
Abstract
Normothermic machine perfusion (NMP) of donated livers is emerging as a superior preservation technology versus static cold storage (SCS) for transplant, transforming a metabolically dormant organ to a functioning state that improves outcomes of marginal liver transplants. Mechanisms underlying improved NMP restoration of donation after brain death (DBD) and donation after circulatory death (DCD) livers remain incompletely defined. We tested the hypothesis that NMP would decrease transcripts encoding inflammatory mediators following both perfusion and transplant of DBD and DCD livers. Biopsy transcript expression profiles were determined from SCS DBD livers at pre-SCS preservation and transplant reperfusion and from benchmark and outside benchmark criteria DBD and DCD livers pre-NMP, after 6–7 h of NMP, and after transplant reperfusion. Compared to SCS livers, NMP programs converged transcript profiles of DCD and DBD livers, decreasing transplant reperfusion-induced inflammatory transcripts while increasing transcripts promoting wound healing and tissue repair processes, but did not obviate the high occurrence of adverse events in the outside benchmark DCD livers transplants.
Similar content being viewed by others

Introduction
Liver transplantation for end-stage liver disease patients is limited by discrepancies between organ need and supply where an estimated 15–20% of candidates die without receiving a liver transplant1,2. This problem is compounded by the 15–25% of donated livers that are discarded following assessment of poor quality and designation as marginal livers3,4,5. Static cold storage (SCS), the preservation modality that has been used for solid organs for more than 4 decades, is a key factor promoting liver graft injury after transplant, with marginal livers being particularly susceptible to this injury2,6,7,8. During SCS organs experience injury through two mechanisms: (1) direct cold injury on the cell membrane; and, (2) increased tissue ischemia from hypoxia. Following liver re-vascularization and reintroduction of blood and oxygen, the ischemic cells metabolize O2 to reactive oxygen species (ROS), which directly mediate tissue injury and trigger production of proinflammatory cytokines, leukocyte chemoattractants and expression of integrin and other adhesion molecule expression that promote recipient leukocyte interaction with graft cells and infiltration into the graft9,10,11. The increased magnitude of ischemia-reperfusion injury (IRI) generated during transplant reperfusion of cold stored grafts is a critical risk factor for early injury, delayed graft function, increased donor-reactive immune responses, biliary complications, and poorer long-term outcomes.
Normothermic machine perfusion (NMP) has been developed as a potentially superior preservation technology for liver transplants compared to SCS. Organ preservation by warm oxygenated perfusion is based on the rationale that hypoxia and hyperthermic injury is prevented and the delivery of oxygen and nutrients as well as maintenance of physiologic temperature, promote healthy cell metabolism during preservation9,12,13,14. In contrast to SCS, NMP transforms a metabolically dormant and continuously injured liver into a functioning organ and offers three advantages over SCS: (1) better preservation that allows transplant of many livers that would normally be discarded; (2) a tool for testing liver injury and function before transplantation; and, (3) decreases in the intensity of IRI following transplant reperfusion. NMP also offers an opportunity to provide critical information on organ viability during and after perfusion.9,11) During the past 8 years, our team has pioneered NMP technology in liver transplantation using an institutionally developed device15. Initial clinical studies perfused 21 livers for 200–500 min followed by successful transplantation and presented much better hemodynamics and reduced graft injury after reperfusion compared to SCS preserved controls15.
Studies of liver grafts subjected to either SCS or NMP preservation indicate decreased early post-transplant injury in NMP livers7,12. Microarray analyses of biopsy RNA before liver transplantation versus after transplantation indicated decreased expression of proinflammatory genes associated with IRI following transplantation of NMP vs. SCS preserved grafts16. Other studies have used RNA sequencing to compare NMP-induced changes in liver transcripts17,18,19. These studies have begun to elucidate molecular changes induced after transplantation of SCS and NMP preserved grafts. To gain further mechanistic insights underlying the improvements in liver grafts subjected to NMP, we utilized the multiplex NanoString nCounter platform to identify transcript profiles expressed in liver biopsies to ask: (1) does NMP decrease or change the inflammatory transcript landscape of graft tissue following perfusion and then at transplant; and, (2) do standard benchmark criteria and beyond benchmark criteria donation after brain death (DBD) and donation after circulatory death (DCD) livers respond differently to NMP, both at the end of perfusion and following transplant? Overall, the results provide a comprehensive dissection of the effects of NMP on liver graft status and insights into the inflammatory and regulatory changes to the graft tissue of DBD and DCD livers after NMP and transplantation.
Methods
Biopsy samples
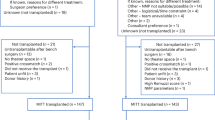
Liver biopsy samples were collected from 47 subjects transplanted between February 2018 and June 2022. Subject demographics are shown in Table 1. Thirteen livers were subjected to SCS prior to transplantation (control) and 34 were treated with NMP. Livers were stratified by donor type and risk factors20,21. Benchmark criteria were defined as follow for all primary liver transplants with donation after brain death (DBD) or donation after circulatory death (DCD) grafts: young donors, low meld recipients and low Balance of Risk (BAR) recipients up to a BAR score of 9 points, low meld recipients with up to a meld of 20 points and, no acute liver failure, ICU admission, or ventilation or renal replacement therapy at transplantation. Specific to DCD grafts, the donor warm ischemia time was short and not more than 15 min asystolic and 30 min total donor warm ischemia time and cold storage kept within 6 h—with no more than a 7 minute difference for benchmark and outside benchmark livers. Liver transplant cases outside benchmark criteria were those with donor and/or recipient risk factors outside the above-described benchmark criteria, including cases with more risk for elevated reperfusion injury due to a presumed inferior liver quality. The 13 control livers subjected to SCS preservation were from benchmark criterion DBD donors. Twenty NMP-treated livers were from benchmark criteria donors (10 DBD and 10 DCD) and 14 were from outside benchmark criteria donors (6 DBD and 8 DCD).
