
Abstract
Double negative (DN) B cells, defined as CD27-IgD- B cells, are increased in older healthy individuals as well as in patients with certain diseases. However, the relationship between DN B cells and Sjögren’s disease (SjD) in newly diagnosed patients remains unclear. Seventy SjD patients and thirty-six healthy controls (HCs) were recruited in this study. Peripheral blood B cell subsets were analyzed using flow cytometry. The percentage and absolute count of DN B cells were significantly lower in SjD patients compared to HCs (p = 0.000 and p = 0.007, respectively). Patients with medium to high disease activity, defined by an EULAR Sjögren Syndrome Disease Activity Index (ESSDAI) score ≥ 5, exhibited lower DN B cell levels compared to those with low disease activity (ESSDAI score < 5, p = 0.029 and p = 0.000, respectively). Moreover, lower DN B cell percentages were associated with glandular involvement (p = 0.039) and neutropenia (p = 0.034). Regression analysis revealed a negative correlation between DN B cells and SjD disease activity (B=-0.240, 95% CI:-0.468 to -0.013, p = 0.039). Additionally, DN B cells showed weak negative correlation with the percentage of total B cells (r=-0.266, p = 0.026). This study demonstrates that DN B cells are decreased in SjD, particularly in patients with glandular involvement and high disease activity. Moreover, the inverse correlation between DN B cells and total B cells suggested that DN B cells may play a role in the pathogenesis of SjD.
Similar content being viewed by others

Introduction
Sjögren’s disease (SjD) is a chronic autoimmune disorder characterized by progressive destruction of salivary and lacrimal glands, leading to dry mouth and eyes. The disease spectrum ranges from sicca syndrome to diverse systemic manifestations1. Hematologic involvement, including leukopenia, anemia, and thrombocytopenia, is observed in approximately one-third of patients with SjD2. Leukopenia, occurring in 20–60% of patients with SjD, is associated with positive anti-SSA antibodies and multiple glandular involvements3. Anemia is also common, affecting 11.2–19% of patients4. Thrombocytopenia, though relatively rare, can be severe and resistant to treatment in some cases. Hyperactivation of B cells may lead to lymphoma in about 5% of patients with SjD, which represents one of the most severe complications5.
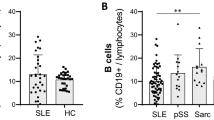
The pathogenesis of SjD involves multiple factors, with abnormalities in B-lymphocyte subsets playing a crucial role6. These abnormalities contribute to the production of autoantibodies and cytokines. They also affect antigen presentation and T cell responses7,8,9. Among these, double negative (DN) B cells, a poorly understood subset lacking both IgD and CD27, were first identified in systemic lupus erythematosus (SLE) patients by Huang et al. in 200210. DN B cells increase in older healthy individuals11 and patients with other autoimmune12,13,14 and infectious diseases15. In SLE, DN B cells have been identified as precursors of antibody-secreting cells (ASCs), including plasma cells and plasmablasts16. In some autoimmune diseases, DN B cells can perform antibody-independent functions through antigen presentation and the secretion of pro-inflammatory cytokines17. Additionally, DN B cells can migrate to pro-inflammatory sites via the expression of CXC-chemokine receptor (CXCR) 3 and C-C motif chemokine receptor (CCR) 614.
To our knowledge, data on the expression of DN B cells and their relationship with the EULAR Sjögren Syndrome Disease Activity Index (ESSDAI) in untreated SjD patients are limited. Therefore, this study aims to explore the relationship between DN B cells and the clinical characteristics of SjD in newly diagnosed patients, with a focus on understanding the potential role of DN B cells in the pathogenesis of SjD.
