
Abstract
Therapeutic effects of patellofemoral arthroplasty (PFA) on patellofemoral arthritis are presented. All patellofemoral arthroplasties performed from 2008 to 2023 were retrospectively reviewed using case notes, radiographs and clinic appointments until their latest follow-up period. 132 arthroplasties in 126 patients were followed up for an average period of 31.8 months (range 3–90 months). The average age was 54.2 years with 112 female patients and 14 male patients. No severe complications were detected during follow-up period. Knee function: straight 0°, flexion average 120° (110 to 135°). Feller score was 24.8 points (22 to 28 points). Arthroplasty is required when conservative treatments were ineffective. Although total knee arthroplasty (TKA) has achieved good results in the treatment of tricompartment osteoarthritis, there is still controversy over the treatment of pure patellofemoral arthritis. PFA has minimal trauma, good clinical efficacy, less osteotomy, and more preservation of tibiofemoral joint bone mass, without affecting possible future TKAs. This surgical procedure has satisfactory mid-term efficacy, but close follow-up is needed for its long-term efficacy.
Similar content being viewed by others

Introduction
When knee osteoarthritis (OA) progresses to the late stage, the cartilage is severely worn and loses its ability to regenerate and repair1,2. Arthroplasty is then used for its treatment with ineffective conservative treatment. However, TKA seems not optimum for severe isolated patellofemoral osteoarthritis (PFOA)3,4. PFA has minimal surgical trauma and can achieve satisfactory clinical outcomes. With less osteotomy and no involvement of the tibiofemoral joint, it will basically not affect future TKA surgeries5,6. Author applied 132 PFA surgeries in 126 cases of isolated PFOA, obtaining satisfactory mid-term therapeutic effects. The following report combines its design features and clinical significances.
Materials and methods
Patients
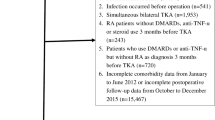
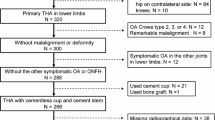
This is a retrospective report of patients who underwent PFA due to simple PFOA with a course of one to six years in our hospital from 2008 to 2023, which is licensed by the Ethics Committee of the Second Affiliated Hospital of Soochow University under decision number JD-HG-2025-017. All methods were carried out in accordance with relevant guidelines and regulations. Due to the retrospective nature of the study, the need of obtaining informed consent is waived by the Ethics Committee of the Second Affiliated Hospital of Soochow University. 126 patients were included and followed up, with 14 males (14 knees) and 112 females (118 knees), ranging from 45 to 68 years (mean 54.2 years). Inclusion criteria were (1) anterior knee pain obvious with a rolling feeling when bending knees especially on going up or down stairs, while no pain when walking on flat land. (2) disappeared space of patellofemoral joint and osteophyte with normal tibiofemoral joint space and limb alignment demonstrated on X-ray. (3) a large area defect in patellofemoral articular cartilage of grade IV wear, with no obvious degeneration of tibiofemoral articular cartilage and normal meniscus ligaments on MRI. Exclusion criteria include (1) Systemic and progressive inflammatory arthropathies, such as rheumatoid arthritis or gouty arthritis. (2) MRI confirmed anterior cruciate ligament (ACL) tear or failure of ACL reconstruction. (3) Extensive bone defects in the femoral condyle or patella that cannot provide stable support for the prosthesis. (4) Knee flexion contracture greater than 15 degrees. Feller’s patellar scoring system were assessed with an average score of 12.3 (range 7–16) preoperatively.
Surgical procedure
PFJ patellofemoral prosthesis of American Zimmer company was applied in this group.
General anesthesia or continuous epidural anesthesia was performed and lower extremity tourniquet was used. The anteromedial skin incision of knee and the medial parapatellar joint capsule approach were taken to expose the patellar articular surface and femoral condyle. Whiteside line or Insall line was marked as a reference. Under the guidance of the locator, osteotomy was performed on the anterior femoral condyle to ensure that the osteotomy surface was parallel to the anterior femoral cortex with a 3 to 6° external rotation7,8. The curved osteotomy surface was made in the intercondylar recess to accommodate the femoral trochlear prosthesis, ensuring the surface of the prosthesis is flat with the surrounding cartilage surface after implantation.
