
Abstract
Diabetes mellitus remains a major global public health challenge. Mobile applications and digital platforms offer innovative opportunities to enhance diabetes self-management. This study aimed to evaluate the impact of diaB, a digitally delivered diabetes self-management education and support (DSMES) program, on clinical outcomes and diabetes-related knowledge in individuals with type 2 diabetes. This quasi-experimental, multicenter, open-label study involved 163 adults with type 2 diabetes, allocated to either a DSMES intervention group (n = 81) or a usual care control group (n = 82). The intervention group participated in a ten-week educational program delivered via the diaB mobile app and other digital platforms, based on the DSMES framework recommended by the American Diabetes Association. The program included online group video sessions led by doctors, nutritionists, and health coaches. Clinical outcomes—including fasting blood glucose (FBG), HbA1c, lipid profiles, weight, BMI, waist circumference, and diabetes knowledge (assessed using the Michigan Diabetes Knowledge Test, MDKT)—were measured at baseline and after the intervention. The intervention group showed significant improvements in clinical outcomes. FBG decreased from 7.5 to 6.7 mmol/L (P < 0.001), with a greater reduction than the control group (P = 0.004). HbA1c declined from 7.8 to 7.3% (P < 0.001), with no significant change in the control group. In multivariable linear regression adjusted for the disease risk score (DRS), the intervention was independently associated with greater HbA1c reduction (β = –0.72; 95% CI –1.14 to –0.31; P = 0.001), while higher DRS predicted less improvement (β = +0.57; 95% CI 0.12 to 1.01; P = 0.013). The intervention group also demonstrated greater gains in MDKT scores (+ 3 vs. –1; P < 0.001), more favorable changes in lipid profiles (P < 0.001), and greater weight loss among participants with baseline BMI ≥ 25 kg/m2 (–1.5 kg vs. 0 kg; P = 0.02). DiaB, a digitally delivered DSMES program, significantly improved glycemic control, diabetes knowledge, and metabolic outcomes. Integrating such digital interventions into routine diabetes care may enhance both clinical management and patient education in resource-limited settings.
Similar content being viewed by others

Introduction
Diabetes mellitus is a major global public health challenge. According to the International Diabetes Federation’s 2024 report, an estimated 589 million adults were living with diabetes, projected to reach 853 million by 20501. In Vietnam, diabetes has risen in rank as a cause of death and disability, and the economic burden is substantial, with complications driving markedly higher medical costs2,3.
Adherence to nonpharmacologic strategies—regular physical activity and healthy diet—has been associated with lower healthcare utilization and expenditures among people with diabetes4. Yet translating these benefits into everyday practice remains challenging in many low- and middle-income countries (LMICs), where patients often lack the knowledge and skills needed for day-to-day diabetes self-management. In Vietnam, diabetes knowledge among adults aged 40–64 remains limited, particularly in rural areas5. The Diabetic Retinopathy Barometer Study similarly points to inadequate patient education, insufficient professional training, and limited access to affordable care—issues especially pronounced in LMICs1.
The American Diabetes Association (ADA) advocates a comprehensive approach that integrates pharmacologic treatment with structured lifestyle interventions to improve outcomes6.
Diabetes self‑management education and support (DSMES), endorsed by the ADA, equips patients with skills to modify diet, activity, and medication behaviors7. In Vietnam, an offline DSMES model has demonstrated benefits5, but implementation is constrained by personnel demands, logistics, geography, and clinic time. In parallel, digital health solutions—including mobile applications—have shown efficacy in improving HbA1c, weight, and lipid profiles across clinical trials and meta-analyses8,9,10,11,12,13.
