
Abstract
Parkinson’s disease (PD) is not a single condition and has multiple heterogeneous presentations with several endophenotypes as well as collateral factors affecting care and health. However, clinical consultations globally often miss these important aspects in clinic. The Stepped Care pathway of care was developed from PD patients’ opinion and attempts to combine these gaps in care in a simple 3-stage clinical paradigm. We conducted a survey across twenty (20) countries to explore the views of clinicians and PD patients on the process, acceptability and need of the Stepped Care pathway. A structured questionnaire was administered in both affluent and under-resourced clinics, capturing data from a multi-ethnic and diverse patient base. 99% patients (White, Asian and Black) felt Stepped Care toolkit asked relevant questions addressing needs and concerns in PD care that are often missed, and 96% agreed with the importance of using this toolkit during Outpatient Clinic visits. Moreover, a significant majority of PD patients (96%) felt Stepped Care makes them understand their condition better. 92% of clinicians indicated that the Stepped care toolkit could be an effective asset in clinical practice, while 91% of clinicians agreed that the toolkit provides holistic care which is often missed in clinic. This novel global survey of the efficacy and useability of Stepped Care for PD is overwhelmingly endorsed by PD patients and clinicians from a diverse, multi-ethnic background across high- and low- income countries. Stepped Care can be used in clinical practice in order to ensure a holistic and comprehensive care for PD.
Similar content being viewed by others

Introduction
Parkinson’s disease (PD) is a neurodegenerative disorder primarily caused by degeneration of the pars compacta of the substantia nigra1,2. However, PD is a complex, multifaceted syndrome involving at least four distinct neurotransmitter systems- dopaminergic, cholinergic, noradrenergic, and serotonergic- affected by oligomeric α-synuclein and other pathologies3,4,5. These disruptions contribute to the diverse motor and non-motor symptoms (NMS) of PD and may underpin recently described cholinergic, noradrenergic and serotonergic subtypes of PD, as well as natural history patterns5,6. Several PD non-motor subtypes are now recognized, each dominated by dysfunction in specific neurotransmitter systems, further reinforcing the notion that PD is a syndromic disorder with highly variable clinical presentations3,5,7,8,9. Others suggest that PD is a systemic condition with manifestations that extend beyond the classical motor manifestations10.
Given this complexity, effective PD management needs to adopt a holistic approach from the outset, addressing both motor and non-motor subtypes and, more importantly, many “collateral” symptoms often not addressed in clinic. A “one size fits all” reliance on purely dopaminergic therapies is inadequate. To tackle this challenge, a clinical prompt based toolkit, the Stepped Care, which incorporates clinical motor and non-motor assessments, subtyping and the use of the Chaudhuri dashboard for PD has been developed, the latter identifying key “vitals” for personalized patient care11,12,13. An international survey revealed significant gaps in the recognition and management of these vitals- such as gut, bone, and vision health, as well as comorbidities and use of polypharmacy- despite their substantial impact on PD clinical outcomes and quality of life (QoL)14. The clinical impact of not following Stepped Care in clinic may range from poor oral levodopa response, to fractures, as well as possible worsening of cognition and sudden onset of sleep events at work or while driving15.
To address this critical gap in care, we created the Stepped Care pathway and toolkit for PD management, designed for global applicability, including resource-limited settings11. The primary objective of this study was to evaluate whether the Stepped Care toolkit can be effectively used in clinical settings, irrespective of healthcare resource availability which includes manpower resources as well as time constraints. We canvassed the views of relevant stakeholders (HCPs and PD patients) and additionally, this international survey aimed to assess stakeholders’ views on the practical use of the toolkit in clinic as well as it’s efficiency and usability in the management of PD. Our ultimate goal is to establish a concise, clinically valuable toolkit that comprehensively addresses all aspects of PD, enabling its integration into everyday practice.
With the global rise in PD cases, particularly in underserved regions of Asia and Africa, addressing these care gaps is increasingly urgent16,17. Studies have shown significant health discrepancies and health inequality between countries and income groups regarding PD care and research18,19,20. The proposed Stepped care toolkit can be applied anywhere globally. In this paper, we present data from 20 countries, including low-resource clinics, evaluating the suitability, usability, and efficacy of the Stepped Care toolkit in real-world clinical settings as evaluated by health care professionals (HCPs) and PD patients.
