
Abstract
Evaluate the fracture resistance of premolar teeth with MOD cavities restored with Diatomite Zirconia/Silica Filled Resin Composite Versus Barium Glass/Yetterbium Fluoride Filled resin composite systems. A 40 maxillary premolar were divided equally into four main groups (10 teeth each); a positive control group of unprepared teeth and a negative control group with prepared and unrestored MOD cavity. While the two other restored groups in which teeth with prepared MOD cavities were restored either with Diatomite Zirconia/Silica Filled Resin Composite (Zircon Fill composite, ZF) or Barium Glass/Yetterbium Fluoride Filled resin composite (Neo Spectra Composite, NS). A standardized MOD cavity was prepared in premolar teeth. Teeth were restored according to the corresponding group, and then exposed to thermocycling prior fracture resistance tested. Data collected from fracture resistance and failure mode were collected and statistically analyzed with ANOVA test. The significance level was set at p < 0.05 within all tests. There was a significant difference between different tested groups, with prepared teeth having significantly lower fracture resistance than sound teeth and samples restored with both restorative materials (p < 0.001). For Neo Spectra, most samples had mixed while Zirconfil were either had adhesive or cohesive failures with no statistically significant difference (p = 0.077). All the associations between fracture resistance and failure modes were not statistically significant. The two tested resin composites exhibited similar fracture resistance to each other and to sound teeth. Diatomite Zirconia/Silica Filled Resin Composite versus Barium Glass/Yetterbium Fluoride Filled resin composite systems were able to reinforce and restore the strength properties of the tooth.
Similar content being viewed by others
Introduction
MOD cavity design critically weakened the tooth structure. From a biomimetic perspective, preserving the balances between mechanical, biological, adhesive, functional, and esthetic characteristics depends critically on the conservation and preservation of tooth structures. Nevertheless, corono-radicular proportions frequently restrict this choice in premolar teeth. The loss of the tooth’s marginal ridges, which are regarded as the tooth anchor, severely weakened the tooth because they experience significant cuspal deflection, which drastically reduces the tooth’s resistance to fracture and leads to the development of cuspal microfractures brought on by pragmatic occlusal forces. This would provide a unique challenge for the filling materials in terms of durability and resistance to tooth breakage1.
To solve this frequent problem, tooth restorations made of a material that is resistant to fracture under high occlusal pressure are required. Because resin composite can strengthen a tooth by bonding the restoration material to the tooth structure, it is regarded as an appropriate restorative material for posterior teeth located in stress-bearing zones. They may also function as an internal splint to further support the teeth and greatly boost the dental structure’s fracture resistance2,3. When compared to alternative materials, their wear characteristics and growing strength make them a formidable option in the therapeutic resources. The characteristics of fillers, the resin matrix, or the interaction between fillers and matrix are the main areas of study for resin composites. Fillers are crucial components of dental composites because they regulate various aspects of the restoration, including its wear resistance, strength, stiffness, radiopacity, thermal expansion, smoothness, and polishability. Nonetheless, the composite materials continue to be vulnerable to fractures, degradation of the margins, and secondary caries, which is the most frequent cause of restorative replacement4.
Over the past few years, there has been a considerable improvement in the clinical performance of dental composites that have recently been developed. Numerous researchers have discovered various options to alter the material structure to increase the qualities of composites3. Concerning the matrix of composites, some research has addressed the instability of methacrylate and bisphenol A toxicity by modifying the functional groups or creating antimicrobial monomers4. But in searching for the filler particles, the primary modifications were more about shaping and shrinking in size. These days, spherically shaped barium glass and zirconium particles with nanometric or nano and micrometric sizes (also known as nanohybrid composites) are the most often utilized particles5,6. An obvious advancement in dental materials is the use of nanoparticles and their clusters to create nanocomposites. It appears reasonable to state that these materials provide good strength and final aesthetics because of their superior polishing capacity7,8.
Certain porous fillers have been added to dental composites due to the need for additional improvements in mechanical properties and matrix/filler interactions9. In this regard, composite incorporating diatomite is currently accessible. Diatomite, a porous silicate sourced from diatomaceous algae, has a large surface area, a low density, is less expensive than other filler materials, and has been utilized to improve the mechanical properties of polymeric composites10. Controlling diatomite pore size and morphology can enhance its photonic, mechanical, absorptive, and diffusive capabilities, according to current developments in nanotechnology research11. Furthermore, a drug delivery method for medicinal and regenerative objectives has recently been employed with this porous silica. Aside from that, research has shown that adding diatomite to polymeric materials improves their mechanical qualities for a variety of uses. 12 In this sense, the effects of diatomite incorporation in dental composites may present an intriguing substitute in terms of better entanglement between the matrix and filler and monomer interpenetration through diatomite pores during polymerization. This may lead to a higher degree of conversion and favorable mechanical properties13. The manufacturer claimed that the resin composite material containing zirconia filler and diatomite will improve the mechanical properties of the material so it could be used successfully in posterior restoration, particularly in MOD cavities. This addition of zirconia filler will reinforce the material for posterior restoration.
