
Abstract
Depression represents a challenging neuropsychiatric issue following strokes and conceptualized as a network of individual symptoms that could affect each other in network theory. Clinical characteristics of depression are influenced by mutuality of stroke survivors and their spouses. No relevant research has examined the structure of depression network and how mutuality is related to depression among Chinese stroke survivors. This study aimed to investigate the structure of the depression network model, identify the pivotal symptoms influencing depression and explore the nodes that bridge depression and mutuality among Chinese stroke survivors. A sample of 847 stroke survivors in Henan Province, China, were invited to complete a survey that included the Patient Health Questionnaire (PHQ-9) and the 15-item Mutuality Scale (MS), which assessed depressive symptoms and mutuality, respectively. Results indicated that within the network of depressive symptoms, sadness (PHQ2) emerged as the central symptom. Getting help from spouse (MS6), attachment relationship (MS5), and concentration (PHQ7) were identified as the pivotal nodes bridging the connection between mutuality and depressive symptoms. Conversely, suicide ideation (PHQ9) and sleep disorders (PHQ3) were among the symptoms demonstrating the lowest predictability, indicating that their variance was less likely influenced by other depressive symptoms within the network. This is among the first studies investigating the inter-relationships between mutuality and depressive symptom from the network approach. Our findings provide an empirically-based perspective on the significance of dyadic interventions, with potential clinical implications for alleviating depressive symptom among stroke survivors.
Similar content being viewed by others

Introduction
Stroke represents one of the most prevalent global health concerns, with an estimated 12.2 million new cases and 101 million existing cases in 2019, contributing significantly to clinical and economic burdens across numerous countries1. The incidence of stroke in developing regions is high and has notably surged over the years in China2. In China, for instance, there was an 86% rise in annual stroke incidences between 1990 and 2019, resulting in an estimated 3.94 million new cases1. Depression emerges as the most prevalent and weighty neuropsychiatric complication following a stroke, exerting detrimental effects on functional recovery and rehabilitation outcomes3. It significantly impairs social engagement, diminishes quality of life, and poses risks such as suicide and increased mortality rates4,5,6. Globally, around one-third of stroke survivors experience depression7, while in China, a meta-analysis reported that approximately 34.9% of stroke survivors are affected by this condition8. To mitigate the risks associated with depression and offer timely and effective interventions, a comprehensive understanding of the underlying psychopathological mechanisms driving depression in stroke survivors is imperative.
Traditionally, depression has been perceived as a syndrome with shared underlying causes. This conventional approach utilizes standardized scales that evaluate the presence of diverse depressive symptoms and generate a cumulative score indicating the severity of depression. However, this method assumes that depressive symptoms are interchangeable manifestations of the same disorder9, neglecting the crucial distinctions between distinct symptoms and their interconnections. In contrast, network analysis approaches, considered novel statistical methodologies, regard mental health issues as systems comprising interconnected symptoms that can potentially influence each other during the progression toward a disorder10,11. The network analysis method (NAM) constructs a network of symptoms, representing them as nodes, and delineates their relationships, determining core and bridge symptoms within this network structure based on centrality indicators (such as mediation, proximity, and intensity)12. Core symptoms denote those strongly linked to other symptoms; addressing them may trigger downstream effects on other symptoms, potentially deactivating the entire network12,13. Bridge symptoms, on the other hand, exhibit robust connections between different parts of the network; treating these symptoms could sever pathways between disorders, potentially improving prognosis by disconnecting the progression from one disorder to another12,14,15.
Network analysis has been employed to investigate the depressive symptoms of stroke survivors in certain Western nations16,17. However, the manifestations and clinical features of depression are profoundly shaped by environmental and socioeconomic factors, resulting in considerable heterogeneity across different populations. In Chinese populations, post-stroke depression commonly manifests as a blend of emotional, cognitive, and somatic symptoms, such as low mood, fatigue, and sleep disturbances18,19. Additionally, influenced by Confucian values that emphasize emotional restraint and discourage open expression of psychological distress, many individuals do not actively report or even avoid discussing emotional symptoms20. In contrast, stroke survivors in Western contexts are generally more inclined to articulate their psychological experiences and tend to exhibit more pronounced affective and cognitive symptoms, including excessive guilt, hopelessness, and suicidal ideation21,22, frequently accompanied by substance use disorders23. Therefore, examining the network structure of depressive symptoms within distinct cultural and socioeconomic contexts is crucial for capturing symptom variability and informing the development of culturally tailored interventions11. Most studies scrutinizing the network structure of depression have been conducted in Western settings, limiting the generalizability of their findings to China. Hence, the primary objective of this study is to unravel the structure of the depression symptom network and its key characteristics among Chinese stroke survivors.