Methods
Objective
The primary objective is to assess the logistics and acceptability of the clinical and practical use of the Stepped Care toolkit in clinical settings. We have aimed to achieve this by performing a questionnaire survey of patients and clinicians across 20 countries of varying health care facilities and resources. This questionnaire survey aimed to assess stakeholders’ views on the toolkit’s efficiency and usability in the management of PD.
Setting
In this global, cross-cultural, multicentre survey, HCPs, including physician consultants, physician trainees, and PD nurses from 20 countries were included. For parity, we included participants from Western affluent countries as well as those from developing countries such as Egypt, South Africa (SA), India, Malaysia and Chile based on assignment of low, middle and high income country status by the World Bank. Centres were chosen based on experience in using nonmotor profiling in patients, those who took part in the preceding survey to address gaps in care of PD in clinics15 and those who have been part of previous collaborative work in nonmotor aspects of PD and previous studies of the PD nonmotor group.
The toolkit
The Stepped care toolkit was first developed after several consultations with expert patient groups, caregivers, and a review of related literature addressing holistic care in PD and was based on the concept of personalised medicine for PD. Expert patient groups included the CRISP group as well as Movers and Shakers, a publicly well-known expert patient group of PD patients running a highly successful global podcast21. Stepped care and use of the “dashboard” for PD is specifically mentioned in their podcast called “Pumps” (Pumps–Movers and Shakers: a podcast about life with Parkinson’s – Apple Podcasts) which was aired on 30 Nov 202422. Each centre familiar with the care and management of PD patients presented the proposed “Stepped care toolkit” to HCP, patients and their caregivers. Surveys were then conducted among the participants to assess the real-life useability of the toolkit. Figure 1 Where required, the concept and questions were explained to the patients in their local language, as has been done in many previous cognitive pre-test studies, such as during the validation of SCOPA and PD nonmotor symptoms scales24,25,26 .
The “Stepped care toolkit” consists of a 3-step process. Step 1 includes the assessment of motor function, non-motor symptoms, motor fluctuations, dyskinesias, and gait disturbances using simple yet validated tools such as the Hoehn and Yahr stage developed in the 1960’s and still widely used as well as the globally used PD nonmotor questionnaire (NMSQuest)24. Step 2 is optional and identifies disease subtypes (cholinergic, sleep subtype, autonomic/noradrenergic, or overlap syndromes) using the NMSQuest as an anchor and subdomain analysis (Fig. 2). If a subtype can be assigned then subtype specific therapies can be considered27. Step 3 focuses on attention to three key health vitals or domains contained in the published dashboard for PD and include : vitals 3: gastrointestinal assessment, vision, oral health ; vital 4: bone health and frailty and vital 5 evaluating co-medications and comorbidity focusing mainly on anticholinergic use and its risk of aggravating cognitive problems as well as impulse control disorders in addition to noting relevant comorbidities such as diabetes. (Appendix) The toolkit relies on some well used clinical scales and standard scoring systems apply although this is not essential as the scorings are only relevant if one wants to validate the subtypes in a future research study. For example, we have proposed scoring for a combined grading of PD ( motor and nonmotor symptoms ) based in the proposal by Martinez-Martin26 while in Fig. 2 we show how specific items flagged in subdomains of the NMSQuest as part of Step 1 could aid in clinical recognition of some of the nonmotor subtypes. This system is likely to ensure that key symptoms are not overlooked and that medications are appropriately chosen, avoiding significant interactions. The pathway to the development of the entire “Stepped care toolkit” is shown in Fig. 1 and is based on the concept of personalised medicine for PD, non-motor subtyping and subtype specific management of PD supported by patient feedback27,26.

A diagram of the pathway followed in the survey data collection regarding Stepped Care.

A proposed flow chart showing the practical clinical real-life application of Stepped Care pathway in the clinic using the Parkinson’s disease Non-Motor Symptoms questionnaire (NMSQ) as an anchor. Specific self-flagged symptoms could trigger screening for specific subtypes. P and LF test: Pentagon copy and Lexical fluency test. MOCA = Montreal Cognitive Assessment. * = optional tests if available locally, GBA1 = pathogenic glucocerebrosidase mutation, RBDSQ = Rapid eye movement behaviour disorder screening questionnaire, KPPS/KPPQ = Kings Parkinson pain scale and questionnaire, NA = Noradrenergic, PET = Positron emission tomography, PSG = Polysomnography, MSLT = Multiple sleep latency test, Mx = measurement. ESS = Epworth Sleepiness Scale.
