
Abstract
In recent times, research has delved into the impact of dietary elements on alleviating menopausal symptoms. We endeavored to examine the correlation between the modified Mediterranean diet score (mMDS) and quality of life, menopausal symptoms, discriminative ability and determination of the optimal cut-off point. A total of one hundred forty-nine postmenopausal females were selected to participate in the cross-sectional study from June 2021 to June 2022. Upon completion of data collection through interviews, the relevant variables were calculated. The assessment of participants’ food consumption in the preceding year was conducted using a 117-item food frequency questionnaire. postmenopausal women who were referred to healthcare clinics in Lar. The participants were exclusively women aged 40 and above who had not undergone a menstrual cycle for a minimum of 12 months. We observed that mMDS associated with the severity of sexual and vasomotor symptoms. The third tertile of mMDS had a significantly lower odds ratio for severe to moderate sexual (OR: 0.17; 95% CI: 0.068, 0.450) and vasomotor (OR: 0.20; 95% CI: 0.064, 0.658) symptoms compared to the first tertile. Also, mMDS showed significant discriminative ability in identifying women with severe to moderate poor quality of life (AUC = 0.997, 95% CI = 0.988–1.000; p-value = 0.001), vasomotor (AUC = 0.727, p-value < 0.001), psychological (AUC = 0.867, p-value < 0.001), physical (AUC = 0.934, p-value < 0.001) and sexual symptoms (AUC = 0.753; p-value < 0.001). There is promising yet incongruous data indicating the potential of the Mediterranean diet in the management of vasomotor symptoms in menopausal women. Further comprehensive, extended research is essential for the development of precise dietary recommendations.
Similar content being viewed by others

Introduction
Menopause is an inherent physiological phenomenon that signifies the cessation of menstrual cycles in females. The condition is distinguished by the absence of menstruation, a decrease in ovarian function, and a range of symptoms1,2. The symptoms associated with menopause encompass vasomotor symptoms, namely hot flashes and night sweats, as well as genitourinary symptoms, including vaginal dryness and discomfort. Additionally, mood changes, fatigue, depression, headaches, joint pains, and weight gain may also manifest3. The mean age of menopause in the United States is approximately 51 years, however it can manifest between the ages of 40 and 504.
Hormonal therapy, including estrogen-containing hormone therapy, has demonstrated efficacy in the treatment of vasomotor symptoms, such as hot flashes and night sweats5. Vasomotor symptoms can also be addressed with the use of nonhormonal drugs, such as selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, and gabapentin6. The efficacy of cognitive behavior therapy and therapeutic hypnosis in mitigating vasomotor symptoms and their corresponding sleep disruptions has been demonstrated7. Nutritional therapies and lifestyle modifications have demonstrated potential in the management of symptoms associated with postmenopause8. Research has indicated that the implementation of these therapies has the potential to ameliorate the intensity of depression and anxiety symptoms in women throughout the menopausal transition and the subsequent postmenopausal period8,9. The adoption of a more nutritious dietary regimen, characterized by increased intake of vegetables, whole grains, and unprocessed foods, has been associated with reduced severity of psychological symptoms, sleep disturbances, vasomotor symptoms, urogenital symptoms, and somatic symptoms9. However, it has been shown that a significant consumption of processed foods, saturated fats, and sweets is linked to an increased severity of these symptoms10. It is suggested that embracing a more nutritious eating regimen, such as the Mediterranean diet, could perhaps mitigate prevalent symptoms associated with menopause9,11. The diet is distinguished by a substantial consumption of olive oil, fruits, vegetables, non-refined breads and cereals, potatoes, legumes, and nuts. It involves a moderate intake of fish and poultry, a low consumption of dairy products, red meat, processed meats, and sweets, and a moderate consumption of wine with meals12,13. The Modified Mediterranean Diet Score (mMDS) is a scoring technique employed to assess compliance with the Mediterranean diet. This 10 unit dietary score was designed by Mrs. Trichopoulou et al.14,15. In this research, a modified version of the score was employed to account for non-Mediterranean populations characterized by limited consumption of olive oil. Specifically, the replacement of monounsaturated fatty acid (MUFA) consumption with the combined intake of monounsaturated and polyunsaturated fatty acids (PUFA) was implemented16. Numerous studies have employed different iterations of this score and have documented negative correlations with diverse diseases and total mortality17,18,19.