Because of the mechanical mating of the monomer inside the pores, resin-based materials with a zirconia-silica structure showed a higher degree of conversion and reduced polymerisation shrinkage in a clinical context. In terms of flexure strength and elastic modulus, the diatomite-based resin composite showed similar mechanical properties and dentin bonding to traditional resin composites13. Thus, evaluating the fracture resistance of premolar teeth with MOD cavities treated with diatomite Zirconia/Silica Filled Resin Composite versus Barium Glass/Yetterbium Fluoride Filled Resin Composite systems was shown to be helpful because there is a limited amount of research comparing these materials. The study’s null hypothesis examined the idea that there wouldn’t be a discernible difference in the fracture resistance of resin composite restorations with different types of fillers.
Methods
Two types of resin composite materials with different composition and amount of filler loading were used in the current study and listed in Table 1. Neo Spectra Composite (NS, Dentsply, Konstanz, Germany) with ST Sphere Tec granular filler technology and Zircon Fill Composite (Maquira Dental group, Brazil) with Silica filler associated with zirconia and diatomite which is porous silica. The materials used in this study, their descriptions, compositions and manufacturers were mentioned in Table 1.
Study setting
The study protocol of this experimental laboratory preclinical study was approved by the research ethical committee at the Faculty of Dentistry, October 6 University, Egypt (RECO6U/2-2024) at its meeting held on January 3, 2024, that is in accordance with the declaration of Helsinki and its later modification.
The selection of teeth and storage
This study used non-carious human maxillary premolar teeth that were extracted for orthodontic purposes from patients between the ages of 20 and 35 visiting the clinic of oral surgery department according to ethical approval and infection control protocols. An informed consent was obtained from all the participants whose teeth were extracted and used in the study. Teeth were subsequently immersed in a 1% chloramine-T solution for duration of 72 h, serving as a disinfectant. The teeth were examined using magnification lens of ×7 to exclude any tooth with cracks or structural defects. The chosen teeth were carefully cleared of calculus and tissue buildup, polished with pumice, and rotated with a brush at a standard speed. Teeth were then stored in distilled water at 37 °C ± 1 °C, using and incubator (BTC, model: BT1020, Cairo, Egypt). This isolation was replaced every five days. Using a digital caliper, all the chosen teeth’s bucco-lingual dimensions at the point of maximal convexity of their crowns were found to be between 8.4 and 9.4 mm, with none of them exhibiting hypoplastic defects or cavities.
Specimen preparation and grouping
Based on previous study16, A total of 40 freshly extracted maxillary premolar teeth were randomly and equally divided into four main groups (10 teeth each); a positive control group of unprepared teeth and a negative control group with prepared and unrestored MOD cavity. While the two other restored groups in which teeth with prepared MOD cavities were restored either with diatomite Zirconia/Silica Filled Resin Composite (Zircon Fill composite, ZF) or Barium Glass/Yetterbium Fluoride Filled resin composite (Neo Spectra Composite, NS).
Cavity preparation
To avoid operator influences in cavity preparation and restorative procedure, a single operator performed all of the restorative procedures. Using a high-speed handpiece (PANA MAX, NSK, Japan) and a no. 245 carbide bur (Healthico, USA), a standardized MOD cavity was created in premolar teeth while a lot of water coolant was used. The cavity dimension was as an occlusal extension of 2 mm depth and roughly one-third of the buccolingual width, connecting mesial and distal proximal boxes that were intended to be positioned for the cervical margins around 1 mm above the CEJ. the occlusal shape of the proximal boxes was calculated as roughly one-third of the mesiodistal size and half of the buccolingual intercuspal distance.
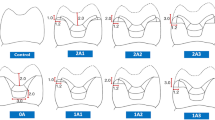
Twice every ten preparations, the carbide bur was replaced. Next, the outline was marked on the tooth, and the measurements of the cavity preparation were measured with a digital caliper. The approximate standardization of cavity preparation dimensions was determined to be 1.5 mm axial wall depth and 4 mm occluso-gingival height. The mesial cavity preparation was standardized to a bucco-lingual width of 2.5 mm in terms of width. The pulpal floor had an isthmus width of 2 mm and a depth of 2.0 mm from the preparation’s occlusal cavo-surface boundary. The external angle at the gingival floor was 90° to the external surface located 0.5 mm coronal to CEJ. During cavity preparation, the cavity dimensions were checked with a digital caliber. (Fig. 1)

Illustrated 3D Model of standardized cavity dimensions of MOD prepared cavity in premolar.
