
Abstract
The neutrophil-to-lymphocyte ratio (NLR), a simple marker of systemic inflammation, may assist in differentiating polycythemia vera (PV) from secondary polycythemia (SP), especially when access to JAK2 mutation testing is limited due to cost or delayed turnaround. We retrospectively analyzed 655 patients with erythrocytosis who underwent JAK2 mutation testing between 2007 and 2024 across three South Korean tertiary hospitals. PV and SP were diagnosed per 2016 WHO criteria. NLR was calculated from complete blood counts and compared to serum erythropoietin (EPO) using receiver operating characteristic (ROC) analysis. The mean NLR was significantly higher in PV than SP (6.92 vs. 2.24, p < 0.001). NLR outperformed EPO in distinguishing PV (AUC 0.919 vs. 0.835, p < 0.001), and the combination further improved diagnostic accuracy (AUC 0.955). Notably, 98.8% (159/161) of patients with NLR < 1.5 had SP, suggesting these patients may safely undergo delayed JAK2 testing while secondary causes are prioritized. NLR may serve as a cost-effective triage marker to identify patients at low risk for PV, potentially reducing unnecessary molecular testing and expediting appropriate diagnostic pathways in erythrocytosis.
Similar content being viewed by others
Introduction
The 2016 revision of the WHO diagnostic criteria for polycythemia vera (PV), which lowered the hemoglobin thresholds from > 18.5 to > 16.5 g/dL in men and from > 16.5 to > 16.0 g/dL in women, has broadened the population of patients referred for diagnostic evaluation of erythrocytosis1. In a large population-based cohort (n = 147,167), the incidence of erythrocytosis increased from 0.3 to 3.4% when applying the WHO 2016 diagnostic criteria, compared to the 2008 criteria2.
Secondary erythrocytosis can arise from a variety of causes, including chronic hypoxia (e.g., smoking, chronic obstructive pulmonary disease, or high-altitude residence), renal disease, and exogenous androgens. More recently, drug-associated erythrocytosis has attracted increasing attention, particularly with sodium-glucose cotransporter-2 (SGLT2) inhibitors, whose widespread use in patients with heart failure and chronic kidney disease has coincided with growing reports of elevated hemoglobin3. SGLT2 inhibitors have been associated with erythrocytosis in a number of studies, possibly due to hemoconcentration and erythropoietin stimulation. In some patients, hemoglobin levels may even exceed the WHO diagnostic thresholds for polycythemia, necessitating careful differentiation from PV4. Given the prognostic and therapeutic implications of PV, establishing or excluding this diagnosis remains the central challenge in the evaluation of erythrocytosis.
In the diagnostic workup of erythrocytosis, detection of a JAK2 mutation remains the single most important criterion for diagnosing PV. However, routine testing for JAK2 mutations may be delayed or omitted due to high cost, limited accessibility, or prolonged turnaround times, especially in community-based settings.
There is thus an increasing need for cost-effective triage tools to stratify patients with erythrocytosis prior to molecular testing. The neutrophil-to-lymphocyte ratio (NLR), an inexpensive inflammatory marker derived from routine complete blood counts, has been proposed as a potential surrogate marker in the diagnostic approach to PV5.
In this retrospective multicenter cohort study, we investigated whether a low NLR could serve as a reliable clinical indicator to exclude PV in patients with erythrocytosis. We hypothesized that NLR could aid in prioritizing diagnostic steps and optimizing the use of molecular testing resources.
Materials and methods
Study design and population
We conducted a retrospective cohort study of patients with erythrocytosis who underwent JAK2 mutation testing between June 2007 and October 2024 at three tertiary care centers affiliated with Soonchunhyang University in South Korea (Seoul, Bucheon, and Cheonan). Erythrocytosis was defined as hemoglobin ≥ 16.5 g/dL in men and ≥ 16.0 g/dL in women, consistent with the 2016 WHO diagnostic criteria, which reflects the thresholds commonly used in clinical practice during the study period. Patients were included if they had undergone testing for the JAK2 V617F and/or exon 12 mutation, which were typically performed concurrently. Patients were excluded if serum erythropoietin (EPO) levels were unavailable or if a bone marrow biopsy was required but not performed. Conversely, patients were classified as PV—regardless of biopsy—if they had hemoglobin > 18.5 g/dL (men) or > 16.5 g/dL (women), JAK2 mutation, and subnormal EPO, in accordance with the exception clause of the 2016 WHO criteria. The study was approved by the Institutional Review Board of Soonchunhyang University Hospital (IRB no. 2025-05-009) and conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study.
