
Abstract
Rapid Access Chest Pain Assessment Clinic (RACPAC) offers an outpatient evaluation for patients with troponin-negative, low-to-intermediate risk chest pain. This 10-year study assessed its role in the early identification of patients at cardiovascular risk and compared the modes of coronary investigation performances. A single-centre, observational, retrospective cohort study from July 2012 to July 2022 assessed patients who underwent diagnostic tests: CT coronary angiography (CTCA), treadmill stress echocardiogram (TSE), myocardial perfusion scan (MPS), or invasive coronary angiogram (ICA). True positive cases were defined by obstructive disease on subsequent ICA. Baseline characteristics, investigation choice, results, conversion rates to ICA, and identification of new modifiable risk factors to potentially reduce future cardiovascular events were analysed. A total of 3976 patients with low-to-intermediate risk chest pain, mean age (55.2 ± 11.6) years, 51% male, with prevalent risk factors such as positive family history (49%) and dyslipidaemia (42%). Initial investigations: TSE (49.2%), CTCA (43.7%), MPS (4.6%), and ICA (2.5%). CTCA showed superior performance compared to TSE in positive predictive value (97% vs. 82%), negative predictive value (66% vs. 27%) for those proceeding to ICA despite initial negative/inconclusive results, and attendance rates (97% vs. 92%). Incidental findings occurred in 4% of cases, predominantly with CTCA. New modifiable CVD risk factors were identified in 33% of patients, and 17% had CAD with pre-existing CVD risk factors needing stricter control. Our study highlights the effectiveness of CTCA as a primary investigation for troponin-negative, low-to-intermediate risk chest pain patients, with high predictive values, incidental findings and attendance rates. It also emphasises RACPAC’s potential role in identifying patients at cardiovascular disease risk and perhaps reducing future cardiovascular morbidity and mortality.
Similar content being viewed by others
Introduction
Chest pain frequently emerges as a common presentation to the Emergency Department (ED), accounting for 5–10% of all adult ED admissions1. 41% of these patients are admitted to the hospital for further investigation, with the remainder either discharged or referred for outpatient follow-up2. The associated costs are substantial, particularly when patients are admitted for further investigation. Furthermore, most ED patients with symptoms of acute coronary syndrome (ACS) do not have a cardiac cause for their presentation and the current guideline-based process of assessment of this cohort, according to the National Heart Foundation and Cardiac Society of Australia and New Zealand (NHF/CSANZ) guidelines, requires significant resources including time and cost3.
The contemplation of alternative outpatient pathways offers a promising prospect that could yield mutual benefits for patients and healthcare systems. Establishing specialised chest pain clinics is a notable solution among these pathways. This approach has garnered favourable outcomes on a global scale, particularly within the United Kingdom, showcasing substantial cost reductions by sidestepping the need for hospitalisation, all while upholding unwavering safety standards. The Rapid Access Chest Pain Assessment Clinic (RACPAC) was developed in the United Kingdom in the 1990 s, based on data from the United States of America, to shift the burden of low-risk patients away from hospitals4,5.
The RACPAC was established at the Austin Hospital, Melbourne, Australia, in 2012, based on the United Kingdom model, to provide direct and timely access for patients presenting with chest pain symptoms. Numerous studies have examined the advantages of an RACPAC in terms of safety and efficiency6,7. However, there is currently a scarcity of data on cardiac investigation selection within the RACPAC cohort and the clinic’s capacity to reduce long-term cardiovascular disease events.
Thus, our study aims to evaluate the performance of investigations within a RACPAC cohort and to determine the clinics’ potential as a primary or secondary prevention resource for cardiovascular disease and related events.
Materials and methods
Study design and referral criteria
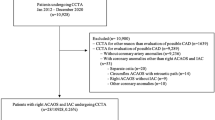
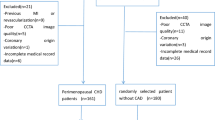
This retrospective, observational, single-centre cohort study utilised patient data from the Austin Hospital RACPAC, a large quaternary referral centre in Melbourne, Australia, from July 2012 to July 2022. Patients attending the clinic were referred from the Austin Hospital ED, other clinical units, or by general practitioners in the community. All patients were required to have low-to-intermediate risk chest pain where ACS was not suspected, as determined by the NHF/CSANZ guidelines8, with no ischemic ECG changes and a negative high-sensitivity troponin result if available at the time of referral. Before 2019, the referred patients fell within the age range of 40 to 75 years old. In 2019, this referral criteria expanded to patients above and below these age limits.