Restoration of prepared cavities with resin composite materials
In the dental study model (El Banna, Egypt), every tooth with MOD-prepared cavities was positioned so that it was in appropriate mesial and distal contact with neighboring ivory teeth. Palodent Sectional Matrix System, Dentsply, USA, a pre-contoured sectional matrix standard kit, was utilized. Two matrices of standard size were positioned mesially and distally with the appropriate wooden wedge size, featuring BiTine round rings. Using nanofilled resin composite materials, all produced cavities in the restored groups were restored in accordance with the designated group. The bonding procedure was followed in accordance with the manufacturer’s guidelines. Using a disposable microbrush, the adhesive system (Prime and Bond Universal Dental Adhesive, Dentsply, Konstanz, Germany) was applied. It was then agitated for 10 s, thinned with a gentle air stream under light pressure for 5 s, and polymerized for 20 s at zero distance using an LED curing unit (800 mW/cm2). Using a gold-plated composite applicator (Miltax, Germany), incremental amounts of the resin composite were added to each of the two cavities. After that, the resin composite material was light cured using an LED light curing device in accordance with the testing groups that were previously mentioned. Using the integrated radiometer, the light irradiance was measured prior to each curing cycle.
Mounting in acrylic blocks
To replicate the periodontal tissue, the roots were submerged in molten pink wax to generate a homogeneous layer of wax with an average thickness of 0.2 to 0.3 mm, which corresponds to the typical width of the periodontal ligament space. Each tooth was placed separately in blocks of polymethyl-methacrylate (PMMA) resin, oriented vertically along its long axis, and inserted into the resin to a depth of 2.0 mm apically from the center of the mesial and distal surfaces to the cemento-enamel junction (CEJ). The acrylic blocks were made using specially made cylindrical Teflon molds that had an internal diameter of 20 mm, an external diameter of 30 mm, and a height of 20 mm to fit the acrylic resin. Every mold has a cover that is secured to the top with two tiny pins. To locate the center of the acrylic block, there is a rounded hole with a diameter of 5.0 mm in the middle of this cover.
A soft mixture of polymethyl-methacrylate (PMMA) resin was poured into the Teflon mold, which was placed on the surveyor’s base. Using the mold cover, the center of the acrylic block was measured. The mold cover was then removed while the mixture was still soft. Each tooth was mounted inside the acrylic blocks using a paralleling device Surveyor (Ney dental Surveyor, Anaheim CA, USA) to guarantee specimen centralization and alignment precisely parallel to the tooth’s long axis. After that, the tooth was left in place until the acrylic resin solidified. Finger pressure on the acrylic block’s base allowed the tooth specimen inside to be extracted from the mold. The specimens were then stored in distilled water to prevent dehydration of the teeth till the next step.
Thermo-mechanical cycling procedure
Using a Robota automated thermal cycle system (ROBOTA chewing simulator; ROBOTA Model ACH-09075DCT, LTD., Germany), all specimens underwent a thermocycling regimen of 10.000-cycle cycles to simulate one year of clinical service of composite restorations. 5 °C was the lowest temperature and 55 °C was the highest temperature. Each water bath had a dwell period of 25 s and a lag time of 10 s respectively for 60 s14. Meanwhile, the specimens were subjected to 500,000 mechanical chewing cycles representing long-term clinical wear, while steatite antagonists provide a standardized, enamel-like abrasive challenge to assess material durability under functional stress.
Fracture resistance test
A universal testing machine (Model LRX-plus; Lloyd Instruments Ltd., Fareham, UK) was used to assess the fracture resistance of each specimen group, including the positive control, negative control, and restored groups. After that, the specimens were compressed until either the restoration, the tooth, or both broke. A steel cylinder with a rounded end and a diameter of 5.7 mm was used to provide compressive force at a cross-head speed of 0.5 mm/min while aligned parallel to the tooth’s long axis. Both the buccal and lingual cusps’ occlusal inclined planes were in touch with the rounded end. Loads were measured in Newtons of force using Lloyd Instruments’ Nexygen-4.1 PC software. (Fig. 2)

A universal testing machine was used to assess the fracture resistance of each specimen group, A: specimen placed in universal testing machine, B: A steel cylinder with a rounded end and a diameter of 5.7 mm was used to provide compressive force at a cross-head speed of 0.5 mm/min while aligned parallel to the tooth’s long axis.
Failure mode analysis
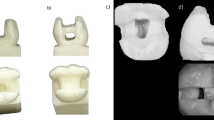
Fractured teeth were examined with USB digital microscope at 25X magnification and photographed using image analysis software (ViewTi Capture 1.3.0.1) (Fig. 3). The specimens’ mechanisms of failure were evaluated and classified as cohesive, adhesive, and mixed modes. Adhesive failures occurred at the interface between the resin and the tooth, whereas cohesive failures occurred within most of the tooth structure or restoration (without exposing any adhesive layer). A combination of cohesive and adhesive failure types was present in the mixed failure. By using an optical microscope to examine the fragmented specimens, the failure mode was found. Each group’s total number of specimen failure types was noted, and the percentages of each type were computed.