Rapid smartphone adoption in Vietnam (79.03 million users in 2023, projected to 97.19 million by 2029) creates a favorable context for digital DSMES delivery14. Mobile apps can reinforce lifestyle change and glucose control and are increasingly used as adjuncts to routine care12. The diaB digital DSMES program in Vietnam integrates app‑based lessons over multiple weeks, clinician‑led online group education, health coaching via Zoom and online group chats to support real‑world behavior change. Health coaching, though variably defined, has been associated with improvements in HbA1c and BMI in type 2 diabetes15,16,17.
Following preliminary implementation, we conducted a quasi‑experimental, multicenter, open‑label evaluation to assess whether the diaB digital DSMES program improves glycemic control and diabetes‑related knowledge compared with usual care over 12 weeks.
Materials and methods
Study design
The study was conducted among outpatients with type 2 diabetes at two sites: Hoan My Cuu Long Hospital (Can Tho, Vietnam) from March to July 2023, and Nguyen Tri Phuong Hospital (Ho Chi Minh City, Vietnam) from May to September 2023. The follow-up period was three months, which was considered sufficient to detect meaningful changes in both diabetes knowledge and HbA1c levels.
This study utilized a multicenter, open-label, quasi-experimental comparative design to evaluate the effectiveness of diaB, a digital Diabetes Self-Management Education and Support (DSMES) program for individuals with type 2 diabetes in Vietnam. Participants were allocated to either the intervention or control group based on their eligibility and willingness to participate. The primary objectives were:
-
1.
To assess the effectiveness of the diaB program in improving diabetes-related knowledge, measured using a modified version of the Michigan Diabetes Knowledge Test (MDKT).
-
2.
To evaluate the program’s impact on glycemic control and other key clinical outcomes.
Participants
Diagnostic criteria
Type 2 diabetes diagnosis followed ADA 2022 criteria6: fasting plasma glucose ≥ 7.0 mmol/L (126 mg/dL), 2-h plasma glucose ≥ 11.1 mmol/L (200 mg/dL) during a standard 75-g oral glucose tolerance test, HbA1c ≥ 6.5% (48 mmol/mol), or random plasma glucose ≥ 11.1 mmol/L with classic symptoms of hyperglycemia or hyperglycemic crisis. In the absence of unequivocal hyperglycemia, diagnosis required two abnormal test results from the same sample or from two separate samples.
Inclusion criteria
(1) aged ≥ 18 years; (2) newly or previously diagnosed with type 2 diabetes (per ADA 2022); (3) no initiation or intensification of antidiabetic therapy within the preceding 3 months; (4) ownership of an internet-connected smartphone (intervention group only); (5) provision of written informed consent; and (6) willingness to return for a 3-month follow-up visit.
Exclusion criteria
Pregnancy or plans to become pregnant; use within the last 3 months of agents that acutely alter glycemia (e.g., systemic glucocorticoids, thyroid hormones); severe acute illness; communication barriers due to significant visual or auditory impairments; psychiatric disorders or ongoing psychotropic medication treatment; alcohol or psychostimulant abuse; and inability to use a smartphone (for the intervention group).
Group assignment
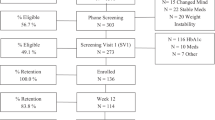
Participants were allocated to the intervention group (n = 81) or the usual-care control group (n = 82). Individuals who declined participation in, or did not meet inclusion criteria for the digital program were enrolled in the control group (Fig. 1). Control participants received routine endocrine clinic care and lifestyle counseling but did not attend intervention sessions and did not install the diaB application.

Flow diagram of participants: recruitment, intervention and follow-up.
Intervention
Participants in the intervention group received a ten-week digital DSMES program (diaB) grounded in the ADA DSMES framework7 and informed by self-determination theory18. The diaB mobile application delivered 26 structured lessons (video or text) covering diabetes knowledge, nutrition, home-based physical activity, and behavior change. Videos were concise (5–12 min) and culturally adapted with Vietnamese examples. Participants attended twice-weekly Zoom sessions led by diabetologists, nutritionists, psychologists, and physical coaches. Between sessions, health coaches moderated group chats via local instant-messaging platform Zalo to reinforce learning and address barriers. Participants were encouraged to record home blood-glucose readings in the app. Coaches and clinicians reviewed entries and provided individualized feedback (diet, activity, and medication-use advice within routine care). All participants continued routine endocrine-clinic follow-up.