Structure of the RACPAC
The RACPAC at the Austin Hospital operated as a once-weekly clinic staffed by a team of cardiologists, nurse practitioners and liaison nurses. Patients attended their appointment within 21 days of their initial ED presentation. Patients were requested to undergo a series of blood tests, including a full blood count, urea and electrolytes, haemoglobin A1c (HbA1c), blood sugar levels, a lipid profile, a high sensitivity C-reactive protein (hs-CRP) and a troponin level if these tests were not already completed prior to the referral. A patient’s clinical, medical, family and medication history were recorded during the appointment. Subsequently, a cardiologist reviewed the patient’s clinical profile and blood test results, leading to a decision on further investigations. Options included discharge without additional testing or a non-invasive investigation, with choices being a CT Coronary Angiogram (CTCA), Myocardial Perfusion Scan (MPS) or a Treadmill Stress Echocardiogram (TSE) (Fig. 1).

Evaluation of patients at the RACPAC.
From 2011 to 2014, scans were performed using 64-slice scanner technology (LightSpeed, GE Healthcare). Between 2015 and 2020, a 256-slice scanner (Revolution, GE Healthcare) was utilised, and since 2021, scans have been conducted using the advanced 256-slice scanner (Revolution Apex, GE Healthcare). MPS was performed using Single-Photon Emission Computed Tomography (SPECT), with either Technetium-99 m-sestamibi or Thallium-201 selected according to availability. TSE was also performed in combination with dobutamine or adenosine when indicated.
In some cases, an Invasive Coronary Angiogram (ICA) was ordered, recognised as the gold standard for diagnosing and potentially treat underlying coronary artery disease9. If further sequential investigations were required for a patient, these were chosen at the cardiologist’s discretion. The selection of cardiac investigations was based on patient risk factors and the presence of contraindications to specific testing. For instance, individuals with renal impairment were favoured for TSE or MPS, while those with multiple risk factors or mobility issues were likely to undergo CTCA (Fig. 2).

Structural vs. Functional Tests.
After completing all investigations, a recommendation letter, including risk factor modifications, was sent to a patient’s GP and the patient was discharged from the clinic. The RACPAC model offered timely assessment; the median wait time was 19 days (IQR 13–27), compared to conventional outpatient clinical models. It implemented strict referral criteria of low-to-intermediate risk chest pain and limited follow-up duration by discharging patients to their primary care provider for ongoing risk factor modification.
Diagnostic tests
CTCAs were defined as positive if demonstrating > 25% obstructive coronary disease, albeit not being the reason for a patient’s chest pain presentation. Positive CTCA results were further classified as mild (25–49% stenosis), moderate (50–69% stenosis), or severe disease (70–99% stenosis)10. All CTCAs were co-reported by a specialist cardiologist and radiologist. TSEs were defined as positive if they demonstrated inducible ischemia. MPSs were considered positive if an inducible perfusion defect emerged or absent myocardial perfusion was observed at rest and during stress. ICA was the gold-standard investigation and was defined as positive if it demonstrated obstructive coronary disease. ICA’s findings were further categorised as no obstructive CAD, mild-to-moderate disease (medical management alone), severe disease requiring percutaneous intervention (PCI) or severe disease requiring coronary bypass surgery (CABG).
Data extraction
Five authors (H.A.-F., R.A., M.S., Y.L., Z.L.) independently extracted data using a standardised spreadsheet for all patients referred to the clinic over the ten years. Additionally, a random 2% sample of the extracted dataset was independently validated by another investigator. Inter-rater reliability was assessed using Cohen’s kappa, which demonstrated substantial agreement (K = 0.95). Due to the retrospective nature of the study, the need to obtain the informed consent was waived by the Austin Health Ethics Committee (AHEC). All methods were performed in accordance with the guidelines and regulations of AHEC.