Materials and methods
Patients and healthy controls
This observational retrospective study included 70 patients with SjD admitted to the Second Affiliated Hospital of Dalian Medical University from March 2023 to June 2024. All patients met the 2016 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) Classification Criteria for SjD. Exclusion criteria included a history of head and neck radiotherapy, active hepatitis C virus infection, acquired immunodeficiency syndrome, sarcoidosis, amyloidosis, graft-versus-host disease, and IgG4-related disease18. Additionally, Patients who had recent infections or taken glucocorticoids or disease-modifying antirheumatic drugs (DMARDs) in the last six months were also excluded. Furthermore, thirty-six age-matched healthy controls (HCs) were enrolled. The study was conducted in accordance with the principles of the Helsinki Declaration and approved by the ethical committee of the Second Affiliated Hospital of Dalian Medical University (No. KY2024-230-01). Written informed consent was obtained from all participants.
Flow cytometry analysis
Fresh whole blood samples were processed within 24 h of collection and incubated with antibodies at room temperature for 15 min in the dark. After red blood cell lysis (BioLegend, San Diego, USA), the samples were centrifuged, and the supernatants were discarded. The cells were then washed twice with phosphate-buffered saline (PBS). B cell subsets were classified using murine anti-human monoclonal antibodies: anti-CD27-FITC (Biolegend), anti-CD19-PE-Cy7 (BD Biosciences), anti-CD24-PE (eBioscience), anti-IgD-PerCP (Biolegend), anti-CD38-BV421 (BD Biosciences), anti-CD45-V500 (BD Biosciences), and anti-CD20-APC-Cy7 (Biolegend). Total B cells were defined as the percentage of lymphocytes identified as CD19+. DN B cells were defined as CD19 + CD27-IgD-; Naïve B cells as CD19 + CD27-IgD+; Memory B cells as CD19 + CD27 + IgD-; and plasmablasts as CD20-CD19 + CD27 + CD38^hi. B10-like cells are a functional subtype that regulates immune responses and is characterized by IL-10 production in humans and mice. Since we did not detect IL-10 production, we refer to CD19 + CD27 + CD24^hi cells as memory B cells with regulatory functions, termed B10-like cells. Flow cytometry was performed using a BD FACSCanto II (BD Biosciences, San Jose, CA), and data were analyzed using FlowJo version X (TreeStar, Woodburn, OR).
Data collection
Data collected from patients’ medical records included gender, age at diagnosis, disease duration, xerostomia, xerophthalmia. Other organ manifestations were also recorded, including general symptoms, lymphadenopathy, glandular involvement, cutaneous, articular, pulmonary, renal, muscular, nervous system, and hematological system. Disease activity was assessed using the ESSDAI at the time of initial treatment, with scores ranging from 0 to 12319. Peripheral blood parameters included absolute neutrophil counts ≤ 1.5 × 10^9^/L (neutropenia), lymphocyte counts ≤ 1.0 × 10^9^/L (lymphopenia), hemoglobin ≤ 120 g/L (anemia), and platelet counts ≤ 150 × 10^9^/L (thrombocytopenia). Immunological indices, including antinuclear antibody (ANA), anti-Ro60/SSA, anti-La/SSB, anti-Ro52, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), immunoglobulin G (IgG), immunoglobulin A (IgA), immunoglobulin M (IgM), complement C3, and rheumatoid factor (RF), were measured at the time of hospitalization. The absolute counts of B-cell subsets were calculated by multiplying the percentage of each subset obtained from flow cytometry by the total lymphocyte count from the complete blood count (CBC) analyzer.
Statistical analysis
Data were analyzed using SPSS version 25 and R software version 4.2.3. Normally distributed continuous variables were presented as mean ± standard deviation (SD), and group differences were assessed using Student’s t-test. Non-normal distributed continuous variables were expressed as median [interquartile range], and the Mann-Whitney U test was used for comparisons. Spearman correlation coefficients were used to analyze the relationship between clinical indicators and B cell subsets. Regression analysis was used to explore the relationship between B cell subsets and SjD. A p-value < 0.05 was considered statistically significant.
Results
Demographic characteristics of SjD patients
The study included 70 SjD patients and 36 HCs, matched for age and gender (age, 53.93 ± 11.85 vs. 52.89 ± 14.02, p = 0.085; male/female, 4/66 versus 6/30, p = 0.085, in SjD and HC, respectively). Patient characteristics of SjD are summarized in Table 1. The mean duration of SjD patients was 53.4 months, and the median ESSDAI was 4 (range from 0 to 10).