Treatments of patellar articular surface were carried out in different ways of patellar prosthesis replacement and patelloplasty with patella preservation9. The former procedure was performed in 98 cases with 101 knees as long as the thickness of the patella allows. The patellar articular surface was resected by electric saw with the remaining thickness of 12–14 mm, and a hole was made outside the center of the osteotomy surface to accommodate the artificial patellar prosthesis pedicle10. While the latter way was performed in 28 cases with 31 knees, including removal of proliferative osteophyte around, denervation by cauterizing the periphery of patella and trim of patella. The patellar prosthesis and femoral trochlear prosthesis were fixed with bone cement. Intraoperatively, PMMA bone cement with 0.5–0.55 g gentamicin was utilized. Patients with severe patellofemoral subluxation were treated with lateral release and medial overlapping tight suture. Confirming that the range of motion and patellar trajectory of flexion and extension were satisfactory using “no thumb test”, the surgical incision was closed layer by layer. Pre-operative and Psot-operative radiographs of a 52-year-old woman underwent bilateral PFA was presented in Figs. 1, 2, 3 and 4.
Postoperative treatment and rehabilitation exercise
Antibiotics were routinely used 2 days after operation, and the drainage tube was removed within 48 h. Anticoagulation with low molecular weight heparin was started 12 h after operation, and the lower limb pneumatic pump were given to promote venous blood reflux. Analgesic and detumescence treatments were routinely administered. The functional exercise dominated by quadriceps femoris was started on the second day after surgery11, combined with CPM machine assisted exercise12. Patients can walk with weight after removal of drainage tube and increase the range of motion of surgical joint, with bending more than 90 ° in 5 days. Duration of discharge was 7–14 days postoperatively.
Results
The average operation time was 45 min (range 30 to 60 min) with little bleeding. The average postoperative drainage fluid was 125 ml (range 50–200 ml). The average follow-up time was 31.8 months (range 3 to 90 months), with no cases of wound infection. All 126 patients recovered their daily life 3 months after operation. Among them, 125 patients could completely resist resistance with no limit in walking and standing. One patient could walk 2500 m and stand for more than 30 min. Meanwhile, 123 patients could squat completely, while the other 3 ones were slightly limited. (Squats are performed to a maximum knee flexion of 111°±23°. The half squat uses a range of 80° to 100°, while the quarter squat is executed at a shallower angle of 110° to 140°.)13,14 No flexion deformity, joint instability or patellar dislocation was found and all patients could walk independently without support. In terms of knee function, straightening was 0 degree and the average flexion of knee was 120 degrees (range 110 to 135 degrees). The average Feller patellar score at follow-up was 24.8 (range 22 to 28).

Pre-operative radiographs of bilateral knee of a 52-year-old woman with isolated patellofemoral arthritis. MRI indicated grade Ⅳ wear of the patellofemoral joint cartilage.

The patient underwent bilateral PFA. Anteroposterior and lateral radiographs of both knees were re-examined two days after operation.

X-ray reviewed 2 months postoperatively.

X-ray reviewed 4 months postoperatively.