Process evaluation and app usage monitoring
App analytics automatically logged lesson completion status, video watch time, and quiz attempts. Attendance for live sessions and coaching meetings was recorded from Zoom rosters and coach logs. The study team reviewed engagement dashboards weekly to identify participants below predefined adherence thresholds (< 60% lesson completion) for targeted outreach.
Data collection
At the study’s outset, baseline characteristics—including age, sex, diabetes duration, smoking status, weight, height, BMI, waist circumference, blood pressure, comorbidities (hypertension, dyslipidemia), and the use of antidiabetic medications—were recorded. Simultaneously, various biological parameters were collected, encompassing HbA1c, fasting blood glucose (FBG), creatinine, estimated glomerular filtration rate (eGFR), and lipid profile.
In conjunction with these measurements, diabetes knowledge, as an educational outcome was evaluated during the inclusion visit using the modified Michigan University Diabetes Knowledge Test (MDKT), a widely employed tool featuring 23 items19. The first 14 items gauged general knowledge, while the remaining 9 items assessed knowledge regarding insulin use. The original questionnaire underwent translation into Vietnamese and cultural adaptation. This Vietnamese version had been previously utilized in a study conducted in Vietnam and demonstrated good validation5. Each correct response in the multiple-choice questions earned one point. Participants scoring ≥ 12 points were categorized as having sufficient diabetes knowledge (passing the test), while those scoring < 12 points were considered test failures. All the baseline variables mentioned above were once again reviewed three months after the initiation of the study.
For the assessment of the primary outcome in the study, which involved a significant change in diabetes knowledge measured by the MDKT questionnaire, the sample size was determined using the following formula:
The significance level (α) was set at 5%, and the statistical power at 90%. Other variables in the formula were derived from a previous study conducted in Vietnam, which evaluated the change in diabetes knowledge after direct group-intervention sessions5. The calculated minimum required sample size was 37 patients for each group, accounting for a 20% estimated drop in participants. Consequently, the final minimum sample size needed was 44 patients for each group.
Outcomes
Primary clinical outcome was change in HbA1c from baseline to 12 weeks. Secondary outcomes included changes in fasting plasma glucose, lipid profile (LDL-C, HDL-C, triglycerides, total cholesterol), weight, BMI, waist circumference, and diabetes knowledge (MDKT). HbA1c was assayed in hospital laboratories accredited to national standards (NGSP-aligned methods).
Ethical considerations
This study was approved by the Ethics Committees of Hoan My Cuu Long Hospital and Nguyen Tri Phuong Hospital. All methods were performed in accordance with the relevant guidelines and regulations. Written informed consent was obtained from all participants before inclusion in the study.
Statistical analysis
Descriptive statistics were presented as mean (standard deviation) or median (interquartile range) for continuous variables, and as counts (percentages) for categorical variables, as appropriate. Group comparisons of categorical variables were performed using the chi-square test or Fisher’s exact test when expected cell counts were low. For continuous variables, Student’s t-test was used for normally distributed data, while the Mann–Whitney U test was applied for non-normal distributions. Within-group comparisons (baseline vs. 3 months) were conducted using paired t-tests for normally distributed variables and Wilcoxon signed-rank tests for non-normal data. The McNemar test was used for paired categorical variables.