Considering the adverse effects of menopausal symptoms on health and quality of life, the important role of nutrition in controlling and improving these symptoms, and to address these gaps in the literature, we conducted a cross-sectional study to assess the association between adherence to mMDS and menopause-specific quality of life and symptom severity in postmenopausal women. To our knowledge, this is the first study in the region to evaluate the association between mMDS and a comprehensive range of menopausal symptoms and quality of life domains in postmenopausal women. Our findings provide new insights into the potential role of dietary patterns in the management of menopausal symptoms, which may inform future dietary recommendations for this population.
Materials and methods
Study participants
The research endeavor spanned a duration of around one year, namely from June 2021 to June 2022. It involved the examination of 149 postmenopausal women who were referred to healthcare clinics in [location anonymized for peer review]. Only women who satisfied the specified criteria were chosen for the interview. The participants were exclusively women aged 40 and above who had not undergone a menstrual cycle for a minimum of 12 months. Additional criteria for inclusion were: (1) Absence of mental diseases, malignancies, autoimmune conditions, and other severe medical conditions, (2) When diabetes, high blood pressure, or thyroid issues were present, it was crucial to ensure that the disease was fully managed, (3) No chronic smoking, (4) The BMI ranged from 18.5 to 40 kg/m2. Women possessing these attributes were omitted: (1) Adhering to a dietary regimen characterized by a caloric intake below 800 kcal or beyond 4000 kcal, (2) Employing hormone therapy or dietary supplements, (3) Administering psychiatric medications, (4) Demonstrating a lack of willingness to sustain collaboration. The research ethics committee of the [blinded] granted approval for our study protocol.
Assessment of general characteristics, socioeconomic status, anthropometry, and physical activity
The sociodemographic, familial, medications, dietary supplements, health conditions, and medical records were collected using the standard general information questionnaire. Weight was measured with an accuracy of 100 g, while height was measured with an accuracy of 0.5 cm using a Seca brand digital scale and a wall-mounted tape measure, following the recommended instructions. The body mass index (BMI) was computed for each participant using the anthropometric measures that were gathered. We employed the General Physical Activity Questionnaire (GPAQ), a straightforward instrument designed for individuals aged 16 to 7420, to assess the physical activity levels of the participants. This survey had three inquiries pertaining to an individual’s level of physical activity during work hours, the total duration of physical activity within the past week, and their walking pace. Ultimately, the subjects were classified into four distinct degrees of physical activity. The data was gathered by proficient researchers via in-person interviews.
Dietary assessment
The assessment of participants’ food consumption in the preceding year was conducted using a 117-item food frequency questionnaire that was specifically tailored for the [blinded] population. The questionnaire’s validity and reliability have been shown in prior research21. Standard and traditional serving sizes were used to evaluate the consumption amounts of 117 products. The participants provided their self-reported frequency of food item consumption using a set of nine suggested response options, which ranged from never or less than once a month to 6 times or more per day. The recorded values for each item were transformed into daily consumption quantities (in grams), and the energy, micronutrient, and macronutrient intakes of each individual were determined using USDA data22 and the [blinded]-modified version of IV Nutritionist software ®.
mMDS
Trichopoulou et al. have developed a scale that quantifies the level of adherence to the traditional Mediterranean diet15,23. Each of the nine mentioned components was assigned a value of either zero or one, with the sex-specific medians among the participants serving as the cut-off values. Individuals who consumed less than the median amount of considered beneficial components (such as vegetables, legumes, fruits, cereals, and fish) were given a value of zero, while those who consumed more than the median were given a value of one. Individuals who consumed meat and dairy products below the median intake were assigned a value of one, while those who consumed them above the median were assigned a value of zero. Women who consumed between 5 g and 25 g were assigned a value of one. The lipid intake was determined by calculating the ratio of the combined amount of monounsaturated and polyunsaturated lipids to saturates. The modified score for the Mediterranean diet incorporates both monounsaturated and polyunsaturated fats in the numerator of the lipid ratio. This number ranges from zero, indicating minimal adherence, to nine, indicating optimal adherence.