Discussion
The incidence of simple patellofemoral osteoarthritis is about 9% in the population over 40 years old. It is common in women and is often accompanied by abnormal patellar trajectory and force line15,16. Conservative treatments improve the symptoms, while due to the gradual wear of articular cartilage, it is difficult to go upstairs and downstairs and squat down, with increasing swelling and pain of knee. Although TKA achieves good results, it is not suitable for relatively young patients, nor for single compartment osteoarthritis17. Patellofemoral joint surface arthroplasty has not been widely used in clinical practice due to the problems of prosthesis design and surgical techniques18. While the improvement of prosthesis design, indication selection and surgical technique have improved the clinical efficacy of patellofemoral joint surface arthroplasty in recent years19,20. Sarda21 reported 45 cases of PFA with an average follow-up of 4.5 years. The survival rate of the prosthesis was 95.6%. Dahm compared TKA and PFA, with similar curative effects. But the amount of surgical bleeding in PFA group was significantly reduced, the length of hospital was shortened, and no serious complications occurred. Odumenya22 evaluated 50 knees with PFA for simple patellofemoral osteoarthritis, with average follow-up of 5.3 years. The survival rate of the prosthesis was 100% in 5 years. The end point of follow-up over 5 years was mainly the progression of tibiofemoral osteoarthritis, and 11 knees (20%) showed osteoarthritis on X-ray. Charalambous23 analyzed 51 cases of PVA of group movable patella. The three-year survival rate was only 63% and the revision rate was 46%. It is considered that the movable patella is the most fundamental defect. The rotation of polyethylene patella parts makes the metal backing collide with the metal pulley, resulting in inflammation and pain. Therefore, good prosthesis design is the guarantee of good prosthesis survival rate.
Consideration on the design characteristics of patellofemoral prosthesis
PFJ patellofemoral joint used in this research include femoral intercondylar trochlear part and patella part. As the second-generation PFA prosthesis, it has changed the design concept of the first-generation prosthesis Inlay and the design concept of Onlay was adopted24. To replace the original patellofemoral joint area with a surface replacement prosthesis, not only the lesion area of the trochlear, but also the corresponding relationship between the placement of the trochlear prosthesis and the anatomy of the distal femur has been fully considered. The design concept of the femoral intercondylar trochlear component is that the anterior part is as thin as possible to reduce the amount of bone cutting. Its proximal end is continuous with the anterior femoral cortex, allowing sufficient patella mobility in the knee extension position. The funnel-shaped design keeps the patella in the trochlear fossa, prevents lateral subluxation and restores good engagement of the patellofemoral joint within the range of extension and flexion. At the middle angle of knee flexion, the shape of trochlear fossa is consistent with that of patella, which can control the movement track of patella. Prosthesis edge is reduced to prevent impact on the support belt. The distal end of the prosthesis is in a “U” shape and is placed higher than the intercondylar fossa to protect the cruciate ligament and meniscus. The dome shaped design of the polyethylene patella component has an inward eccentricity of about 3 mm, which makes the patella better match the femoral medial condyle during deep flexion, and is convenient to correct the abnormal trajectory and force line.
Selection of indications for patellofemoral arthroplasty
The indications obtained from literatures are: degenerative osteoarthritis limited to patellofemoral joint; Severe patellofemoral joint symptoms affecting daily activities treated ineffectively with 3-month conservative treatment; Posttraumatic osteoarthritis; Cartilage lesions above grade 3, especially in the trochlear groove of femur, the inner side and distal end of patella; Failure of patellofemoral joint decompression operation; Osteoarthritis induced by malalignment and deformity of patellofemoral joint25,26. All patients in this group suffered from univentricular osteoarthritis limited to patellofemoral joint, with serious symptoms and ineffective regular conservative treatment. Special attention was paid to the X-ray findings of localized patellofemoral joint degeneration, narrowing of joint space, subchondral bone sclerosis and cystic change, with normal tibiofemoral joint space. PFA should be avoided for patients with anatomical deformity of tibiofemoral joint and poor force line of lower limbs. Since abnormal patellar trajectory can not be adjusted in PFA, orthopedic surgery should be performed before or at the same time as PFA. Otherwise, poor patellar trajectory, patellar subluxation and tibiofemoral joint degeneration are likely to occur after PFA, resulting in unsatisfactory curative effects. Therefore, the full-length X-ray of both lower limbs were taken before operation. MR examination was performed in each patient to confirm patellofemoral osteoarthritis, no obvious degeneration of tibiofemoral articular cartilage, and normal meniscus and cruciate ligament. In other words, joint instability, abnormal trajectory and abnormal force line were excluded. Lonner27 reports that the incidence of tibiofemoral osteoarthritis is about 20% 15 years after operation, with a portion of patients undergoing TKA. Tauro28 et al. reported that the satisfaction rate of Lubinus prosthesis was only 45% and 28% of the knee joints needed revision. One-third of the revision cases were caused by the progression of tibiofemoral joint lesion. Therefore, accurate selection of indications is the guarantee of satisfactory curative effect.