Statistical analysis
Statistical analysis was conducted using Stata (Version 17). Descriptive analysis was performed on baseline characteristics of patients. Categorical variables were presented as numbers (percentages), and normality of continuous variables was assessed using the Shapiro–Wilk test, and data were summarised as mean (standard deviation) given their approximately normal distribution. Bar charts were utilised to visually depict the distributions of cardiovascular risk factors and the use of cardiovascular medications. Additionally, baseline blood test results were presented using box plots with outliers removed, and they were further categorised into binary variables with outcomes of normal or abnormal blood test results (see Appendix A for criteria).
The order and overall number of investigations were described with percentages and presented in a flow diagram format. The investigation results were categorised as positive, negative, or inconclusive for evidence of CAD or as patients failing to attend. Incidental findings were also documented for each investigation. Unpaired t-tests were used to compare the results of non-invasive investigations. Additionally, we evaluated the correlation of each non-invasive investigation’s results with ICA results using positive predictive values. We also conducted a descriptive analysis by examining the proportion wiithin each of these investigation cohorts with negative or inconclusive test results who still underwent an ICA and the negative predictive value for these groups.
Finally, the clinic’s capacity for primary and secondary prevention of cardiovascular events was investigated by calculating the percentages of patients with newly identified modifiable cardiovascular risk factors and those diagnosed with coronary disease with adjustable cardiovascular risk factors.
Results
Baseline characteristics
Within the 10-year study period, 3976 patients were planned for review in the RACPAC. The baseline characteristics of this study population are seen in Table 1. The mean age of the cohort was 55.2 ± 11.6 years, with males comprising 51% (2039/3976) of the cohort. The most prevalent cardiovascular risk factors within the cohort included family history of ischemic heart disease (49%), dyslipidaemia (42%), hypertension (38%) and past (21%) or current (19%) smoking. The most frequently prescribed medications in the cohort were ACE inhibitors or ARBs (27%), statins (26%) and Aspirin (17%). Figure 3 illustrates the distributions of cardiovascular risk factors and medication use among the patient cohort. Only medications and risk factors related to cardiovascular disease were included. Notably, 51% of patients were not taking any cardiovascular medications, while 59% had two or more cardiovascular risk factors present.

Risk Factors Present and Cardiovascular Medication Use. Risk factors: Hypertension, Dyslipidaemia, Diabetes Mellitus, Smoking, Peripheral Vascular Disease and FHx of IHD. Cardiovascular medications: ACEi/ARB, BB, CCB, Statin, Ezetimibe, Fenofibrate, Diuretic, SGLT2i, DPP4 or GLP1 Inhibitor, P2Y12 inhibitor and Aspirin.
The baseline blood test results of the cohort are seen in Table 2; Fig. 4. Of the patients who completed the requested baseline blood test results before review, 6% (158/2455) had abnormal troponin levels. A substantial number of patients exhibited abnormal lipid panels, with 71% (1817/2574) having elevated LDL levels. A smaller proportion showed evidence of hypertriglyceridemia, 22% (562/2602) and decreased HDL levels, 1% (276/2555). Of those who completed an HbA1c test, 15.3% (304/1985) had elevated levels, and of those with known haemoglobin levels, 3% (104/3001) were anaemic.

Blood Test Results – Boxplots. Outside values were excluded, and instead, the median value, 25th and 75th percentile values, as well as lower and upper adjacent values, were shown.
Coronary investigation choice
Of the total cohort, 216 patients were discharged without cardiac investigation. Figure 5 presents a flow diagram of the order of tests within the RACPAC for the study population.

Flow diagram of the order of tests within the RACPAC.
In total, 4307 investigations were ordered for patients over the ten years. Among those who underwent further investigations, the initial test of choice was TSE, selected in most cases, 49.2% (1850/3760). This was closely followed by CTCA, 43.7% (1643/3760), then by MPS, 4.6% (174/3760), and finally by ICA, 2.5% (93/3760). Subsequent investigations predominantly involved ICA, accounting for 43% (217/506) of the second tests and 59% (26/43) of the third tests ordered.
