
Abstract
Postoperative intracranial infection represents significant complications closely associated with a poor prognosis in patients with brain tumors. We aimed to investigate the value of cerebrospinal fluid (CSF) parameters in detection and monitoring of postoperative intracranial infection. This study assessed the diagnostic values CSF parameters for postoperative intracranial infection through the ROC curve and Fisher discriminant model, as well as the prognostic values through Kaplan-Meier analysis and multivariate Cox regression in brain tumor patients. 7 statistically significant CSF variables were extracted and identified, leading to the development of the infection discrimination model with a diagnostic sensitivity of 86.79% and a specificity of 77.01%. Its performance was in excellent agreement with clinical confirmation, as indicated by a κ value of 0.609, which also was validated by the external validation, with 92.86% sensitivity and 64.00% specificity, as well as a κ value of 0.602. Furthermore, elevated levels of CSF total protein, leukocytes, multinucleated cells, and multinucleated cell ratio, along with reduced glucose levels, were found to be associated with prolonged infection control, underscoring their prognostic significance. Multivariate Cox regression analyses identified elevated CSF total protein, reduced glucose and increased leukocyte count as independent predictors of prolonged time to infection control. We established and validated a Fisher model to objectively and quantitatively discriminate true-positive intracranial infection, as well as predicted the infection control time using CSF parameters.
Similar content being viewed by others


Introduction
Postoperative intracranial infection represents significant complications closely associated with a poor prognosis in patients with brain tumors, primarily resulting from pathogens invading the brain parenchyma and meninges1. Although it has been decreased markedly due to ongoing advancements in aseptic techniques and the implementation of prophylactic antibiotics2, the complete elimination of postoperative intracranial infections still remains a challenge3. A retrospective analysis of brain tumor patients who underwent craniotomy revealed an overall incidence of 6.8%4. Therefore, timely and accurate identification is essential to initiate appropriate treatment and improve prognosis for patients diagnosed with intracranial infection5.
The gold standard for diagnosis of intracranial infection is cerebrospinal fluid (CSF) culture6, which is crucial for antimicrobial susceptibility testing and molecular epidemiology7. However, it requires at least one day for results with the limited sensitivity8, as well as the high negative rates ranging from 10% to 40%, which is largely because prophylactic antibiotics during the perioperative period can lead to a decrease in culture yield9,10. Besides, Other methods have been also used in clinical application. For example, polymerase chain reaction (PCR) and metagenomic next-generation sequencing (mNGS) are increasingly being applied in clinical laboratories for unbiased culture-independent diagnosis7,11. Nevertheless, their positive detection rate still depends on the presence of pathogens, like CSF culture12. Relying solely on CSF pathogens for confirming intracranial infection may lead to treatment delays, ultimately adversely affecting patient prognosis13.
Given that, clinicians often rely on clinical features, such as the classic triad of bacterial meningitis (fever, headache, and neck stiffness), as well as laboratory parameters to initiate empiric antimicrobial therapy, but is commonly restricted by the limited specificity and sensitivity14,15. Trauma, hemorrhage and postoperative aseptic inflammation are capable to induce some changes not only in hemogram and procalcitonin (PCT) levels, but also in CSF cytological and biochemical characteristics, interfering with the diagnosis of intracranial infection10,16,17. However, a large portion of patients with shunt meningitis exhibited normal leukocyte count, protein levels and CSF glucose to blood glucose ratio in CSF18, indicating the complexity of intracranial infections, and it might be unsuitable to assess these infections based solely on one or a few parameters considering the subjective judgment of clinicians19.
In the current study, we retrospectively analyzed the inspection parameters in CSF and circulation, including cytological and biochemical characteristics in the patients with brain tumors. Accordingly, we stablished and validated a Fisher model to objectively and quantitatively discriminate true-positive intracranial infection, as well predicted the infection control time using CSF parameters, providing the novel insight for the early identification and outcomes evaluation of postoperative intracranial infection.