To assess the independent effect of the intervention on the primary outcome (change in HbA1c from baseline to 3 months), a multivariable linear regression model was used, adjusting for potential confounders including age, sex, hospital site, baseline BMI, diabetes duration, and baseline knowledge score. To further address selection bias due to the non-randomized design, we applied disease risk score (DRS) adjustment. The DRS was constructed using a linear regression model predicting HbA1c change from baseline covariates (age, sex, hospital site, baseline BMI, diabetes duration, and knowledge score) and included as a covariate in the final regression model. The application of a disease risk score (DRS) for a continuous endpoint (ΔHbA1c) follows the prognostic score framework, where the score represents the conditional mean outcome under usual care rather than a probability. Accordingly, linear regression is the natural modeling choice, serving as the continuous analog to logistic/probit models used when outcomes are binary. This approach is supported by prognostic score theory20, methodological work demonstrating efficiency gains with linear adjustment for continuous outcomes21 regulatory guidance endorsing prognostic covariate adjustment in clinical trials22, and empirical applications of DRS in observational research23. In line with this evidence, we estimated the DRS via ordinary least squares from baseline covariates (age, sex, site, baseline BMI, diabetes duration, baseline knowledge score) and included it as a covariate in the final regression model.
All statistical tests were two-sided with a significance level of 0.05. Data entry was performed using Microsoft Excel 2016, and statistical analyses were conducted using Stata/MP version 14.0 (StataCorp LLC).
Results
Participant characteristics
A total of 163 individuals with type 2 diabetes were included in the study. The overall median age was 62 years, with participants in the intervention group being slightly younger than those in the control group (59 vs. 64 years; P = 0.004). The median diabetes duration was 8 years across both groups. Most participants had an estimated glomerular filtration rate (eGFR) > 60 mL/min/1.73m2, with no significant differences between groups (P = 0.27). Baseline characteristics—including gender, family history of diabetes, hypertension, dyslipidemia, and smoking status—were similar between groups (Table 1).
Anthropometric changes
At baseline, there were no significant differences between groups in median weight, BMI, or waist circumference (Table 1). After the intervention, the intervention group showed a significant reduction in median weight and BMI (P < 0.001, Table 2). Among participants with baseline BMI ≥ 25 kg/m2, the intervention group experienced a median weight loss of –1.5 kg compared to 0 kg in the control group (P = 0.02, Table 3). Waist circumference did not significantly change in either group (Table 2).
Glycemic control
Baseline median FBG and HbA1c levels, as well as the proportion of participants with HbA1c ≥ 7%, did not differ between groups (Table 4). After 12 weeks, the intervention group showed significant reductions in both FBG (from 7.5 to 6.7 mmol/L; P < 0.001) and HbA1c (from 7.8% to 7.3%; P < 0.001), with no significant changes observed in the control group (Table 5). Between-group differences in FBG and HbA1c change were statistically significant (P = 0.004 and P < 0.001, respectively; Table 6). The proportion of participants with HbA1c ≥ 7% decreased from 79.0% to 60.5% in the intervention group (P < 0.001), while remaining unchanged in the control group. However, among participants with BMI ≥ 25 kg/m2, HbA1c changes did not significantly differ between groups (P = 0.71, Table 6). Use of insulin and other medications remained unchanged before and after the intervention in both groups (Table 7).
Lipid profile
At baseline, lipid levels (LDL, HDL, total cholesterol) were comparable between groups, except for triglycerides, which were higher in the intervention group (Table 4). Following the intervention, the intervention group showed significant reductions in LDL, triglycerides, and total cholesterol (P < 0.001 for all; Table 8), while no significant changes were seen in the control group. Between-group comparisons confirmed greater improvements in the intervention group for all lipid parameters (Table 9).
Diabetes knowledge
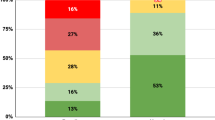
There were no significant differences in baseline MDKT scores or the proportion of participants with sufficient diabetes knowledge (≥ 12 points) between groups (Table 1). After 12 weeks, the intervention group had significantly higher median MDKT scores [16 (14–18) vs. 12 (8–14); P < 0.001] and a greater proportion of participants achieving sufficient knowledge (85.2% vs. 59.8%; P < 0.001) compared to the control group (Table 10). Intra-group analysis showed an increase in MDKT score from 12 to 16 in the intervention group (P < 0.001), while the control group had a modest decline from 13 to 12 (P = 0.02; Table 11). The median change in MDKT score was significantly greater in the intervention group [+ 3 (0–5) vs. –1 (–3 to 1); P < 0.001, Table 10].