Data collection
Firstly, verbal informed consent about this good clinical practice-based survey was obtained from all study participantsstudy participantss and we followed the methodology adopted by the Parkinson’s disease nonmotor group (PDNMG) who led global validation of the PD nonmotor symptoms questionnaire24 and scale25 both adopted by the International Parkinson’s disease and movement disorders society. In this evaluation process, HCPs completed a seven-point scoring questionnaire, which noted their current position and clinical environment, including the time allocated for patient visits and the support they received from other team members. The pre-test questions for participants included whether the Stepped Care toolkit was relevant to their daily practice and if it reflected their current clinical practice. Participants were also asked if the Stepped care plan, provided as a “prompt” during clinic visits, would help them deliver more comprehensive care for patients. Furthermore, they were asked if the questions in the toolkit covered essential aspects of PD assessment and care, whether the questions and plan were too lengthy, and if all the questions and intended actions were easy to understand. Lastly, they were asked if any questions or actions needed to be completed or answered and whether they would like to use the Stepped Care prompt/pathway in their clinic Similar questions were posed to patients in these clinics where they were asked if the scale was relevant to their needs and whether it helped them better understand their or others’ current health status with PD. Additionally, they were asked if the toolkit assessed the critical aspects of the disease comprehensively.
Statistical analysis
Data analysis included descriptive statistics of the respondents’ characteristics and the items composing the Stepped Care Toolkit questionnaire. It also analysed clinician pre-testing questions and the time to respond to the questionnaire. Frequency and percentages were used for categorical variables, while mean and standard deviation (SD) were applied to continuous variables. Data reported in this study are exploratory findings of an uncontrolled, observational study. No sample size calculation was or could be performed; therefore, the findings and p-values are not intended to be interpreted with confirmatory intent. Categorical data are presented by frequency and the percentage of available data.
Ethical approval
The study was part of the ongoing nonmotor symptoms in PD longitudinal cohort study (NILS, UKCRN The NILS study was authorised by local ethics committees NRES Southeast London REC, 10084, 10/H0808/141) and was specifically approved by the Research Ethics Committee at Poznan University, the main coordinating centre for Stepped Care in PD (792/24). All individual centres discussed the survey with local relevant ethics committee as well.
The survey based data collection involving human patients were performed in accordance with the Declaration of Helsinki and all methods were performed in accordance with the relevant guidelines and regulations.
Results
Data from our international multicentre survey were collected from 20 countries. Two hundred-six physicians and seventy-two patients and caregivers participated. Clinical and motor and non-motor assessments data for patients are shown in Table 1. Data were collected in anonymised fashion and human participants’ names and other HIPAA identifiers were removed. Centres were identified by a prefix and number (example: Poznan was POZ 1).
SD standard deviation
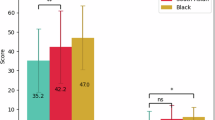
Among the patients, there were 72 patients (mean age 62.7 ± 9.9 years (range 39–85 years) ; 37.5% were Caucasian, 33.3% were Asian, 13.9 were Asian Chinese, and 15.3% were black, suggesting we included a reasonably diverse patient population base. The majority (45.1%) were at a moderate to severe stage of PD, and most had a mild to moderate NMS burden (Table 1). From the patient and caregiver perspective, 99% reported that the toolkit’s questions were relevant, addressing their specific needs and concerns in PD care. Additionally, 96% of patients and caregivers underscored the importance of the toolkit’s pathway, emphasising its role in providing consistent and effective care (Table 2).
Among the physicians, 38% were movement disorder specialists, and 46% were general neurologists. The average clinic consultation time per PD patient ranged from 20 min (34%) to 30 min (36%). 92.2% of all clinicians surveyed indicated that the Stepped care toolkit could be effectively used as a prompt in clinical practice to improve the delivery of comprehensive care for patients with PD Table 3. Furthermore, 91.7% of clinicians agreed that the toolkit adequately covers all essential aspects of PD assessment and management that should be addressed in a clinic.