Assessment of menopausal symptoms
The menopausal-specific quality of life questionnaire (MENQOL) was employed to evaluate the manifestation and intensity of menopausal symptoms24,25,26. This survey comprised a total of 29 items, which were categorized into four distinct subgroups pertaining to menopausal problems25. Out of the 29 items in this test, 3 pertained to vasomotor symptoms, 7 assessed psychological issues, 16 pertained to physical concerns, and 3 pertained to sexual problems. Falahzadeh et al., conducted an investigation of the validity and reliability of the Persian version of the MENQOL27. In response to each inquiry, the participant indicated if she has encountered these symptoms within the preceding month. If the response was affirmative, the participant assigned a numerical value ranging from 0 to 6 based on the intensity of the symptom encountered. The quantification of quality of life was achieved by aggregating all of these ratings. A greater total score on the MENQOL scale was indicative of a diminished quality of life. To enhance interpretability, MENQOL scores were categorized into two groups: <5 (mild or no symptoms) and ≥ 5 (moderate to severe symptoms). While no established cut-off exists in the literature for this classification, this decision was made based on the instrument’s scoring scale: a score of 5 indicates “quite a bit bothersome,” reflecting higher symptom intensity, and scores of 6 indicate “extremely bothersome.” Therefore, the ≥ 5 threshold was used to identify clinically meaningful moderate/severe symptom burden.
Statistical analysis
Statistical analysis were conducted using SPSS 22 ®. All analytical tests were two tailed and the significance level was assumed as P-value < 0.05. Quantitative and qualitative characteristics were described using the mean (standard deviation) and frequency report (percentage). Graphical methods and Kolmogorov-Smirnov (or Shapiro-Wilk) test were used to assess the normality of all variables, and logarithm (log) transformations were applied to non-normal variables. Initially, mMDS were classified into tertiles for the purpose of analysis. Demographic information and food intakes were compared between three distinct groups in each model using a one-way analysis of variance and chi-square testing. An analysis of multiple regression was conducted to examine the influence of demographic variables on MENQOL. Additionally, the scores of different subgroups were assessed. Three distinct tests were conducted in order to examine the correlation between mMDS and symptoms associated with menopause. We conducted an analysis of variance to compare the mean (standard deviation) of the overall score of the questionnaire with the tertile groups of mMDS. During the concluding phase, we partitioned each subgroup into two distinct tiers. To achieve this objective, the scores were aggregated by a factor of two and varied between 2 and 8. The absence of symptoms was also regarded as a 1 point. If the average score of each subtype exceeded 5, it was categorized as “moderate to severe”, whereas if it fell below 5, it was classed as “mild or no symptoms”. Logistic regression was subsequently employed to assess the odds ratios associated with severe to moderate intensity symptoms in the tertiles of mMDS, including both crude and adjusted data. Confounding variables were controlled for in this study, including age (years), length of time since menopause (years), energy (Kcal), job (employed or not), education (academic or not), physical activity, underlying diseases (having controlled diabetes, high blood pressure or thyroid disorder or not), and body mass index (kg/m2). The regression model incorporated all elements of mMDS, such as dietary groups, micro and macronutrients, and energy intake, to evaluate their impact on the scores obtained for each subgroup. Receiver operating characteristic (ROC) curves were constructed to assess the discriminative ability of the mMDS for identifying moderate to severe symptoms and poor menopause-specific quality of life. The area under the curve (AUC), sensitivity, specificity, and accuracy were calculated. However, no internal validation techniques (such as cross-validation or bootstrapping) were applied in this exploratory analysis.