It was noted that TSE usage increased from 28.3% of all investigations ordered in 2012 to 60.4% in 2021. Conversely, CTCA use decreased from 63.8% in 2012 to 27.7% in 2021. MPS usage remained low, although it increased over time, reaching 10.1% in 2019.
Coronary investigation results
Overall, 23% (1000/4307) of all planned investigations yielded positive findings of coronary artery disease, while 69% (2974/4307) were negative. 3% (112/4307) were inconclusive, and 5% (221/4307) were not completed due to patients failing to attend. Notably, failure-to-attend rates were initially 29% at the inception of the clinic but steadily declined to 5% by the ninth year, reflecting improved patient adherence over time.
Figure 6 illustrates the percentage of each investigation type (A = CTCA, B = TSE, C = MPS, D = ICA) with positive results, negative results or inconclusive outcomes for CAD. It also displays instances in which patients failed to attend their planned investigation. When comparing non-invasive testing, CTCA had a higher percentage of positive CAD findings, albeit not necessarily severe disease, compared to positive TSE results [37% (635/1720) vs. 3% (58/2028) P < 0.001] and positive MPS results [37% (635/1720) vs. 16% (35/224) P < 0.001]. A more significant proportion of TSEs were left incomplete due to patients failing to attend their investigation in comparison to CTCAs [8% (155/2028) vs. 3% (44/1720) P < 0.001]. Similarly, a higher proportion of MPS scans were not completed in contrast to CTCAs [8% (17/224) vs. 3% (44/1720) P < 0.001]. Among the patients with coronary artery disease on CTCA, 52% (331/635) were classified as having mild disease, 25% (160/635) as moderate, and 23% (144/635) as severe.

Proportion of Investigation Outcomes.
CAD was confirmed in 81% (272/335) of the planned invasive coronary angiograms of cases. Within these instances, 51% (139/272) were categorised as mild to moderate severity requiring medical management alone, 33% (89/272) exhibited severe CAD necessitating PCI and 16% (44/272) demonstrated a degree of severity suitable for coronary bypass grafting.
Incidental findings were present in 4% (159/4307) of all planned investigations. Of note was the substantially higher occurrence of these findings in CTCA scans, 8% (134/1720) when compared to TSE, 1% (18/2028), MPS, 2% (4/224) and ICA, 1% (3/335) investigations. Incidental findings on CTCA encompassed aorto-cardiac anomalies such as aortic root dilation and aortic plaques, 37% (50/134), pulmonary findings like nodules and parenchymal changes 29% (39/134), and gastrointestinal findings, 30% (40/134). Comparatively, all TSE and ICA incidental findings were aorto-cardiac, whilst the few MPS incidental findings were related to osteolytic bone disease (1/224), pulmonary (2/224) and gastrointestinal disease (1/224).
Figure 7 shows Receiver Operator Characteristics (ROC) curves for TSE and CTCA vs. CA. CTCA’s Area under the Curve (AUC) is 0.722, compared to TSE’s AUC of 0.542. This indicates that CTCA is more accurate in diagnosing CAD than TSE.

ROC CTCA vs. TSE against Gold-Standard of Coronary Angiogram.
Correlation with ICA
The positive predictive value of confirming coronary artery disease on ICA was found to be 97% (145/149) for CTCA in comparison to 82% (40/49) for TSE and 90% (18/20) for MPS. Significant disparities emerged in the rates of ICA utilisation for individuals with negative or inconclusive non-invasive results and variations in negative predictive values within these groups.
A smaller proportion of individuals with initially negative or inconclusive CTCA tests proceeded to undergo ICA compared to the TSE group [1% (9/1041) vs. 2% (40/1815) P = 0.008] or the MPS cohort [1% (9/1041) vs. 5% (9/172) P < 0.001]. The negative predictive value favoured the CTCA cohort, 66% (6/9), over the TSE cohort, 27% (11/40) and the MPS group, 22% (2/9). Among patients with negative or inconclusive non-invasive results who went on to be diagnosed with CAD on ICA, severe disease was found in 31% (9/29) of those in the TSE cohort yet was absent in both the MPS and CTCA cohorts.