Wedge biopsies were collected at two or three timepoints as illustrated in Fig. 1. A pre-SCS/NMP sample was collected from both groups after procurement prior to NMP or SCS preservation. For NMP livers a biopsy was collected at the end of machine perfusion (post-NMP). Reperfusion biopsies in both groups were collected approximately 90 min after transplant reperfusion of the graft, prior to closure. Biopsy samples were placed immediately into RNALater (ThermoFisher Scientific) and frozen at -80 °C until processing.

Blue arrows indicate sample collection points. (a) Biopsy samples from 34 livers treated with normothermic machine perfusion (NMP) were collected at three timepoints: pre-SCS or NMP preservation, before the beginning of machine perfusion; post-NMP, after completion of machine perfusion; and reperfusion, after transplantation into the recipient, just before closure. Twenty of the NMP livers were from benchmark criterion donors, 10 donation after brain death (DBD) and 10 donation after cardiac death (DCD). Fourteen NMP livers were from outside benchmark criterion donors, 6 DBD and 8 DCD. (b) Biopsy samples from 13 control livers were collected at two timepoints: baseline (pre), after dissection, while the liver was on the back table in the operating room; and reperfusion, after transplantation into the recipient, before closure. All of the control livers were from benchmark criterion DBD donors. Abbreviations: DBD, donation after brain death; DCD, donation after cardiac death; NMP, normothermic machine perfusion.
Informed consent was obtained from all subjects. The performed studies adhere to the Ethical Principles for Medical Research Involving Human Subjects outlined in the Declarations of Helsinki Istanbul and were approved by the Cleveland Clinic Institutional Review Board.
Normothermic machine perfusion
NMP was performed as previously described by Liu and colleagues using our institutionally developed perfusion device15. The protocols included off-the-shelf cardiopulmonary bypass equipment, a customized organ basin, and a plasma-packed red blood cell-based perfusion solution.
RNA isolation and NanoString nCounter analysis
RNA was isolated using the Qiagen RNeasy Mini kit (Germantown, MD) and gene expression measured with the NanoString PanCancer Immune Profiling codeset (Seattle, WA). The Rosalind platform (https://rosalind.bio/) was used for preliminary data analysis including quality control, normalization of raw counts, and determination of differentially expressed genes. Gene expression changes of fold-change ≥ 2 or ≤ -2 and having p value ≤ 0.05 were considered significant. Gene set scores were calculated for each sample by taking the sum of the mean-subtracted log2 normalized expression levels of each gene in the heatmap. Enrichr (https://maayanlab.cloud/Enrichr/) was used for pathway analysis.
Statistics
Continuous variables were reported as median (interquartile range) and p values determined using Students’ t test or Mann-Whitney U test, according to distribution normality and variance equality. Categorical variables were presented as counts and percentages and analysed using Fisher exact test. Statistical analysis was done using GraphPad Prism Version 10. PCA plots were created in R.
Results
Biopsy transcript expression by DBD and DCD livers at pre-SCS/NMP
Before determining the impact of NMP on transcript profiles expressed by DBD and DCD livers following transplant, it was necessary to establish the profiles at the first biopsy time point as pre-SCS/NMP. Biopsies were obtained from all livers received for transplant prior to initiation of NMP or SCS preservation and the pre-SCS/NMP transcript profiles of the DBD and DCD livers were compared. There was a marked increase in 26 inflammatory transcripts and a decrease in 4 transcripts in the pre-preserved DBD vs. DCD livers (Fig. 2a). Increased transcripts in DBD vs. DCD livers pre-SCS/NMP included those promoting inflammation, the recruitment of lymphocytes, myeloid cells and dendritic cells (IL1RN, CCL2, CCL20, CXCL10, TREM1) and cell adhesion (THBS1, TNFRSF12A, LIF) and the decreased transcripts were primarily involved with promoting inflammation (C reactive protein and TNFSF14) and directing the trafficking of resident dendritic cells and naïve T cells (CCL19) (Fig. 2b). The transcript profiles of the control, pre-SCS liver biopsies were compared to those of the 4 groups preserved with NMP, there was little difference with the benchmark DBD, but the outside benchmark DBD and DCD as well as the benchmark DCD livers had increased expression of 14 transcripts encoding inflammatory mediators (Supplementary Fig. 1).

Baseline gene expression reveals increased inflammatory transcript profiles in DBD versus DCD livers. (a) Gene expression was measured by NanoString in 16 DBD and 18 DCD livers prior to machine perfusion. Differently expressed genes were defined by log2 fold-change ≥ 1 or ≤ -1 and p value ≤ 0.05. (a) Heatmap indicating higher expression of 26 genes and decreased expression of 4 genes in the DBD livers when compared to the DCD livers at baseline. (b) volcano plot showing the differently expressed genes. The horizontal dotted line on the volcano plot is p value = 0.05. The two vertical dotted lines are log2 fold-change − 1 and 1. Red dots indicate DEGs with increased expression in DBD livers compared with DCD livers and blue dots indicate DEGs with decreased expression in DBD livers. Abbreviations: DBD, donation after brain death; DCD, donation after cardiac death; NMP, normothermic machine perfusion.