Results
This study evaluated a group of 149 women who had reached menopause and were between the ages of 42 and 63. Figure 1 depicts the enrollment of the participants. The document labelled as Table 1 presents the general characteristics of those participating in the study categorized into tertiles based on mMDS. The mean ± SD of mMDS in the present research was 4.01 ± 1.36. When we analyzed the data by dividing it into three categories based on mMDS, we found that persons in the highest tertile were older and had fewer underlying disease. We found a marginally significant P-value for physical activity, occupation, and husbands’ education status. No other significant differences were seen.

Flow diagram of participant enrollment.
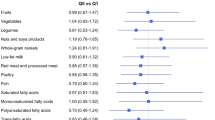
Table 2 provides the comparison of the average consumption of food groups in tertiles of mMDS. Individuals in the highest tertile of mMDS had significantly greater consumption of vegetables, fishes, legumes, and MUFA + PUFA/SFA, whereas their intake of dairy products and meats was notably lower compared to those in the lowest tertile.
Table 3 presents a comparison of the average score of MENQOL and its subscales, categorized according to the tertile of mMDS. There was no significant difference observed in the mean score of MENQOL, vasomotor symptoms, psychological symptoms, physical symptoms, and sexual symptoms across the tertile of mMDS.
Table 4 presents the crude and multivariable-adjusted ORs of suffering from severe to moderate levels of each symptom including vasomotor symptoms, psychological symptoms, physical symptoms, sexual symptoms and MENQOL in relation to various mMDS categories. The risk of experiencing severe to moderate menopausal vasomotor symptoms was significantly inversely correlated with mMDS in the crude model (OR: 0.18; 95% confidence interval (CI): 0.063, 0.550).
After adjusting for potential confounding factors (The confounders adjusted for in the regression models were age, years since menopause, energy intake, occupation, education, physical activity, underlying diseases (controlled diabetes, hypertension, or thyroid disorder), and BMI, as described in the Statistical Analysis section), the analysis still showed a significant correlation (OR: 0.20; 95% CI: 0.064, 0.658). Individuals in the highest tertile of mMDS were 83% less likely to have severe to moderate menopausal sexual symptoms before (OR: 0.17; 95% CI: 0.070, 0.419) or after correcting for potential confounders (OR: 0.17; 95% CI: 0.068, 0.450). The other relationship under investigation, however, did not show statistical significance.
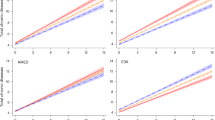
The prediction ability of mMDS for general symptoms of menopause and quality of life (MENQOL) was shown to be statistically significant, as indicated by the ROC curves. The index’s discriminative ability is displayed by the area under the curve (Table 5). Based on ROC analysis, mMDS scores of − 2 showed the highest discriminative ability for identifying poor quality of life (AUC = 0.997, 95% CI: 0.988–1.000), with 95% sensitivity and specificity. The discriminative ability was lower but still statistically significant for vasomotor (AUC = 0.727), psychological (AUC = 0.867), physical (AUC = 0.934), and sexual symptoms (AUC = 0.753). These results should be interpreted with caution, as no internal validation was performed (Table 5).
Discussion
The association between the risk of experiencing severe to moderate menopausal vasomotor symptoms and mMDS was found to have a significant negative correlation in both the unadjusted model and even after accounting for potential confounding variables, the analysis continued to reveal a noteworthy relationship. Those individuals situated in the uppermost tertile of mMDS exhibited an 83% decreased likelihood of encountering severe to moderate menopausal sexual symptoms, both prior to and subsequent to adjusting for potential confounding elements. mMDS displayed substantial prognostic capability concerning vasomotor, psychological, physical, and sexual subcategories.