Assessment of fractured teeth with USB digital microscope at 25X magnification and photographed using image analysis software (ViewTi Capture 1.3.0.1).
Statistical analysis
Categorical data were presented as frequency and percentage values and were analyzed using chi-square test. Numerical data was represented as mean and standard deviation (SD) values. Shapiro-Wilk’s test was used to test for normality. The homogeneity of variances was tested using Levene’s test. Data were normally distributed. However, for intergroup comparison, the homogeneity assumption was violated, and it was analyzed using the Welch one-way ANOVA test followed by the Games-Howell post hoc test. For the associations with the mode of failure, all the assumptions were validated, and they were analyzed using one-way ANOVA followed by Tukey’s post hoc test. The significance level was set at p < 0.05 within all tests. Statistical analysis was performed with R statistical analysis software version 4.4.1 for Windows15.
Results
Summary statistics and intergroup comparison are presented in Table (2) and Figure (4). Results showed that there was a significant difference between different tested groups, with prepared teeth having significantly lower fracture resistance than sound teeth and samples restored with both restorative materials (p < 0.001). as presented in Table 2 the mean and standard deviation of Zirconfil was 1300.89 ± 204.19, followed by Neo Spectra composite that was 1073.45 ± 155.98, as for sound tooth it was 1160.38 ± 104.30. However, that of prepared tooth was 692.72 ± 60.96.Summary statistics and intergroup comparison for failure mode distribution are presented in Table (3) and Figures (5–8). Results showed that for samples restored with Neo Spectra, most samples had mixed failures (60%) and 40% adhesive failure. However, a higher percentage of samples restored with Zirconfil either had adhesive or cohesive failures, where the adhesive failure was 40%, cohesive failure was 40% and 20% mixed failure. The difference between both groups was not statistically significant (p = 0.077). All the associations between fracture resistance and failure modes presented in Table (4) and Figures (6) and (7) were not statistically significant. The results revealed that the mean and standard deviation for Zirconfil composite was (1351.29 ± 267.83) for cohesive failure, (1288.81 ± 144.91) for adhesive failure and (1224.22 ± 273.00) for mixed failure. while Neo Spectra composite recorded (999.15 ± 110.61) for adhesive failure and (1122.99 ± 170.57) for mixed failure. However, the overall association revealed (1143.98 ± 195.49) for adhesive failure, (1351.29 ± 267.83) for cohesive failure and (1148.29 ± 183.37) for mixed failure.

Bar chart showing mean and standard deviation values of fracture resistance (N).

Stacked bar chart showing failure mode distribution.

Bar chart showing mean and standard deviation values of fracture resistance (N) for different modes of failure (A).

Bar chart showing mean and standard deviation values of fracture resistance (N) for different modes of failure (B).

failure mode analysis, A: mixed failure NS, B: mixed ZF.
Discussion
The cusps in teeth with large Class II cavities may break due to tiredness of the fragile tooth structure caused by the growth of microcracks under continuous stacking, and occlusally applied burdens may force the cusps apart. Wide cavities filled with dental mixture have frequently resulted in cuspal cracks because the material is unable to support the weak cusp. One of the most crucial aspects of dental materials’ properties is their resistance to fractures. It is dependent on the material’s ability to withstand internal flaws that cause cracks to spread. These fissures may lead to large-scale filling fractures or little fractures of the repair margins. Since resin composites can reinforce the residual dental tissue by bonding to the tooth structure, teeth’s resistance to fracture has significantly improved since their introduction1.
The goal is to increase the composites’ strength and resilience to sustain mastication stresses while reducing polymerization shrinkage. However, one of the main issues with stress-bearing posterior restorations is the considerably increased brittleness and decreased fracture strength of the latest dental composites. Modern resin composites differ greatly in their mechanical qualities and filler features (size, volume, geometry, composition)4,5.
This experimental preclinical study was designed to compare the fracture resistance of premolar teeth with MOD cavities treated with diatomite Zirconia/Silica Filled Resin Composite versus Barium Glass/Yetterbium Fluoride Filled Resin Composite. The null hypothesis postulated in this in-vitro study was accepted. The results of the current study revealed that there was no statistical significance difference between the two tested materials and the sound tooth as positive control regarding the fracture resistance, while there was statistical significance difference when compared to prepared cavities as negative control. This denoted that both resin composite materials were able to reinforce the tooth structure and restore their biomechanical properties against functional stresses. This might be attributed to that the filler content and average filler particle sizes as well as the structural arrangement of the fillers have an impact on the mechanical behavior of resin composite materials, which rise with the quantity of inorganic material4,5. The filler percentages of the resin composite materials examined in this investigation were as follows, per the manufacturers: ZF 80% and NS: 78–80%. Additionally, the producer stated that NS contains non-agglomerated barium glass, ytterbium fluoride, and spherical, pre-polymerized fillers. On the other hand, ZF contains porous silica filler called diatomite, which is linked to zirconia.