In the realm of stroke nursing, mutuality holds particular significance24 and is strongly linked to depression25. Mutuality represents the positive rapport between caregivers and the individuals under their care, reflecting the favorable quality of the relationship between patients and caregivers26,27. Comprising dimensions like love and affection, pleasurable activities, shared values, and reciprocity, mutuality serves as a crucial supportive resource aiding patients in coping with their condition and fostering mental well-being28,29. Previous research has explored the connection between mutuality and depression among patients with stroke, chronic heart failure, and Parkinson’s disease, with findings suggesting that higher levels of mutuality are associated with reduced depression in patients27,30,31. However, most existing studies have relied on regression analysis, considering the overall depression score as the unit of analysis. This approach overlooks the specific points at which mutuality impacts depression—namely, which dimensions of mutuality influence particular symptoms of depression, thereby influencing the overall depression network. Hence, the secondary aim of this study is to explore the specific interactions between mutuality and depression symptoms among stroke survivors using network analysis methods. This approach aims to identify the precise contact points where mutuality influences depression symptoms, thereby providing a foundation for targeted clinical interventions.
Methods
Study participants
This cross-sectional study was conducted between August 2021 and June 2023 in Henan Province, China. Convenience sampling was used, and data were collected from the inpatient departments of three tertiary hospitals: the Second Affiliated Hospital of Zhengzhou University, the Fifth Affiliated Hospital of Zhengzhou University, and the Luoyang Central Hospital Affiliated to Zhengzhou University. Stroke survivors meeting specific criteria were included in the study, which encompassed the following criteria: (a) aged 18 years or older; (b) met the diagnostic criteria for cerebrovascular disease and were diagnosed with cerebral infarction or cerebral hemorrhage by head computed tomography or magnetic resonance imaging; (c) were able to sufficiently comprehend and communicate in Chinese; and (d) demonstrated willingness to participate in the study and provided informed consent. Participants were excluded if they met any of the following criteria: (a) presence of cognitive impairment or mental illness; (b) suffering from severe complications; and (c) participation in other ongoing research studies.
Measurements
Mutuality scale
The Mutuality Scale, comprising 15 items, was utilized to assess the perceived mutuality existing between patients and their spousal caregivers. Originally developed by Archbold et al32. in 1990, this scale encompasses four dimensions: love and affection, sharing joy, common values, and reciprocity. Respondents rate items on a 5-point Likert scale ranging from 0(representing “not at all”) to 4 (representing “a great deal”). The total score attainable on this scale ranges from 0 to 75, with higher scores indicating a stronger sense of mutuality between the individuals. In this study, the Mutuality Scale was adapted for use in the Chinese context by Shyu et al33., demonstrating robust reliability and validity in previous research within the Chinese population24,33. Specifically, in the current study, the Cronbach’s alpha coefficient for internal consistency reliability was calculated to be 0.95, indicating high reliability of the scale’s measurements in this particular context.
Patient health Questionnaire-9
The Chinese iteration of the Patient Health Questionnaire (PHQ-9), as used in this study, was employed to evaluate depressive symptoms experienced over the preceding two weeks34. Participants rated items on a 4-point Likert scale, ranging from 0 (indicating “not at all”) to 3 (indicating “nearly every day”). The total score obtainable on the PHQ-9 spans from 0 to 27, with higher scores indicating more pronounced and severe depressive symptoms. Extensive validation studies have confirmed the reliability and validity of the PHQ-9 within Chinese populations35. In the context of this specific study, the Cronbach’s alpha coefficient, which measures internal consistency reliability, was calculated to be 0.88, indicating a high level of reliability in assessing depressive symptoms using the PHQ-9 among the study participants.
Ethics approval and consent to participate
The study was approved by the Zhengzhou University Life Science Ethics Committee (approval number: ZZUIRB2021-124) and was performed in accordance with guidelines and regulations as stated in the Declaration of Helsinki. A formal approval letter was obtained and submitted to all three participating hospitals. Written informed consent was obtained from all patients who agreed to participate in the study.
Data collection
Team members received detailed training about this cross-sectional study and familiarized themselves with the data collection instruments in advance. Subsequently, the team members introduced the objective of the survey to the patients and asked whether they were willing to participate. Written informed consent was obtained before they filled out the questionnaires. The patients completed the questionnaires anonymously and returned them on the spot. Data were collected from August 2021-June 2023.