Transcript changes following transplant reperfusion of SCS versus NMP preserved DBD livers
The inflammatory transcript profiles in the DBD livers from pre-SCS/NMP were compared to those expressed after transplant reperfusion in the recipient. For DBD livers subjected to SCS, 60 transcripts were increased from pre-SCS/NMP to transplant reperfusion (Fig. 3a and b). Increased transcripts included those involved in neutrophil trafficking, cell adhesion and promotion of inflammation. The heat map indicated that the increased transcripts induced by transplant reperfusion of the SCS DBD livers separated into 2 clusters with one cluster expressing lower increases of the transcripts and the other expressing markedly higher increases (Fig. 3a). When gene set scores (GSS) were determined for each sample, the GSS placed the samples into one of the two clusters with one cluster expressing low levels of the inflammatory genes (mean GSS = 17.4) and a second cluster expressing almost five-fold higher levels of the transcripts (mean GSS = 82.6). Of the 10 most highly increased transcripts during transplant reperfusion of the SCS preserved DBD livers, a high increase in chemoattractant CCL4 transcripts was unique to the SCS preserved DBD livers and the other 9 increased transcripts were shared with those induced during transplant reperfusion of NMP preserved benchmark criteria DBD livers (Fig. 3b). Liver grafts from the higher cluster had significant increases in peak AST levels (1,354 vs. 385 U/L, p = 0.019) and bilirubin (2.4 vs. 1.3 mg/dl, p = 0.025) production and the liver with the highest AST level and bilirubin experienced early allograft dysfunction whereas one liver graft from the lower cluster experienced an acute rejection episode (Table 2).

Transplant reperfusion induces different gene expression changes from baseline to reperfusion in control SCS and NMP conditioned livers. (a) Heatmap indicating gene expression changes between baseline and reperfusion biopsies measured by NanoString in 13 control SCS conditioned benchmark criterion DBD livers and 10 NMP benchmark criterion DBD livers. DEGs were defined by log2 fold-change ≥ 1 or ≤ -1 and p value ≤ 0.05 with 60 DEGs with increased expression after reperfusion in control SCS livers. (b) Volcano plot illustrates the 27 DEGs that were unique to the control SCS group in red and 33 shared DEGs upregulated in both control SCS and NMP conditioned benchmark criterion DBD livers in blue. The horizontal dotted line on each volcano plot is p value = 0.05. The two vertical dotted lines are log2 fold-change − 1 and 1. (c) Heatmap showing the 56 genes with increased expression and 4 genes with decreased expression after reperfusion in NMP benchmark criterion DBD livers. (d) Volcano plot illustrates in red 23 genes increased and 4 genes decreased only in NMP livers, and in blue the 33 genes increased in both control and NMP benchmark criterion DBD livers. Abbreviations: BM, benchmark criterion; DBD, donation after brain death; DEG, differently expressed gene; NMP, normothermic machine perfusion; SCS, static cold storage.
Analysis of transplant reperfusion-induced vs. pre-NMP transcripts in benchmark criterion DBD grafts indicated increases of 56 and decreases of 4 transcripts (Fig. 3c), with 33 of the 56 increased transcripts shared with the SCS preserved DBD livers (Fig. 3d), including those involved in encoding mediators of cell trafficking and adhesion, promotion of tissue inflammation, platelet aggregation, apoptosis and regulation of innate and adaptive immune responses. Transplant reperfusion of the NMP preserved benchmark DBD livers induced 23 unique transcripts not observed in SCS preserved DBD livers, including transcripts encoding components involved with wound healing, intracellular activation (cathepsin L, ISG20 and SMAD3), and cell adhesion and extracellular vesicle generation (ITGB3 and CD9). As observed for SCS preserved DBD livers, transplant reperfusion-induced transcript profiles of NMP-preserved benchmark criteria DBD livers separated into two clusters with one cluster of 4 samples expressing higher increases of inflammatory genes vs. the pre-NMP levels (mean GSS = 70.6) than the other cluster of 6 samples (mean GSS = 17.4). Peak AST and ALT levels were elevated more than two-fold in recipients with the cluster containing the higher transcript levels (1632 vs., 582 U/L, p = 0.04; and 393 vs. 185 mg/dl, p = 0.67). Notably, these NMP preserved liver grafts had significantly longer total preservation time (899 vs. 530 min, p = 0.015) and had two incidences of early graft dysfunction and one episode of acute rejection (Table 2).
Impact of NMP on transplant reperfusion induced transcript profiles in benchmark DBD livers
The use of benchmark criteria DBD livers preserved with either SCS or NMP allowed a direct assessment of the impact of NMP on transcript profile changes induced by transplant reperfusion in individual grafts. When the transcripts expressed during transplant reperfusion in these DBD livers were compared there was an increase of 10 transcripts and a decrease in 25 transcripts in livers preserved with NMP vs. SCS (Supplemental Fig. 2). The induced transcripts in the NMP preserved livers included those involved in regulation of inflammation expressed by immune cells and/or liver epithelial cells, including HAVCR2, MGFE8, SMAD3, LGALS3, and ITGB3. The decreased transcripts included those involved in acute phase inflammation, leukocyte chemotaxis, promotion of cell adhesion, and activation of innate immune cells.