The link between the Mediterranean diet and vasomotor symptoms of menopause, including hot flashes and night sweats, is garnering increased attention in the realms of nutritional epidemiology and women’s health. The Mediterranean diet is abundant in phenolic compounds and emphasizes high consumption of fruits, vegetables, whole grains, legumes, nuts, and extra-virgin olive oil as the main source of added fat, along with a moderate intake of fish and poultry. This dietary pattern has been studied for its potential advantages in managing menopausal symptoms, especially vasomotor symptoms and the age of onset28. The position paper of the European Menopause and Androgen Society (EMAS) suggests that the Mediterranean diet can alleviate vasomotor symptoms in women undergoing menopause, underscoring the potential advantages of this dietary regimen in managing symptoms associated with menopause29. Although the EMAS acknowledges the Mediterranean diet, our study provides new evidence by examining the association between mMDS and specific menopausal symptom domains in an underrepresented population, and by identifying potential cut-off points for dietary adherence. Studies indicate that following the Mediterranean Diet can lead to a reduction in the frequency and severity of menopausal symptoms, especially among women with obesity9,30. The intake of legumes and extra-virgin olive oil, specific elements of the Mediterranean diet, have been linked to a decrease in the severity of vasomotor and sexual symptoms during menopause31. Additionally, a diet rich in plants and daily intake of soybeans has been found to considerably lessen the frequency and severity of hot flashes and related symptoms after menopause. This suggests that dietary changes could be an effective strategy for managing vasomotor symptoms29,32. Conversely, the consumption of poultry and low-fat dairy products has been associated with an exacerbation of menopausal symptoms32. Thus, embracing the Mediterranean diet could be a useful approach for women looking to control vasomotor symptoms during menopause.
An Australian cross-sectional study in 2024 assessed Mediterranean Diet adherence using the MEDAS tool and menopausal symptoms with the Menopause Rating Scale in 207 peri- and menopausal women aged 40–60. The researchers found that overall adherence to the Mediterranean diet was not associated with the severity of menopausal symptoms. However, low consumption of sugar-sweetened beverages was inversely associated with joint and muscle complaints, and lower intake of red and processed meats was linked to better general health and physical function33. Another study examined the relationship between adherence to a Mediterranean diet and the severity of menopausal symptoms in women living in Ireland. A total of 304 women over age 40 (154 perimenopausal and 150 postmenopausal) participated, with dietary adherence assessed using the 14-item Mediterranean Diet Assessment Tool (MDAT) and menopausal symptoms measured by the Menopause Rating Scale (MRS). Most participants had moderate diet adherence, while high adherence was rare. The study found that lower adherence to the Mediterranean diet in postmenopausal women predicted worse menopausal symptoms, and higher BMI also correlated with greater symptom severity in both peri- and postmenopausal groups. These findings suggest that both increased body weight and lower adherence to a Mediterranean dietary pattern may contribute to a more symptomatic menopausal experience, highlighting the need for further research in this area34.
There are several proposed mechanisms through which the Mediterranean diet may influence menopausal symptoms. This mechanism has been proposed in the literature, although further research is needed to confirm its role in menopausal symptom management. The impact of the Mediterranean diet on sex hormone levels and the age of menopause suggests it could play a role in easing vasomotor symptoms. In general, adhering to the Mediterranean diet might regulate hormonal fluctuations, potentially lessening the severity of vasomotor symptoms experienced during menopause35. The Mediterranean diet’s potential to decrease the frequency and severity of menopausal symptoms is largely due to its high phytoestrogen content, particularly in foods such as soy. These phytoestrogens may exert a mild estrogen-like effect, which could help alleviate vasomotor symptoms9,30.
The Mediterranean diet has been linked to decreased inflammation, as evidenced by reduced levels of inflammatory indicators such as tumor necrosis factor (TNF-α) and interleukin 1 beta (IL-1β)36. This could aid in the relief of menopausal symptoms, given that inflammation has been associated with a rise in vasomotor symptoms31. Evidence suggests that the Mediterranean diet can reduce markers of oxidative stress, including malondialdehyde (MDA) and oxygen radical absorbance capacity (ORAC). This could potentially aid in alleviating symptoms associated with menopause37. The Mediterranean diet is associated with a more beneficial gut microbiota, which aids in maintaining the function of the gut barrier and decreasing inflammation38. This could contribute to the overall health and well-being of women going through menopause, potentially easing symptoms. Higher adherence to the Mediterranean dietary pattern can help manage weight gain and the distribution of visceral fat during menopause, which affects hormonal balance. Sticking to the Mediterranean diet has been linked to less significant increases in waist circumference over time in women post-menopause. This is crucial as an increased waist circumference and obesity are risk factors for worsening menopausal symptoms, including vasomotor symptoms. However, the diet was not linked to significant changes in overall weight or the risk of becoming overweight or obese. Furthermore, the anti-inflammatory and antioxidant properties of the Mediterranean diet, along with its impact on weight management, can help alleviate typical menopausal metabolic disorders, such as type 2 diabetes and cardiovascular diseases35,39.