Primary and secondary prevention of cardiovascular events
The RACPAC assessed modifiable cardiovascular risk factors, including hypertension, diabetes mellitus, dyslipidaemia, and smoking. Among the 3976 patients who attended the clinic, 1333 (33%) received new diagnoses of at least one modifiable cardiovascular risk factor. Specifically, 1% (38/3976) were diagnosed with diabetes mellitus, while 33% (1310/3976) were diagnosed with dyslipidaemia. Overlap existed with 15 patients receiving diagnoses of both conditions simultaneously.
Patients newly diagnosed with CAD who exhibit modifiable risk factors benefit from more rigorous management of risk factors11. Within the RACPAC cohort, 17% (687/3976) of patients were identified as having CAD and at least one modifiable cardiovascular risk factor requiring stricter control. Specifically, 12% (484/3976) had abnormal lipid levels coupled with evidence of CAD, while 2% (98/3976) displayed abnormal HbA1c levels in conjunction with a CAD diagnosis. Additionally, 5% (185/3976) of those with a new CAD diagnosis were current smokers, and 10% (410/3976) had a history of hypertension. Overlapping cases were observed among these patient groups.
Discussion
Our study contrasted the current investigations commonly chosen at an Australian RACPAC and evaluated the clinic’s capacity to recognise patients at cardiovascular risk and act in a primary prevention manner for CAD—furthermore, early identification of non-cardiac incidental findings assisted in early diagnosis and potential active management. To our knowledge, no other studies have investigated these aspects of a RACPAC in real-life practice.
In general, patients sent to the RACPAC were deemed to be at low-to-intermediate risk of acute coronary syndrome based on their clinical history (in ED or via GP), ECG, and troponin levels. On average, our cohort had a baseline cardiovascular risk likely more elevated than the general population, with the majority of patients having at least two cardiovascular risk factors.
Investigation choice and results
Most of the initial investigations for the RACPAC patients were CTCA or TSE. This likely reflects the ease of accessibility to either investigation compared to both MPS and ICA in Australia and the non-invasive and inexpensive nature of both when contrasted to ICA alone10,12. Unsurprisingly, ICA was mainly used as a second or third-line test to confirm or exclude advanced CAD. It was a gold standard diagnostic and potentially therapeutic test when prior testing suggested significant CAD. Alternatively, instances where an ICA was performed despite prior negative testing frequently served the purpose of alleviating patient concerns regarding ongoing episodic chest pain or when a significant clinical suspicion for significant CAD persisted even in the face of negative initial testing.
Most testing showed no evidence of coronary artery disease in patients referred to the RACPAC. Among the non-invasive tests, CTCA had a significantly higher yield of CAD than TSE and MPS. Although these findings may not have caused the patient’s presentation, they facilitated early identification of CAD and established the foundation for primary prevention.
CTCA had a significantly lower proportion of patients failing to complete their appointments. It is unclear why, as all bookings occur via a cardiology liaison nurse, a text message and a phone call to confirm appointments are delivered. However, this could be attributed to longer waiting times for TSE and MPS than CTCA, leading patients to explore alternative pathways through their general practitioners. Additionally, patients undergoing TSE were relatively younger and had fewer risk factors than the CTCA cohort, possibly due to selection bias. This, in turn, might have led to fewer patients needing to undergo the requested investigations.
CTCA had a higher Positive Predictive Value (PPV) and a notably lower proportion of patients with negative or inconclusive results that required a subsequent ICA compared to TSE and MPS. Moreover, CTCA provides additional information on a patient’s CAD status and future risk in the form of severity classification and calcium score13,14,15,16. It is essential to consider the cost differences among CTCA ($700), TSE ($310) and MPS ($449–834)11, the radiation risk associated with CTCA and MPS17, and the difference in investigation results interpretation. Whilst TSE and MPS enable the functional assessment of significant underlying coronary artery disease, CTCA acts as a structural assessment for the presence of coronary artery disease18.