Statistical analysis
Network Estimation
The analysis of networks involves nodes representing individual symptoms and edges denoting relationships between these symptoms. To visualize these relationships effectively, we utilized the Fruchterman-Reingold algorithm, which arranges nodes based on their strong connections, bringing closely linked nodes closer to each other in the network visualization. For conducting the network analysis, we employed the R-package qgraph. The estimation of regularized partial correlation networks was accomplished using the graphical least absolute shrinkage and selection operator (LASSO) method, a technique that diminishes false-positive associations and identifies the genuine network structure by reducing insignificant correlations to zero. This process was detailed by Epskam et al36.. The qgraph function cor_auto automatically detects the variable types and computes appropriate correlations, such as Pearson, polychoric, or polyserial correlations, for the analysis.
The estimation of the network structure utilized the EBICglasso procedure, which determines the optimal model by minimizing the Extended Bayesian Information Criterion (EBIC). To regulate the degree of shrinkage and reduce the likelihood of spurious edges and false-positive connections, we set the hyperparameter g (typically ranging between 0 and 0.5) to a value of 0.5. This choice aligns with the recommendation by Foygel and Drton37 and favors a more parsimonious model while maintaining robustness in network estimation.
Node centrality and predictability
In the analysis performed using the R package networktools, the computation of expected influence for each node was conducted to ascertain node centrality within the network. Expected influence represents the cumulative impact of both positive and negative edges connected to a particular symptom. Symptoms with higher expected influence are more strongly linked to other symptoms, thus indicating greater centrality within the network. Conversely, symptoms with low expected influences exhibit fewer or weaker connections with other symptoms. Additionally, node predictability was estimated to gauge the degree to which the variance of a given node can be accounted for by other nodes in the network38. This measure assesses how likely a particular node is influenced by its neighboring nodes, assuming that all connections in the network are directed toward this specific node. The computation of node predictability involved using the R package mgm, with R2 being employed as the measure to quantify the predictability for each node within the network. The R2 value represents the proportion of variance in a node explained by its neighboring nodes in the network.
Network stability and accuracy
The evaluation of the stability of expected influence involved employing the case-dropping subset bootstrap method. This technique computes the correlation stability coefficient to assess the robustness of expected influence measures within the network. The correlation stability coefficient represents the maximum proportion of cases that can be dropped while still maintaining a correlation, with 95% confidence, of 0.7 or higher with the original centrality values. Stability is considered adequate if the correlation stability coefficient reaches 0.25 and good if it achieves 0.536. To assess network accuracy, we estimated 95% confidence intervals (CIs) on the edge weights and node expected influence. This estimation was carried out using nonparametric bootstrapping, and subsequently, bootstrapped difference tests were conducted to ascertain significant differences between these estimations36. The R package bootnet was utilized to analyze both network stability and accuracy, providing insights into the reliability and precision of the expected influence measures and edge weights within the network structure.
Bridge symptoms
In the analysis, nodes representing mutuality were incorporated into the network comprising depressive symptoms to assess the interaction between mutuality and depression. Using the R package networktools, bridge symptoms were identified based on their bridge expected influence. This metric quantifies the cumulative impact of both positive and negative edge weights from a particular node to all nodes in another community within the network39,40.
A negative value for the bridge expected influence suggests that the node has an overall net negative association with another community, while a positive value indicates the opposite - a net positive association. It’s noteworthy that due to the scoring disparity between PHQ-9 (Patient Health Questionnaire) and MS (Mutuality Scale), a more negative bridge expected influence signifies a more influential bridge symptom. This negative value reflects the reversal in scoring direction between these measures, indicating the strength of influence or connection between different communities within the network.
Results
Descriptive statistics
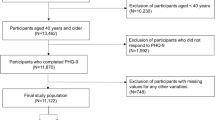
A total of 860 stroke survivors were invited to take part in the survey, out of which 847 stroke survivors were included in the analysis, resulting in an effective recovery rate of 98.49%. 9 patients were recruited for this study, but declined participation citing their poor physical condition. Of the 851 potential participants, 4 were excluded due to patterned responses. The average age of the participants was 58.74 years, with a standard deviation (SD) of 10.76. Descriptive statistics on the characteristics of the participants were provided in Table 1.