The Mediterranean diet, when combined with a comprehensive lifestyle medicine strategy that encompasses regular exercise, stress management, and the avoidance of harmful substances, may collectively alleviate vasomotor symptoms. This integrated approach emphasizes the significance of maintaining a healthy lifestyle in managing symptoms associated with menopause30.
While there are some encouraging results, the evidence regarding the connection between the Mediterranean diet and vasomotor symptoms is not entirely conclusive. Some research indicates positive outcomes, but other studies advocate for more comprehensive research to formulate definitive dietary recommendations for women going through menopause.
This investigation marks the initial attempt to juxtapose and assess the correlation and prognostic capability of three distinct indicators concurrently. Within this study, diverse statistical methodologies were trialed, culminating in the documentation of the outcomes derived from two methodologies deemed more suitable, thereby affording the clinicians a comprehensive perspective on the results and their practical implications. Moreover, endeavors were made to enhance the applicability and user-friendliness of the findings at a clinical level by ascertaining the optimal cut-off point. Noteworthy strengths of this study encompass the meticulousness of the trained interviewer in data collection, thus minimizing potential reporting inaccuracies, the utilization of culturally appropriate questionnaires tailored for the [blinded] populace, comprehensive and precise inclusion criteria, as well as meticulous adjustment for numerous confounding variables.
Our investigation, akin to others, is not devoid of limitations that necessitate acknowledgment. This endeavor was executed in a cross-sectional manner, thereby precluding definitive assertions regarding causality in the observed relationships among the variables of interest. The outbreak of the coronavirus posed a constraint on the sample size. Data gathering relied on self-reports during interviews, notwithstanding the interviewer’s diligence in error mitigation, the inherent reliance on individual memory introduces an inevitable margin of error. Cultural sensitivities may lead to unrealistic responses, particularly concerning inquiries of a sexual or psychological nature. While the food frequency questionnaire was tailored for the [blinded] context, the scant representation of local cuisine peculiar to the region might impact the derived food index scores. Additionally, the cut-off values identified through ROC analysis were not validated using internal methods such as cross-validation or bootstrapping. This limits the generalizability of the proposed thresholds and should be addressed in future studies. Furthermore, the use of a modified mMDS that incorporates both MUFA and PUFA in place of only MUFA, due to limited olive oil consumption in the population, may affect comparability with traditional Mediterranean Diet Scores. This methodological adaptation, while contextually appropriate, should be considered when interpreting the results.”
Conclusion
In summary, there is encouraging but inconsistent evidence suggesting that the Mediterranean diet could help manage vasomotor symptoms during menopause. More robust, long-term studies are required to formulate clear dietary guidelines. The potential advantages of the Mediterranean diet, coupled with other lifestyle changes, present a non-drug alternative for managing menopausal symptoms. This could be particularly beneficial for women who are unable or choose not to undergo hormone therapy.
Data availability
Data is provided within the manuscript or supplementary information files.
Abbreviations
- mMDS:
-
modified mediterranean diet Score
- MUFA:
-
monounsaturated fatty acid
- PUFA:
-
polyunsaturated fatty acids
- GPAQ:
-
General Physical Activity Questionnaire
- MENQOL:
-
menopausal-specific quality of life questionnaire
- ROC:
-
receiver operating characteristic
- EMAS:
-
European Menopause and Androgen Society
- TNF-α:
-
tumor necrosis factor
- MDA:
-
malondialdehyde
- ORAC:
-
oxygen radical absorbance capacity
References
Santoro, N. & Johnson, J. Diagnosing the onset of menopause. Jama 322, 775–776 (2019).