Interestingly, over the 10 year period, utilisation of TSE approximately doubled while CTCA use halved, despite CTCA demonstrating superior diagnostic performance in our cohort. This trend is likely multifactorial. During the COVID-19 pandemic, access to hospital CT scanners was restricted, with priority given to urgent inpatients, leading to reduced availability of CTCA within the RACPAC and greater reliance on TSE, often through external providers. In addition, the referral age criteria were broadened in 2019. This expansion increased referrals of younger patients, who are generally more suited to TSE, and older patients, for whom CTCA may be less favourable due to coronary calcification and comorbidities. These system-level and demographic factors likely explain the observed shift in test utilisation, rather than any change in perceived diagnostic superiority.
Our study highlights and compares the results of non-invasive investigations in an Australian RACPAC. It showed a strong performance of CTCA in comparison to other non-invasive testing in low-to-intermediate risk chest pain patients. Specifically, CTCA was able to effectively rule out CAD, detect incidental findings, risk stratify patients and finally, identify both clinically significant and non-clinically significant CAD, facilitating primary prevention of cardiovascular disease and reducing potential future cardiovascular events.
Primary prevention of cardiovascular morbidity and mortality
Extensive research has delved into the cost-effectiveness and importance of primary prevention of cardiovascular events within at-risk populations19,20,21,22,23,24,25. Although the primary objective of the RACPAC undoubtedly revolves around ruling out coronary artery disease and identifying patients requiring invasive angiography for possible CAD, a secondary and often overlooked aspect is the clinic’s potential for reducing future cardiovascular events through risk factor modification.
A substantial proportion of our cohort exhibited either newly identified risk factors or an uncontrolled risk factor in conjunction with a new diagnosis of coronary artery disease, thereby necessitating stricter risk factor control11. A traditional barrier to effective primary prevention has been the lack of healthcare capital to identify and screen those at risk, with many individuals being lost to follow-up. Compared to traditional models of care, the cost-effectiveness of RACPAC allows it to provide timely and targeted care to a significantly larger catchment of previously neglected patients7. By sheer volume of consultations, specialist RACPAC clinicians can provide targeted cardiac care and advice whilst handing over to local practitioners for ongoing care, maximising the utility of limited public resources. These findings highlight the clinic’s potential to serve at a pivotal moment in implementing modifications, whether through lifestyle changes or pharmacological interventions, to mitigate cardiovascular risk factors.
Our study was not designed to investigate whether RACPAC early intervention resulted in improved long-term outcomes, as it is an observational and non-randomised cohort. Furthermore, to avoid long waiting times, patients were discharged back to their general practitioners with a letter of advice if no invasive assessment occurred. Whether aggressive medical management was implemented in this setting was left to the discretion of the general practitioner in consultation with the patients themselves.
Notably, the Scot-Heart Trial demonstrated that the use of CTCA, compared with standard care alone, led to improved detection of CAD and was associated with a significant reduction in cardiovascular events at five-year follow-up. Hence, the RACPAC is well positioned within the community to play the role of a primary and secondary prevention clinic in addition to rapid assessment of chest pain26. Our group plans to conduct long-term follow-up, during which information about active management will be collected. However, we have opted for a 10-year follow-up period, considering that our cohort is low-to-intermediate risk and relatively young.
Non-cardiac incidental findings
CTCA exhibited a higher detection rate of incidental findings, particularly non-vascular. Although only 8%, this rate remained significantly higher than other imaging modalities. Findings varied from simple solitary pulmonary nodules requiring regular follow-up to advanced lung disease necessitating urgent attention. Some of these findings would have been missed if CTCA was not the test of choice and could have resulted in adverse outcomes. Robertson and his colleagues have only looked at the cost-effectiveness of following up on solitary pulmonary nodules reported on CTCA but have yet to mention the related costs of other findings27. To the best of our knowledge, most of what has been published are case reports, and there is no study investigating these other incidental findings on a CTCA, how they are managed, or the cost involved. Moreover, as Teng et al. said, “An Opportunity to Seize From Low Hanging Fruits”28 in regards to incidental findings of calcified coronary arteries on CT chest, we believe this similarly is an opportunity to recognise pathologies that could have been missed potentially preventing future morbidity and mortality.