In this group, 126 patients were followed up for an average of 31.8 months, showing that the knee function and the overall curative effect were satisfactory. No disease of tibiofemoral joint was found during the follow-up period. Commonly used knee scoring systems, such as HSS, Lysholm and Tegner, were not adopted in this research. Most of these methods focus on the symptoms and functions of the whole knee joint, which are not sensitive to evaluate simple patellofemoral arthritis. The Feller patella scoring system is used. The evaluation of four aspects, including anterior knee pain, quadriceps femoris muscle strength, sitting position standing ability and stair climbing ability, can accurately reflect the condition of patellofemoral joint, with a full score of 30 points. The Feller score in this group increased from an average of 12.3 before operation to an average of 24.8 after operation.
Key points of patellofemoral arthroplasty
Correctly mastering the key points of artificial PFA is the basic condition to ensure the curative effect of PFA. Early PFA surgery lacks accurate prosthesis operation system, and lack of standardization increases the unpredictability of surgical efficacy. While with the progress of technology, the current PFA operation is more accurate and standardized. The surgical position and incision are similar to that of TKA. Only osteotomy of the anterior femoral condyle is required. Take the Whiteside line from the lowest part of the trochlear to the highest part of the femoral intercondylar notch or the Insall line through the femoral epicondylar axis as a reference, so that the osteotomy surface is parallel to the anterior cortex of the femoral shaft with 3–6° external rotation. The prosthesis was placed slightly 1–2 mm laterally to reduce the lateral subluxation of the patella. The embedded depth of the prosthesis should be level with the surrounding joint surface, so as to avoid the collision and uncomfortable sound of the prosthesis.
The treatment of patella is the same as that of TKA. Patella can be replaced or not. The key of PFA is to restore the patellofemoral force line. An ideal patellofemoral prosthesis has a good coping line, which can maintain an ideal motion trajectory in the knee flexion and extension activities, preserve the function of the prosthesis and reduce the wear of the prosthesis without abnormal stress between patellofemoral joints. During the operation, “no thumb test” should be used to observe the patellar trajectory and judge the stability of the patella. In the range of extension and flexion, the medial surface of the patella should always be in good contact with the trochlear fossa of the femur. When flexing at 110°, the odd surface of the patella should be in contact with the medial femoral condyle. While at 120°, it should be confirmed that there is no impact. After careful treatment of the patella, further lateral release should be performed if the inner side of the patella tends to separate from the trochlear fossa of femur. If patellar trajectories cannot be recovered after sufficient release, additional soft tissue or bone realignment surgery or TKA can be considered. All cases in this group were released laterally enough to obtain a good patellar trajectory.
Conclusion
Patellofemoral joint arthroplasty is an effective method for the treatment of severe simple patellofemoral arthritis, which can significantly improve the symptoms such as pre-patellar pain. The meniscus, ligament structure and proprioception were preserved, with the normal movement mechanism maintained. Patients could climb, descend the stairs and squat, stand up autonomously shortly after surgery. Due to the small amount of osteotomy and the retention of appropriate stress stimulation, the range of bone loss at the lower end of the femur after PFA is smaller than that after TKA, which is especially suitable for young or active patients. As young patients have long life expectancy and high activity, early acceptance of TKA will increase the probability of revision. PFA retains the bone mass and complete joint structure, which can delay the time of TKA, without affecting the future TKA. The key to improve the survival rate of prosthesis is the accurate selection of indications and skilled surgical operation. TKA should be prepared during operation. If there is more than 1 cm articular cartilage defect in the tibiofemoral joint during the operation, especially the lesion located in the lateral condyle, TKA is appropriate to be performed. Because the disease of articular cartilage of lateral condyle will progress rapidly after PFA, it is not recommended in this case. On the other hand, TKA presents a constellation of severe long-term issues for younger patients under 55, such as finite implant survivorship, incompatibility with higher activity levels, and the sacrifice of native proprioception and biomechanical function. Consequently, joint-preserving strategies are predominantly employed. In this patient cohort, the pathomechanism frequently originates from a rotational malalignment of the lower extremity. A femoral osteotomy corrects this fundamental aetiology, and when combined with a concomitant decompression procedure to address resultant localised pathology, it serves to maximally preserve the functional integrity of the native knee. This integrated approach constitutes a definitive joint preservation intervention.