Decreased DN B cells in peripheral blood of SjD patients
As shown in Fig. 1A and B, the percentage and absolute count of DN B cells were comparable between HCs and SjD patients. Specifically, the percentage of DN B cells (of total CD19 + B cells) was significantly lower in SjD patients (median = 3.40, p = 0.000), compared to HCs (median = 7.70). The absolute count of DN B cells was also lower between SjD patients and HCs (median = 6.66 vs. 10.11, p = 0.007). The total B cell count was compared between SjD patients and HCs (median = 267.50 vs. 164.50, p = 0.054).

Mann-Whitney test was used for comparisons of blood DN B cells between healthy controls (n = 36) and SjD patients (n = 70). Lower levels of DN B cells were detected in SjD patients than in healthy subjects.
Expression of DN B cells in disease activity index and clinical parameters of SjD patients
The percentages and absolute counts of DN B cells were compared between groups with or without various clinical manifestations and laboratory indicators (Table 2). In SjD patients, medium-high disease activity was defined as ESSDAI ≥ 5, and low disease activity as ESSDAI < 5. DN B cell percentages were lower in medium-high disease activity patients (2.75%) compared to those with low disease activity (4.05%) (p = 0.029; Table 2; Fig. 2B). Similar findings were observed in the absolute counts of DN B cells between moderate to high and low disease activity groups (median = 5.32 vs. 9.69, p = 0.000, Fig. 2C).

Comparative analysis of blood DN B cells in peripheral blood from different groups of SjD patients. B lymphocyte typing and identification process. B cell subsets were classified using anti-human murine monoclonal antibodies: anti-CD27-FITC, anti-CD19-PE-cy7, anti-CD24-PE, anti-IgD-PerCP, anti-CD38-BV421, anti-CD45-V500, and anti-CD20-APC-cy7. Total B cells were identified as CD19+, DN B cells as CD19 + CD27-IgD-, naïve B cells as CD19 + CD27-IgD+, memory B cells as CD19 + CD27 + IgD-, plasmablast cells as CD20-CD19 + CD27 + CD38hi, transitional B cells as CD19 + IgD + CD27-CD24brightCD38bright and B10-like cellsasCD19 + CD27 + CD24hi. (A) The percentage of DN B cells in different clinical and laboratory indicators of SjD patients. Compared with the percentage of DN B cells of 4.05% in low disease activity patients, a decrease in the percentage of DN B cells to 2.75% was observed in medium-high disease activity patients (p = 0.029). There was a statistically difference in the percentage of DN B cells between patients with and without glandular involvement (median = 2.15 vs. 3.55, p = 0.039). Furthermore, the percentage of DN B cells differed significantly between patients with and without neutropenia (median = 2.55 vs. 3.55, p = 0.034). (B) The absolute counts of DN B cells in different groups of SjD patients.The absolute counts of DN B cells were also observed in the presence or absence of xerophtalmia (median = 7.08 vs. 9.60, p = 0.008), general symptoms (median = 4.91 vs. 8.26, p = 0.024), hematological system (median = 7.34 vs. 10.37, p = 0.015), lymphopenia (median = 4.34 vs. 9.11, p = 0.000), and elevated CRP (median = 5.83 vs. 8.10, p = 0.026), respectively. Lower absolute counts of DN B cells were associated with an increased likelihood of xerophtalmia, general symptoms, lymphopenia and the higher level of CRP.
The percentage of DN B cells differed significantly between patients with and without glandular involvement (median = 2.15 vs. 3.55, p = 0.039). Additionally, there was a statistically difference in the percentage of DN B cells between patients with and without neutropenia (median = 2.55 vs. 3.55, p = 0.034, Fig. 2B). In Fig. 2C, the absolute counts of DN B cells were significantly lower in patients with xerophthalmia (median = 7.08 vs. 9.60, p = 0.008), general symptoms (median = 4.91 vs. 8.26, p = 0.024), hematological system involvement (median = 7.34 vs. 10.37, p = 0.015), lymphopenia (median = 4.34 vs. 9.11, p = 0.000), and elevated CRP (median = 5.83 vs. 8.10, p = 0.026), compared to those without these conditions, respectively. These findings indicate that lower absolute counts of DN B cells were associated with an increased likelihood of xerophthalmia, general symptoms, lymphopenia, and elevated CRP.