Specifically, most respondents (86.4%) found the questions and recommended actions in the toolkit straightforward and easy to understand and implement. Although 32.5% noted that the tool was somewhat lengthy, 56.8% considered the format robust and effective. 77.7% thought the questions were easy to comprehend and address (Table 3). 33.5% were interested in implementing the Stepped care toolkit in the clinic, while 47.6% were very interested although these were additional questions posed.
Discussion
In this paper we present a patient and clinician perception of the use of the Stepped Care toolkit in real life PD clinic in a global setting. The study is inclusive in the sense our patient cohort is equitably distributed between white and Asian study participants as well as including a reasonable proportion of black PD patients. Lack of Asian and Black PD patients in clinical trials, population health studies and surveys has been a focus of much attention lately, highlighting the issue of health care inequity. 19 Additionally, we sought stakeholder and user input from a wide range of physicians, including movement disorder specialists and general neurologists with a survey including participants from 20 countries.
The data suggests an overwhelming endorsement of use the Stepped care pathway in clinics, from those in well-resourced teaching hospital clinics to under-resourced busy clinics in low-income countries. This underpins the global appeal of this approach, which is simple, yet clinically validated, and can be supported, if applicable, by relevant laboratory and imaging tests. The fact that 99% of the patients find the Stepped care questions relevant to clinical practice and 86% did not have any further comments suggests a high acceptability rate in the examined population of PD patients. Our patient base was not only racially diverse, but also well-distributed in terms of motor stage (ranging from mild to severe, Table 1) and non-motor burden (ranging from mild to very severe). Consequently, the views expressed on Stepped Care use in the clinic was not biased towards a specific severity subgroup of PD patients and could be applied across various stages. A very similar view is also expressed by clinicians across all countries surveyed with 91% reporting that Stepped care questions were relevant to their clinical practice. In 28% responses from clinicians it was evident that this pathway was not in use in local clinics and this is reassuring as the expectation was that this figure would be higher.
What then might be the clinical implications of adopting the Stepped care pathway in clinical practice? The Stepped care toolkit addresses both motor and non-motor aspects of PD using simple, validated assessments and questions that add minimal time to consultations in addition to addressing key “collateral” history crucial for wellbeing in PD and other chronic conditions28. A key angle to Stepped care is also to assign PD non-motor subtyping as far as possible by simple use of the motor and non-motor strategies and then additional embellishments as required and shown in a flowchart in Fig. 2. While effective subtyping is not possible on all occasions, a combined motor and non-motor burden grading, as it is proposed in Stepped Care after step1, allows a comprehensive care package to be developed23. We are mindful that inspite of strong endorsement of the pathway by clinicians some may find the process to be too long to be implemented in a busy clinic. However, we emphasise that final implementation of stepped care is based on the clinical decision of the clinician in consultation with the patients and the pathway can be adapted and shortened as required. Moreover, the relevant activation of the dashboard as indicated in Fig. 2 allows a comprehensive delivery of personalised modern care encompassing dopaminergic, non-dopaminergic, non-pharmacological and lifestyle related care and completion of other steps may not be required in clinic if time constraints apply24. Simple tests, such as the lexical fluency and pentagon copy, could signpost the cholinergic subtype, while screening with the Epworth Sleepiness Scale may help identify the “Park-sleep” subtype. This latter subtype may carry special sensitivity to dopamine D3 receptor agonists which may trigger “sleep attacks” with potentially dangerous consequences if the patient is still driving11,12,27.
There are of course limitations to this proposed pathway, Clinicians may still find the process time consuming while symptoms such as urinary problems, sexual dysfunction, skin changes, thermoregulatory problems are not specifically addressed. However, as part of stepped care pathway, the NMSQuest is used in Step 1 and this questionnaire would address some of these nonmotor symptoms.