Depression symptom network
Figure 1 illustrates the depressive symptom network alongside the expected influence values for each symptom. Within the depression symptom network, 5 out of 36 potential edges (13.9%) were set to zero by the EBICglasso algorithms. Detailed analyses regarding edge weight accuracy are provided in supplemental Fig. 1. Depression symptoms were positively intercorrelated within the network. Notably, the network model highlighted that the connection between PHQ1 (“Anhedonia”) and PHQ2 (“Sadness”) emerged as the strongest positive edge within the PHQ-9 community. This was followed by the edges PHQ2 (“Sadness”) - PHQ6 (“Guilt”), and PHQ6 (“Guilt”) - PHQ9 (“Suicide ideation”). Bootstrapped difference tests confirmed the statistical strength of these edges compared to others. In terms of node centrality, the correlation stability coefficient for expected influence was 0.75, indicating excellent stability. PHQ2 (“Sadness”) exhibited the highest expected influence, positioning it as the central symptom in the depression network (Fig. 2). Further bootstrapped difference tests revealed that PHQ2’s expected influence, strength, closeness, and betweenness were significantly greater compared to other depressive symptoms. Regarding node predictability, the average node predictability was determined to be 0.46, suggesting that approximately half of the variation in nodes could be explained by their neighboring nodes. Notably, PHQ2 (“Sadness”) and PHQ1 (“Anhedonia”) were the most predictable nodes, with 66.3% and 61.9% of variance explained by neighboring nodes, respectively. Conversely, PHQ9 (“Suicide ideation”) and PHQ3 (“Sleep disorders”) were identified as the least predictable nodes, sharing 32.2% and 36.3% of their variance with other nodes, respectively.

The network of depressive symptoms. Blue and red edges represent positive and negative associations, respectively. Thicker and darker edges represent stronger associations, and vice versa.

Z-standardized centrality estimates.
Bridge nodes
Figure 3 illustrated the combined network of depressive symptoms and mutuality, along with the bridge expected influence index. The correlation stability coefficient for the bridge expected influence was calculated at 0.361, signifying a relatively stable expected impact of the bridge (supplemental Fig. 2). The Bridge Expected Influence Index (Fig. 4) identified ‘getting help from spouse’ (MS6), ‘attachment’ (MS5), and ‘concentration’ (PHQ7) as key bridge nodes fostering the relationship between comorbid mutuality and depressive symptoms. Supplementary Fig. 3 provided the outcomes of the bootstrapped difference tests for the bridge expected influence.

The network of depressive symptoms and mutuality. Green and red edges represented positive and negative associations, respectively. Thicker and darker edges represented stronger associations, and vice versa. Orange and blue nodes represented depressive symptoms and mutuality, respectively. The pie surrounding each node represented its predictability.

Z-standardized centrality estimates.
Discussion
To the best of our knowledge, this study represents the first attempt to investigate the network structure of depressive symptoms within a substantial cohort of Chinese stroke survivors. Additionally, it is pioneering in its exploration of the interplay between mutuality and depressive symptoms using network analysis methodology. The primary findings can be summarized as follows: (1) ‘sadness’ emerged as the most central depressive symptom within the depression network, and (2) ‘getting help from spouse’ played a crucial bridging role in connecting mutuality with depression.
The study revealed that depressive symptoms exhibited positive interrelations within the network, with certain symptoms exerting a more significant influence than others. These findings align with prior research investigating depressive symptom networks in American stroke patients17, individuals with chronic pain41, and those with eating disorders42. Notably, the global centrality estimates underscored ‘sadness’ as the foremost central symptom in the network of depressive symptoms among Chinese stroke survivors. This outcome aligns with Lau et al.‘s discovery17, indicating that ‘sadness’ holds a central position in depression networks, as measured by the 20-item Center for Epidemiologic Studies Depression Scale (CESD-20).
Sadness, as per the diagnostic criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5) for Major Depressive Disorder (MDD), is recognized as a hallmark symptom43. Stroke diagnosis and treatment often encompass various challenges such as hemiplegia, dizziness, aphasia, swallowing disorders, emotional and cognitive consequences, as well as insurance issues44,45,46. These factors collectively contribute to a diminished quality of life for stroke patients47,48. Notably, stroke survivors, as integral members of both their families and society, often shoulder multiple roles and responsibilities, such as those of a parent, spouse, and child. The considerable disease burden and high risk of recurrence associated with stroke frequently shift patients’ post-diagnosis priorities toward coping with health-related challenges. As a result, their ability to fulfill social and familial roles is significantly diminished, leading to marked impairments in role functioning and community participation. In addition, high rates of unemployment and increased financial pressure further exacerbate emotional distress49,50, potentially contributing to persistent feelings of sadness. Focusing on addressing sadness in treatment holds the potential to influence other closely interconnected symptoms more effectively within the network51. In clinical practice, sadness could be targeted by clinicians using reminiscence therapy (RT), which is designed to target affective symptoms of depression and promote better adaptation to current life circumstance by systematically guiding individuals to recall and reconstruct positive or neutral life experiences52. Prior studies have demonstrated the beneficial effects of reminiscence therapy in reducing depressive symptoms among stroke survivors53,54. Furthermore, dyadic interventions, which involve the active participation of both the patient and a close partner, such as a family member or caregiver, have emerged as a promising therapeutic approach. Recent findings suggest that dyadic reminiscence therapy may further enhance treatment outcomes for depression, but additional high-quality studies are needed to establish its efficacy and long-term benefits55,56.
