for the management of endocarditis. Eur. Heart J. 44, 3948–4042 (2023).
Wang, H., Ding, H., Wang, Z. Y. & Zhang, K. Research progress on microcirculatory disorders in septic shock: A narrative review. Med. (Baltim). 103, e37273 (2024).
Yajnik, V. & Maarouf, R. Sepsis and the microcirculation: the impact on outcomes. Curr. Opin. Anesthesiology. 35, 230 (2022).
Shahin, J., deVarennes, B., Tse, C. W., Amarica, D. A. & Dial, S. The relationship between inotrope exposure, six-hour postoperative physiological variables, hospital mortality and renal dysfunction in patients undergoing cardiac surgery. Crit. Care. 15, R162 (2011).
Singer, M. Catecholamine treatment for shock–equally good or bad? Lancet 370, 636–637 (2007).
Andersen, L. W. Lactate elevation during and after major cardiac surgery in adults: A review of etiology, prognostic value, and management. Anesth. Analg. 125, 743–752 (2017).
Hajjar, L. A. et al. High lactate levels are predictors of major complications after cardiac surgery. J. Thorac. Cardiovasc. Surg. 146, 455–460 (2013).
Pope, J. V. et al. Multicenter study of central venous oxygen saturation (ScvO2) as a predictor of mortality in patients with sepsis. Ann. Emerg. Med. 55, 40–46e1 (2010).
Textoris, J. et al. High central venous oxygen saturation in the latter stages of septic shock is associated with increased mortality. Crit. Care. 15, R176 (2011).
Saha, S., Baraki, H., Kutschka, I. & Hadem, J. Predictive value of ScvO2 monitoring for pericardial tamponade after cardiac surgery. Herz 44, 76–81 (2019).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
P.S.:Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Visualization, Writing - original draft; C.T.: Data curation; S.S.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing - original draft; D.W.: Resources, Writing – review & editing; C.K.: Writing – review & editing; C.M.: Writing – review & editing; K.H.: Data curation; S.P.: Writing – review & editing; C.H.: Resources, Supervision, Writing – review & editing; D.J.: Conceptualization, Investigation, Methodology, Project administration, Validation, Writing – review & editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the institutional ethics committee of the Ludwig Maximilian University Munich (Project Nr.:22–0612) on the 03rd of August 2022.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schnackenburg, P., Ternka, C., Saha, S. et al. The predictive value of the vasoactive inotropic score in the postoperative treatment of patients suffering from infective endocarditis. Sci Rep 15, 37587 (2025). https://doi.org/10.1038/s41598-025-16769-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-16769-w