Previous studies reported that when filler loading was substantial (over 60% weight%), Barium Glass showed an increase in flexural strength. When wrinkled mesoporous silica is utilized as a reinforcing material for dental resin composites, a similar trend has been seen4,5,6,7. Additionally, the compression strength increased, reaching a value of nearly 150 MPa at 40 weight%, thereby enabling more effective stress dissipation, improved the mechanical properties of the dental resin composites, decreased the number of fracture steps, and eliminated voids, indicating a better adherence between amorphous Barium glass particles and the polymeric matrix, which accounts for the improvement of all mechanical properties, permitted the formation of a loose or an intermediate percolated particle structure, respectively17.
This is consistent with Al-Jeaidi’s claim that composite materials’ fracture resistance might be increased by adding zirconia nanoparticles18. Because composite resins and dentin share a similar elastic modulus, using them is advised to ensure that the tooth is resistant to fracture18,19. Furthermore, the transformational toughening effect of zirconia inhibits the growth of cracks and gives composites strong mechanical characteristics20.ZF In a clinical setting, a greater degree of conversion and less polymerization shrinkage are made possible by the mechanical mating of the monomer inside the pores. The diatomite-based resin composite exhibited comparable mechanical characteristics and dentin bonding to conventional resin composites in terms of flexure strength and elastic modulus13.
Regarding ZF it was reported from the manufacturer that the main ingredients in the filler are diatomite and barium glass. Furthermore, the kind and amount of filler have an impact on the composites’ microhardness. In this particular composite, the inclusion of diatomite and zirconia nanohybrid particles was a factor in the composite’s high initial microhardness values. However, the diatomite-infused novel composite showed some vulnerability to solvent degradation for a maximum of 21 days before stabilizing. This condition most likely resulted from the plasticizing action, which causes the molecules in the polymer network to split and causes the microhardness to decrease. It is commonly known that chemical drinks and saliva in the mouth cavity can damage dental restorations. although in the present in-vitro study only the fracture resistance was tested. However, this factor is very critical and require further investigation to consider the different environmental stresse encountered by the material in the oral cavity. Additionally, it was reported that the matrix filler interface in the composite structure is negatively impacted by the pH and temperature fluctuations in those drinks. However, the microhardness stayed higher than 100 KHN. It’s possible that the diatomite-matrix interaction’s high degree of conversion and mechanical stability prevent a disastrous drop in microhardness brought on by the pH differences across solutions. The results presented here suggest that diatomite is an interesting particle to be used as filler in dental composites, as it improves degree of conversion, mechanical properties, and reduces chemical degradability to dietary solutions, even though this is an in vitro study focused on basic characterization of the composite. However, nothing is known about these composites’ surface characteristics, such as color stability, surface roughness, and gloss loss. To establish the distinctions between the diatomite-containing composites and those including other types of filler, more research can be done to assess these qualities. Thus, more research may be done to assess these characteristics and contrast composites containing diatomite with those having other fillers to establish their distinctions and forecast their clinical effectiveness13,18,19,20.
Regarding Failure mode analysis and its association to fracture resistance, the results of the current study revealed that for samples restored with Neo Spectra, most samples had mixed failures. However, a higher percentage of samples restored with Zirconfil either had adhesive or cohesive failures. The difference between both groups was not statistically significant (p = 0.077). Also all the associations between fracture resistance and failure modes were not statistically significant. In this attempt, specific consideration should be given to the established shrinkage stress. Because the composite resins are bounded by their attachment to the cavity walls during the curing process, the shrinkage causes the resins to distort, which causes stress. Nonetheless, the primary determinants of stress developments are not solely associated with the shrinkage of the composite polymerization; they are also linked to the development of the elastic modulus, the level of dentin adhesion, the cavity configuration factor (C-factor), cavity size, and compliance. Stress buildup during polymerization has the potential to weaken adhesive bonds, resulting in retention loss and/or the creation of marginal gaps. It should be underlined once more that low volumetric shrinkage does not always translate into low development of polymerization stress. Indeed, considering the role of the elastic modulus is necessary to successfully limit polymerization shrinkage stress21,22,23.