Regression analysis of Circulating B cell subsets in SjD patients
We performed a logistic regression analysis to examine whether B cell subsets participated in SjD occurrence (Table 3; Fig. 3) and found that DN B cells were negatively correlated with the occurrence of SjD (odds ratio, OR = 0.491, 95% CI:0.330–0.732, p = 0.000). Further linear regression analysis was conducted to assess the association between B cell subsets and SjD disease activity (Table 4; Fig. 4), and the results showed that DN B cells were negatively correlated with SjD disease activity (B=−0.240, 95% CI:−0.468 to −0.013, p = 0.039).

Logistic regression analysis of circulating B cells subsets for SjD. DN B cells were negatively correlated with the occurrence of SjD (odds ratio, OR = 0.491, 95% CI: 0.330–0.732, p = 0.000).

Linear regression analysis of circulating B cell subsets for ESSDAI in SjD. An inverse correlation was observed between the percentage of DN B cells and ESSDAI (B=−0.240, 95% CI:−0.468- −0.013, p = 0.039).
Correlation between DN B cells and other B cell subsets in SjD patients
We further analyzed correlations between DN B cells and other B cell subsets in SjD patients. We found that DN B cells showed a weak negative correlation with the percentage of total B cells (r = −0.266, p = 0.026; Table 5; Fig. 5). However, no significant associations were found between DN B cells and naïve B cells, memory B cells, Plasmablast B cells, or B10-like cells. We also measured the correlation between DN B cells and laboratory indicators in SjD patients. No significant associations were observed between DN B cells and age, neutrophils, lymphocytes, or CRP level.

Correlations of percentage of DN B cells with the other B cell subsets in SjD patients. DN B cells had a weak negative correlation with the percentage of B cells (of total lymphocyte) (r = −0.266, p = 0.026).
Discussion
B cells are lymphocytes that play a key role in adaptive immune responses. B cells produce high-affinity antibodies, generate immune memory, act as antigen-presenting cells, and secrete cytokines7,8,20,21. Most mature B cells are classified into naive B cells, memory B cells and DN B cells based on the presence of surface markers IgD and CD27. DN B cells account for about 5% of total B cells in healthy individuals22, but are potentially involved in many diseases, including various autoimmune diseases, infection and cancers11,12,13,18,23,24,25,26,27,28,29. DN B cells have dual roles, potentially producing antibodies and pro-inflammatory factors, while also suppressing immune responses13,25,26,29. Table 6 summarizes the frequency of DN B cells in different populations and their possible roles.
There is little literature on the frequency of DN B cells in treatment-naive SS patients. In this cross-sectional study, we observed a decrease in the percentage of circulating DN B cells in patients with SjD compared to healthy controls, and the absolute counts were similarly decreased. Since DN B cells may have a role in immune suppression13,24, a lower frequency of DN B cells was observed in patients with higher ESSDAI scores, despite an abundance of circulating B cells. The correlation between DN B cells and clinical indicators suggest that DN B cells may be involved in the pathogenesis of SjD.
Our study showed that DN B cells were at low levels in SjD patients. This result is consistent with previous studies that found the frequency of DN B cells in SjD was decreased compared to axial spondyloarthritis (axSpA) and healthy donors30. In addition, our regression analysis showed that DN B cells potentially acted as a “protective” factor in the pathogenesis of SjD. SjD is a prototypical B cell-mediated autoimmune disease characterized by the production of a variety of autoantibodies31. Therefore, we inferred that DN B cells may “consume” themselves in order to exert immunosuppressive function. We found a weak negative correlation between DN B cells and total B cells, suggesting that DN B cells may be involved in immunosuppression. Consistent with this result, Centuori SM et al. observed DN B cells was inversely correlated with classical matured B cells (IgD-CD27+) within tumor tissue of human non-small cell lung cancer (NSCLC)24,32.