Limitations
The main limitations of this retrospective cohort study stem from its observational nature, single-centre design and selection bias. As with many observational studies, the non-randomisation of the study cohort resulted in baseline characteristic differences between different investigation cohorts (See Table B1 and B2), which are likely to impact the reviewed statistics. Patients chosen to undergo a CTCA were found to have higher baseline risks than those undergoing TSE or MPS. This elevated risk and, therefore, higher prevalence of CAD would undoubtedly increase positive finding yields, PPV, and rates of incidental findings (assuming increased comorbidity risk)29 and potentially increase investigation attendance rates30. We understand this is due to a selection bias; hence, these statistics should be interpreted in the context of these differences.
Further notable limitations of the study are the differences in the stratification of positive findings of the investigations. While a positive result from a TSE or MPS resulted in subsequent ICA, most CTCAs with mild or moderate CAD did not result in ICA and were omitted when comparing PPVs. Hence, a significant proportion of the CTCA cohort with mild or moderate disease have an unknown PPV, and our study’s interpretation of their CTCA results is uncertain. Despite this, other research has alluded to the reliability of a CTCA’s disease classification31.
Finally, whilst our study alludes to the clinic’s capacity to act in a primary prevention manner, it does not provide related outcome data. Therefore, overdiagnosis and overtreatment of newly diagnosed coronary artery disease that may never become clinically relevant without treatment is a distinct possibility. Further research, facilitated through outcome data and randomised control trials, would be necessary to provide a more comprehensive understanding of the benefits and potential drawbacks of primary prevention interventions at the RACPAC. That said, our research group has already set the foundation for assessing the long-term (10-year) outcome of the RACPAC cohort, including a focus on Major Adverse Cardiovascular Events (MACE).
Despite this, our study aims to show RACPAC’s current effectiveness in real-world non-invasive investigations and cardiovascular event prevention. It specifically suggests CTCA as a reliable test for ruling out and identifying coronary artery disease in this cohort.
Conclusion
Our study highlights CTCA’s high yield, reliability, and capacity to rule out coronary artery disease in a RACPAC setting compared to other non-invasive tests. Secondly, our study emphasises the RACPAC’s capacity to act in a primary prevention manner, offering pivotal interventions to mitigate future cardiovascular morbidity and mortality. Finally, the higher rate of non-cardiac incidental findings on CTCA is an opportunity to seize low-hanging fruits.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Kuhlman, J. et al. Clinical transformation through change management case study: chest pain in the emergency department. EClinicalMedicine 10, 78–83 (2019).
Australian Institute of Health and Welfare. National heart foundation of australia., national centre for monitoring cardiovascular disease (Australia). Heart, stroke and vascular diseases: Australian facts 2004.
Cullen, L. et al. Cost and outcomes of assessing patients with chest pain in an Australian emergency department. Med. J. Aust. 202, 427–432 (2015).
Goodacre, S. View from the united kingdom: chest pain center progress. Crit. Pathw. Cardiol. 4, 131–133 (2005).
Goodacre, S. W. Should we Establish chest pain observation units in the UK? A systematic review and critical appraisal of the literature. J. Accid. Emerg. Med. 17, 1–6 (2000).
Black, J. A. et al. Evaluating the benefits of a rapid access chest pain clinic in Australia. Med. J. Aust. 210, 321–325 (2019).
Kozor, R. et al. Rapid access chest pain clinics: an Australian cost-benefit study. Heart Lung Circ. 31, 177–182 (2022).
Chew, D. P. et al. National heart foundation of Australia & cardiac society of Australia and new zealand: Australian clinical guidelines for the management of acute coronary syndromes 2016. Heart Lung Circ. 25, 895–951 (2016).
Mangla, A., Oliveros, E., Williams, K. A. & Sr., Kalra, D. K. Cardiac imaging in the diagnosis of coronary artery disease. Curr. Probl. Cardiol. 42, 316–366 (2017).
Gary Leiw, M. F. & Stephen Worthley. Noninvasive Coronary Artery Imaging: Current Clinical Applications (Cardiac Society of Australia and New Zealand guideline, 2010).
Sidney, C. et al. Stein and Kathryn A. Taubert. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update. Circulation 124, 2458–2473 (2011).