Many approaches to managing shrinking stress have been well documented and debated22. It has been determined that the main factors minimizing the development of stress are the modification of the resin matrix and filler phase. Polymerization shrinkage is mostly a resin matrix attribute, as evidenced by the literature, and as such, the composition of composite resins needs to be carefully examined. This is because polymerization shrinkage is dependent on the degree of monomer conversion. On the other hand, as the total amount of matrix is decreased, an increase in the filler fraction added to a composite resin’s matrix typically results in a decrease in the polymerization shrinkage of the resin22. In the current in-vitro study, the filler fraction by volume for the composite resins under investigation ranged from 80% Silica filler associated with zirconia and diatomite which is a porous silica with an average particle size: 15.8 μm and an average nanoparticle size: 20 nanometers in ZF, while for NS has 78–80% Spherical, pre-polymerized SphereTEC fillers with an average particle size of 15 μm of non-agglomerated barium glass and ytterbium fluoride. Despite of that both ZF and NS have almost similar amount of filler content, it was reported in previous study that the ZF group had the largest linear shrinkage. One could speculate that this result is due to the type of matrix and how the filler and matrix fraction are arranged in ZF23. this was explained as it might be attributed to high and low molecular weight monomers, such as TEGDMA, which increases the mobility of molecules during polymerization and, as a result, increases their degree of conversion and polymerization shrinkage, may be the cause of the rise in linear polymerization shrinkage in ZF. Furthermore, co-polymerizing Bis-GMA with UDMA and TEGDMA boosts conversion and produces dense, rigid, and strongly cross-linked polymer networks23,24. Furthermore, unlike traditional silica fillers, the diatomite used in this innovative composite resin has a permeable structure of nanometric pores. The firm claims that this architecture enables monomers to enter the pores of the diatomite particles, improving the mechanical and optical qualities of the resin composite intrinsically25. There are no studies examining the shrinkage caused by polymerization of this resin combination in the literature. However, in comparison to other resin composites, ZF was found to have a worse mechanical behavior in other experiments26,27.
Limitation of the study
As any laboratory study there are several inevitable limitations that might affect the clinical consideration as the humidity, temperature, acidity and oral stresses. However, all efforts were performed to minimize variables or operator bias. Moreover, this in-vitro study is very essential to accurately determine and properly interpret the mode of failure before clinical evaluation. However, future studies to assess how environmental factors such as pH, moisture, and temperature fluctuations might impact the behavior of these materials in vivo.
As this is an in-vitro study and because of the anatomical variances and the varied nature of tooth tissue, using actual teeth in experiments might be problematic, thus, to mimic clinical scenarios, the choice of a complete natural maxillary premolar appeared to be a reasonable one. To ensure consistent premolar size measurements and trustworthy data, the bucco-lingual dimensions of the chosen teeth at the point of maximal convexity in their crowns were within the 8.4–9.4 mm range16. Each tooth was mounted inside the acrylic block precisely parallel to its long axis using a paralleling device (surveyor) to ensure that the mechanical force would be delivered at the intended angulation to yield the most accurate results.
Every effort was made to replicate clinical situations and standardize the technique in this investigation. Each tooth’s mesial and distal cavities were prepared in the conventional box shape for cavities of moderate width (1/3 ICD) and wide width (1/2 ICD). Furthermore, a standard cavity preparation dimension would lead to a standard amount of polymerization for the composite restoration16.
As the thermally induced stresses resulting from the mismatch between the restorative material’s coefficient of thermal expansion and the natural tooth structure can cause gap formation and microleakage, thermocycling is a crucial procedure for testing the sealing ability of restorative material14. In order to replicate aging circumstances, specimens in this study underwent 10,000 thermal cycles at temperatures ranging from 5 °C to 55 °C, with a 25-second dwell period in each water bath. In previous studies by Özcan et al. and Rinastiti et al. showed that 5000 thermal cycles affect the bond strength of composites. On the other hand, Gale et al. suggested that 10,000 thermal cycles (considering the fact that 20 to 25 thermal cycles averagely occur per day) correspond to one year of clinical service of composite restorations28,29,30. The 500,000 cycles align with prior studies (Alsahafi et al., 2023) and represent long-term clinical wear, while steatite antagonists provide a standardized, enamel-like abrasive challenge to assess material durability under functional stress. [31]
As the cross-head speed is more sensitive in evaluating the fracture resistance of restored teeth, the fracture resistance test in this study was carried out by a universal testing machine at a cross head speed of 0.5 mm/min in accordance with the ISO standard recommendation for the rate of loading. A steel cylinder with a rounded end and a diameter of 5.7 mm, positioned parallel to the tooth’s long axis, was used to apply the compressive load. Beyond the margin restorations, the rounded end was contacting the occlusal inclined planes of the buccal and lingual cusps16.