DN B cells are present at elevated levels in the peripheral blood of patients with many autoimmune diseases12,13,25, especially in SLE, which has been reported the most28,33. Wei et al. pointed out that DN B cells were correlated with a history of lupus nephritis, multiple disease-specific antibodies and a high SLE disease activity score33. You et al. indicated DN B cells were positively correlated with 24-h urine protein excretion levels, but had no correlation with disease activity28. Interestingly, we found that DN B cells were inversely associated with disease activity in SjD patients. In addition to the higher ESSDAI, the more DN B cells needed to be “consumed” for immunosuppression, we hypothesized that part of DN B cells may be transferred to the gland to perform its biological function. A previous study found reduced DN B cells in blood and increased DN B cells in the gut, which implied that DN B cells were recruited from the blood to the gut in inflammatory bowel disease (IBD)26. Our study discovered that the SjD patients with gland involved had significantly lower DN B cells than those without gland involved. In the future, we will also outline the potential for conducting biopsies and paired analyses of gland and blood B cells in future research. Glandular pathology will be performed to confirm the expression of DN B cells and strengthen our conclusions regarding their role in glands. Taken together, these results indicate that DN B cells might migrate to the glands and play a role in SjD through their immunosuppressive function.
The relationship between DN B cells and SjD is sophisticated, and our study had some limitations. First, DN B cells are still less well studied and needed a unified name to define CD27– lgD– B cells. The absence of a unified name for CD27–lgD– B cells may cause confusion. Moreover, further studies are necessary to investigate the signaling pathways and cellular interactions through which DN B cells may exert immune effects. Furthermore, SjD is a heterogeneous disease that can be grouped according to different types of immunological profiles. DN B cells should be analyzed within different patient groups to better understand their role in the pathogenesis of SjD34. Third, we split Table 2 into multiple 2 × C contingency tables for pairwise comparisons, each comparison may produce its own type I error, which is inevitable. To control the overall type I error rate, Bonferroni correction should be applied to the significance level of each pairwise comparison. However, since we performed many comparisons, the adjusted significance level becomes very small. This may cause many important discoveries with small effect sizes, yet of great medical significance, to be missed. Therefore, to balance type I and type II errors, we did not perform Bonferroni correction based on clinical experience and literature reports. Fourth, we used the volume method to calculate the absolute count of B cell subsets. However, this method has certain limitations due to differences in sample processing between CBC and flow cytometry, as well as variations in handling whole blood samples for each technique.
In conclusion, this study demonstrates that DN B cells were decreased in SjD patients, particularly in those with glandular involvement and high disease activity. Decreased DN B cells inversely correlated with the total B cells. The correlation between DN B cells and clinical factors indicated that DN B cells may be involved in the pathogenesis of SjD. Further studies are needed to elaborate the function of DN B cells in SjD.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Cafaro, G. et al. One year in review 2019: Sjögren’s syndrome. Clin. Exp. Rheumatol. 37 (Suppl 118), 3–15 (2019).
Wu, J. et al. Clinical and laboratory features of primary Sjögren’s syndrome complicated with mild to severe thrombocytopenia. Ann. Transl Med. 10, 300. https://doi.org/10.21037/atm-22-162 (2022).
Cafaro, G., Gerli, R. & Bartoloni, E. Association between glandular infiltrate and leukopenia in Sjögren syndrome (SS): data from the Italian research group on SS (GRISS). J. Rheumatol. 47, 1840–1841. https://doi.org/10.3899/jrheum.200328 (2020).
Wen, W. et al. Clinical and serologic features of primary Sjögren’s syndrome concomitant with autoimmune hemolytic anemia: a large-scale cross-sectional study. Clin. Rheumatol. 34, 1877–1884. https://doi.org/10.1007/s10067-015-3081-0 (2015).
