
Abstract
Cardiovascular diseases (CVDs) have been the leading cause of death in China. Depression and anxiety are recognized as significant risk factors for poor prognosis and disability among Chinese CVD patients. However, these mental health conditions have received limited clinical attention in the context of CVD management. To date, comprehensive national epidemiological data on the prevalence of depression and anxiety in cardiovascular clinics (CVCs) in China are lacking. The present study aims to describe the prevalence, recognition and therapeutic inequity in CVCs so as to improve the overall health outcomes of CVD patients. A multicenter, cross-sectional study was conducted across secondary and tertiary hospitals in China (January 2021 to December 2022), enrolling 1049 CVD patients from CVCs consecutively. Depression and anxiety symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7), respectively. Sociodemographic and clinical data were collected via standardized questionnaires. Risk factors were analyzed by multivariable logistic regression, meanwhile recognition rates and treatment inequities were systematically evaluated. The pooled prevalence of depression and anxiety were 61.4% and 53.4% respectively, with 23.9% exhibiting moderate-to-severe symptoms. The multivariable logistic regression analyses disclosed that residing in South Central China, usual activities impairment, as well as experiencing pain or discomfort in daily life were associated with the presence of both depression and anxiety among patients in CVCs. Alarmingly, only 41.5% of depressed patients and 44.1% of anxious patients were recognized; and fewer than 50% accessed guideline-recommended interventions (psycho-education or medications). Patients residing in South Central China, having moderate or severe mental symptoms and having anxiety and depression comorbidity were more likely to be recognized and treated by cardiologists. This first national study to demonstrate the “high burden-low care” paradox in Chinese CVCs highlights systemic gaps in mental health integration. Urgent implementation of collaborative care models is warranted, prioritizing standardized screening protocols and equity-focused interventions for vulnerable subgroups. These findings provide pivotal evidence for advancing Chinese CVD clinical guidelines to address the mental health crisis in cardiology.
Trial registration: The trial was registered with ClinicalTrials.gov under the identifier NCT03225586 (Registration Date: 2017-07-19).
Similar content being viewed by others

Introduction
Cardiovascular diseases (CVDs) remain the leading cause of global mortality, accounting for approximately 20.5 million deaths in 2021, nearly one-third of all deaths worldwide1. Growing evidence underscores the bidirectional relationship between CVDs and mental health problems, driven by shared biological, genetic, and behavioral pathways2. Since the landmark 1972 study reporting a 65% prevalence of emotional distress in ischemic heart disease patients3, subsequent research has consistently demonstrated that depression and anxiety significantly exacerbate cardiovascular risks. For instance, major depressive disorder (MDD) increases the risk of cardiovascular morbidity and mortality by ~ 80%4, while anxiety disorders elevate coronary heart disease (CHD) risk by 26% and cardiac mortality by 48%5. In China, longitudinal studies have revealed similar trends, with hazard ratios for non-fatal myocardial infarction as high as 6.33 [95% CI: 2.96 ~ 13.79] and cardiac rehospitalization as high as 14.08 [95% CI: 4.99 ~ 41.66] among depressed comorbid anxiety patients over 1-year follow-up6,7. These findings highlight an urgent need to address mental health comorbidities in cardiovascular care to reduce premature mortality.
Cardiovascular clinics (CVCs), as the primary interface for CVD management, are critical hubs for early detection and intervention. There is substantial evidence indicating that patients with anxiety and depression often exhibit poor treatment adherence or responsiveness. This can result in unnecessary medical investigations and referrals, which may further exacerbate both the medical and financial burden on these patients8,9,10,11. Early recognition of depression and anxiety symptoms in patients can improve outpatient cardiac rehabilitation completion rates, thereby promising a better prognosis for CVDs12. While validated tools like the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7) are recommended for routine screening of depression and anxiety symptoms13,14,15,16,17, their adoption in China remains inconsistent, particularly in under-resourced regions. A meta-analysis of the prevalence of depression across various outpatient clinics in several countries revealed that the prevalence of depression in CVCs ranges from 19.7% to 31.0%18,19,20,21. However, systematic underrecognition of depression and anxiety persists globally. In the United States, over 50% of depressed patients remain undiagnosed in outpatient settings, with screening rates as low as 3%22,23. Similarly, the recognition rate of mental disorders among CVD patients in China is alarmingly low, with a depression recognition rate of 25.5% in tertiary general hospitals in a 2007 study and only 4% for depression and anxiety in primary hospitals in a 2010 study24,25. Beyond recognition, psychological interventions, including pharmacotherapy, psychotherapy, and exercise, have been shown to alleviate depressive and anxious symptoms, thereby enhancing the quality of life for individuals with CVDs26,27. However, even when recognized, treatment inequities persist: fewer than 11% of depressed CVD patients in U.S. cardiac units receive guideline-concordant care28, and similar barriers—awareness, medication access, and provider expertise—plague China’s healthcare system.