Conclusions
Both tested materials; Diatomite Zirconia/Silica Filled Resin Composite versus Barium Glass/Yetterbium Fluoride Filled resin composite systems had similar biomechanical performance in term of fracture resistance compared to that of sound teeth. Comparing Diatomite Zirconia/Silica Filled Resin Composite versus Barium Glass/Yetterbium Fluoride Filled resin composite systems, both materials were able to reinforce and restore the strength properties of the tooth. Future clinical trials with long-term follow up are required, to evaluate the impact of thermal and mechanical aging on these materials.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- Bis-GMA:
-
bisphenol A glycidyl methacrylate
- bisEMA:
-
ethoxylatedbis-phenol A dimethacrylate
- bisEMA(6):
-
(2,2-bis[4-methacryloxypolyethoxyphenyl)propane
- DMA:
-
dimethacrylate
- UDMA:
-
urethane dimethacrylate
- TEGDMA:
-
triethylene glycol dimethacrylate
- PMMA:
-
poly methyl methacrylate
- ZF:
-
zirconfil
- NS:
-
Neospectra
References
Ausiello, P., Apicella, A., Davidson, C. L. & Rengo, S. 3D-finite element analyses of cusp movements in a human upper premolar, restored with adhesive resin-based composites. J Biomech. ;34(10):1269-77. (2001). https://doi.org/10.1016/s0021-9290(01)00098-7. PMID: 11522306.
Cramer, N. B., Stansbury, J. W. & Bowman, C. N. Recent advances and developments in composite dental restorative materials. J. Dent. Res. 90 (4), 402–416. https://doi.org/10.1177/0022034510381263 (2011).
Kiho Cho, G., Rajan, P., Farrar, L., Prentice, B. & Gangadhara Prusty Dental resin composites: A review on materials to product realizations, Composites Part B: Engineering 2022, 230, 109495. https://doi.org/10.1016/j.compositesb.2021.109495
Henry, A., Rodrأguez, W. M., Kriven, H. & Casanova Development of mechanical properties in dental resin composite: effect of filler size and filler aggregation state. Mater. Sci. Engineering:C2019, 101, 274–282, https://doi.org/10.1016/j.msec.2019.03.090
Randolph, L. D., Palin, W. M., Leloup, G. & Leprince, J. G. Filler characteristics of modern dental resin composites and their influence on physico-mechanical properties Dent. Mater 32, 1586–1599 (2016).
Aydınoğlu, A. & Yoruç, A. B. H. Effects of silane-modified fillers on properties of dental composite resin. Mater. Sci. Eng. C Mater. Biol. Appl. 79, 382–389. https://doi.org/10.1016/j.msec.2017.04.151 (2017). Epub 2017 Apr 27. PMID: 28629032.
Gurgan, S., Koc Vural, U. & Miletic, I. Comparison of mechanical and optical properties of a newly marketed universal composite resin with contemporary universal composite resins: an in vitro study. Microsc Res. Tech. 85 (3), 1171–1179. https://doi.org/10.1002/jemt.23985 (2022). Epub 2021 Nov 12. PMID: 34766666.
Vinagre, A. et al. Surface Roughness Evaluation of Resin Composites after Finishing and Polishing Using 3D-Profilometry. International Journal of Dentistry. 2023. 1–12. (2023). https://doi.org/10.1155/2023/4078788
Wang, R., Habib, E. & Zhu, X. X. Synthesis of wrinkled mesoporous silica and its reinforcing effect for dental resin composites. DentMater 33, 1139–1148 (2017).
Wu, X. et al. Reinforcement of dental resin composite via zirconium hydroxide coating and phosphate ester monomer conditioning of nano-zirconia fillers. J Mech Behav Biomed Mater. ;94:32–41. doi: 10.1016/j.jmbbm.2019.03.002. Epub 2019 Mar 4. PMID: 30856477. (2019).
Shekofteh, K. et al. Evaluation of physical/mechanical properties of an experimental dental composite modified with a zirconium-based metal-organic framework (MOF) as an innovative dental filler. Dent. Mater. 39 (9), 790–799 (2023). Epub 2023 Jul 14. PMID: 37455205.
Guo, G., Fan, Y., Zhang, J. F., Hagan, J. L. & Xu, X. Novel dental composites reinforced with zirconia-silica ceramic nanofibers. Dent. Mater. 28 (4), 360–368. https://doi.org/10.1016/j.dental.2011.11.006 (2012). Epub 2011 Dec 6. PMID: 22153326; PMCID: PMC3299838.
de Souza Araújo, I. et al. Diatomite filler for resin composites application – A new approach for materials improvement. Res. Soc. Dev. e268111637738. https://doi.org/10.33448/rsd-v11i16.37738 (2022). 11.
Yoshikawa, T., Morigami, M., Sadr, A. & Tagami, J. Effects of light curing method and resin composite composition on composite adaptation to the cavity wall. Dent. Mater. J. 33 (4), 499–503. https://doi.org/10.4012/dmj.2013-360 (2014). Epub 2014 Jul 2. PMID: 24988883.
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL (2024). https://www.R-project.org/
Al-Ibraheemi, Z. A., Abdullah, H. A., Jawad, N. A. & Haider, J. Assessing fracture resistance of restored premolars with novel composite materials: an in vitro study. Int. J. Dent. 2021, 5512708. https://doi.org/10.1155/2021/5512708 (2021). PMID: 34462637; PMCID: PMC8403034.