Among the network nodes, ‘getting help from spouse’ and ‘attachment’ emerged as key bridge nodes connecting mutuality and depressive symptoms. In theoretical network models, such bridge symptoms are pivotal treatment targets, as interventions targeting them can disrupt powerful maintenance loops39. The significant roles of ‘getting help from spouse’ and ‘attachment’ suggest that spousal support, along with the survivor’s attachment relationship with their spouse, may significantly impact the pathway between mutuality and depressive symptoms. The majority of stroke survivors frequently experience hemiplegia and potential loss of physical function, leading to psychosocial challenges like depression and emotional distress57,58,59. Individuals with secure attachment styles generally demonstrate greater adaptability and are better equipped to cope with psychological distress in a constructive manner60. Moreover, support from spouses proves beneficial in helping stroke survivors cope with their diagnosis and its consequences, thereby improving their depressive symptoms. In this study, ‘concentration’ was bridge symptom of mutuality and depressive symptoms among patients with stroke. Stroke-related damage to specific brain regions, including the prefrontal cortex, basal ganglia, and thalamus, can directly impair neural networks responsible for attention regulation. Furthermore, core depressive symptoms frequently observed in stroke survivors, such as sadness and fatigue, consume substantial cognitive resources, resulting in emotion-attention competition and further impairing concentration4,61. Consequently, healthcare providers may consider employing dyadic coping interventions, as one of their essential components involves promoting healthy behaviors and psychological adjustment by facilitating couples to cope jointly with stressful events62. Furthermore, the inherent psychoeducational approach in dyadic coping interventions, such as family-centered empowerment and coping skill training, holds considerable promise for the psychological rehabilitation of stroke survivors. These interventions empower both stroke survivors and their spouses with coping strategies - ranging from problem-solving skills to body relaxation and stress reduction techniques - aimed at managing the consequences of stroke and fostering mental well-being. The feasibility and efficacy of dyadic coping interventions in improving outcomes for stroke survivors have been well-evaluated and demonstrated63,64. Consequently, incorporating these interventions into standard care practices may offer valuable support in enhancing the overall well-being and recovery trajectory of stroke survivors.
The study notably highlights that certain depressive symptoms, particularly suicide ideation and sleep disorders, demonstrated lower predictability. This suggests that these symptoms exhibit greater independence and are less susceptible to being influenced by changes in other depressive symptoms. According to network theory, low predictability does not necessarily imply that these symptoms should be prioritized for intervention. However, previous research has shown that suicidal ideation is a major risk factor for self-harm and mortality among stroke patients21, while persistent sleep disturbances are closely associated with poor emotional regulation, limited functional recovery, and increased rates of disability and recurrence among stroke survivors65. Given their high clinical urgency and potential for serious outcomes, early assessment and targeted interventions to effectively address these symptoms are essential. In line with these results, interventions such as dyadic coping strategies could be beneficial in addressing sleep disorders and suicidal ideation. Techniques involving dyadic cognitive-behavioral modification and personalized psychoeducation could offer valuable approaches to target these symptoms66. Implementing tailored interventions addressing specific symptoms may prove essential in effectively managing these aspects of depression among stroke survivors.
Limitations
There were several limitations in this study. First, it employed a cross-sectional design to construct the networks relating to mutuality and depressive symptoms. Consequently, this approach doesn’t allow for drawing causal inferences regarding whether mutuality influences depressive symptoms or vice versa. Second, our dataset was confined by the specific symptoms selected and defined within our network. The incorporation of additional symptoms could potentially yield an altered psychological network. Third, this study relied on self-report measures, possibly introducing biases related to memory and response tendencies. Fourth, this study used the PHQ-9 to assess depressive symptoms. As a screening tool primarily designed for detecting mild-to-moderate depression in primary care settings, the PHQ-9 lacks the sensitivity to adequately capture severe depressive symptoms and the specificity for comprehensive suicide risk assessment67. These limitations may have influenced our findings, particularly in the interpretation of symptom-level associations within the network analysis. Future research should consider incorporating clinician-administered instruments, such as the Hamilton Depression Rating Scale (HAMD) or the Montgomery-Åsberg Depression Rating Scale (MADRS), to enhance diagnostic precision and validity.
Conclusion
This study significantly contributes to our understanding of the relationship between mutuality and depressive symptoms among stroke survivors. Notably, sadness emerges as the focal depressive symptom within the depression network, while the aspect of receiving support from one’s spouse plays a pivotal bridging role, connecting depressive symptoms and mutuality. These findings highlight the potential of these symptoms as key targets for intervention strategies within this specific context. For instance, interventions focusing on dyadic coping, which involve couples working together to manage stressful situations, could prove beneficial for individuals experiencing depressive symptoms. Tailoring interventions to address these specific symptoms - such as targeting sadness and emphasizing spousal support - might offer promising avenues for enhancing the mental well-being of stroke survivors.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
References
Thayabaranathan, T. et al. Global stroke statistics 2022. Int. J. Stroke. 17, 946–956 (2022).