In response to these challenges, China has issued national guidelines emphasizing psycho-cardiological integration since 201029. In 2021, the mind-heart-body connection was further affirmed by the American Heart Association (AHA)30. Yet, no large-scale study has quantified the current burden of depression and anxiety in Chinese CVCs. This nationwide study aims to analyze the clinical characteristics and risk factors associated with depression and anxiety symptoms within the context of CVCs and to identify factors that influence the recognition and management of these conditions from the perspective of cardiologists in China. By doing so, this study may enhance doctors’ attention to depression and anxiety in outpatient settings, improve specialized training for cardiologists, and optimize the allocation of healthcare resources at both the regional and hospital levels. Ultimately, these efforts are expected to enhance the efficiency of healthcare delivery for patients with CVDs in China.
Method
Subjects and procedures
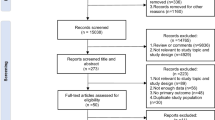
This cross-sectional study aimed to determine the prevalence of anxiety and depression among patients in CVCs. Ethical approval was granted by the ethics committees of all participating centers, and written informed consent was obtained from each participant. Initially, 1072 adults aged over 18 years visiting CVCs in secondary and tertiary hospitals were enrolled in the study. The exclusion criteria were applied to exclude individuals who met any of the following conditions: (1) Cardiogenic shock, (2) Recurrent chest pain with ECG ST-T changes, (3) A diagnosis of schizophrenia, (4) Communication impairments or dyslexia, (5) Cognitive impairment or organic brain diseases, (6) Acute left heart failure, (7) Seeking treatment unrelated to cardiovascular issues, (8) Solely seeking medication. Participants who failed to complete questionnaires, cooperate with the research, or provided inaccurate or significantly deviating survey responses were also excluded. After applying these exclusions, the final analysis included data from 1049 participants.
Investigators sequentially invited patients in the CVC awaiting consultation to participate in the survey. Written informed consent was obtained from the research subjects or their legal representatives, as well as the attending physicians, prior to the study’s commencement. Each participant completed a basic patient information questionnaire, the PHQ-9, the GAD-7, and the three-level EuroQol-5D scale (EQ-5D-3 L) on-site, as well as medical information, a process that typically took approximately 10 min.
The Case Report Form (CRF) was diligently filled out by the investigators, ensuring comprehensive documentation for each enrolled case. Following completion, the CRFs were meticulously reviewed by the research team, and data entry was carefully performed after the collection of all samples.
All researchers involved in sample collection received comprehensive training on the specified collection methods. The research team regularly monitored the collected samples to ensure their accuracy and integrity. Post data entry, a random selection of forms was subjected to a rigorous examination to assess input quality, detect any potential issues, and implement necessary corrections.
Assessment instrument
-
(1)
Patient Basic Information Questionnaire: A self-designed questionnaire was utilized to elicit comprehensive patient demographics and background information. Essential details encompassed initials of the name and contact information, while demographic data comprised gender, age, ethnicity, height, weight, educational background, occupational status, average monthly family income, and marital status.
-
(2)
Medical History and Diagnostic Medication (completed by the attending physician): This section captures pertinent patient information including their status as an outpatient or inpatient, duration of CVDs, type of CVDs, cardiac symptoms, prevalent risk factors, and lifestyle considerations. It delineates the diagnosis rendered by the physician and the corresponding prescribed medications. The previous and current diagnoses of depression or anxiety by cardiologists in CVCs were collected and compared against the findings from the current questionnaire. The recognition rate was subsequently calculated based on this comparison. Furthermore, it documents whether guidance pertaining to psycho-therapeutic interventions was imparted during this outpatient visit, with options including psycho-education, treatment with traditional Chinese medicine, Western medicine, combination of Western and Chinese medicine, and treatment not provided. The hospital level and the region in which the hospital is located were also recorded. The 20 provinces are divided into six regions: North China (Beijing, Tianjin, Hebei, Shanxi), East China (Shandong, Jiangsu, Shanghai, and Zhejiang), Central and South China (Henan, Hubei, Hunan, Guangdong, and Guangxi), Northeast China (Liaoning, Heilongjiang, and Inner Mongolia), West China (Gansu, Sichuan, Yunnan, and Chongqing).
-
(3)
PHQ-9: Each response is scored as follows: Not at all (0 points), Several days (1 point), More than half the days (2 points), and Nearly every day (3 points). Cumulative scores range from 0 to 27. Interpretation of scores is as follows: 0–4, absence of depression; 5–9, potential mild depression; 10–14, possible moderate depression; 15–19, potential moderate to severe depression; and 20–27, a likelihood of major depressive disorder (MDD). For the purposes of this study, we categorized both moderate to severe and MDD as indicative of severe depression symptoms15.
-
(4)
GAD-7: Responses are scored as follows: Not at all (0 points), Several days (1 point), More than half the days (2 points), and Nearly every day (3 points). Total scores range from 0 to 21. Interpretation of scores is as follows: 0–4, absence of anxiety; 5–9, potential mild anxiety; 10–13, possible moderate anxiety; 14–18, potential moderate to severe anxiety; and 19–21, a likelihood of severe anxiety. For the purposes of this study, we classified both moderate to severe and severe anxiety as indicative of severe anxiety14.