Materials and methods
Study population
A total of 694 brain tumors patients at Shandong Cancer Hospital and Institute from February 1st, 2020, to April 30th, 2024, were enrolled in the current study. Patients were included ≥ 16 years diagnosed with intracranial tumor who were subjected to neurosurgery and sampled for CSF culture. Exclusion criteria included the following: age < 16 years; no surgery performed; >1 dose antibiotics; absence of a brain tumor; incomplete information; other infectious, immune system disorders, psychiatric abnormalities, metabolic diseases. The external validation cohort was conducted using 81 independent cases from the Affiliated Hospital of Jining Medical University, all of which strictly met the predefined inclusion and exclusion criteria. This study was reviewed and approved by the Ethics Committee of Shandong Cancer Hospital Affiliated to Shandong First Medical University and Shandong Academy of Medical Sciences in accordance with the Declaration of Helsinki. As a retrospective analysis of irreversibly anonymized clinical data, the requirement for written informed consent was formally waived by the Ethics Committee. All information obtained from patient files was treated confidentially, and no patient-identifying information was captured.
Diagnostic criteria for intracranial infection
Post-neurosurgical intracranial infection was determined by the doctor in charge when the patient met any of the following diagnostic criteria: (1) clinical diagnosis: high fever, intracranial hypertension, cloudy or purulent CSF, white blood cells ≥ 10 × 106, serum glucose < 2.2mmol/L, and CSF glucose/serum glucose ≤ 0.4; (2) positive results for bacterial culture in specimen smear, drainage tube head, implant and CSF on the basis of clinical diagnosis.
Data collection
CSF collection adhered to the following protocol: samples were obtained via aseptic lumbar puncture (L3-L4 or L4-L5 interspace) or existing ventricular drainage catheters, with specimens collected within 24 h after the onset of postoperative symptoms (e.g., fever > 38 °C, new-onset headache, or meningeal signs) for suspected infection cases, or systematically during postoperative days 3–7 for routine monitoring; all samples underwent cytological, biochemical, and microbiological analyses within 30 min of collection to ensure validity.
Microbial detection included direct plating and automated broth enrichment cultivation. Fresh samples are inoculated onto Columbia blood agar and chocolate agar plates for direct culture under 5% CO₂ aerobic conditions. Microbial growth observed within 24–48 h is identified using the BRUKER microflex MALDI TOF/TOF mass spectrometer (BRUKER Corporation, Massachusetts, USA). Concurrently, residual CSF is transferred into culture bottles for 5-day enrichment. Positive signals undergo false-positive screening via time-to-positivity thresholds and growth curve slope analysis. Positive broths are Gram-stained, subcultured onto agar plates, and incubated for 24 h; colonies are confirmed using the same MALDI-TOF platform. A BD Phoenix M50 automated microbial system (Becton, Dickinson and Company, New Jersey, USA) was adopted for bacterial drug sensitive analysis. All procedures were conducted in accordance with the manufacturers’ instructions and the BC standards of the Clinical Laboratory Standards Institute.
For physicochemical parameters of CSF, Beckman Coulter analyzer AU5800 (Beckman Coulter, Brea, CA, USA) was used to measure total protein, glucose levels and chlorine ion; Sysmex XN-550 (Sysmex Corporation, Kobe, Japan) was employed for assay of cell counts and classification. Qualitative tests including CFS color, turbidity and Pandy’s results were performed by the senior inspection technicians. Interpretation standard referred to the operating procedures for clinical examinations in China. The “0” was assigned for negative (colorless, transparent, and (-) Pandy’s test), and “1” for positive (colored, non-transparent, (+) Pandy’s test) of qualitative tests, respectively.
For hematological parameters, Roche Cobas e801 analyzer (Roche Diagnostics GmbH, Mannheim, Germany) was used to quantify the serum PCT, with level of < 0.05 ng/mL considered normal. High Sensitivity C-reactive Protein (CRP) and blood cell counts and classifications were analyzed using an automatic hematological analyzer Mindray BC-7500 (Mindray Healthcare, Shenzhen, China). The CRP reference value provided by the manufacturer was < 10 mg/L.