Guo, L., Zauszniewski, J. A., Liu, Y., Yv, S. & Zhu, Y. Is resourcefulness as a mediator between perceived stress and depression among old Chinese stroke patients? J. Affect. Disord. 253, 44–50 (2019).
Ezema, C. I. et al. Influence of Post-Stroke depression on functional independence in activities of daily living. Ethiop. J. Health Sci. 29, 841–846 (2019).
Guo, J., Wang, J., Sun, W. & Liu, X. The advances of Post-Stroke depression: 2021 update. J. Neurol. 269, 1236–1249 (2022).
Sadanandan, S., Renjith, V. & D, S. F. & Depression among rural stroke survivors: A Cross-Sectional study. Indian J. Community Med. 46, 309–312 (2021).
Zhou, X. et al. Intervention patterns and preliminary effectiveness on social participation following stroke: A scoping review. Bmc Neurol. 23, 275 (2023).
Castilla-Guerra, L., Fernandez, M. M., Esparrago-Llorca, G. & Colmenero-Camacho, M. A. Pharmacological management of Post-Stroke depression. Expert Rev. Neurother. 20, 157–166 (2020).
Li, S., Feng, W., Cui, F., Fang, B. & Yang, Q. Prevalence of depression among Chinese stroke patients: a Meta-Analysis (in Chinese). J. Pract. Med. 37, 2058–2064 (2021).
Fried, E. I. Problematic assumptions have slowed down depression research: why Symptoms, not syndromes are the way forward. Front. Psychol. 6, 309 (2015).
Borsboom, D. A. Network theory of mental disorders. World Psychiatry. 16, 5–13 (2017).
Cheung, T. et al. Network analysis of depressive symptoms in Hong Kong residents during the Covid-19 pandemic. Transl Psychiatry. 11, 460 (2021).
Borsboom, D. & Cramer, A. O. Network analysis: an integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 9, 91–121 (2013).
Lin, Y. et al. Prevalence, Correlates, and network analysis of depression and its association with quality of life in survivors with myocardial infarction during the Covid-19 pandemic. J. Affect. Disord. 336, 106–111 (2023).
Cramer, A. O., Waldorp, L. J., van der Maas, H. L. & Borsboom, D. Comorbidity: A network perspective. Behav. Brain Sci. 33 (150), 137 (2010).
Wang, Y. F. et al. Network analysis of comorbid Depression, suicidality and biomarkers on Hpa axis among mood disorder patients to psychiatric emergency services. Transl Psychiatry. 13, 203 (2023).
Ashaie, S. A., Hung, J., Funkhouser, C. J., Shankman, S. A. & Cherney, L. R. Depression over time in persons with stroke: A network analysis approach. J Affect. Disord Rep 4, (2021).
Lau, S., Connor, L. T., Lee, J. M. & Baum, C. M. Depressive symptomatology and functional status among stroke survivors: A network analysis. Arch. Phys. Med. Rehabil. 103, 1345–1351 (2022).
Gao et al. Clinical research progress in acupuncture for the treatment of Post-Stroke depression (in Chinese). Chin. J. Inf. Tradit Chin. Med. 03, 186–191 (2025).
Liu et al. Latent profile analysis of depressive symptoms among patients with stroke and its influencing factors. Mil Nurs. 38, 5–8 (2021).
Kleinman, A. Culture and depression. N Engl. J. Med. 351, 951–953 (2004).
Vyas, M. V., Wang, J. Z., Gao, M. M. & Hackam, D. G. Association between stroke and subsequent risk of suicide: a systematic review and Meta-Analysis. Stroke 52, 1460–1464 (2021).
Dong, L. et al. Prevalence and course of depression during the first year after mild to moderate stroke. J. Am. Heart Assoc. 10, e20494 (2021).
Rabat, Y., Sibon, I. & Berthoz, S. Implication of problematic substance use in poststroke depression: an Hospital-Based study. Sci. Rep. 11, 13324 (2021).
Mou, H. & Chien, W. T. Psychosocial factors associated with coping of inpatient stroke survivors and family caregivers: a dyadic analysis. Rehabil Psychol (2023).
Pucciarelli, G. et al. Moderator role of mutuality on the association between depression and quality of life in stroke Survivor-Caregiver dyads. J. Cardiovasc. Nurs. 36, 245–253 (2021).