-
(5)
EQ-5D-3L Assessment: This instrument gauges the patient’s health utility value. Comprising two components, the EQ-5D health description system encompasses five dimensions: mobility, self-care ability, daily activity ability, pain or discomfort, and anxiety or depression. Each dimension comprises three levels: no difficulty, some difficulty, and extreme difficulty. The EQ-5D index value is derived through the conversion of the responses into a weighted health-stateindex. A higher EQ-5D index represents a better health status of the patient. For this investigation, the utility value conversion specific to Japan, as provided on the official website of EQ-5D (https://euroqol.org/), was utilized for computation31,32.
Statistical analysis
All data analyses and plots will be presented using R (version 4.3.1). Data conforming to a normal distribution will be statistically summarized using mean ± standard deviation (SD) and 95% confidence intervals (CI). Between-group comparisons will be conducted using the t-test, while comparisons among multiple groups will be assessed using one-way analysis of variance (ANOVA). For non-normally distributed data, statistical description will be based on median and quartile distances, with inter-group comparisons evaluated via the Chi-square test for percentage. And Fisher exact probabilities were calculated when necessary. Multivariate logistic regression analyses were performed for examining risk factors of depression/anxiety. A significance level of p < 0.05 will be applied for all analyses.
Results
Baseline profiles of patients
A total of 1,049 consecutive patients were recruited from CVCs located in secondary- and tertiary-level hospitals across five Chinese regions. The cohort comprised 572 men (54.5%), 299 middle-aged adults (28.5%), and 659 elderly adults (62.8%), with a mean age of 62.96 ± 12.86 years. Comprehensive sociodemographic and clinical characteristics are presented in Table 1.
Overall, 61.4% of participants screened positive for depressive symptoms and 53.4% for anxiety symptoms; the majority of cases were mild in severity. Both conditions were most prevalent in Northeast China and least prevalent in East China. Patients attending tertiary hospitals demonstrated significantly higher rates of depression and anxiety than those seen in secondary hospitals (p < 0.05).
Chest distress was the most frequently reported symptom (87.5%), followed by chest pain (60.7%) and palpitations (52.4%). Dyspnea, although present in only 27.0% of the entire sample, was markedly over-represented among patients with depression (74.6%) and anxiety (67.1%).
Depression and anxiety were significantly more common among individuals with heart failure (HF), myocardial infarction (MI), coronary heart disease (CHD), metabolic disorders (diabetes and dyslipidemia), and cerebrovascular disease (all p < 0.05). The highest prevalence was observed in patients with HF (depression, 80.4%; anxiety, 66.4%), followed by those with MI (74.6% and 64.0%, respectively).
Risk factors of depression or anxiety in patients attending CVCs
Advanced age conferred a modest but significant protective effect against depression (OR = 0.71; 95% CI, 0.52–0.98; p = 0.037), whereas female sex was associated with a higher risk of anxiety (OR = 1.35; 95% CI, 1.00-1.82; p = 0.048). Unemployment was associated with an 84% elevation in anxiety risk (OR = 1.84; 95% CI, 1.09–3.14; p = 0.023).
Relative to East China, residence in South Central China was associated with a 2.08-fold increase in depression risk and a 2.45-fold increase in anxiety risk. Residence in Northeast China conferred a nearly two-fold elevation in anxiety risk only (OR = 1.99; 95% CI, 1.28–3.11; p = 0.002). Attending tertiary hospitals was associated with a 2.15-fold increase in depression risk compared with attending secondary hospitals (OR = 2.15; 95% CI, 1.33–3.49; p = 0.002).
Among quality-of-life dimensions, impaired mobility increased the odds of depression (OR = 1.76; 95% CI, 1.12–2.80; p = 0.016), whereas limitations in usual activities heightened the risk of both depression (OR = 1.92; 95% CI, 1.27–2.92; p = 0.002) and anxiety (OR = 1.52; 95% CI, 1.03–2.24; p = 0.034). Self-reported pain or discomfort emerged as the strongest predictor for both depression (OR = 2.62; 95% CI, 1.89–3.65; p < 0.001) and anxiety (OR = 3.33; 95% CI, 2.38–4.69; p < 0.001).
With respect to somatic symptoms, fatigue was significantly associated with depression (OR = 1.52; 95% CI, 1.11–2.10; p = 0.010), whereas chest distress (OR = 1.59; 95% CI, 1.02–2.50; p = 0.042) and palpitations (OR = 1.68; 95% CI, 1.24–2.28; p < 0.001) were independently associated with anxiety. Among comorbidities, dyslipidemia conferred a significant increase in depression risk (OR = 1.42; 95% CI, 1.02–1.96; p = 0.034), and previously undiagnosed cardiovascular disease was associated with a 2.43-fold elevation in anxiety risk (OR = 2.43; 95% CI, 1.14–5.27; p = 0.029). Complete multivariable effect estimates are presented in Table 2.