Statistical analysis
Statistical analysis was performed using SPSS 26.0 statistical software (SPSS, Chicago, IL, USA) and GraphPad Prism version 9.5 (GraphPad Software, San Diego, CA, USA). For comparisons of non-normal continuous variables, Mann-Whitney U-test for two independent samples. Categorical data were compared using X² test or Fisher’s exact test. For the diagnostic accuracy the following were calculated: sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), and the area under the curve (AUC) of the receiver operating characteristic (ROC) curve. The optimal cut-off points were determined using the Youden index. The discriminant model was obtained by Fisher discriminant analysis. Suspected infection cases were imported into the interpretation model to verify the validity of the discriminant function. Consistency between model estimation and clinical confirmation was assessed by Kappa test. Infection control time was measured from the time of confirming intracranial infection to clinical evaluation of infection relief or discharge. Kaplan-Meier (KM) survival curves were plotted to visualize the relationship between different parameter levels and infection control time, and the Log-rank test was used to examine intergroup differences. Building on this, multivariate Cox proportional hazards regression models were further applied to identify independent predictors influencing infection control time. Data were presented as the percentages or median (interquartile range, IQR). Significance was established at P < 0.05.
Results
Study cohort and microbiological characteristics of infected samples
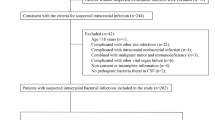
According to inclusion and exclusion criteria, 389 patients were eligible and underwent CSF culture. Among the 92 culture-positive patients, 35 were excluded due to surgical incision and scalp infections, actinobacterial and fungal infections, inconclusive diagnoses, or contamination. Consequently, a total of 57 patients with positive CSF culture were defined as the “Infection Group”. In the 297 CSF negative patients, 157 patients with normal hemogram and clinical presentation were defined as “Non-infected Group”; the other 140 patients were defined as “Suspected Group” due to following at least one of the below criteria1,12,15,19,20: clinical manifestation of intracranial infection (fever > 38 °C, headache, meningeal sign, or focal neurological symptoms); abnormal hemogram or/and inflammatory mediators (PCT, or/and CRP). Flow diagram of study population was shown in Fig. 1. The clinical and laboratory features were summarized in Table 1.

Flow diagram of episodes and classification for study. CSF, cerebrospinal fluid.
Among 57 patients in the infected group, a total of 68 pathogens were identified by CSF culture. 8 patients suffered from multiple pathogens, including 5 with two pathogen infections and 3 with three pathogen infections. The remaining were infected with a single pathogen. In 42 cases with gram-positive bacteria, coagulase-negative Staphylococcus predominated (25 cases, 36.76% of total positive cultures), followed by Viridans Streptococci (13 cases, 19.12% of all positives). Among 26 gram-negative bacteria, Acinetobacter spp. and Enterobacter spp. were common pathogens (8 cases, 11.76% of all positives, respectively). Detailed results regarding bacterial composition and distribution of muti-drug resistant bacteria isolated from CSF specimens were shown in Fig. 2.

Distribution of pathogens in CSF for intracranial infection. (A) The bacterial composition isolated from CSF culture specimens submitted after surgery. (B) The distribution of muti-drug resistant bacteria. spp., species pluralis; MRSA, methicillin-resistant staphylococcus aureus; MRSCoN, methicillin-resistant staphylococcus coagulase-negative; CRE, carbapenem-resistant enterobacterales; ESBL, extended-spectrum β-lactamase; CR-PA, carbapenem-resistant pseudomonas aeruginosa; CR-AB, carbapenem-resistant acinetobacter baumannii.
Diagnostic accuracy of aberrant CSF parameters for intracranial infection
First, we compared the differential physicochemical parameters between infected and non-infected groups. As shown in Fig. 3, the levels of CSF total protein, leukocytes, multinucleated cells and proportion of multinucleated cells were significantly increased (P < 0.0001), while the CSF Cl− (chlorine ion, C-Cl−), glucose and glucose ratio (CSF: Serum, C-Glu/S-Glu), were lower in infected group (P = 0.0015, < 0.0001, 0.0016, respectively) (Fig. 3A and B). Moreover, PCT and CRP were significantly elevated when intracranially infected (P < 0.0001, respectively; Fig. 3C). Similarly, significant differences in color, turbidity and Pandy’s tests were also observed between the two groups (P < 0.0001, respectively; Table 2), The median levels and IQR of index tests were shown in Table S1.