Brito-Zerón, P. et al. Systemic activity and mortality in primary Sjögren syndrome: predicting survival using the EULAR-SS disease activity index (ESSDAI) in 1045 patients. Ann. Rheum. Dis. 75, 348–355. https://doi.org/10.1136/annrheumdis-2014-206418 (2016).
Baldini, C. et al. Pathogenesis of Sjögren’s disease: one year in review 2024. Clin. Exp. Rheumatol. 42, 2336–2343. https://doi.org/10.55563/clinexprheumatol/i8iszc (2024).
Shen, P. & Fillatreau, S. Antibody-independent functions of B cells: a focus on cytokines. Nat. Rev. Immunol. 15, 441–451. https://doi.org/10.1038/nri3857 (2015).
Rastogi, I. et al. Role of B cells as antigen presenting cells. Front. Immunol. 13, 954936. https://doi.org/10.3389/fimmu.2022.954936 (2022).
Veenbergen, S., Kozmar, A., van Daele, P. L. A. & Schreurs, M. W. J. Autoantibodies in Sjögren’s syndrome and its classification criteria. J. Transl Autoimmun. 5, 100138. https://doi.org/10.1016/j.jtauto.2021.100138 (2022).
Huang, W. et al. The effect of anti-CD40 ligand antibody on B cells in human systemic lupus erythematosus. Arthritis Rheum. 46, 1554–1562. https://doi.org/10.1002/art.10273 (2002).
Colonna-Romano, G. et al. A double-negative (IgD-CD27-) B cell population is increased in the peripheral blood of elderly people. Mech. Ageing Dev. 130, 681–690. https://doi.org/10.1016/j.mad.2009.08.003 (2009).
Fraussen, J. et al. Phenotypic and Ig repertoire analyses indicate a common origin of IgD(-)CD27(-) double negative B cells in healthy individuals and multiple sclerosis patients. J. Immunol. 203, 1650–1664. https://doi.org/10.4049/jimmunol.1801236 (2019).
Yagi-Numata, N., Matsushita, T., Takehara, K. & Hamaguchi, Y. Increased expression levels of FcγRIIB on naïve and double-negative memory B cells in patients with systemic sclerosis. Clin. Exp. Rheumatol. 37 (Suppl 119), 23–31 (2019).
Hardt, U. et al. Integrated single cell and Spatial transcriptomics reveal autoreactive differentiated B cells in joints of early rheumatoid arthritis. Sci. Rep. 12, 11876. https://doi.org/10.1038/s41598-022-15293-5 (2022).
Ruschil, C. et al. Specific induction of double negative B cells during protective and pathogenic immune responses. Front. Immunol. 11, 606338. https://doi.org/10.3389/fimmu.2020.606338 (2020).
Jenks, S. A. et al. Distinct effector B cells induced by unregulated Toll-like receptor 7 contribute to pathogenic responses in systemic lupus erythematosus. Immunity 49, 725–739e726. https://doi.org/10.1016/j.immuni.2018.08.015 (2018).
Claes, N. et al. Age-Associated B cells with Proinflammatory characteristics are expanded in a proportion of multiple sclerosis patients. J. Immunol. 197, 4576–4583. https://doi.org/10.4049/jimmunol.1502448 (2016).
Shiboski, C. H. et al. American college of rheumatology/european league against rheumatism classification criteria for primary Sjögren’s syndrome: a consensus and data-driven methodology involving three international patient cohorts. Arthritis Rheumatol 69, 35–45 (2017). (2016). https://doi.org/10.1002/art.39859
Seror, R. et al. EULAR sjogren’s syndrome disease activity index: development of a consensus systemic disease activity index for primary sjogren’s syndrome. Ann. Rheum. Dis. 69, 1103–1109. https://doi.org/10.1136/ard.2009.110619 (2010).
Claes, N., Fraussen, J., Stinissen, P., Hupperts, R. & Somers, V. B. Cells are multifunctional players in multiple sclerosis pathogenesis: insights from therapeutic interventions. Front. Immunol. 6, 642. https://doi.org/10.3389/fimmu.2015.00642 (2015).