Recognition of anxiety/depression symptoms in CVCs
Only 41.5% of patients with depression and 44.1% of those with anxiety were formally identified. Recognition varied markedly by region: South Central China achieved the highest rates (depression, 56.1%; anxiety, 58.4%), whereas East China recorded the lowest (depression, 25.4%; anxiety, 25.2%). Tertiary hospitals under-performed secondary hospitals in detecting both conditions (depression, 40.0% vs. 55.7%, p = 0.025; anxiety, 42.0% vs. 63.2%, p = 0.004). Comprehensive recognition rates across regions and hospital levels are provided in Suppl. Tables S1 and S2. Recognition increased monotonically with symptom severity (p < 0.001). Notably, the co-occurrence of depression and anxiety was more readily identified (46.6%) than either symptom in isolation (isolated depression, 24.7%; isolated anxiety, 25.8%; p < 0.001). Detailed data are presented in Table 3.
Treatment of anxiety/depression symptoms in CVCs
Overall, 44.3% of patients with depressive symptoms and 45.5% of those with anxiety symptoms received any treatment (Table 4). The specific modalities were psycho-education (8.5%), traditional Chinese medicine (17.6%), Western medicine (4.2%), and combined Chinese-Western medicine (6.7%).
Marked regional heterogeneity was evident: South Central China recorded the highest treatment rates (50.8%), whereas East China reported the lowest (22.4%) (Suppl. Figure S1). Treatment modality varied by age group; psycho-education was most common in young adults (17.6%), declining to 9.7% in middle-aged and 6.7% in elderly participants. Conversely, use of traditional Chinese medicine increased with age (young adults, 7.7%; middle-aged, 19.1%; elderly, 18.4%).
Patients with comorbid depression and anxiety were more likely to receive treatment than those with isolated depression or anxiety (47.4% versus 34.0% and 31.8%, respectively; p < 0.001). Across all diagnostic subgroups, traditional Chinese medicine was preferred to Western pharmacotherapy (only depression: 19.3% vs. 6.0%; only anxiety: 10.6% vs. 3.0%; comorbidity: 23.7% vs. 9.3%; p < 0.001). Treatment rates did not differ significantly between tertiary and secondary hospitals (Suppl. Figure S2).
Discussion
This study delivers an updated, nationally representative profile of depression and anxiety among Chinese CVCs, integrating contemporary prevalence estimates, risk factors, and recognition and treatment patterns, while providing direct comparisons across different regions and hospital levels. The observed prevalence of depressive symptoms (61.4%) and anxiety symptoms (53.4%) substantially exceeds the rates reported in earlier investigations33,34,35,36, underscoring an escalating burden of affective disorders in this population. Regional heterogeneity persists: the highest prevalence of both depression and anxiety was documented in Northeast and South Central China, whereas East and West China exhibited comparatively lower rates. This temporal increase may be attributed to rapid socioeconomic transformation, urbanization, and concomitant psychosocial stressors24,37; the additional psychological sequelae of the COVID-19 pandemic warrant dedicated investigation. Moreover, prior research has demonstrated that affective symptoms were significantly more prevalent among outpatients than inpatients24, emphasizing the imperative to prioritize mental-health assessment and intervention within CVCs.
Previous investigations have examined depression and anxiety separately among patients with CHD, MI, hypertension, and those undergoing percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG)38,39. However, data comparing the prevalence of these affective disorders across the entire spectrum of CVD remain scarce, particularly in China. The present study addresses this evidence gap by demonstrating a high prevalence of comorbid depression and anxiety in CVD, exceeding 60% in patients with HF or MI. Undiagnosed cardiovascular disease independently predicted anxiety, corroborating earlier findings that fear of an unknown cardiac condition substantially elevates anxiety levels40. Consistent with prior observations—where 42% of chest-pain patients in CVCs reported anxiety and 31% reported depression19—our results indicate that specific somatic symptoms exhibit distinct associations with affective disorders. Fatigue was more strongly linked to depression, whereas chest distress and palpitations were more indicative of anxiety, thereby clarifying the relationship between typical cardiac symptoms and psychiatric morbidity. Individuals with depression engage less frequently in physical activity (e.g., walking, gardening, strenuous exercise)41,42,43,44, a behavioral pattern that may predispose to dyslipidemia. Consequently, dyslipidemia emerged as a clinically accessible marker for depression in this population. Together, these findings equip cardiologists with an evidence-based framework for the early recognition of affective disorders in CVD patients, especially in those presenting with multiple or atypical symptoms.
Prior North American studies have reported recognition rates for depression and anxiety in CVCs ranging from 20% to 40%45,46,47. In 2008, a study conducted in six general hospitals in Guangzhou, China, identified only 9.7% of depressed and 12.6% of anxious patients48. In the present nationwide cohort, recognition has improved markedly—to 41.5% for depression and 44.1% for anxiety—reflecting substantial advances in Chinese psycho-cardiology over the past two decades. This progress is plausibly attributable to the nationwide dissemination of expert consensus statements and the systematic implementation of “double-heart” training programs for cardiologists49. Notwithstanding these gains, recognition remains suboptimal in tertiary hospitals, possibly because their clinical priorities favour complex cardiovascular interventions over routine mental-health screening. Substantial regional inequities also persist: South Central China consistently outperforms other regions, underscoring the influence of socioeconomic and cultural determinants on care delivery. These findings emphasize the urgent need for targeted capacity-building initiatives that encompass all hospital levels and economically disadvantaged regions to ensure uniform, effective identification and management of depression and anxiety in CVD patients.