Comparisons between infected group and non-infected group. The CSF and parameter levels of C-TP, C-Cl-, C-Glu, C-Glu/S-Glu (A), C-leukocytes, C-multinucleated, C-multinucleated % (B), PCT and CRP (C). The horizontal lines represented the median. Statistical significance was calculated with Mann-Whitney test. **, p < 0.01; ****, p < 0.0001; C-TP, CSF total protein; C-Cl-, CSF chlorine ion; C-Glu, CSF glucose; C-Glu/S-Glu, CSF: serum glucose ratio; C-multinucleated, CSF multinucleated cells; C-multinucleated %, CSF proportion of multinucleated cells; PCT, procalcitonin; CRP, hypersensitive C-reactive protein.
Next, ROC curves were employed to evaluate the diagnostic accuracy of the above parameters for intracranial infection. It was found that CSF leukocyte count possessed favorable accuracy with an AUC of 0.927, followed by multinucleated cells with the AUC of 0.909. CSF parameters including total protein, Cl−, glucose, glucose ratio (CSF: Serum) and proportion of multinucleated cells demonstrated the AUCs of 0.846, 0.645, 0.799, 0.752 and 0.747, respectively (Fig. 4A) These data were summarized in Fig. 4B and Table S2., in which cut-off values were calculated based on the best sensitivity and specificity (Youden index), which could better help clinicians determine whether the presence of postoperative intracranial infections.

Accuracy of CSF parameters in distinguishing post-neurosurgical intracranial infection in patients with brain tumors. ROC curves of C-TP, C-Cl-, C-Glu, C-Glu/S-Glu (A), C-leukocytes, C-multinucleated, C-multinucleated % (B) for the diagnosis of post-neurosurgical intracranial infection. (C) AUC with 95% CI and P-value of ROC curves. C-TP, CSF total protein; C-Cl-, CSF chlorine ion; C-Glu, CSF glucose; C-Glu/S-Glu, CSF: serum glucose ratio; C-multinucleated, CSF multinucleated cells; C-multinucleated %, CSF proportion of multinucleated cells; AUC, area under the ROC curve.
Establishment of discriminant model for the verification of suspected cases
According to aberrant CSF parameters by variable comparison analysis (Mann–Whitney U-test or X² test), 9 variables were initially selected. CSF Cl− were excluded due to insufficient diagnostic efficacy (AUC = 0.645). Subsequent multicollinearity diagnosis revealed significant collinearity between leukocyte count and multinucleated cell count (variance inflation factor, VIF > 10). Given the inclusion of multinucleated cells ratio containing equivalent pathological information, the redundant multinucleated cell count variable was eliminated. The final Fisher discriminant model incorporated 7 independent variables, yielding the intracranial infection discrimination equation, < F=-8.801 + 0.598× total protein + 2.704× glucose + 0.000171× leukocytes + 0.044× proportion of multinucleated cells + 0.920× color-0.465× turbidity + 4.645× Pandy’s tests>.
To verify the validity of the above model, 140 cases “Suspected Group” as selected in Fig. 1 were taken into the discriminant model, and the calculated results were compared with the final clinical diagnosis (53 infected and 87 uninfected cases). The result showed that the diagnostic sensitivity and specificity of this model were 86.79% and 77.01%, respectively. Kappa analysis demonstrated the favorable consistency between the discriminant model and final clinical diagnosis (κ = 0.609, P < 0.0001; Table 3).
To further validate the discriminative model, an external verification was performed using 81 independently collected samples from external medical institutions that met the inclusion criteria. The model’s outputs were compared with definitive clinical diagnoses. Results revealed a diagnostic sensitivity of 92.86% and specificity of 64.00%. Kappa agreement analysis indicated substantial concordance between the model predictions and clinical diagnoses (κ = 0.602, P < 0.0001; Table 4).