David Prior, A. M. Cardiac stress testing stress electrocardiography and stress echocardiography. Aus. Fam. Physician. 41, 119–122 (2012).
Mehta, A. et al. Predictive value of coronary artery calcium score categories for coronary events versus strokes: impact of sex and race: MESA and DHS. Circ. Cardiovasc. Imaging. 13, e010153 (2020).
Chua, A., Blankstein, R. & Ko, B. Coronary artery calcium in primary prevention. Aust J. Gen. Pract. 49, 464–469 (2020).
Fyyaz, S. et al. Computed tomography coronary angiography: diagnostic yield and downstream testing. Clin. Med. (Lond). 20, 81–85 (2020).
Rossi, A. et al. Quantitative computed tomographic coronary angiography: does it predict functionally significant coronary stenoses? Circ. Cardiovasc. Imaging. 7, 43–51 (2014).
Cordiner, D. et al. Estimates of radiation exposure and subsequent risk of malignancy due to cardiac imaging in the emergency department for evaluation of chest pain: a cohort study. Coron. Artery Dis. 30, 626–628 (2019).
Brenna, C. T. A. A. F. et al. Chest pain investigation in patients at low or intermediate risk: what is the best first-line test to rule out coronary artery disease? Can. Fam Physician. 66, 24–30 (2020).
Ettehad, D. et al. Blood pressure Lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet 387, 957–967 (2016).
Force, U. S. P. S. T. et al. Statin Use for the primary prevention of cardiovascular disease in adults: Us preventive services task force recommendation statement. JAMA 328, 746–753 (2022).
Franco, O. H., der Kinderen, A. J., De Laet, C., Peeters, A. & Bonneux, L. Primary prevention of cardiovascular disease: cost-effectiveness comparison. Int. J. Technol. Assess. Health Care. 23, 71–79 (2007).
Cobiac, L. J., Magnus, A., Barendregt, J. J., Carter, R. & Vos, T. Improving the cost-effectiveness of cardiovascular disease prevention in australia: a modelling study. BMC Public. Health. 12, 398 (2012).
Okorare, O. et al. Smoking cessation and benefits to cardiovascular health: a review of literature. Cureus 15, e35966 (2023).
Wing, R. R. et al. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care. 34, 1481–1486 (2011).
Stewart, J., Addy, K., Campbell, S. & Wilkinson, P. Primary prevention of cardiovascular disease: updated review of contemporary guidance and literature. JRSM Cardiovasc. Dis. 9, 2048004020949326 (2020).
Adamson, P. D. & Newby, D. E. The SCOT-HEART Trial. What we observed and what we learned. J. Cardiovasc. Comput. Tomogr. 13, 54–58 (2019).
Robertson, J. et al. Incidental pulmonary nodules are common on Ct coronary angiogram and have a significant cost impact. Heart Lung Circ. 28, 295–301 (2019).
Teng, L. E. K. L., Lok, S. C., O’Rourke, E. & Premaratne, M. An opportunity to seize from low hanging fruits: capitalising on incidentally reported coronary artery calcification. Heart Lung Circ. 32, 1222–1229 (2023).
Buddeke, J. et al. Comorbidity in patients with cardiovascular disease in primary care: a cohort study with routine healthcare data. Br. J. Gen. Pract. 69, e398–e406 (2019).
Tenny, S. H. M. Jan. Prevalence. In: StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2024 ;PMID: 28613617. (2023).
Iyengar, S. S. et al. Diagnostic accuracy of high-definition CT coronary angiography in high-risk patients. Clin. Radiol. 71, 151–158 (2016).
Author information
Authors and Affiliations
Contributions
H.A.-F. and R.A. wrote the main manuscript text. Z.L and Y.C.L. performed the statistical analysis. F.P., N.B., and C.Z. provided administrative assistance. A.A-F. reviewed the manuscript. All authors extracted the data.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Al-Fiadh, H., Azzopardi, R., Shawki, M. et al. An Australian experience of the Rapid Access Chest Pain Assessment Clinic. Sci Rep 15, 43601 (2025). https://doi.org/10.1038/s41598-025-25478-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-25478-3