Psychological interventions in CVCs encompass psycho-education, behavioral management, traditional Chinese medicine, and antidepressant medications; these modalities are endorsed by both national guidelines and international psycho-cardiological consensus statements50. Lu et al. previously reported a depression treatment rate of only 9.5% in Chinese CVCs between 2012 and 201551. In the present nationwide cohort, treatment rates for depression and anxiety have risen to approximately 50%, substantially exceeding earlier figures. This improvement may be attributed to the publication of the Chinese Expert Consensus on Psychological Prescriptions for patients with CVD, as well as the implementation of training courses in fundamental psychological skills for cardiologists in China50. Marked geographic heterogeneity persists. South Central China, characterised by more rapid socioeconomic development, demonstrated the highest treatment rates, whereas economically disadvantaged regions lagged behind. These disparities underscore the necessity of region-specific, culturally adapted mental-health strategies for CVD patients. Notably, 40.7% of participants with depression symptoms and 40.1% with anxiety symptoms exhibited mild severity that did not fulfil formal diagnostic criteria14. Among these mild cases, treatment rates were 39.8% and 40.4%, respectively. Given that two-thirds of these patients also reported concurrent cardiovascular symptoms (e.g., chest distress, dyspnea, palpitations), misattribution and suboptimal management remain concerns. Both the “Recommendations from the Chinese Consensus of Standard Psycho-Cardiology Clinics” and the “Psychological Health, Well-Being, and the Mind-Heart-Body Connection: A Scientific Statement from the American Heart Association” emphasize that mild depression and anxiety in CVD can be effectively managed with psycho-education or behavioral interventions, leading to improved cardiovascular outcomes, mental health, and quality of life29,30. Consequently, cardiologists should maintain heightened vigilance for even sub-threshold psychological symptoms in this population.
This study further demonstrates that Chinese cardiologists exhibit a pronounced preference for traditional Chinese medicine in the management of depression and anxiety among patients with CVDs whereas psycho-education is comparatively underutilised. In accordance with current guidelines, psycho-education constitutes the recommended first-line intervention for mild affective disorders in this population; given the high proportion of mild depression and anxiety observed in Chinese CVCs, greater emphasis on structured psycho-education is warranted. Although prior studies have provided preliminary evidence supporting the efficacy of specific traditional Chinese medicine formulations in mild-to-moderate depression and anxiety52,53, rigorous, large-scale clinical trials are required to validate their safety and effectiveness specifically in CVD patients. Conversely, the prescription of Western pharmacotherapy rose incrementally with symptom severity but remained below 10% even in severe cases. This limited utilisation, coupled with infrequent referral to mental-health specialists, underscores a critical gap in cardiologists’ training and highlights the pressing need for enhanced educational initiatives and integrated care pathways.
Limitation
The mentioned results should be considered under the light of several limitations. First, the assessment was done at 121 subcenters across 20 provinces. Therefore, the possibility of variation between subcenters exists. However, all participating subcenters completed a standardized assessment process before the study, and stringent quality control procedures were used during the study. Second, we only used self-report questionnaires for depression and anxiety assessment. However, the inventories are highly reliable and have strong construct validity from prior research, as described in the introduction and methods. Additionally, this study was designed to simulate the process of rapid screening for anxiety and depressive symptoms in the CVC to provide cardiologists with premise for initial treatment and referrals to the psychological department. Therefore, self-report measures were used to facilitate the assessment of a sample of CVCs. Third, behavioral risk profiles, especially smoking and drinking habits, were not included in the regression analysis. However, some comorbidities (e.g., dyslipidemia and diabetes) were included in the regression analysis, which to some extent reflected the impact of lifestyle habits. Finally, the cross-sectional design of the study makes any inference of a causal relationship between mental health and predictors weak.
Conclusion
This study highlights the substantial mental-health burden among Chinese CVCs and underscores the urgent need for systematic integration of psycho-cardiology into routine clinical practice. Implementation of level-specific training curricula—emphasizing advanced diagnostic algorithms in tertiary hospitals—should be prioritized. Concurrently, eliminating regional inequities, enhancing cardiologists’ competencies, and proactively managing mild cases are likely to improve patient-centred outcomes and attenuate long-term healthcare expenditures.
Future investigations should adopt longitudinal designs to delineate the bidirectional relationship between CVD progression and mental-health trajectories. Priority research agendas include (i) comparative effectiveness analyses of clinical outcomes in recognized versus unrecognized cases, and (ii) rigorous evaluation of the relative efficacy of structured psycho-education versus traditional Chinese medicine in patients with mild depression or anxiety.
Data availability
Data is provided within the manuscript.