Now that we have completed a global survey of this pathway, the next step would be to assess the impact of using this pathway in clinical care across several clinics and address healthcare resource utilisation. Our a priori hypothesis would be that the adoption of Stepped Care would lead to more efficient personalised care and, potentially, to the avoidance of preventable health problems in PD, such as poor oral levodopa efficacy, problems of sudden onset of sleep at work, or missing patients with osteoporosis putting them at higher risk of fractures. The pathway is also especially relevant to subtypes as anticholinergic drugs with high anticholinergic index, for instance should be avoided in the cholinergic subtype of PD while in Park-sleep, one should avoid certain dopamine agonists. The global endorsement of Stepped Care highlights the wide acceptance of this pathway in clinical care across racial and geographical boundaries. Additional benefits of adopting this toolkit-empowered pathway are that the non-motor subtyping would allow for genuine subtype-specific care, as well as creating a “trial ready” cohort for relevant and bespoke clinical trials, including studies on pain, sleep dysfunction, and cognition in PD. Holistic care of Parkinson’s disease (PD), encompassing direct care as well as comorbidities, including gut, vision, oral, bone health, and comedication history, is a global unmet need resulting in impaired patient care. A combined grading of motor and nonmotor function can also be completed as has been documented previously25. This global, multi-ethnic survey was conducted to solicit PD patients’ and clinicians’ views on the use of the Stepped Care pathway which aims at addressing this gap. This survey of PD patients and clinicians from 20 countries provides evidence for the first time that the Stepped Care pathway for PD can be globally used in diverse patient populations across rich and poor countries and will empower patients to understand their own health needs. We expect Stepped Care to be adopted by national policy making bodies, such as the UK NICE guidelines for Parkinson’s disease, national guidelines for Parkinson’s management across the world and in Europe as well as empower prominent patient groups to ask for Stepped Care in clinic. Our findings suggest that both HCPs and patients view the toolkit as a valuable asset, despite concerns from some clinicians regarding the length of the questions and the development of the pathway. The next stage of this work, where Stepped Care is implemented and its impact on care is measured, would address this issue. Currently, however, we recommend adoption and use of the Stepped Care pathway as far as possible in clinics addressing care for PD. The Stepped Care protocol is shown in Appendix 1.
Data availability
The data reflects patient and clinician views from 20 different countries and also is anonymised. The countries are ruled by different data protection laws and hence raw data share is not possible because all patients have not specifically consented to their data being shared in open journal public platform. If required, the anonymised data used for statistical analysis can be provided by corresponding author for perusal.
References
Jankovic, J. Parkinson’s disease: clinical features and diagnosis. J Neurol. Neurosurg Psychiatry. 79, 368–376 (2008).
Hughes, A. J., Daniel, S. E., Kilford, L. & Lees, A. J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry. 55, 181–184 (1992).
Titova, N., Padmakumar, C., Lewis, S. J. G. & Chaudhuri, K. R. Parkinson’s: a syndrome rather than a disease? J. Neural Transm (Vienna. 124, 907–914 (2017).
Jellinger, K. A. Neuropathology of sporadic Parkinson’s disease: evaluation and changes of concepts. Mov. Disord. 27, 8–30 (2012).
Schapira, A. H. V., Chaudhuri, K. R. & Jenner, P. Non-motor features of Parkinson disease. Nat. Rev. Neurosci. 18, 435–450 (2017).
Jankovic, J. & Tan, E. K. Parkinson’s disease: etiopathogenesis and management. J. Neurol. Neurosurg. Psychiatry. 91, 795–808 (2020).
Ray Chaudhuri, K., Leta, V., Bannister, K., Brooks, D. J. & Svenningsson, P. The noradrenergic subtype of Parkinson disease: from animal models to clinical practice. Nat. Rev. Neurol. 19, 333–345 (2023).
Tall, P. et al. The park sleep subtype in Parkinson’s disease: from concept to clinic. Expert Opin. Pharmacother. 24, 1725–1736 (2023).
Bohnen, N. I. et al. Cholinergic system changes in Parkinson’s disease: emerging therapeutic approaches. Lancet Neurol. 21, 381–392 (2022).
Adams, B. et al. Parkinson’s disease: a systemic inflammatory disease accompanied by bacterial inflammagens. Front. Aging Neurosci. 11, 210 (2019).
Popławska-Domaszewicz, K., Falup-Pecurariu, C. & Chaudhuri, R. An overview of a stepped-care approach to modern holistic and subtype-driven care for Parkinson’s disease in the clinic. TouchREVIEWS Neurol. 20, 27–32 (2024).
Chaudhuri, K. R., Titova, N., Qamar, M. A., Murăan, I. & Falup-Pecurariu, C. The dashboard vitals of Parkinson’s: not to be missed yet an unmet need. J. Pers. Med. 12, 1994 (2022).
Qamar, M. A. et al. Chaudhuri’s dashboard of vitals in Parkinson’s syndrome: an unmet need underpinned by real life clinical tests. Front. Neurol. 14, 1174698 (2023).