Variables and definitions
Blood samples were collected under fasting conditions using EDTA-2K, heparin sodium, and siliconized tubes. Complete blood counts (CBC) with six-part white blood cell differentials were analyzed using the Alinity HQ Analyzer® (Abbott, USA). The NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count. Serum EPO levels were interpreted categorically based on institutional reference ranges (4.3–29.0 mIU/mL); values below this range were considered subnormal. This approach reflects real-world clinical decision-making and aligns with the WHO diagnostic criteria for PV. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Obesity was defined as BMI ≥ 25 kg/m2, consistent with WHO guidelines for Asian populations. Smoking status was classified as current if the patient smoked at least one cigarette per day at the time of health screening.
Statistical analysis
Categorical variables were summarized as counts and percentages and compared using the Chi-square test or Fisher’s exact test, as appropriate. Normality of continuous variables was assessed using the Shapiro–Wilk test. Variables with a normal distribution were expressed as mean ± standard deviation and compared using independent t-tests, whereas non-normally distributed variables were presented as medians with interquartile ranges and analyzed using the Mann–Whitney U test. Diagnostic accuracy of the NLR and serum EPO levels for identifying PV was evaluated using receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC) values were compared using the DeLong test. To explore the clinical utility of NLR as a triage tool, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated across a range of NLR thresholds. All statistical analyses were performed using R version 3.6.1 and Rex version 3.0.3 (RexSoft Inc., Seoul, Korea). A p value < 0.05 was considered statistically significant.
Results
Study population
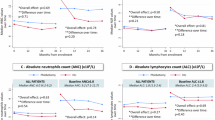
From January 2007 to October 2024, 2114 patients underwent JAK2 mutation testing at Soonchunhyang University Hospitals. Of these, 1349 patients tested for other indications (e.g., thrombocytosis, myelofibrosis) were excluded. The remaining 765 patients were evaluated for erythrocytosis. After excluding 110 patients with insufficient diagnostic data, a total of 655 patients were included in the final analysis: 168 diagnosed with PV and 487 with SP (Fig. S1). Among the 168 patients diagnosed with PV, 166 were positive for the JAK2 V617F mutation and 2 were positive for JAK2 exon 12 mutation. Following the 2016 WHO revision that lowered the diagnostic hemoglobin threshold for PV, the volume of JAK2 testing increased markedly. However, the number of confirmed PV cases remained stable over time, while diagnoses of SP increased substantially (Fig. S2). This trend highlights the growing diagnostic burden and potential overuse of JAK2 testing.Baseline characteristics are summarized in Table 1. Patients with PV were older (mean age 65.5 ± 11.7 vs. 51.0 ± 14.9 years, p < 0.001), and SP was more common in males, smokers, and individuals with higher BMI. As expected, patients with PV showed significantly higher levels of white blood cell and platelet counts. C-reactive protein (CRP) levels did not differ significantly between the groups.
Diagnostic performance of NLR
The median NLR was significantly higher in the PV group than in the SP group (6.92 ± 5.57 vs. 2.24 ± 2.45, p < 0.001). In ROC analysis, NLR showed superior diagnostic performance to serum EPO (AUC, 0.919 95% confidence interval [95% CI] 0.894–0.940 vs. AUC, 0.835; 95% CI 0.803–0.866; p < 0.001), and the combination of both parameters yielded a significantly improved diagnostic value (AUC, 0.955; 95% CI 0.932–0.974) compared to NLR alone (p < 0.001) (Fig. 1).

Diagnostic performance of NLR and EPO in distinguishing PV from SP. Receiver operating characteristic (ROC) curves show that the neutrophil-to-lymphocyte ratio (NLR) had superior diagnostic accuracy compared to serum erythropoietin (EPO) levels (AUC 0.919 vs. 0.835, p < 0.001). The combination of NLR and EPO further improved the area under the curve (AUC 0.955).
The optimal NLR cutoff maximizing the AUC was identified as 2.97. Given that dichotomous variables are more practical for clinical application, we evaluated the diagnostic performance at key NLR thresholds:
-
At NLR < 1.5, sensitivity and NPV were both 98.8%, outperforming subnormal EPO.