CSF parameter indicators and intracranial infection outcomes
After CSF culture and Fisher discriminant analysis, a total of 123 intracranial infection patients were identified, and involved into the follow-up analysis for infection control time. 2 patients were excluded due to the incomplete data (Fig. 5). Finally, 121 infected patients were divided into two groups based on the median levels of various CSF parameter and subjected to KM survival curve. As shown in Fig. 6A, high CSF total protein, leukocytes, multinucleated cells and proportion of multinucleated cells as well as low glucose had significantly longer infection control time (P = 0.0003, < 0.0001, < 0.0001, 0.0063, 0.0002, respectively), indicating it was closely correlated with prognosis of intracranial infection. Furthermore, elevated CSF total protein (HR = 1.51, 95% CI: 1.02–2.23), reduced glucose (HR = 1.84, 95% CI: 1.22–2.78), and increased leukocyte count (HR = 2.34, 95% CI: 1.06–5.14) were identified as independent predictors of prolonged time to infection control in multivariable Cox regression analyses (all p < 0.05, Table 5).

Flowchart for follow up of Intracranial Infection.

CSF parameter indicators were correlated with intracranial infection outcomes. KM analysis was conducted on infection control time by using various CSF parameter indicators such as C-TP, C-Glu, C-leukocytes, C-multinucleated, C-multinucleated % (A), and high, medium and low- risk group groups (B). C-TP, CSF total protein; C-Glu, CSF glucose; C-multinucleated, CSF multinucleated cells; C-multinucleated %, CSF proportion of multinucleated cells.
We defined the CSF parameters with longer infection control time as “+” to represent high-risk, and “+” number for each patient based on five significant indicators was calculated. Patients with indicators ranging from 4 to 5 “+”, 2 to 3 “+”, and ≤ 1 “+” were sequentially classified as high, medium and low- risk group. As shown in Fig. 6B, low-risk group presented the shorter infection control time compared with high and medium-risk group (P < 0.0001).
Discussion
Postoperative intracranial infection remains a significant worldwide problem, resulting in substantial morbidity/mortality if not combatted quickly and energetically21,22. Therefore, it is urgently needed to identify pathogens timely and accurately for postoperative infection control23. In current study, we established and validated a Fisher model to discriminate postoperative intracranial infections, as well predicted their outcome in brain tumors patients based on the physicochemical parameters.
CSF culture is the gold standard for diagnosing intracranial infection, often restricted by high false-negative rate24. In the current study, 53 patients were finally diagnosed as positive intracranial infection from 140 negatively cultured patients. It meant that false-negative rate of CSF culture was 37.86% in our cohort, consistent with previous researches3,25,26, which might be closely linked to the widespread use of preventive antibiotics27. Given that, we established discriminant model for verification of suspected infection, possessing overall accuracy of 80.71% with 86.79% sensitivity and 77.01% specificity. This model utilized the most common clinical CSF parameters, could provide timely diagnostic information for effective clinical management within one hour, overcoming the delays by CSF culture8. It was independent of subjective judgment of the clinician19, and exerted excellent consistency with the final clinical diagnosis as demonstrated by Kappa analysis. Taken together, we established a timely and accurate model for objective quantification of intracranial infections.
Due to poor clinical outcomes, empirical antimicrobial treatment is usually started in the absence of bacteriological results28. It’s important to find rapid screening indicators to predict the prognosis of intracranial infections. Previous study had demonstrated heparin-binding protein (HBP), IL-6, IL-10, and PCT in the CSF could be an important indicator for incidence and clinical outcomes of post-neurosurgical intracranial infection1. This study aimed to investigate the prognosticative role of laboratory indexes in disease monitoring. Through KM analysis and multivariable Cox regression, we found that the conventional CSF parameters measured at the onset of infection were associated with the duration of infection control, suggesting that CSF examination might be beneficial in assessing the prognosis of patients with intracranial infection. Nevertheless, the computed results from Fisher discriminant model were not incorporated into the analyses. It was initially configured to predict early intracranial infection between positive and negative CSF bacterial culture groups, and in turn validated the consistency between the discriminant model and final clinical diagnosis in the suspected group. The Fisher discriminant model aimed to reduce the false negative rate of CSF culture, as well as to promote the diagnosis but not prognosis.