TKA is mostly regarded as the first choice for treating severe patellofemoral arthritis in clinical practice, while it has been proven that PFA can also achieve same clinical efficacy. It is believed that with the advancement in research on the anatomical physiology and kinematic coordination mechanisms of the normal patellofemoral joint’s dynamic corresponding structures, especially studies on the anatomical correspondence between the patellofemoral joint and the femoral condyle joint at the distal femur, the formation mechanism of the patellar trajectory and its influencing factors, as well as the kinematic coordination mechanism between the patellofemoral joint and the tibiofemoral joint, the understanding of the pathological mechanisms of isolated PFOA and the relevant knee joint anatomy and physiology will be further enhanced. This will undoubtedly significantly propel the development and optimization of patellofemoral joint prosthesis design, surgical instrument operating systems, and surgical techniques. PFA preserves the vast majority of the knee joint’s anatomical structures, encompassing bone reserves and the patient’s own ligaments. This procedure is more minimally invasive compared to TKA, and it enables a more rapid rehabilitation of knee joint function postoperatively. Undoubtedly, these merits will secure a prominent position for patellofemoral joint arthroplasty in the realm of artificial knee joint surface arthroplasty.
Data availability
The data generated and analyzed during the current study are included in this article.
References
McAlindon, T. E., Snow, S., Cooper, C. & Dieppe, P. A. Radiographic patterns of osteoar- thritis of the knee joint in the community: the importance of the patellofemoral joint. Ann. Rheum. Dis. 51, 844–849 (1992).
Zhang, J. et al. Radiomics analysis of patellofemoral joint improves knee replacement risk prediction: data from the multicenter osteoarthritis study (MOST). Osteoarthr. Cartil. Open. 6 (2), 100448 (2024).
Rogers, J. T. et al. Short-term functional outcomes and complications of custom patellofemoral arthroplasty. Arthroplast Today. 26, 101335 (2024).
Lachance, A. D., Steika, R., Lutton, J. & Austin, D. Conversion of patellofemoral arthroplasty to Robotic-Assisted total knee arthroplasty. Arthroplast Today. 23, 101215 (2023).
Dahm, D. L. et al. Patellofemoral arthroplasty versus total knee arthroplasty in pa- tients with isolated patellofemoral osteoarthritis. Am. J. Orthop. (Belle Mead NJ). 39, 487–491 (2010).
Li, C., Li, Z., Shi, L., Gao, F. & Sun, W. The short-term effectiveness and safety of second-generation patellofemoral arthroplasty and total knee arthroplasty on isolated patellofemoral osteoarthritis: a systematic review and meta-analysis. J. Orthop. Surg. Res. 16 (1), 358 (2021).
Beitzel, K., Schöttle, P. B., Cotic, M., Dharmesh, V. & Imhoff, A. B. Pro- spective clinical and radiological two-year results after patellofemoral arthroplasty using an implant with an asymmetric trochlea design. Knee Surg. Sports Traumatol. Arthrosc. 21, 332–339 (2013).
Nakano, N. et al. The influence of patellar height on patellofemoral contact force during total knee arthroplasty. J. Joint Surg. Res. 1 (1), 186–191 (2023).
Yamawaki, Y. et al. Internal rotation, varus, and anterior femoral component malalignments adversely affect patellofemoral joint kinematics in patellofemoral arthroplasty. Arthroplast Today. 21, 101124 (2023).
Shatrov, J. & Coolican, M. R. Isolated patellofemoral arthroplasty-surgical technique and tips: current concepts. J. ISAKOS. 9 (4), 814–821 (2024).