References
Roth, G. A. et al. Global burden of cardiovascular diseases and risk Factors, 1990–2019. J. Am. Coll. Cardiol. 76 (25), 2982–3021. https://doi.org/10.1016/j.jacc.2020.11.010 (2020).
Goldfarb, M. et al. Severe mental illness and cardiovascular disease. J. Am. Coll. Cardiol. 80 (9), 918–933. https://doi.org/10.1016/j.jacc.2022.06.017 (2022).
Cay, E. L., Vetter, N., Philip, A. E. & Dugard, P. Psychological status during recovery from an acute heart attack. J. Psychosom. Res. 16 (6), 425–435. https://doi.org/10.1016/0022-3999(72)90068-2 (1972).
Penninx, B. W. J. H. Depression and cardiovascular disease: epidemiological evidence on their linking mechanisms. Neurosci. Biobehav Rev. 74 (Pt B), 277–286. https://doi.org/10.1016/j.neubiorev.2016.07.003 (2017).
Roest, A. M., Martens, E. J., de Jonge, P. & Denollet, J. Anxiety and risk of incident coronary heart disease: a meta-analysis. J. Am. Coll. Cardiol. 56 (1), 38–46. https://doi.org/10.1016/j.jacc.2010.03.034 (2010).
Meng, R. et al. Association between depression and All-cause and cardiovascular mortality in Chinese adults. JAMA Netw. Open. 3 (2), e1921043. https://doi.org/10.1001/jamanetworkopen.2019.21043 (2020).
Wu, M. et al. Anxiety and depression prevalence and risk factors among patients with cardiovascular diseases in Post-COVID-19 China. Front. Public. Health. 9, 758874. https://doi.org/10.3389/fpubh.2021.758874 (2021).
Zigmond, A. S. & Snaith, R. P. The hospital anxiety and depression scale. Acta Psychiatr Scand. 67 (6), 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x (1983).
Benjenk, I. & Chen, J. Effective mental health interventions to reduce hospital readmission rates: a systematic review. J. Hosp. Manag Health Policy. 2, 45. https://doi.org/10.21037/jhmhp.2018.08.05 (2018).
Moffic, H. S. & Paykel, E. S. Depression in medical in-patients. Br. J. Psychiatry J. Ment Sci. 126, 346–353. https://doi.org/10.1192/bjp.126.4.346 (1975).
Maguire, G. P., Julier, D. L., Hawton, K. E. & Bancroft, J. H. Psychiatric morbidity and referral on two general medical wards. Br. Med. J. 1 (5902), 268–270. https://doi.org/10.1136/bmj.1.5902.268 (1974).
Edwards, B. L. & Sydeman, S. J. Depression is associated with reduced outpatient cardiac rehabilitation completion rates: A SYSTEMATIC LITERATURE REVIEW AND META-ANALYSIS. J. Cardiopulm. Rehabil Prev. 39 (6), 365–372. https://doi.org/10.1097/HCR.0000000000000419 (2019).
Siu, A. L. et al. Screening for depression in adults: US preventive services task force recommendation statement. JAMA 315 (4), 380–387. https://doi.org/10.1001/jama.2015.18392 (2016).
Stocker, R. et al. Patient health questionnaire 9 (PHQ-9) and general anxiety disorder 7 (GAD-7) data contributed by 13,829 respondents to a National survey about COVID-19 restrictions in Australia. Psychiatry Res. 298, 113792. https://doi.org/10.1016/j.psychres.2021.113792 (2021).
Levis, B. et al. Accuracy of the PHQ-2 alone and in combination with the PHQ-9 for screening to detect major depression: systematic review and Meta-analysis. JAMA 323 (22), 2290. https://doi.org/10.1001/jama.2020.6504 (2020).
Schutt, P. E., Kung, S., Clark, M. M., Koball, A. M. & Grothe, K. B. Comparing the Beck depression Inventory-II (BDI-II) and patient health questionnaire (PHQ-9) depression measures in an outpatient bariatric clinic. Obes. Surg. 26 (6), 1274–1278. https://doi.org/10.1007/s11695-015-1877-2 (2016).
Yuan, J. et al. Screening for depression in acute coronary syndrome patients: A comparison of patient health Questionnaire-9 versus hospital anxiety and depression Scale-Depression. J. Psychosom. Res. 121, 24–28. https://doi.org/10.1016/j.jpsychores.2019.03.018 (2019).
Wang, J. et al. Prevalence of depression and depressive symptoms among outpatients: a systematic review and meta-analysis. BMJ Open. 7 (8), e017173. https://doi.org/10.1136/bmjopen-2017-017173 (2017).
Rohani, A., Akbari, V. & Zarei, F. Anxiety and depression symptoms in chest pain patients referred for the exercise stress test. Heart Views Off J. Gulf Heart Assoc. 12 (4), 161–164. https://doi.org/10.4103/1995-705X.90903 (2011).