We also analyzed statistical differences of intracranial infections among different modus operations, which indeed demonstrated a significant different infection rate, indicating histopathological diagnosis of tumors, along with the surgical approach, play a crucial role in the development of intracranial infection29. Previous researches had demonstrated that prolonged operative time, inadequate surgical wound cleaning, placement of extracorporeal CSF drainage or monitoring devices, and postoperative CSF leakage were the independent risk factors for intracranial infection4, and incidence of postoperative intracranial infection varies widely30,31,32. This did not undermine the conclusion of the current study. Its primary objective wasn’t to evaluate the risk factors associated with intracranial infection, but rather to predict its occurrence, reduce the false-negative rate of CSF culture, promote early and rapid diagnosis and treatment, and ultimately improve patient survival rates and clinical outcomes.
Notably, our Fisher discriminant model demonstrates three key advantages. First, it significantly enhances clinical efficiency. By integrating routine CSF parameters, the model delivers diagnostic results within one hour, representing a substantial improvement in turnaround time compared to the complex nomogram model33, while also offering superior cost-effectiveness relative to the biomarker detection protocol established by Pan et al.1. Second, the model introduces notable methodological innovation. By proactively incorporating 37.86% (53/140) of culture-negative infection cases with prior antibiotic exposure, it establishes a distinct comparative perspective. This contrasts with the approach of Zhai et al.19 that was confined solely to culture-positive cases. Finally, the model’s robustness was rigorously validated through a multimodal approach. The integrated diagnostic-prognostic solution demonstrated consistent performance across both internal (κ = 0.609) and external (κ = 0.602) validation cohorts. Collectively, characterized by its rapid turnaround, cost-effectiveness, and adaptability to antibiotic usage scenarios, this solution presents a comprehensive and practical approach to intracranial infection management.
Several limitations should be carefully considered in the present study. First, the retrospective design research is based on historical clinical data, with limitations of potential bias and incomplete data. Therefore, not all patients underwent completely identical laboratory testing protocols (see Table S3). Second, we acknowledge the limitations of CSF culture as the diagnostic gold standard. Its high false-negative rate (66/297 in this cohort) may affect the accuracy of case inclusion, posing challenges particularly in definitively confirming the infection status in culture-negative cases. Moreover, empirical antibiotic use prior to CSF sampling contributes significantly to the high false-negative culture rate. This necessary clinical practice consequently limits the availability of microbiologically confirmed “true positive” cases for model training. Finally, the relatively small cohort size (especially the confirmed infection group, n = 53) reflects the low incidence of postoperative intracranial infection. Although this constrains statistical power and the generalizability of the results, it aligns with real-world diagnostic challenges and highlights the clinical need this study aims to address. Another notable limitation is the exclusive focus on postoperative brain tumor patients. Althoug these CSF parameters are universally employed in diagnosing neurosurgical infections, the generalizability of our specific criteria to other neurosurgical populations (such as trauma or vascular cases) remains unestablished. We hypothesize that the distinct pathophysiological mechanisms or baseline clinical characteristics of these patient groups could necessitate differential the model optimization process, including parameter weighting, combination, and diagnostic cut-off values, to ultimately validate its broader clinical applicability.
In summary, we have developed and validated a multi-parameter CSF-based discriminant model that effectively predicts postoperative intracranial infection in brain tumor patients (86.79% sensitivity, 77.01% specificity) with significant prognostic value. To advance clinical implementation, we propose integrating the algorithm into hospital laboratory information systems for automated real-time risk scoring during routine CSF analysis, alongside advocating its inclusion as an auxiliary diagnostic criterion in neurosurgical infection guidelines through professional society collaborations. Future efforts will focus on enhancing diagnostic sensitivity through novel biomarkers (e.g., CSF IL-6, HBP, mNGS), conducting large-scale prospective trials to validate impacts on antibiotic initiation timing and outcomes, and exploring dynamic CSF parameter monitoring to guide antibiotic de-escalation strategies.
Data availability
The data used and analyzed during the current study are available from the corresponding authors upon reasonable request.
References
Pan, X. et al. Diagnostic, monitoring, and prognostic value of combined detection of cerebrospinal fluid heparin-binding protein, interleukin-6, interleukin-10, and procalcitonin for post-neurosurgical intracranial infection. Cytokine 179, 156593 (2024).