Multivariable regression analyses
To adjust for potential selection bias from the non-randomized design, multivariable linear regression was used to assess factors associated with HbA1c change over 12 weeks. After adjusting for age, sex, hospital site, baseline BMI, diabetes duration, and baseline knowledge score, the intervention remained significantly associated with greater HbA1c reduction (β = –0.68; 95% CI: –1.11 to –0.25; P = 0.002). Other covariates were not significantly associated with HbA1c change (Table 12).
A second model adjusting for the disease risk score (DRS)—constructed from baseline covariates—also confirmed a significant intervention effect (β = –0.72; 95% CI: –1.14 to –0.31; P = 0.001). The DRS itself was positively associated with HbA1c change (β = + 0.57; 95% CI: 0.12 to 1.01; P = 0.013), indicating that individuals with higher baseline risk experienced less improvement. This model explained 10.8% of the variance in HbA1c change (adjusted R2 = 0.0971; P < 0.001).
Participant engagement
Engagement with the digital intervention was high. Participants completed an average of 76.1% of lessons on the diaB app. Completion rates for live educational sessions led by specialists were 81.1%, and for group coaching sessions, 73.2% (Table 13).
Discussion
This quasi-experimental study demonstrates that a digitally delivered DSMES program, integrated with group education, app-based learning, health coaching, and peer counseling, significantly improved glycemic control over 12 weeks among Vietnamese adults with type 2 diabetes. Participants in the intervention group achieved notable improvements in fasting blood glucose, HbA1c, LDL cholesterol, and triglyceride levels. Furthermore, diabetes-related knowledge increased significantly, reflecting enhanced understanding of self-management practices and disease control.
To address the limitations of the non-randomized design, we applied disease risk score (DRS) adjustment instead of propensity score matching. This approach preserved the full sample size and statistical power while effectively controlling for confounding based on baseline predictors of HbA1c change. The intervention effect remained robust and statistically significant after DRS adjustment. Additionally, the DRS itself was independently associated with HbA1c outcomes, indicating that individual baseline characteristics play a critical role in glycemic response.
These findings underscore the potential of the ‘diaB digital program’ to facilitate effective diabetes management and lifestyle modifications. The positive outcomes observed in the intervention group can be attributed, at least in part, to the effectiveness of the diaB digital program.
A recent meta-analysis revealed that clinical trials of digital interventions typically involved an average of 143 participants, exhibiting an average HbA1c level of approximately 8.5%, with follow-up periods ranging from 1 to 24 months. In comparison to standard care, digital interventions were found to lower HbA1c levels by an average of around 0.31%. Particularly noteworthy was the high-intensity intervention group, which experienced an average HbA1c reduction of about 0.46%24. Therefore, with a HbA1c reduction of 0.5%, our study once again validates the efficacy of digital interventions, consistent with findings from prior research.
Despite the promising outcomes, this study faces several limitations, including the non-randomized allocation, unmeasured confounders, and short follow-up. Nonetheless, our methodological approach strengthens the internal validity and supports the conclusion that the intervention improves glycemic control. The ten-week duration of the intervention may have restricted our ability to observe long-term effects on self-management behaviors and outcomes. Extending the intervention period could provide deeper insights into sustained behavioral changes and their impacts on long-term health outcomes. Additionally, compared to other studies, our study did not explore personal motivation factors or measure self-management behavioral skills comprehensively, which are essential for understanding the full impact of DSMES programs.