Erquicia, J. I. et al. Standard versus dysplastic inlay implant for patellofemoral arthroplasty: surgical technique and Decision-Making. Arthrosc. Tech. 13 (5), 102962 (2024).
Hutt, J., Dodd, M., Bourke, H. & Bell, J. Outcomes of total knee replacement after patellofemoral arthroplasty. J. Knee Surg. 26, 219–224 (2013).
Beutler, A. I., Cooper, L. W., Kirkendall, D. T. & Garrett, W. E. Jr. Electromyographic analysis of Single-Leg, closed chain exercises: implications for rehabilitation after anterior cruciate ligament reconstruction. J. Athl Train. 37 (1), 13–18 (2002).
Hartmann, H., Wirth, K. & Klusemann, M. Analysis of the load on the knee joint and vertebral column with changes in squatting depth and weight load. Sports Med. 43 (10), 993–1008 (2013).
Lonner, J. H. Patellofemoral arthroplasty. Orthopedics 33, 653 (2010).
Arvesen, J. E. & Wyland, D. J. Patellofemoral replacement with tibial tubercle osteotomy. Arthrosc. Tech. 10 (1), e67–e72 (2021).
Lüring, C. et al. Therapy of isolated arthritis in the patellofemoral joint: are there evidence-based options? (Article in German). Orthopade 40, 902–906 (2011).
Serino, J. 3rd et al. Complications and costs of patellofemoral arthroplasty versus total knee arthroplasty. Knee 41, 58–65 (2023).
Lustig, S., Magnussen, R. A., Dahm, D. L. & Parker, D. Patellofemoral arthroplasty, where are we today? Knee Surgery, sports traumatology. Arthroscopy 20, 1216–1226 (2012).
Kamikovski, I., Dobransky, J. & Dervin, G. F. The clinical outcome of patellofemoral arthroplasty vs total knee arthroplasty in patients younger than 55 years. J. Arthroplasty. 34 (12), 2914–2917 (2019).
Sarda, P. K., Shetty, A. & Maheswaran, S. S. Medium term results of Avon patellofemoral joint replacement. Indian J. Orthop. 45, 439–444 (2011).
Odumenya, M. et al. The Avon patellofemoral joint replacement: five-year results from an independent centre. J. Bone Joint Surg. Br. 92, 56–60 (2010).
Charalambous, C. P. et al. The low contact stress patellofemoral replacement: high early failure rate. J. Bone Joint Surg. Br. 93 (4), 484–489 (2011).
Cardenas, C. & Wascher, D. C. Outcomes of isolated patellofemoral arthroplasty. J. ISAKOS. 9 (4), 796–805 (2024).
Leadbetter, W. B. et al. Patellofemoral arthroplasty: a multi-centre study with minimum 2-year follow-up. Int. Orthop. 33 (6), 1597–1601 (2009).
Peng, G. et al. Patellofemoral arthroplasty versus total knee arthroplasty for isolated patellofemoral osteoarthritis: a systematic review and meta-analysis. J. Orthop. Surg. Res. 16 (1), 264 (2021).
Lonner, J. H. & Bloomfield, M. R. The clinical outcome of patellofemoral arthroplasty. Qld. Gov. Min. J. 44, 271–280 (2013).
Tauro, B., Ackroyd, C. E., Newman, J. H. & Shah, N. A. The lubinus patellofemoral arthroplasty. A five- to ten-year prospective study. J. Bone Joint Surg. Br. 83 (5), 696–701 (2001).
Author information
Authors and Affiliations
Contributions
Xiao Ze and Ye Xie recorded and analyzed patients’ statistics and wrote the main manuscript text.Qirong Dong and Haibin Zhou drafted and revised the manuscript.All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ze, X., Dong, Q., Zhou, H. et al. Midterm outcomes of patellofemoral arthroplasty in patients of isolated patellofemoral arthritis. Sci Rep 15, 41563 (2025). https://doi.org/10.1038/s41598-025-25465-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-25465-8