When differentially expressed genes (DEGs) generated post-transplant reperfusion vs. pre-SCS/NMP in the SCS- and NMP-preserved benchmark criteria DBD livers were compared, there were 27 DEGs unique to the SCS preserved livers that were comprised of many proinflammatory genes and 23 DEGs unique to the livers preserved with NMP that were comprised of genes involved in attenuation of inflammation and promoting wound healing and tissue repair (Fig. 4a). In addition, 33 DEGs were shared between the two groups of transplanted livers that were comprised mostly of transcripts encoding proinflammatory and leukocyte recruitment factors. These results were supported by pathway analysis of the transcript profiles induced by transplant reperfusion of NMP preserved livers indicating increased expression of transcripts regulating innate and adaptive immune responses and wound healing, including matrix organization (Fig. 4b), whereas reperfusion of SCS preserved DBD livers increased expression of transcripts promoting proinflammatory cytokine production and innate immune recruitment to mediate allograft inflammation. Overall, the results indicated that NMP preservation of benchmark criteria DBD livers promoted expression of transcripts encoding mediators resolving inflammation and promoting tissue repair, but without obviating expression of all transcripts encoding inflammatory mediators.

Wound healing and anti-inflammatory gene sets are increased between baseline and reperfusion in NMP-conditioned livers but not control livers. (a) Gene expression changes between baseline and reperfusion were determined for 13 control and 10 NMP benchmark criterion DBD livers. The Venn diagram indicates the numbers of shared and unique DEGs with increased expression at the time of reperfusion compared with baseline. GO biological pathways that are unique to the control group, unique to the NMP group, and common to both groups are listed. (b) Gene expression at the time of reperfusion was measured by NanoString in 13 control and 10 NMP benchmark criterion DBD livers. Differently expressed genes were defined by log2 fold-change ≥ 1 or ≤ -1 and p value ≤ 0.05. Ten genes were increased in NMP livers relative to control, SCS livers and 25 genes were decreased (see supplemental Fig. 1). Pathway analysis was done in ENRICHR and the most highly significant GO biological pathways were determined. GO biological pathways increased in control, SCS livers are shown in red and those increased in NMP livers are shown in blue. Bars represent the Benjamini-Hochberg adjusted p value. Abbreviations: DBD, donation after brain death; DCD, donation after cardiac death; DEG, differently expressed gene; GO, gene ontology; NMP, normothermic machine perfusion; SCS, static cold storage.
The transplant reperfusion-induced transcript changes compared to pre- NMP were also determined in outside benchmark criteria DBD livers that had been preserved with NMP. Following transplant there was an increase in 21 and a decrease in 9 transcripts when compared to the transcripts expressed prior to preservation (Supplemental Fig. 3a). Unlike the two clusters of transcripts increased during transplant reperfusion of benchmark DBD grafts subjected to preservation with either SCS or NMP, transplant reperfusion-induced transcripts of NMP preserved outside benchmark criteria DBD livers did not separate into clusters and included 21 increased transcripts with most encoding mediators promoting inflammation, neutrophil recruitment, activation and cell adhesion and two mediating down-modulation of inflammation (Supplemental Fig. 3a and 3b). There were also 9 decreased transcripts encoding mediators promoting inflammation. When compared with the transplant reperfusion-induced transcript changes vs. pre- NMP of the benchmark DBD grafts, the outside benchmark livers increased expression of 14 shared and 7 unique transcripts and decreased 3 shared and 6 unique transcripts (Supplemental Fig. 3b and 3c). The 6 grafts of the outside benchmark criteria livers had moderate elevations in peak AST levels when compared to those of the high transcript level cluster of the benchmark DBD livers (median 1758 vs. 1632 U/L), but the ALT levels were similar (median 360 vs. 393 mg/dl), and there were 2 instances of early allograft dysfunction and 2 episodes of acute rejection (Table 2).
Transcript changes following transplant of DCD livers preserved with NMP
The transcript profiles in the DCD livers from pre-NMP to post-transplant reperfusion were also compared. In benchmark criteria DCD livers 95 transcripts were increased and 9 decreased whereas in outside benchmark DCD livers 85 transcripts were increased and 10 decreased (Supplemental Fig. 4a and 4b). Seventy-five of the increased genes were shared between benchmark and outside benchmark criterion donors (Supplemental Fig. 4c), representing GO Biological Process gene sets including granulocyte and neutrophil chemotaxis, cytokine-mediated signaling, and inflammatory response. Whereas 30.33% (3 of 10) of benchmark criteria DCD liver grafts experienced EAD and only 10% (1 of 10) had an acute rejection, 62.5% (5 of 8) of outside benchmark criteria DCD livers had EAD and 37.5% had an acute rejection (Table 2). This was consistent with the histopathology observed in the biopsies obtained at the transplant reperfusion point (i.e. approximately 90 min after initiation of reperfusion) where outside benchmark DCD grafts had patchy hepatocyte necrosis in 5 of 8 grafts and a marked increase in overall tissue injury when compared to the benchmark and beyond benchmark DBD and the benchmark DCD which had only moderate observable injury (Supplemental Fig. 5).
Differential transcript changes in DBD and DCD livers from pre- to post-NMP
It was unclear to what extent the transcriptional changes observed from pre-NMP to post-transplant reperfusion would be observed from pre-NMP to the time NMP was terminated. Differences in transcript expression profiles from pre-NMP to post-NMP were determined in benchmark and outside benchmark criteria DBD and DCD livers (Supplemental Fig. 6a and 6b). There were 30 unique DEGs increased in the benchmark criteria vs. outside benchmark criteria DBD livers with very few (i.e. 3) shared between the two. In contrast, many unique and shared DEGs were observed post-NMP in the benchmark and outside benchmark criteria DCD livers, including shared transcripts encoding mediators of wound healing and negative regulation of inflammation that were not shared between the two groups of DBD livers (Supplemental Table 1). When comparing NMP-induced transcripts in DBD vs. DCD livers, both the benchmark and outside benchmark criteria DCD livers had many more uniquely increased transcripts than their DBD counterparts, (Supplemental Fig. 6c and 6d), indicating NMP had the greatest impact in increasing DEGs in the benchmark and beyond benchmark criteria DCD vs. DBD livers.