Ratilal, B., Costa, J. & Sampaio, C. Antibiotic prophylaxis for surgical introduction of intracranial ventricular shunts. Cochrane Database Syst. Rev. 2006 (3), CD005365 (2006).
Chen, C. et al. The incidence and risk factors of meningitis after major craniotomy in China: A retrospective cohort study. PLoS One. 9 (7), e101961 (2014).
Shi, Z. H. et al. Post-craniotomy intracranial infection in patients with brain tumors: A retrospective analysis of 5723 consecutive patients. Br. J. Neurosurg. 31 (1), 5–9 (2017).
Olie, S. E. et al. Diagnostic accuracy of inflammatory markers in adults with suspected central nervous system infections. J. Infect. 88 (3), 106117 (2024).
Zheng, G. et al. Development and verification of a discriminate algorithm for diagnosing post-neurosurgical bacterial meningitis-A multicenter observational study. J. Clin. Lab. Anal. 34 (2), e23069 (2020).
Wu, H. M. et al. Accuracy of real-time PCR, gram stain and culture for Streptococcus pneumoniae, neisseria meningitidis and haemophilus influenzae meningitis diagnosis. BMC Infect. Dis. 13, 26 (2013).
Zhang, Z. et al. Epidemiology of patients with central nervous system infections, mainly neurosurgical patients: A retrospective study from 2012 to 2019 in a teaching hospital in China. BMC Infect. Dis. 21 (1), 826 (2021).
Brouwer, M. C., Tunkel, A. R. & van de Beek, D. Epidemiology, diagnosis, and antimicrobial treatment of acute bacterial meningitis. Clin. Microbiol. Rev. 23 (3), 467–492 (2010).
Panic, H. et al. Etiology and outcomes of Healthcare-Associated meningitis and Ventriculitis-A single center cohort study. Infect. Dis. Rep. 14 (3), 420–427 (2022).
Corless, C. E. et al. Simultaneous detection of neisseria meningitidis, haemophilus influenzae, and Streptococcus pneumoniae in suspected cases of meningitis and septicemia using real-time PCR. J. Clin. Microbiol. 39 (4), 1553–1558 (2001).
Karvouniaris, M. et al. Current perspectives on the diagnosis and management of Healthcare-Associated ventriculitis and meningitis. Infect. Drug Resist. 15, 697–721 (2022).
Staal, S. L. et al. Granulocytes in cerebrospinal fluid of adults suspected of a central nervous system infection: A prospective study of diagnostic accuracy. Infection 52 (4), 1415–1423 (2024).
Khatib, U. et al. Adults with suspected central nervous system infection: A prospective study of diagnostic accuracy. J. Infect. 74 (1), 1–9 (2017).
Yu, Y. & Li, H. J. Diagnostic and prognostic value of procalcitonin for early intracranial infection after craniotomy. Braz J. Med. Biol. Res. 50 (5), e6021 (2017).
van Soest, T. M. et al. Bacterial meningitis presenting with a normal cerebrospinal fluid leukocyte count. J. Infect. 84 (5), 615–620 (2022).
Lenski, M. et al. Inflammatory markers in serum and cerebrospinal fluid for early detection of external ventricular Drain-associated ventriculitis in patients with subarachnoid hemorrhage. J. Neurosurg. Anesthesiol. 31 (2), 227–233 (2019).
Conen, A. et al. Characteristics and treatment outcome of cerebrospinal fluid shunt-associated infections in adults: A retrospective analysis over an 11-year period. Clin. Infect. Dis. 47 (1), 73–82 (2008).
Zhai, T. et al. Application of combined cerebrospinal fluid physicochemical parameters to detect intracranial infection in neurosurgery patients. BMC Neurol. 20 (1), 213 (2020).
Tunkel, A. R. et al. 2017 infectious diseases society of america’s clinical practice guidelines for Healthcare-Associated ventriculitis and meningitis. Clin. Infect. Dis. 64 (6), e34–e65 (2017).