-
At NLR > 4.5, specificity reached 96.3% and PPV 83.9%, again exceeding the performance of EPO alone.
Table 2 summarizes sensitivity, specificity, PPV, and NPV across various NLR cutoffs. When patients were ranked by increasing NLR, 98.8% (159 of 161) of those with NLR < 1.5 were diagnosed with SP. Likewise, 97.2% (275 of 283) of patients with NLR < 2.0 had SP (Fig. S3). These findings suggest that a low NLR is strongly associated with SP and may be clinically useful to rule out PV, especially in resource-limited settings or when JAK2 mutation testing is delayed.
Discussion
This study demonstrated that the NLR was significantly higher in patients with PV compared to those with SP (6.92 ± 5.57 vs. 2.24 ± 2.45, p < 0.001). In ROC analysis, NLR showed superior diagnostic performance over serum EPO levels (AUC: 0.919 vs. 0.835, p < 0.001), and combining both markers further enhanced diagnostic accuracy (AUC: 0.955). Notably, low NLR values were strongly associated with SP, as 98.8% of patients with NLR < 1.5 and 97.2% of those with NLR < 2.0 were ultimately diagnosed with SP. Although our study was conducted based on the 2016 WHO criteria, the 2022 WHO classification retained the same hemoglobin cutoffs for PV diagnosis. Therefore, the diagnostic relevance of our findings remains applicable under the latest framework.
NLR, calculated by dividing the absolute neutrophil count by the lymphocyte count, is a widely used inflammatory marker across clinical settings6. In PV, a myeloproliferative neoplasm with an established inflammatory profile, elevated NLR likely reflects both the systemic inflammatory milieu and characteristic hematologic findings, such as neutrophilia and relative lymphopenia resulting from panmyelosis7. This hematologic pattern directly contributes to elevated NLR levels and aligns with PV pathobiology.
In our previous study, we evaluated the diagnostic utility of NLR while excluding patients with CRP ≥ 1 mg/dL to mitigate confounding from unrelated inflammatory conditions5. However, as NLR is a nonspecific inflammatory marker, elevated levels can also be observed in infections, autoimmune diseases, and malignancies8. Thus, a high NLR must be interpreted cautiously in conjunction with the clinical context and other laboratory findings.
Despite this limitation, the strength of low NLR as a negative predictor remains robust. In this study, NLR < 1.5 was associated with a negative predictive value of 98.8%, suggesting that patients with low NLR are highly unlikely to have PV. This is consistent with the hematologic inverse of panmyelosis; whereas PV typically presents with neutrophilia and lymphopenia, a low NLR may instead reflect the lack of panmyelosis, which characteristically distinguishes SP from PV. This approach is conceptually similar to the use of D-dimer in venous thromboembolism (VTE) diagnosis, where a low value helps exclude disease and avoid unnecessary imaging procedures9,10. Similarly a low NLR may guide clinicians toward evaluating for secondary causes before proceeding with molecular testing, potentially streamlining diagnostic efforts.
Additional support for the utility of NLR comes from a subgroup within our cohort: 66 patients with erythrocytosis who were JAK2-negative and had subnormal EPO levels—a group typically requiring bone marrow biopsy to evaluate for panmyelosis and confirm or exclude PV. Among the 27 who underwent biopsy, only 3 were ultimately diagnosed with JAK2-negative PV, whereas 24 had SP. The NLR values in these three PV cases were 1.70, 1.75, and 2.66, while 7 of the 24 SP patients had NLR < 1.5. These data suggest that in selected patients, particularly those with very low NLR, the need for invasive procedures such as bone marrow biopsy may be reduced. This finding further supports the role of NLR as a practical adjunct in the diagnostic workup of erythrocytosis, especially when conventional diagnostic tools yield inconclusive results.
Given its accessibility and performance characteristics, NLR may serve as a practical triage tool, particularly in settings where molecular testing is unavailable, delayed, or resource-constrained. While JAK2 mutation testing remains the cornerstone of PV diagnosis and is indispensable for confirmation, NLR may complement existing tools by reducing unnecessary bone marrow biopsies in equivocal cases. Importantly, molecular testing should never be omitted in suspected cases of masked PV11. For instance, in patients with erythrocytosis and low NLR (e.g., < 1.5), clinicians may consider delaying JAK2 testing to first assess for secondary causes such as hypoxia, smoking, or medication use. If no reversible cause is identified and erythrocytosis persists, molecular and bone marrow evaluation can be pursued subsequently. Conversely, patients with elevated NLR may warrant expedited testing. This tiered strategy may improve diagnostic efficiency and avoid unnecessary testing in patients with low pretest probability of PV.