Different transcript profile changes from NMP to transplant reperfusion in DBD and DCD livers
To further determine the impact of NMP on transplant reperfusion-induced inflammation in liver grafts, transcript profiles induced at reperfusion were compared with those expressed at the end of NMP in benchmark and outside benchmark DBD and DCD livers. The results indicated that the primary change in all the liver groups was transplant reperfusion-induced increases in transcripts without any noticeable decreases and these increases were more prominent in the benchmark and outside benchmark criteria DCD when compared to the DBD livers (Fig. 5a and b). In benchmark criterion livers, 11 DEGs were shared between DBD and DCD livers but an additional 17 were unique to transplant reperfusion of the DCD livers vs. 5 for the DBD livers. Similarly, outside benchmark criteria DBD and DCD livers had increases in 8 shared DEGs but an additional 10 were unique to the DCD livers vs. 7 for the DBD livers (Fig. 5c). Whereas 8 of the 12 transcripts encoding mediators attenuating inflammation and promoting wound healing were shared by at least 3 of the 4 NMP liver groups, only 2 of the 28 inflammation promoting transcripts was shared by three or more of the liver groups preserved with NMP (Supplementary Table 2). Moreover, transplant reperfusion of SCS preserved DBD livers also increased the same 9 anti-inflammatory/wound healing transcripts and all but 7 of the 28 inflammation promoting transcripts observed in the NMP preserved DBD and DCD livers (Supplementary Table 2). Overall, the results indicate that NMP preservation primes the DBD and DCD livers to respond to transplant reperfusion by increasing many transcripts associated with resolution of inflammation and wound healing whereas the expression of inflammation promoting transcripts was diffusely expressed among the 4 groups of livers.

Inflammatory gene expression has greater increases in post-NMP and transplant reperfusion biopsies from DCD livers versus DBD livers. Gene expression changes between post-NMP and transplant reperfusion were determined by NanoString for liver biopsy samples from each of the four donor groups: 10 BM DBD, 10 BM DCD, 6 OSBM DBD, and 8 OSBM DCD. DEGs were defined by log2 fold-change ≥ 1 or ≤ -1 and p value ≤ 0.05. (a, b) Volcano plots show unique and shared inflammatory DEGs in solid and open red, respectively, and unique and shared wound healing and anti-inflammatory DEGs in solid and open blue. The horizontal dotted line on each volcano plot is p value = 0.05. The two vertical dotted lines are log2 fold-change − 1 and 1. (c) Venn diagrams indicate numbers of shared and unique DEGs when comparing DBD to DCD livers. Abbreviations: BM, benchmark criterion; DBD, donation after brain death; DCD, donation after cardiac death; DEG, differently expressed gene; NMP, normothermic machine perfusion; OSBM, outside benchmark criterion.
Transplant reperfusion induced similar transcript profiles in NMP preserved DBD and DCD livers that are distinct from SCS preserved livers
The transplant reperfusion-induced transcripts expressed by NMP preserved benchmark and outside benchmark criteria DBD and DCD livers were directly compared with SCS preserved DBD livers. Transplant reperfusion of the SCS preserved livers clearly increased a distinct set of transcripts encoding inflammatory mediators when compared to the livers preserved with NMP (Fig. 6a). Conversely, transcripts encoding mediators attenuating inflammation and promoting wound healing were increased during transplant reperfusion in most NMP preserved livers when compared with SCS preserved livers, although several of the NMP preserved benchmark DBD livers also expressed low levels of these transcripts. In spite of the low expression levels of the transcripts involved in decreasing inflammation and promoting wound healing, this set of NMP preserved benchmark DBD livers had low levels of recipient serum indicators of graft injury (ALT, AST and ALP) at day 7 post-transplant, suggesting the NMP associated expression of other mediators attenuating transplant reperfusion-induced inflammation.

At the time of reperfusion, SCS and NMP livers express distinct transcript profiles. Gene expression at the time of reperfusion was measured by NanoString in 13 livers from control BM DBD donors and all 34 NMP livers. DEGs were defined by log2 fold-change ≥ 1 or ≤ -1 and p value ≤ 0.05. (a) The heatmap illustrates the 12 genes with increased expression in control livers and 16 genes with increased expression in NMP livers. (b) The PCA plot shows separation between control SCS and NMP livers but not between the 4 NMP groups. Abbreviations: BM, benchmark criterion; DBD, donation after brain death; DCD, donation after cardiac death; NMP, normothermic machine perfusion; PCA, principal component analysis; OSBM, outside benchmark criterion; SCS, static cold storage.
The analyses were extended by comparing the transcript profiles expressed during transcript reperfusion in DBD and DCD livers preserved with SCS or NMP and performing multidimensional scaling of all the samples. The SCS and all of the NMP preserved grafts clustered separately and there was no distinction between the different NMP preserved liver grafts (Fig. 6b). The separation of the SCS and NMP preserved clusters was further reflected by the differences in biological signaling pathways where again transplant reperfusion of SCS preservation skewed the livers to inflammatory signaling pathways and NMP preserved skewed the livers to wound healing and tissue repair pathways (Supplementary Table 3). Collectively, these results indicate the convergence of transcript expression in DBD and DCD livers after NMP preservation and after graft reperfusion in the recipient.