Hajduk, A., Nowicka-Sauer, K., Smoleńska, Ż., Czuszyńska, Z. & Zdrojewski, Z. Prevalence and correlates of suicidal thoughts in patients with neuropsychiatric lupus. Lupus 25 (2), 185–192. https://doi.org/10.1177/0961203315603136 (2016).
ling He, Y. et al. yuan. [A cross-sectional survey of the prevalence of depressive-anxiety disorders among general hospital outpatients in five cities in China]. Zhonghua Nei Ke Za Zhi. 48 (9), 748–751 (2009).
Bhattacharjee, S., Goldstone, L., Vadiei, N., Lee, J. K. & Burke, W. J. Depression screening Patterns, Predictors, and trends among adults without a depression diagnosis in ambulatory settings in the united States. Psychiatr Serv. Wash. DC. 69 (10), 1098–1100. https://doi.org/10.1176/appi.ps.201700439 (2018).
Davis, K. A. S., Sudlow, C. L. M. & Hotopf, M. Can mental health diagnoses in administrative data be used for research? A systematic review of the accuracy of routinely collected diagnoses. BMC Psychiatry. 16, 263. https://doi.org/10.1186/s12888-016-0963-x (2016).
Song, W. X. et al. A survey of the prevalence of depression and anxiety disorders among patient attendees with cardiovascular disease in primary hospitals. J. Chongqing Med. Univ. 37 (10), 911–913. https://doi.org/10.3969/j.issn.0253-3626.2012.10.018 (2012).
Liu, C. et al. Prevalence and recognition of depressive disorder in three medical outpatient departments of general hospitals in Beijing, China. J. Nerv. Ment Dis. 204 (7), 537–541. https://doi.org/10.1097/NMD.0000000000000531 (2016).
Pedersen, S. S. et al. Internet-Delivered, Therapist-Assisted treatment for anxiety and depression in patients with cardiovascular disease: Evidence-Base and challenges. Curr. Cardiol. Rep. 25 (6), 443–453. https://doi.org/10.1007/s11886-023-01867-w (2023).
Jha, M. K., Qamar, A., Vaduganathan, M., Charney, D. S. & Murrough, J. W. Screening and management of depression in patients with cardiovascular disease. J. Am. Coll. Cardiol. 73 (14), 1827–1845. https://doi.org/10.1016/j.jacc.2019.01.041 (2019).
Huffman, J. C. et al. A collaborative care depression management program for cardiac inpatients: depression characteristics and In-Hospital outcomes. Psychosomatics 52 (1), 26–33. https://doi.org/10.1016/j.psym.2010.11.021 (2011).
Psychosomatic Medicine Society of the Chinese Medical Association,Cardiovascular Disease Prevention and Rehabilitation Committee of Chinese Association of Rehabilitation Medicine et al. Chinese expert consensus on the construction standardization of Psycho-cardiology outpatient. Chin. Gen. Pract. 27 (03), 253–261. https://doi.org/10.12114/j.issn.1007-9572.2023.0499 (2024).
Levine, G. N. et al. Psychological Health, Well-Being, and the Mind-Heart-Body connection: A scientific statement from the American heart association. Circulation 143 (10), e763–e783. https://doi.org/10.1161/CIR.0000000000000947 (2021).
Yao, Q., Liu, C., Zhang, Y. & Xu, L. Population norms for the EQ-5D-3L in China derived from the 2013 National health services survey. J Glob Health 11:08001. https://doi.org/10.7189/jogh.11.08001
Zare, F., Ameri, H., Madadizadeh, F. & Aghaei, M. R. Validity and reliability of the EQ-5D-3L (a generic preference-based instrument used for calculating quality-adjusted life -years) for patients with type 2 diabetes in Iran. Diabetes Metab. Syndr. Clin. Res. Rev. 15 (1), 319–324. https://doi.org/10.1016/j.dsx.2021.01.009 (2021).
Yuan, L. X., Ding, R. J., Qin, Y. P., Wu, B. Q. & Qi, R. X. Survey on the current status of common anxiety, depression and somatization symptoms among patients in cardiovascular specialist hospitals. J. Southeast. Univ. (Med Sci. Edi). 39 (5), 608–614. https://doi.org/10.3969/j.issn.1671-6264.2020.05.010 (2020).
Banlan, Y. I., Shu, D. & Hao, X. A study of mood disorders and their influencing factors in cardiology patients in tertiary hospitals and primary hospitals. Chin. J. Clin. Psychol. 30 (03), 645–649. https://doi.org/10.16128/j.cnki.1005-3611.2022.03.029 (2022).
Meng, R. et al. Association of depression with All-Cause and cardiovascular disease mortality among adults in China. JAMA Netw. Open. 3 (2), e1921043. https://doi.org/10.1001/jamanetworkopen.2019.21043 (2020).
Shang, X. et al. Incidence of Medication-Treated depression and anxiety associated with Long-Term Cancer, cardiovascular Disease, diabetes and osteoarthritis in Community-dwelling women and men. EClinicalMedicine 15, 23–32. https://doi.org/10.1016/j.eclinm.2019.08.010 (2019).
Ivanovs, R. et al. Association of depression and anxiety with cardiovascular co-morbidity in a primary care population in latvia: a cross-sectional study. BMC Public. Health. 18 (1), 328. https://doi.org/10.1186/s12889-018-5238-7 (2018).