Ceylan, B. & Özerdoğan, N. Factors affecting age of onset of menopause and determination of quality of life in menopause. Turkish J. Obstet. Gynecol. 12, 43 (2015).
Monteleone, P., Mascagni, G., Giannini, A., Genazzani, A. R. & Simoncini, T. Symptoms of menopause—global prevalence, physiology and implications. Nat. Reviews Endocrinol. 14, 199–215 (2018).
Rana, S. & Panghal, M. R. A study to identify the age of menopause and its relation to socio-economic determinants and to assess the knowledge and attitude about the health effects of menopause. 10, 1118–1126 (2022)
Chang, J. G., Lewis, M. N. & Wertz, M. C. Managing menopausal symptoms: common questions and answers. Am. Family Phys. 108, 28–39 (2023).
Pan, M. et al. Drugs for the treatment of postmenopausal symptoms: hormonal and non-hormonal therapy. Life Sci. 312, 121255 (2023).
Crandall, C. J., Mehta, J. M. & Manson, J. E. Management of menopausal symptoms: a review. Jama 329, 405–420 (2023).
Grigolon, R. B. et al. Effects of nutritional interventions on the severity of depressive and anxiety symptoms of women in the menopausal transition and menopause: a systematic review, meta-analysis, and meta-regression. Menopause 30, 95–107 (2023).
Yelland, S., Steenson, S., Creedon, A. & Stanner, S. The role of diet in managing menopausal symptoms: A narrative review. Nutr. Bull. 48, 43–65 (2023).
Ilesanmi-Oyelere, B. L. & Kruger, M. C. Associations between dietary patterns and an array of inflammation biomarkers and plasma lipid profile in postmenopausal women. BMC Women’s Health. 23, 256 (2023).
rah Kang, A. Managing menopausal symptoms through exercise and dietary changes. (2023).
Sofi, F., Abbate, R., Gensini, G. F. & Casini, A. Accruing evidence on benefits of adherence to the mediterranean diet on health: an updated systematic review and meta-analysis. Am. J. Clin. Nutr. 92, 1189–1196 (2010).
Davis, C., Bryan, J., Hodgson, J. & Murphy, K. Definition of the mediterranean diet: a literature review. Nutrients 7, 9139–9153 (2015).
TRICHOPOULOU, A. Diet and overall survival. EGEA, 9. (2003)
Trichopoulou, A., Costacou, T., Bamia, C. & Trichopoulos, D. Adherence to a mediterranean diet and survival in a Greek population. N. Engl. J. Med. 348, 2599–2608 (2003).
Trichopoulou, A. et al. Modified mediterranean diet and survival: EPIC-elderly prospective cohort study. Bmj 330, 991 (2005).
Lasheras, C., Fernandez, S. & Patterson, A. M. Mediterranean diet and age with respect to overall survival in institutionalized, nonsmoking elderly people. Am. J. Clin. Nutr. 71, 987–992 (2000).
Osler, M. & Schroll, M. Diet and mortality in a cohort of elderly people in a North European community. Int. J. Epidemiol. 26, 155–159 (1997).
Knoops, K. T. et al. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: the HALE project. Jama 292, 1433–1439 (2004).
for Nursing, N. C. C. & UK, S. C. In Irritable Bowel Syndrome in Adults: Diagnosis and Management of Irritable Bowel Syndrome in Primary Care [Internet] (Royal College of Nursing (UK), 2008).
Malekshah, A. F. et al. Validity and reliability of a new food frequency questionnaire compared to 24 h recalls and biochemical measurements: pilot phase of Golestan cohort study of esophageal cancer. Eur. J. Clin. Nutr. 60, 971–977 (2006).
Ahuja, J. et al. USDA food and nutrient database for dietary studies, 5.0–documentation and user guide. US Department of Agriculture, Agricultural Research Service, Food Surveys Research Group: Beltsville, MD, USA (2012).
Trichopoulou, A. et al. Diet and overall survival in elderly people. Bmj 311, 1457–1460 (1995).