Discussion
The increasing use of machine perfusion has led to decreases in donor liver discard with a concomitant two-fold increase in the number of livers transplanted7,12,22,23. In our early experience more than 70% of livers discarded from other centers were successfully transplanted after preservation with NMP using an institutionally developed perfusion device24. This initial report was extended in the current study by determining transcript profile changes in livers subjected to SCS or NMP preservation in biopsies taken prior to pre-SCS/NMP preservation, following NMP preservation, and then after transplant reperfusion in the patients, and comparing the transcript changes at the three time points in benchmark and outside benchmark DBD and DCD livers. Briefly, the results indicated that: pre-SCS/NMP transcript profiles of DBD and DCD livers are distinct, NMP preservation promotes decreases in transcripts encoding mediators of inflammation and increases transcripts mediating wound healing and tissue repair vs. SCS preserved grafts, these transcriptional changes are more marked in DCD livers, both at the end of NMP and following transplant reperfusion, and NMP preservation converges the transcript profiles expressed by benchmark and beyond benchmark DBD and DCD livers after transplant reperfusion.
Studies from other centers have documented transcript profiles in livers procured for transplant to compare transcript changes in either DBD or DCD livers, after NMP or SCS preservation, and/or after transplant reperfusion. An early study used microarray analyses to compare transcript profiles of DBD livers preserved with SCS or NMP before and after preservation and reported that NMP upregulated transcripts involved in tissue regeneration whereas increased induction of transcripts encoding inflammatory mediators was observed in SCS preserved livers, but the impact of SCS vs. NMP preservation on transcript profiles following transplant was not assessed16. Another study used single cell RNA sequencing of cells isolated from biopsies of 6 DCD livers before and at two time points during NMP and reported increased transcripts associated with the appearance innate immune cell activation with perfusion time19.
To extend the range of the previous studies we documented transcripts in biopsies from both DBD and DCD livers to compare transcript profile changes from pre-SCS/NMP to NMP and from post-NMP to post-transplant reperfusion. The biopsy transcripts were quantitated using the NanoString nCounter platform and the Pan Cancer Immunology code set that has 770 probes, limiting the range of the profiling when compared to the RNA array or sequencing used in the 4 other studies. Although the range is not as extensive as RNA sequencing, use of this code set covers most of the major transcripts encoding mediators of inflammation and tissue injury, wound healing and tissue repair, and the phenotypic markers of specific cells involved in these processes. This approach revealed a marked increase in transcripts encoding mediators promoting inflammation in DBD livers when compared to DCD livers at pre-SCS/NMP, with most of the increased transcripts encoding mechanisms promoting apoptosis and tissue inflammation. These differences in transcript profiles at pre-SCS/NMP are not surprising considering the impact of brain death on spontaneous release of cytokines and other components mediating systemic inflammation25,26,27. It is also worth noting that the different donor warm ischemic times the DCD livers were subjected to during procurement, 27 min or less, did not impact the transcript profiles expressed pre-SCS/NMP that included 3 outside benchmark livers expressing the highest levels of proinflammatory transcripts.
Transplant reperfusion of benchmark DBD livers subjected to SCS or NMP preservation induced low and high transcript expression sample clusters with increases as much as 4-fold in the high vs. low expression cluster although there was no difference in the expression of the decreased transcripts between the two clusters. This transcript expression clustering was not reported in studies using RNA microarray or sequencing analyses of NMP preserved livers. We found no liver graft or recipient characteristics that would account for this clear separation within the NMP preserved DBD liver graft group with the exception that grafts with the higher expression cluster had longer total preservation time than those with the lower expression cluster. Furthermore, there was a clear difference in graft outcomes in that NMP-preserved benchmark criteria DBD livers expressing the higher transcript expression cluster had increases of inflammatory genes after transplant reperfusion, elevated peak AST and ALT levels, and had the two incidences of early graft dysfunction and one episode of acute rejection when compared with the DBD livers expressing the lower increases. Livers preserved with SCS also separated into low and high transcript expression clusters with the higher cluster having increased peak AST and bilirubin levels and one experiencing early allograft dysfunction when compared to livers with the lower transcript expression cluster. Given that EAD is a measure of post-transplant liver enzymes associated with graft inflammation, it is internally validating that the identified transcripts correlate with clinical inflammatory markers.
When tested at the end of perfusion, NMP induced many transcripts encoding mediators resolving inflammation and promoting wound healing and tissue repair in benchmark and beyond benchmark criterion DBD and DCD livers. Transplant reperfusion of these livers decreased several of these transcripts, but also induced expression of other transcripts encoding mediators of these processes. The primary change in all the liver groups preserved with NMP was transplant reperfusion-induced increases in transcripts without any noticeable decreases and these increases were more prominent in the DCD livers when compared to the DBD livers. These results indicate a progression of gene expression that is initiated during NMP but is not stable following initiation of transplant reperfusion. The results also raise the possibility that the transcript profiles observed following NMP evolve with time after transplant reperfusion with subsequent changes influenced by the innate cellular and molecular components recruited to the liver graft.
While there was a convergence of transcript profiles of NMP preserved standard criterion and beyond benchmark criteria livers following transplant reperfusion, beyond benchmark criteria DCD livers had greater histopathological indicated injury and a higher rate of post-transplant complications than livers in the other three NMP preservation groups. We attempted to identify the expression of specific transcripts following NMP or transplant reperfusion that were indicative of EAD or acute rejection development in DBD and/or benchmark criteria DCD livers but did not find any associated transcripts predictive of these outcomes. The increased incidence of post-transplant complications observed in outside benchmark criteria DCD livers is consistent with published literature and is at least partially due to biliary complications resulting from ischemic-induced cholangiopathy28,29,30,31,32. Despite the convergence of transcript profiles with livers from DCD livers with the other 2 NMP preserved liver groups, the results implicate changes in transcriptional profiles that appear at later times after transplant reperfusion of beyond benchmark DCD livers that impact graft injury and function in these grafts.