This study has several limitations. Its retrospective design and single-country dataset may limit generalizability, particularly across diverse ethnic or practice settings. Additionally, Prospective studies across broader populations are warranted to validate NLR thresholds and confirm their role in clinical algorithms.
In conclusion, NLR is a readily available marker that reflects the pathophysiology of PV and offers high diagnostic utility. While elevated values should be interpreted within clinical context, low NLR—especially values < 1.5—showed high negative predictive value and may effectively guide clinicians toward secondary causes of erythrocytosis before molecular testing. Incorporating NLR into the diagnostic algorithm may enhance efficiency, reduce cost, and improve patient stratification in the evaluation of erythrocytosis.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author (jhwon@schmc.ac.kr) on reasonable request.
References
Barbui, T. et al. The 2016 WHO classification and diagnostic criteria for myeloproliferative neoplasms: Document summary and in-depth discussion. Blood Cancer J. 8(2), 15 (2018).
Wouters, H. et al. Erythrocytosis in the general population: Clinical characteristics and association with clonal hematopoiesis. Blood Adv. 4(24), 6353–6363 (2020).
Hussain, A. et al. Utilization rates of SGLT2 inhibitors among patients with type 2 diabetes, heart failure, and atherosclerotic cardiovascular disease: Insights from the department of veterans affairs. JACC Heart Fail. 11(8 Pt 1), 933–942 (2023).
Gangat, N. et al. JAK2 wild-type erythrocytosis associated with sodium-glucose cotransporter 2 inhibitor therapy. Blood 138(26), 2886–2889 (2021).
Kim, M. J. et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as new possible minor criteria for diagnosis of polycythemia vera. Int. J. Lab. Hematol. 45(6), 853–859 (2023).
Guthrie, G. J. et al. The systemic inflammation-based neutrophil–lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 88(1), 218–230 (2013).
Hasselbalch, H. C. Chronic inflammation as a promotor of mutagenesis in essential thrombocythemia, polycythemia vera and myelofibrosis. A human inflammation model for cancer development?. Leuk. Res. 37(2), 214–220 (2013).
Kourilovitch, M. & Galarza-Maldonado, C. Could a simple biomarker as neutrophil-to-lymphocyte ratio reflect complex processes orchestrated by neutrophils?. J. Transl. Autoimmun.. 6, 100159 (2023).
Pulivarthi, S. & Gurram, M. K. Effectiveness of d-dimer as a screening test for venous thromboembolism: An update. N. Am. J. Med. Sci. 6(10), 491–499 (2014).
Righini, M., Perrier, A., De Moerloose, P. & Bounameaux, H. D-Dimer for venous thromboembolism diagnosis: 20 years later. J. Thromb. Haemost. 6(7), 1059–1071 (2008).
Moliterno, A. R., Kaizer, H. & Reeves, B. N. JAK2V617F allele burden in polycythemia vera: Burden of proof. Blood 141(16), 1934–1942 (2023).
Acknowledgements
This study was supported by the Soonchunhyang University Research Fund.
Author information
Authors and Affiliations
Contributions
Seug Yun Yoon, Seong Soon Kwon wrote the paper; Seug Yun Yoon, Sun Young Jeong, Min-Young Lee, Kyoung Ha Kim, Se Hyung Kim and Sang Byung Bae designed research; Seug Yun Yoon, Namsu Lee, Sung Kyu Park and Jong-Ho Won performed research; Seug Yun Yoon, Seong Soon Kwon and Jong-Ho Won analyzed data: and all authors critically revised the paper and approved the final version. The authors take responsibility for all aspects of the reliability and freedom from bias of the presented data and their discussed interpretation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yoon, S.Y., Kwon, S.S., Jeong, S.Y. et al. Low neutrophil-to-lymphocyte ratio identifies secondary polycythemia in patients with erythrocytosis. Sci Rep 15, 42043 (2025). https://doi.org/10.1038/s41598-025-26200-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-26200-z