Pioli, P. D. Plasma Cells, the next generation: beyond antibody secretion. Front. Immunol. 10, 2768. https://doi.org/10.3389/fimmu.2019.02768 (2019).
Li, Y., Li, Z. & Hu, F. Double-negative (DN) B cells: an under-recognized effector memory B cell subset in autoimmunity. Clin. Exp. Immunol. 205, 119–127. https://doi.org/10.1111/cei.13615 (2021).
Eggers, E. L. et al. Clonal relationships of CSF B cells in treatment-naive multiple sclerosis patients. JCI Insight. 2 https://doi.org/10.1172/jci.insight.92724 (2017).
Centuori, S. M. et al. Double-negative (CD27(-)IgD(-)) B cells are expanded in NSCLC and inversely correlate with affinity-matured B cell populations. J. Transl Med. 16, 30. https://doi.org/10.1186/s12967-018-1404-z (2018).
Nakayamada, S. et al. Differential effects of biological DMARDs on peripheral immune cell phenotypes in patients with rheumatoid arthritis. Rheumatol. (Oxford). 57, 164–174. https://doi.org/10.1093/rheumatology/kex012 (2018).
Pararasa, C. et al. Reduced CD27(-)IgD(-) B cells in blood and Raised CD27(-)IgD(-) B cells in gut-associated lymphoid tissue in inflammatory bowel disease. Front. Immunol. 10, 361. https://doi.org/10.3389/fimmu.2019.00361 (2019).
Woodruff, M. C. et al. Extrafollicular B cell responses correlate with neutralizing antibodies and morbidity in COVID-19. Nat. Immunol. 21, 1506–1516. https://doi.org/10.1038/s41590-020-00814-z (2020).
You, X. et al. Double negative B cell is associated with renal impairment in systemic lupus erythematosus and acts as a marker for nephritis remission. Front. Med. (Lausanne). 7, 85. https://doi.org/10.3389/fmed.2020.00085 (2020).
Hopp, C. S. et al. Atypical B cells up-regulate costimulatory molecules during malaria and secrete antibodies with T follicular helper cell support. Sci. Immunol. 7, eabn1250. https://doi.org/10.1126/sciimmunol.abn1250 (2022).
Wilbrink, R. et al. CD27(-)CD38(low)CD21(low) B-Cells are increased in axial spondyloarthritis. Front. Immunol. 12, 686273. https://doi.org/10.3389/fimmu.2021.686273 (2021).
Brito-Zerón, P. et al. Sjögren syndrome. Nat. Rev. Dis. Primers. 2, 16047. https://doi.org/10.1038/nrdp.2016.47 (2016).
Chung, M. K. Y. et al. Functions of double-negative B cells in autoimmune diseases, infections, and cancers. EMBO Mol. Med. 15, e17341. https://doi.org/10.15252/emmm.202217341 (2023).
Wei, C. et al. A new population of cells lacking expression of CD27 represents a notable component of the B cell memory compartment in systemic lupus erythematosus. J. Immunol. 178, 6624–6633. https://doi.org/10.4049/jimmunol.178.10.6624 (2007).
Soret, P. et al. A new molecular classification to drive precision treatment strategies in primary Sjögren’s syndrome. Nat. Commun. 12, 3523. https://doi.org/10.1038/s41467-021-23472-7 (2021).
Acknowledgements
We thank the patients and staff of the 2nd hospital of Dalian Medical University, who have contributed data to the Sjögren’s syndrome Registry.
Funding
Liaoning Province Doctoral Scientific Research Startup Fund (No. NO.2025-BS-0684).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception. Lin Zhao, Jing Yang, Yida Xing and Xiaodan Kong designed the study, Changyan Liu and Mingxi Xu collected the data, Lin Zhao and Jing Yang analysed the data and wrote the manuscript; Yida Xing and Xiaodan Kong revised the manuscript. The authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhao, L., Yang, J., Liu, C. et al. Decreased IgD- CD27- double negative B cells in Sjögren’s disease correlated with disease activity index. Sci Rep 15, 35815 (2025). https://doi.org/10.1038/s41598-025-19796-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-19796-9