The dropout rates observed—24.3% in the intervention group and 34.4% in the control group— may have impacted the study’s results, raising concerns regarding the general applicability and effectiveness of the program, especially among older adults less familiar with technology. Despite these obstacles, the high engagement levels in educational sessions, particularly those conducted via Zoom by specialists, underscore a significant interest in participation. This suggests the potential efficacy of the diaB digital program in enhancing patient education and engagement. Indeed, the digital program offered assistance to participants facing challenges specifically with the installation of applications on smartphones and interactions with specialists via alternative communication platforms. DiaB supported this effort with a team that offered assistance either directly via the Zalo platform or indirectly through participants’ relatives. To maintain the quality of the program, technologically inexperienced participants were supported in smaller, specialized groups with comprehensive guidance. Consequently, the notion that participant compliance was a major issue within this digital program may be reconsidered.
To better understand the factors contributing to the dropout rate, future research should include motivational assessments for both completers and noncompleters. This could provide valuable insights into barriers to program adherence and help customize the program to better meet participant needs.
Conclusions
The findings from this study highlight the significant role that digital health interventions, like our comprehensive digital DSMES program, can play in supporting diabetes management and enhancing patient education. By integrating such technologies into standard care, healthcare professionals can empower patients to actively manage their health and promote shared decision-making.
Data availability
All data supporting the findings of this study are available within the article. No supplementary files were submitted.
References
IDF Diabetes Atlas (11th ed.). Brussels, Belgium: International Diabetes Federation. 11. (2024).
Safiri, S. et al. Global, regional, and national burden of other musculoskeletal disorders 1990–2017: results from the Global Burden of Disease Study 2017. Rheumatology (Oxford) 60(2), 855–865 (2021).
Pham, T. K. et al. Direct medical costs of diabetes and its complications in Vietnam: A national health insurance database study. Diabetes Res. Clin. Pract. 162, 108051 (2020).
Alfaifi, A. Association between non-pharmacological therapy and healthcare use and expenditure of patients with diabetes mellitus. Saudi Pharm. J. 31(8), 101685 (2023).
Thanh, H. T. K. & Tien, T. M. Effect of group patient education on glycemic control among people living with type 2 diabetes in Vietnam: A randomized controlled single-center trial. Diabetes Ther. 12(5), 1503–1521 (2021).
American Diabetes Association Professional Practice Committee. Standards of medical care in diabetes. Diabetes Care 46, S1–S2 (2022).
American Diabetes Association Professional Practice. Facilitating behavior change and well-being to improve health outcomes: Standards of medical care in diabetes-2022. Diabetes Care 45(Suppl 1), S60–S82 (2022).
Wayne, N. et al. Health coaching reduces HbA1c in type 2 diabetic patients from a lower-socioeconomic status community: A randomized controlled trial. J. Med. Internet Res. 17(10), e224 (2015).
Quinn, C. C. et al. Cluster-randomized trial of a mobile phone personalized behavioral intervention for blood glucose control. Diabetes Care 34(9), 1934–1942 (2011).
El-Gayar, O., Ofori, M. & Nawar, N. On the efficacy of behavior change techniques in mHealth for self-management of diabetes: A meta-analysis. J. Biomed. Inform. 119, 103839 (2021).
Pal, K. et al. 2013 Computer-based diabetes self-management interventions for adults with type 2 diabetes mellitus. Cochrane Database Syst. Rev. 3, CD008776 (2013).
Sy, B. et al. Personalizing self-management via behavioral predictive analytics with health education for improved self-efficacy. Patterns (N. Y.) 3(6), 100510 (2022).
Moschonis, G. et al. Effectiveness, reach, uptake, and feasibility of digital health interventions for adults with type 2 diabetes: a systematic review and meta-analysis of randomised controlled trials. Lancet Digit Health 5(3), e125–e143 (2023).
Degenhard, J. Number of mobile internet users in Vietnam from 2010 to 2029. https://www.statista.com/forecasts/1147340/mobile-internet-users-in-vietnam]. (Accessed 05 September 2025). (2024).