Several limitations of this study are acknowledged and worth noting. These include the low number of livers in each of the 5 groups; however, within each group the transcript profiles of the individual samples appear very similar, including those two groups where the samples broke into high and low expression clusters. This study is also the largest cohort assessing gene expression of NMP vs. SCS livers yet reported. The current study also does not include biopsy samples taken at the end of the SCS preservation preservation for the DBD livers that could be compared to the DBD and DCD livers at the end of NMP. It is likely that despite the SCS preservation that there is some change in expression of transcripts. Studies from the King’s College Hospital group have reported different transcript expression profiles between DBD livers after SCS vs. NMP perfusion and further transcriptional changes between the two groups of livers following transplant reperfusion16. Unlike the current study, transcriptional profiles before the start of preservation were not assessed and the current studies indicate the high expression of inflammatory transcripts in DBD livers at this time point that eventually separated into 2 distinct clusters when compared to DCD livers. The distinct transcript profiles expressed by NMP vs. SCS livers during transplant reperfusion and the convergence of transcripts in NMP preserved livers despite the origin of the livers are consistent with the RNA sequencing results indicating marked transcriptional differences following preservation in DBD livers subjected to SCS vs. NMP. It is important to also note that these studies utilized a home-built perfusion apparatus used in several previous reports from our group24. The importance of this preservation technology in evaluating the suitability of DCD and beyond benchmark DCD livers for transplant has been clinically validated and has compelled the development of several commercially available perfusion devices that are now being used at many centers, including ours. It is also important to note that the impact of hypo- vs. normo-thermic perfusion as well as oxygenated vs. non-oxygenated perfusate is under current investigation and it will be important to perform similar studies to the current study to determine the impact of the perfusion strategy on the response of DBD and DCD livers to the perfusion modality as well as to subsequent transplant reperfusion33,34,35,36,37.
The results of this study indicate that NMP preservation decreases expression of transcripts encoding mediators promoting inflammation and increases transcripts encoding mediators promoting resolution of inflammation and tissue repair when compared to transcript profiles expressed in donated DBD livers preserved with standard of care SCS. Furthermore, NMP preservation primes the DBD and DCD livers to respond to transplant reperfusion by increasing transcripts associated with resolution of inflammation and wound healing whereas the expression of inflammation promoting transcripts remain present but are diffusely expressed among the benchmark and outside benchmark livers. Overall, NMP preservation promotes the convergence of these transcript profiles that are induced in benchmark criteria and outside benchmark criteria DBD and DCD livers during transplant reperfusion.
Data availability
The complete Nanostring dataset used in the study is available as Supplementary table S4.
Abbreviations
- AR:
-
acute rejection
- BM:
-
benchmark criterion
- DBD:
-
donation after brain death
- DCD:
-
donation after cardiac death
- EAD:
-
early allograft dysfunction
- NMP:
-
normothermic machine perfusion
- OSBM:
-
outside benchmark criterion
- SCS:
-
static cold storage
- WIT:
-
warm ischemia time
References
Wolfe, R. A., Merion, R. M., Roys, E. C. & Port, F. K. Trends in organ donation and transplantation in the united states, 1998–2007. Am. J. Transpl. 9, 869–878 (2009).
Yi, Z. et al. Trends in characteristics of patients listed for liver transplantation will lead to higher rates of removal due to clinical deterioration. Transplantation 101, 2368–2374 (2017).
Rana, R. et al. Predicting liver allograft discard: the discard risk index. Transplantation 102, 1520–1529 (2018).
Malik, T. et al. Pediatric discard risk index for predicting pediatric liver allograft discard. Pediatr. Transpl. e13963 https://doi.org/10.1111/petr.13963 (2021).
Patrono, D. et al. Viability assessment and transplantation of fatty liver grafts using end-ischemic normothermic machine perfusion. Liver Transpl. 29, 508–520 (2023).
Wehrle, C. J. et al. Machine perfusion in liver transplantation: recent advances and coming challenges. Curr. Opin. Organ. Transpl. 29, 228–238 (2024).
Nasralla, D. et al. A randomized trial of normothermic preservation in liver transplantation. Nature 557, 50–56 (2018).
Maspero, M. et al. Acute rejection after liver transplantation with machine perfusion versus static cold storage a systematic review and meta-analysis. Hepatology 78, 835–846 (2023).
Panconesi, R. et al. Mitochondria and ischemia reperfusion injury. Curr. Opin. Organ. Transpl. 27, 434–445 (2022).
Anaya-Prado, R., Toledo-Pereyra, L. A., Lentsch, A. B. & Ward, P. A. Ischemia-reperfusion injury. J. Surg. Res. 15, 248–258 (2002).
Czigany, Z. et al. Ischemia-reperrfusion injury in marginal liver grafts and the role of hypothermic machine perfusion: molecular mechanisms and clinical implications. J. Clin. Med. 9, 846. https://doi.org/10.3390/jcm9030846(2020).
Ravikumar, R. et al. Liver transplantattion after ex vivo normothermic machine preservation: a phase 1 (first-in-man) clinical trial. Am. J. Transpl. 16, 1779–1787 (2016).
Martins, P. N., Buchwald, J. E., Mergental, H., Vargas, L. & Quintini, C. The role of normothermic machine Perufsion in liver transplantation. Int. J. Surg. 825, 52–60 (2020).