Qamar, M. A. et al. TheDashPD-Consortium: Importance of addressing bone health and anticholinergics to achieve holistic care in Parkinson’s. Eur. J. Neurol. 31(suppl. 1), 95–96 (2024).
K. Poplawska-Domaszewicz et al. The international validation of the “Stepped Care” toolkit for comprehensive real life clinical care: bridging massive unmet need in care of Parkinson’s disease. [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/the-international-validation-of-the-stepped-care-toolkit-for-comprehensive-real-life-clinical-care-bridging-massive-unmet-need-in-care-of-parkinsons-disease/. Accessed October 11, 2025. (2024).
Ou, Z. et al. Global trends in the incidence, prevalence, and years lived with disability of Parkinson’s disease in 204 countries/territories from 1990 to 2019. Front. Public. Health. 9, 776847 (2021).
Ben-Shlomo, Y. et al. The epidemiology of Parkinson’s disease. Lancet 403, 283–292 (2024).
Goh, Z. H. K. et al. Surveying global availability of Parkinson’s disease treatment. J. Parkinsons Dis. 12, 1023–1034 (2022).
Lau, Y. H. et al. Does ethnicity influence recruitment into clinical trials of Parkinson’s disease? J. Parkinsons Dis. 12, 975–981 (2022).
Metta, V. et al. First two-year o bservational exploratory real-life clinical phenotyping and societal impact study of Parkinson’s disease in Emiratis and expatriate population of United Arab Emirates 2019–2021: the empark study. J. Pers. Med. 12, 1300 (2024).
Qamar, M., Rizos, A., Stones, L., Meachin, C. & Chaudhuri, K. R. Public and patient involvement (PPI) at King’s: community for research involvement and support for people with Parkinson’s (CRISP). Advances in clinical neuroscience & rehabilitation: ACNR 16, 17–20 (2016).
Movers and Shakers: A Podcast About Life with Parkinson’s Podcast — Apple Podcasts. Accessed 5 Jan 2025 (2025).
Chaudhuri, K. R. et al. A proposal for a comprehensive grading of parkinson’s disease severity combining motor and non-motor assessments: meeting an unmet need. PLoS One. 8, e57221 (2013).
Chaudhuri, K. R. et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: the NMSQuest study.Mov Disord. 21(7), 916–9 23 (2006). https://doi.org/10.1002/mds.20844.
Chaudhuri, K. R. et al. The metric properties of a novel non-motor symptoms scale for Parkinson’s disease: results from an international pilot study. Mov. Disord. 22, 1901–1911 (2007).
Martinez-Martin, P. & Ray Chaudhuri, K. Comprehensive grading of Parkinson’s disease using motor and non-motor assessments: addressing a key unmet need. Expert Rev. Neurother. 18 (1), 41–50 (2018). Epub 2017 Nov 7. PMID: 29090594.
Marras, C., Chaudhuri, K. R., Titova, N. & Mestre, T. A. Therapy of Parkinson’s disease subtypes. Neurotherapeutics 17, 1366–1377 (2020).
Neubauer, K. et al. Taking a collateral history: the missing piece of the puzzle. BMJ 382, e076462 (2023).
Acknowledgements
We acknowledge research and philantropic support from Raghuvinder Kataria Foundation. KRC and KPD acknowledges philanthropic support from the Saivansh Chopra Endowment Fund.
Author information
Authors and Affiliations
Contributions
KPD, KRC : conception, design, acquisition, interpretation, review, writingCRB: analysis and interpretation LB, VL, IB, AS, HD, VM, PMM, PO, AA, IS, MRV, AS, MC, WJ, JC, AR, CP, YHL, CFP, TL, HB, DU, GL, CS, WK, SM,. AP, RvC, DT, JS, ADL, SG, KLK, CLO, YT, MGK, NM, VG, RM, SM, SBA, LKP, SD, CS, RB: the acquisition, analysis, review and interpretation of data and review.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Poplawska-Domaszewicz, K., Rodriguez-Blazquez, C., Boura, I. et al. An international 20 country patient and physician survey of the usability and acceptability of Stepped Care pathway in Parkinson’s disease. Sci Rep 15, 39774 (2025). https://doi.org/10.1038/s41598-025-23465-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-23465-2