Beezhold, B., Radnitz, C., McGrath, R. E. & Feldman, A. Vegans report less bothersome vasomotor and physical menopausal symptoms than omnivores. Maturitas 112, 12–17 (2018).
Taşkıran, G. Menopozal Semptom Şiddeti ve Menopoza Özgü Yaşam Kalitesini Etkileyen Faktörlerin İncelenmesi. (2019).
Papadima, E. I. et al. Linguistic translation and validation of the menopause-specific quality of life (MENQOL) questionnaire in Greek menopausal women. Menopause 27, 808–815 (2020).
Fallahzadeh, H. Quality of life after the menopause in iran: a population study. Qual. Life Res. 19, 813–819 (2010).
Flor-Alemany, M., Marín-Jiménez, N., Coll-Risco, I., Aranda, P. & Aparicio, V. A. Influence of dietary habits and mediterranean diet adherence on menopausal symptoms. The FLAMENCO project. Menopause 27, 1015–1021 (2020).
Barnard, N. D. et al. A dietary intervention for vasomotor symptoms of menopause: a randomized, controlled trial. Menopause 30, 80–87 (2023).
Kennard, A. et al. Lifestyle medicine and vasomotor symptoms: an analytic review. American J. Lifestyle Medicine. 8, 100–110 (2024).
Barrea, L. et al. Does mediterranean diet could have a role on age at menopause and in the management of vasomotor menopausal symptoms? The viewpoint of the endocrinological nutritionist. Curr. Opin. Food Sci. 39, 171–181 (2021).
Vetrani, C. et al. Mediterranean diet: what are the consequences for menopause? Front. Endocrinol. 13, 886824 (2022).
Byrne-Kirk, M., Mantzioris, E., Scannell, N. & Villani, A. Adherence to a mediterranean-style diet and severity of menopausal symptoms in perimenopausal and menopausal women from australia: A cross-sectional analysis. Eur. J. Nutr. 63, 2743–2751 (2024).
Murphy, M., Dunne, N., Keegan, B. & Heavey, P. Menopausal symptoms and adherence to a Mediterranean dietary pattern in women living in Ireland. Proceedings of the Nutrition Society 81, E114 (2022).
Barrea, L. et al. Mediterranean diet as medical prescription in menopausal women with obesity: a practical guide for nutritionists. Crit. Rev. Food Sci. Nutr. 61, 1201–1211 (2021).
Mohajeri, M., Mohajery, R. & Cicero, A. F. G. Adherence to the mediterranean diet association with serum inflammatory factors stress oxidative and appetite in COVID-19 patients. Med. (Kaunas). 59. https://doi.org/10.3390/medicina59020227 (2023).
Cirillo, M. et al. Mediterranean diet and oxidative stress: a relationship with pain perception in endometriosis. Int. J. Mol. Sci. 24 https://doi.org/10.3390/ijms241914601 (2023).
Ratajczak, A. E. et al. Should the mediterranean diet be recommended for inflammatory bowel diseases patients? A narrative review. Front. Nutr. 9, 1088693. https://doi.org/10.3389/fnut.2022.1088693 (2022).
Best, N. & Flannery, O. Association between adherence to the mediterranean diet and the Eatwell guide and changes in weight and waist circumference in post-menopausal women in the UK women’s cohort study. Post. Reprod. Health. 29, 25–32. https://doi.org/10.1177/20533691231156643 (2023).
Acknowledgements
We express our appreciation to the participants of this study.
Author information
Authors and Affiliations
Contributions
N.H., and F.SH contributed in conception, design, and statistical analysis. SMG., MN., F.B, and F.SH contributed in data collection and manuscript drafting. F.SH and N.H. supervised the study. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Iran University of Medical Sciences (IR.IUMS.REC.1400.213). Written informed consent was obtained from all subjects/patients.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Haghshenas, N., Ghoreishy, S.M., Noormohammadi, M. et al. Association between modified mediterranean diet score and menopause-specific quality of life and symptoms: a cross-sectional study. Sci Rep 15, 31682 (2025). https://doi.org/10.1038/s41598-025-17578-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-17578-x