Wells, A. et al. Improving the effectiveness of psychological interventions for depression and anxiety in cardiac rehabilitation. Circulation 144 (1), 23–33. https://doi.org/10.1161/CIRCULATIONAHA.120.052428 (2021).
Lai, M. et al. Clinical outcomes and survival analysis in patients with psycho-cardiological disease: a retrospective analysis of 132 cases. J. Int. Med. Res. 49 (3), 030006052199098. https://doi.org/10.1177/0300060521990984 (2021).
Li, Y. et al. The degree of anxiety and depression in patients with cardiovascular diseases as assessed using a mobile app: Cross-Sectional study. J. Med. Internet Res. 25, e48750. https://doi.org/10.2196/48750 (2023).
Anda, R. F. et al. Depression and the dynamics of smoking. A National perspective. JAMA 264 (12), 1541–1545. https://doi.org/10.1001/jama.1990.03450120053028 (1990).
Penninx, B. W. et al. Effects of social support and personal coping resources on depressive symptoms: different for various chronic diseases? Health Psychol. 17 (6), 551–558. (1998).
Stephens, T. Physical activity and mental health in the united States and canada: evidence from four population surveys. Prev. Med. 17 (1), 35–47. https://doi.org/10.1016/0091-7435(88)90070-9 (1988).
DiMatteo, M. R., Lepper, H. S. & Croghan, T. W. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 160 (14), 2101–2107. https://doi.org/10.1001/archinte.160.14.2101 (2000).
Huffman, J. C. et al. Recognition and treatment of depression and anxiety in patients with acute myocardial infarction. Am. J. Cardiol. 98 (3), 319–324. https://doi.org/10.1016/j.amjcard.2006.02.033 (2006).
Glassman, A. H. et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 288(6), 701-709
Lespérance, F. et al. Effects of Citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian cardiac randomized evaluation of antidepressant and psychotherapy efficacy (CREATE) trial. JAMA 297 (4), 367. https://doi.org/10.1001/jama.297.4.367 (2007).
Ye, R. et al. Correlation analysis of somatic symptoms with anxiety and depression in outpatients of cardiology department. Lingnan J. Cardiovasc. Disease. 19 (01), 48–51. https://doi.org/10.3969/j.issn.1007-9688.2013.01.013 (2013).
Li, X., Zhou, J., Wang, M., Yang, C. & Sun, G. Cardiovascular disease and depression: a narrative review. Front. Cardiovasc. Med. 10, 1274595. https://doi.org/10.3389/fcvm.2023.1274595 (2023).
Cardiovascular Disease Committee of the Chinese Rehabilitation Society, Specialized Committee on Cardiovascular and Cerebrovascular Diseases of the Chinese Gerontological Society. Chinese medical association psychosomatic medicine branch. Chinese expert consensus on psychological prescription for patients in cardiovascular department (2020 edition). Chin. J. Intern. Med. 59 (10), 764–771. https://doi.org/10.3760/cma.j.cn112138-20200203-00050 (2020).
Lu, J. et al. Prevalence of depressive disorders and treatment in china: a cross-sectional epidemiological study. Lancet Psychiatry. 8 (11), 981–990. https://doi.org/10.1016/S2215-0366(21)00251-0 (2021).
Liu, Q. et al. Xinkeshu tablets promote angiogenesis in zebrafish embryos and human umbilical vein endothelial cells through multiple signaling pathways. J. Ethnopharmacol. 314, 116636. https://doi.org/10.1016/j.jep.2023.116636 (2023).
Ma, Q. et al. Mingmu Xiaoyao granules regulate the PI3K/Akt/mTOR signaling pathway to reduce anxiety and depression and reverse retinal abnormalities in rats. Front. Pharmacol. 13, 1003614. https://doi.org/10.3389/fphar.2022.1003614 (2022).
Acknowledgements
The authors thank all study participants for their time and effort.
Funding
This study received a grants from Beijing Natural Science Foundation (No. 2108000050) and was funded by National High Level Hospital Clinical Research Funding 2023-PUMCH-E-005.
Author information
Authors and Affiliations
Contributions
D.R.J. designed the study protocol. L.Y.Y., Y.S.C., L.P.Z., Y.G.L., W.W.X., W.D.D., L.W., W.H.Y., Z.M.T., Z.P.Q., Z.Y.L., Z.F.H. conducted data collection. C.R. conducted data management, cleaning. C.R. wrote the first draft of the paper. D.R.J. and C.R. substantially revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained from all participants. The procedures were carried out in accordance with the Declaration of Helsinki. Ethical approval for this study was also obtained from the ethics committee of the Peking University Research Ethics Service (2021-PHB181-001).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, R., Liu, Y., Yang, S. et al. The prevalence, recognition, and treatment of depression and anxiety symptoms among Chinese cardiovascular outpatients. Sci Rep 15, 36798 (2025). https://doi.org/10.1038/s41598-025-20683-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-20683-6