Meng, Y. et al. Risk factors for surgical site infection after intracranial electroencephalography monitoring for epilepsy in the pediatric population. J. Neurosurg. Pediatr. 22 (1), 31–36 (2018).
Hasbun, R. Healthcare-associated ventriculitis: Current and emerging diagnostic and treatment strategies. Expert Rev. Anti Infect. Ther. 19 (8), 993–999 (2021).
Brouwer, M. C. et al. Dilemmas in the diagnosis of acute community-acquired bacterial meningitis. Lancet 380 (9854), 1684–1692 (2012).
Feng, Z. et al. Diagnostic, monitoring, and prognostic value of combined detection of lactate dehydrogenase, beta2-transferrin, and interleukin-10 for acute intracranial infections. Am. J. Transl Res. 13 (4), 2581–2589 (2021).
McClelland, S. 3rd, Hall, W. A. & rd and Postoperative central nervous system infection: Incidence and associated factors in 2111 neurosurgical procedures. Clin. Infect. Dis. 45 (1), 55–59 (2007).
Kourbeti, I. S. et al. Risk factors associated with postcraniotomy meningitis. Neurosurgery. 60(2), 317–325; discussion 325-6 (2007).
Dutta, S. et al. Cerebrospinal fluid and plasma procalcitonin for the diagnosis of neonatal bacterial meningitis. J. Paediatr. Child. Health. 58 (8), 1425–1430 (2022).
Zhang, L. et al. Correlation of levels of lactic acid and glucose in cerebrospinal fluid of cerebral hemorrhage patients with the occurrence of postoperative intracranial infection and clinical prognosis. J. Med. Biochem. 43 (1), 36–42 (2024).
van de Beek, D., Drake, J. M. & Tunkel, A. R. Nosocomial bacterial meningitis. N Engl. J. Med. 362 (2), 146–154 (2010).
Kourbeti, I. S. et al. Infections in patients undergoing craniotomy: risk factors associated with post-craniotomy meningitis. J. Neurosurg. 122 (5), 1113–1119 (2015).
Cassir, N. et al. Risk factors for surgical site infections after neurosurgery: A focus on the postoperative period. Am. J. Infect. Control. 43 (12), 1288–1291 (2015).
Korinek, A. M. et al. Risk factors for adult nosocomial meningitis after craniotomy: role of antibiotic prophylaxis. Neurosurgery 62 (Suppl 2), 532–539 (2008).
Nie, J. et al. Development and validation of a predictive model for postoperative intracranial infections in neurosurgery with risk factor analysis. World Neurosurg. 189, e126–e140 (2024).
Funding
This study was financially supported by Collaborative Academic Innovation Project of Shandong Cancer Hospital (TS-010); Taishan Youth Scholar Program of Shandong Province (No. tsqn202312366); Shandong Natural Science Foundation Innovation and Development Joint Fund (ZR2023LZL011) and Shandong Traditional Chinese Medicine Technology Project (M2023-013).
Author information
Authors and Affiliations
Contributions
Methodology, Investigation, Validation: Shanshan Ding and Xiaoyu Ye; External Validation: Xiaohan Dong; Formal analysis and investigation: Shanshan Ding and Dongmei Li; Data curation: Dongmei L and Wenjing Shang; Writing—original draft: Shanshan Ding; Writing—review and editing, Xingguo Song; Supervision: Xingguo Song; Funding acquisition: Xingguo Song. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
This study was approved by the Ethics Committee of Shandong Cancer Hospital Affiliated to Shandong First Medical University and Shandong Academy of Medical Sciences and conducted in accordance with the local legislation and institutional requirements. This is a retrospective study and the requirement for informed consent was waived, which had been approved by Ethics Committee of Shandong Cancer Hospital Affiliated to Shandong First Medical University and Shandong Academy of Medical Sciences. All experimental protocols and methods were carried out in accordance with relevant guidelines and regulations.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ding, S., Dong, X., Ye, X. et al. Diagnostic and prognostic value of combined cerebrospinal fluid parameters for post-neurosurgical intracranial infection in brain tumor patients. Sci Rep 15, 43038 (2025). https://doi.org/10.1038/s41598-025-25682-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-25682-1