Karlstedt, M., Fereshtehnejad, S. M., Aarsland, D. & Lokk, J. Mediating effect of mutuality on caregiver burden in parkinson’s disease partners. Aging Ment Health. 24, 1421–1428 (2020).
Dellafiore, F. et al. The association between Mutuality, anxiety, and depression in heart failure Patient-Caregiver dyads: an Actor-Partner interdependence model analysis. J. Cardiovasc. Nurs. 34, 465–473 (2019).
Pan, Y., Jones, P. S. & Winslow, B. W. The relationship between Mutuality, filial Piety, and depression in family caregivers in China. J. Transcult Nurs. 28, 455–463 (2017).
Godwin, K. M., Swank, P. R., Vaeth, P. & Ostwald, S. K. The longitudinal and dyadic effects of mutuality on perceived stress for stroke survivors and their spousal caregivers. Aging Ment Health. 17, 423–431 (2013).
Ostwald, S. K., Bernal, M. P., Cron, S. G. & Godwin, K. M. Stress experienced by stroke survivors and spousal caregivers during the first year after discharge from inpatient rehabilitation. Top. Stroke Rehabil. 16, 93–104 (2009).
Tanji, H. et al. Mutuality of the marital relationship in parkinson’s disease. Mov. Disord. 23, 1843–1849 (2008).
Archbold, P. G., Stewart, B. J., Greenlick, M. R. & Harvath, T. Mutuality and preparedness as predictors of caregiver role strain. Res. Nurs. Health. 13, 375–384 (1990).
Shyu, Y. I., Yang, C. T., Huang, C. C., Kuo, H. C. & Chen, S. T. Influences of Mutuality, Preparedness, and balance on caregivers of patients with dementia. J. Nurs. Res. 18, 155–163 (2010).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The Phq-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613 (2001).
Sun, Y., Kong, Z., Song, Y., Liu, J. & Wang, X. The validity and reliability of the Phq-9 on screening of depression in neurology: A cross sectional study. Bmc Psychiatry. 22, 98 (2022).
Epskamp, S., Borsboom, D. & Fried, E. I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods. 50, 195–212 (2018).
Foygel, R. & Drton, M. Extended bayesian information criteria for Gaussian graphical models. Vancouver(CA), :604–612. (2010).
Haslbeck, J. & Fried, E. I. How predictable are symptoms in psychopathological networks? A reanalysis of 18 published datasets. Psychol. Med. 47, 2767–2776 (2017).
Jones, P. J., Ma, R. & McNally, R. J. Bridge centrality: A network approach to Understanding comorbidity. Multivar. Behav. Res. 56, 353–367 (2021).
Jones, P. J., Mair, P. & McNally, R. J. Visualizing psychological networks: A tutorial in R. Front. Psychol. 9, 1742 (2018).
McWilliams, L. A., Sarty, G., Kowal, J. & Wilson, K. G. A network analysis of depressive symptoms in individuals seeking treatment for chronic pain. Clin. J. Pain. 33, 899–904 (2017).
Smith, K. E. et al. A comparative network analysis of eating disorder psychopathology and Co-Occurring depression and anxiety symptoms before and after treatment. Psychol. Med. 49, 314–324 (2019).
First, M. B. Diagnostic and statistical manual of mental Disorders, 5Th Edition, and clinical utility. J. Nerv. Ment Dis. 201, 727–729 (2013).
Chen, N., Dong, Y. & Kua, Z. Addressing mood and fatigue in Return-to-Work programmes after stroke: A systematic review. Front. Neurol. 14, 1145705 (2023).
Duan, C., Wang, Y. & Wang, L. Application effect of Multi-Module rehabilitation nursing model in intelligent Follow-Up of stroke patients (in Chinese). Chin. J. Nurs. 03, 276–282 (2023).
Urech, A. et al. An integrative Neuro-Psychotherapy treatment to foster the adjustment in acquired brain injury Patients - a randomized controlled study. J Clin. Med 9, (2020).
Song, Y. et al. Effects of multicomponent exercise on quality of Life, depression and anxiety among stroke survivors : A systematic review and Meta-Analysis. J. Clin. Nurs. 32, 7677–7690 (2023).
Gurkova, E., Sturekova, L., Mandysova, P. & Sanak, D. Factors affecting the quality of life after ischemic stroke in young adults: A scoping review. Health Qual. Life Outcomes. 21, 4 (2023).
Morsund, A. H. et al. Factors influencing employment after minor stroke and Nstemi. J. Stroke Cerebrovasc. Dis. 29, 105036 (2020).
Hahn, M. et al. Sex disparities in Re-Employment in stroke patients with large vessel occlusion undergoing mechanical thrombectomy. Stroke 53, 2528–2537 (2022).
Beard, C. et al. Network analysis of depression and anxiety symptom relationships in a psychiatric sample. Psychol. Med. 46, 3359–3369 (2016).