Quintini, C. & Liu, Q. Disrupting the field of organ preservation: normothermic preservation in liver transplantation. Transplantation 102, 1783–1785 (2018).
Liu, Q. et al. Ex situ liver machine perfusion: the impact of fresh frozen plasma. Liver Transpl. 26, 215–226 (2020).
Jassem, W. et al. Normothermic machine perfusion (NMP) inhibits Proinflammatory responses in the liver and promotes regeneration. Hepatology 70, 682–695 (2019).
Hautz, T. et al. Immune cell dynamics deconvoluted by single-cell RNA sequencing in normothermic machine perfusion of the liver. Nat. Comm. 14, 2285. 2210.1038/s41467-41023-37674-41468 (2023).
Hoyer, D. P. et al. Transcriptomic profiles of human livers undergoing rewarming machine perfusion before transplantation-first insights. Front. Integr. Genomics. 21, 367–376 (2021).
Ohman, A. et al. Activation of autophagy during normothermic machine perfusion of discarded livers is associated with improved hepatocellular function. Am. J. Physiol. Gastrointest. Liver Physiol. 322, G21–33 (2022).
Muller, X. et al. Defining benchmarks in liver transplantation: a multicenter outcome analysis determining best achievable results. Ann. Surg. 267, 419–425 (2018).
Schlegel, A. et al. A multicentre outcome analysis to define global benchmarks for donation after circulatory death liver transplantation. J. Hepatol. 76, 371–382 (2022).
Chapman, W. C. et al. Normothermic machine perfusion of donor livers for transplantation in the united States. Ann. Surg. 278, e912–e921 (2023).
Watson, C. J. E. et al. Normothermic perfusion in the assessment and preservation of declined livers before transplantation: hyperoxia and vasoplegia-important lessons from the first 12 cases. Transplantation 101, 1084–1098 (2017).
Quintini, C. et al. Transplantation of declined livers after normothermic perfusion. Surgery 171, 747–756 (2022).
JIn, H., Li, M., Jeong, E., Castro-Martinez, F. & Zucker, C. S. A body-brain circuit that regullates body inflammatory responses. Nature 630, 695–703 (2024).
Kusaka, M. et al. Activation of inflammatory mediators in rat renal isografts by donor brain death. Transplantation 69, 405–410 (2000).
Pratschke, J. et al. Brain death and its influence on donor organ quality and outcome after transplantation. Transplantation 67, 343–348 (1999).
Schlegel, A. et al. Recommendations for donor and recipient selection and risk prediction: working group report from the ILTS consensus conference in DCD liver transplantation. Transplantation 105, 1892–1903 (2021).
Croome, K. P., Lee, D. D., Nguyen, J. H., Keaveny, A. P. & Taner, C. B. Waitlist outcomes for patients relisted following failed donation after cardiac death liver transplant: implications for awarding model for end-stage liver disease exception scores. Am. J. Transpl. 17, 2420–2427 (2017).
O’Neill, S., Roebuck, A., Khoo, E., Wigmore, S. J. & Harrison, E. M. A meta-analysis and meta-regression of outcomes including biliary complications in donation after cardiac death liver transplantation. Transpl. Int. 27, 1159–1174 (2014).
Foley, D. P. et al. Donation after cardiac death: the university of Wisconsin experience with liver transplantation. Ann. Surg. 242, 724–731 (2005).
Selck, F. W., Grossman, E. B., Ratner, L. E. & Renz, J. F. Utilization, outcomes, and retransplantation of liver allografts from donation after cardiac death: implications for further expansion of the deceased-donor pool. Ann. Surg. 248, 599–607 (2008).
Czigany, Z. et al. Hypothermic oxygenated machine perfusion reduces early allograft injuury and improves post-transplant outcomes in extended criteria donation liver transplantation from donation after brain death. Ann. Surg. 274, 705–712 (2021).
Czigany, Z. et al. Improved outcomes after hypothermic oxygenated machine perfusion in liver transplantation-Long-term follow-up of a multicenter randomized controlled trial. Hepatol. Comm. 8, e0376. https://doi.org/10.1097/HC9.0000000000000376 (2024).
Schlegel, A. et al. Outcomes of DCD liver transplantation using organs treated by hypothermic oxygenated perfusion before implantation. J. Hepatol. 70, 50–57 (2019).
Tang, G. et al. Hypothermic oxygenated perfusion in liver transplantation: a meta-analysis of randomized controlled trials and matched studies. Int. J. Surg. 110, 464–477 (2023).
Panayotova, C. G. et al. Portable hypothermic oxygenated machine perfusion for organ preservation in liver transplantation (PILOTTM): a randomized open-label, clinical trial. Hepatology 79, 1033–1047 (2023).
Funding
This work was supported by a Center of Excellence award from the Lerner Research Institute of the Cleveland Clinic (WMB, CQ and RLF) and grants from the NIAID RO1-AI40459 and R01 AI158421 (RLF).
Author information
Authors and Affiliations
Contributions
KSK processed the samples, performed the analyses and prepared figures and tables; QL coordinated collection of samples and patient demographics; BTG participated in data analyses; KS, CJ, MZ, KA, BC, and LDP managed sample recording and transport; WMB, CJW, LCP, CM, KH, AS, CQ, and RLF designed the study and prepared the manuscript. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Keslar, K.S., Liu, Q., Baldwin, W.M. et al. Normothermic machine perfusion converges transplant induced transcript profiles in low and high risk DBD and DCD livers. Sci Rep 15, 34419 (2025). https://doi.org/10.1038/s41598-025-17448-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-17448-6