Ana Margarida dos Santos Melo. Aparecida Tharlla Leite de caldas, Josecia Da Nbrega dias, Boniek Castillo Dutra borges, Isauremi Vieira de assun£o, mechanical properties and dentin bonding of semi-direct restorations produced with a diatomite based resin composite. Int. J. Adhes. Adhes. 123, 103357. https://doi.org/10.1016/j.ijadhadh.2023.103357 (2023).
Al Jaedi, Z. Fracture resistance of endodontically treated teeth restored with zirconia filler containing composite core material and fibre posts. Pak J. Med. Sci. 32 (6), 1474–1478 (2016).
Ciavoi, G. et al. Base materials’ influence on fracture resistance of molars with MOD cavities. Materials 14 (18), 5242–5251 (2021).
Kupka, T., Karolus, M. & Fryc, M. The newest clinical version of glass-polyalkenoate restorative biomaterial infused with 3YTZP nanocrystals. J. App Biotech. Bioengin. 5 (6), 338–340 (2018).
Lins, R. et al. Polymerization shrinkage evaluation of restorative Resin-Based composites using fiber Bragg grating sensors. Polym. (Basel). 11 (5), 859. https://doi.org/10.3390/polym11050859 (2019). PMID: 31083498; PMCID: PMC6571745.
Meereis, C. T. W., Munchow, E. A., de Oliveira da Rosa, W. L., da Silva, A. F. & Piva, E. Polymerization shrinkage stress of resin-based dental materials: A systematic review and meta-analyses of composition strategies. J. Mech. Behav. Biomed. Mater. 82, 268–281. https://doi.org/10.1016/j.jmbbm.2018.03.019 (2018).
Goncalves, F., Kawano, Y. & Braga, R. R. Contraction stress related to composite inorganic content. Dent. Mater. 26, 704–709. https://doi.org/10.1016/j.dental.2010.03.015 (2010).
Goncalves, F., Azevedo, C. L., Ferracane, J. L. & Braga, R. R. BisGMA/TEGDMA ratio and filler content effects on shrinkage stress. Dent. Mater. 27, 520–526. https://doi.org/10.1016/j.dental.2011.01.007 (2011).
Zirconfill ®. Zirconfill Technical Specification. Technew; Rio de Janeiro, R. J., Brazil.
Carletti, T. et al. Microhardness Analysis of Different Composites After Chemical Degradation (Abstract); Proceedings of the XXIV Dental Meeting of Piracicaba IX International Dental Meeting; Unicamp, Campinas, Brazil. (2017).
Guarda, M. et al. Restorative Composite With Diatomite Fillers: Evaluation Of Mechanical Properties In Proceedings of XXIV Dental Meeting of Piracicaba IX International Dental Meeting, Unicamp, Campinas, Brazil, (2017).
Ozcan, M., Barbosa, S. H., Melo, R. M., Galhano, G. A. & Bottino, M. A. Effect of surface conditioning methods on the microtensile bond strength of resin composite to composite after aging conditions. Dent. Mater. 23, 1276–1282. https://doi.org/10.1016/j.dental.2006.11.007 (2007).
Rinastiti, M., Ozcan, M., Siswomihardjo, W. & Busscher, H. J. Effects of surface conditioning on repair bond strengths of non-aged and aged microhybrid, nanohybrid, and nanofilled composite resins. Clin. Oral Investig. 15, 625–633. https://doi.org/10.1007/s00784-010-0426-6 (2011).
Gale, M. S. et al. Thermal cycling procedures for laboratory testing of dental restorations. J Dent. ;27:89–99. 10.1016/s0300-5712(98)00037-2. 31., and 2023. Wear of bulk-fill composite resins after thermo-mechanical loading. Operative Dentistry, 48(4), pp.416–424. (1999).
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
R. R. O.O.T.: organized study samples, conducted methodology & wrote the first draft.A.H. I.: organized study samples, conducted methodology & wrote the manuscript. S. H. I.: conceptualization, conducted methodology & wrote and review the manuscript, approved the final draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
All authors read and approved the submission and publication.
Ethical approval and consent to participate
The study protocol of this experimental laboratory study was approved by the research ethical committee at the Faculty of Dentistry, October 6 University, Egypt (RECO6U/2-2024) at its meeting held on January 3,2024, that is in accordance with the declaration of Helsinki and its later modification.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Taha, R.O., Ibrahim, A.H. & Ibrahim, S.H. In vitro assessment of fracture resistance of premolar teeth restored with diatomite zirconia versus barium glass filled resin composite. Sci Rep 15, 32438 (2025). https://doi.org/10.1038/s41598-025-17036-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-17036-8