Wolever, R. Q. et al. A systematic review of the literature on health and wellness coaching: Defining a key behavioral intervention in healthcare. Glob. Adv. Health Med. 2(4), 38–57 (2013).
Sherifali, D. et al. Evaluating the effect of a diabetes health coach in individuals with type 2 diabetes. Can. J. Diabetes 40(1), 84–94 (2016).
Pirbaglou, M. et al. Personal health coaching as a type 2 diabetes mellitus self-management strategy: A systematic review and meta-analysis of randomized controlled trials. Am. J. Health Promot. 32(7), 1613–1626 (2018).
Patrick, H. & Williams, G. C. Self-determination theory: its application to health behavior and complementarity with motivational interviewing. Int. J. Behav. Nutr. Phys. Act. 9, 18 (2012).
Fitzgerald, J. T. et al. Validation of the revised brief diabetes knowledge test (DKT2). Diabetes Educ. 42(2), 178–187 (2016).
Hansen, B. B. The prognostic analogue of the propensity score. Biometrika 95(2), 481–488 (2008).
Schuler, A. et al. Increasing the efficiency of randomized trial estimates via linear adjustment for a prognostic score. Int. J. Biostat. 18(1), 27–46 (2022).
European Medicines Agency. Qualification Opinion for PROCOVA™: Prognostic Covariate Adjustment. EMA/CHMP/SAWP/696836/2021. London: EMA. (Accessed 05 September 2025). (2022).
Glynn, R. J., Gagne, J. J. & Schneeweiss, S. Role of disease risk scores in comparative effectiveness research with emerging therapies. Pharmacoepidemiol. Drug Saf. 21(Suppl 2), 138–147 (2012).
Kerr, D. et al. Digital interventions for self-management of type 2 diabetes mellitus: A systematic literature review and meta-analysis. J. Med. Internet Res. 26, e55757 (2024).
Acknowledgements
The authors would like to express their sincere gratitude to the board of directors, physicians, nurses, and staff members at Nguyen Tri Phuong Hospital and Hoan My Cuu Long Hospital for their invaluable support in facilitating this study. We extend our deep appreciation to the study participants for their cooperation and commitment to completing the intervention. Additionally, we are thankful for the assistance provided by the healthcare professionals, including the diabetologists, nutritionists, psychologists, and health coaches, whose expertise and dedication made the implementation of the digital DSMES program possible. This research would not have been possible without the support of the DiaB Healthcare Technology Company for the development and maintenance of the diaB mobile application, which played a crucial role in the success of the program. Finally, we acknowledge the constructive feedback from our colleagues and peers, which greatly contributed to the refinement of this study.
Author information
Authors and Affiliations
Contributions
Phong Nguyen: Study design, statistical analysis, manuscript drafting. Luong Dai Ly: Manuscript revision, supervision of the study, and final approval of the version to be submitted. Khanh Tran: Co-corresponding author. Contributed to study design, coordination, manuscript review, and final approval of the version to be submitted. Duong Le: Provided clinical expertise, data interpretation, and contributed to the manuscript review. Hoanh Tran: Participated in the collection and interpretation of clinical data, and reviewed the manuscript. Ha Nguyen: Lead health coach. Dai Truong: Provided input on the digital DSMES intervention design and assisted in the coordination of the program’s implementation. Uyen Lam: Contributed to data collection, overall coordination of the research. Nhi To: Contributed to data collection, overall coordination of the research. Viet Tran: Technical support of the diaB mobile application. Nhat Luong: Technical support of the diaB mobile application.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Nguyen, P.V.N., Thach, P.T., Tran, H.K. et al. Effectiveness of a digital diabetes self-management education and support program in Vietnamese adults with type 2 diabetes. Sci Rep 15, 41369 (2025). https://doi.org/10.1038/s41598-025-25245-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-25245-4