Pu, Y. et al. Reminiscence therapy delivery formats for older adults with dementia or mild cognitive impairment: A systematic review and network Meta-Analysis. Int. J. Nurs. Stud. 168, 105085 (2025).
Yu, J. et al. Reminiscence therapy is a feasible care program for improving cognitive Function, Anxiety, and depression in recurrent acute ischemic stroke patients: A Randomized, controlled study. Ir. J. Med. Sci. 192, 1463–1471 (2023).
Cheng, C., Fan, W., Liu, C., Liu, Y. & Liu, X. Reminiscence Therapy-Based care program relieves Post-Stroke cognitive Impairment, Anxiety, and depression in acute ischemic stroke patients: A Randomized, controlled study. Ir. J. Med. Sci. 190, 345–355 (2021).
Zhang, L., Li, X., Wang, J. & Liu, Y. Reminiscence therapy relieves Anxiety, depression and boosts spiritual Well-Being in both stroke patients and their spouse caregivers: A Randomized, controlled study: reminiscence therapy in stroke patients/Caregivers. Ir. J. Med. Sci. 193, 407–415 (2024).
Yueyang, Z. Dyadic reminiscence therapy in perioperative period of primary liver cancer patients application in neuropsychological symptom group (in Chinese). Xinxiang Medical University, (2023).
Mou, H., Wong, M. S. & Chien, W. T. Effectiveness of dyadic psychoeducational intervention for stroke survivors and family caregivers on functional and psychosocial health: a systematic review and Meta-Analysis. Int J. Nurs. Stud 120, (2021).
McCurley, J. L. et al. Preventing chronic emotional distress in stroke survivors and their informal caregivers. Neurocrit Care. 30, 581–589 (2019).
Fong, T., Lo, T. & Ho, R. Indirect effects of social support and hope on quality of life via emotional distress among stroke survivors: A Three-Wave structural equation model. Front. Psychiatry. 13, 919078 (2022).
Wang Ying, P. & Zhengwen, L. A. Zhang Meng. Mediating role of coping style in adult attachment and psychological distress in breast cancer patients (in Chinese). Mil Nurs. 37, 43–46 (2020).
Sobreiro, M. et al. The impact of Post-Stroke depressive symptoms on cognitive performance in women and in men: a 4 month prospective study. Life (Basel) 13, (2023).
Mou, H., Wong, M. S. & Chien, W. P. Effectiveness of dyadic psychoeducational intervention for stroke survivors and family caregivers on functional and psychosocial health: A systematic review and Meta-Analysis. Int. J. Nurs. Stud. 120, 103969 (2021).
Tielemans, N. S. et al. Effectiveness of the Restore4Stroke Self-Management intervention plan Ahead! A randomized controlled trial in stroke patients and partners. J. Rehabil Med. 47, 901–909 (2015).
Chow, E. O., Fung, S. F. & Singh, H. Actor-Partner effects of Wellbeing, hope and Self-Esteem on depression in stroke Survivor-Caregiver dyads: A randomized controlled trial. Clin. Rehabil. 37, 394–406 (2023).
Dan, L. et al. Effect of synchronous brain bionic electrical stimulation in hyperbaric oxygen chamber on Stroke-Related sleep disorders (in Chinese). Chin J. Rehabil Theory Pract 497–504 (2025).
Goodman, M. et al. A pilot randomized control trial of a dyadic safety planning intervention: safe actions for families to encourage recovery (Safer). Couple Family Psychol. 11, 42–59 (2022).
Thombs, B. D., Ziegelstein, R. C. & Whooley, M. A. Optimizing detection of major depression among patients with coronary artery disease using the patient health questionnaire: data from the heart and soul study. J. Gen. Intern. Med. 23, 2014–2017 (2008).
Author information
Authors and Affiliations
Contributions
ZZ(Zhenxiang Zhang), YM(Yongxia Mei) and RW(Ruibo Wang) originated and designed the study. RW, BL(Beilei Lin), and SG(Song Ge) coordinated the writing of the article and contributed to the drafting of the paper. XL(Xin Li) and HJ(Hu Jiang) contributed to the analysis of the data. ZZ(Zhixin Zhao) and HJ contributed to the interpretation of the results. QZ(Qiushi Zhang) contributed to the drafting of the paper, the analysis of the data and coordinated the response to reviewers’ comments during the revision process. All the authors take responsibility for the integrity of the data and the accuracy of the data. All the authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, R., Mei, Y., Lin, B. et al. Network analysis of mutuality and depression symptoms in stroke survivors in China. Sci Rep 15, 40323 (2025). https://doi.org/10.1038/s41598-025-24128-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-24128-y
