
Abstract
The Stroke Life Support Central Health Alliance, Registry & Technology Enabled caRe (SLS CHARTER) Programme addresses stroke patients’ rehabilitation needs through timely evaluation and intervention, but it has not been evaluated. This study evaluated the programme’s outcomes over 6 months. The primary outcome was Post Stroke Checklist (PSC) usage per SLS participant. For the final analysis, 206 SLS and 55 control participants from a public healthcare institution in Singapore were included. Secondary economic outcomes included healthcare utilisation and return to work (RTW). Multivariate analyses, adjusted for demographics and clinical factors, used gamma-log link and Poisson regression for healthcare utilisation, and logistic and Cox regression for RTW outcomes, to evaluate associations with intervention status. PSC usage increased from 50.5% 1-month post stroke to 86.9% 6-month post stroke; mean utilisation rose from 1.76 to 4.25. SLS participants reported longer lengths of stay (LOS) in certain rehabilitation institution and less day care visits. Additionally, there was varying RTW for different patient subgroups. Our findings suggest the SLS CHARTER Programme increases PSC usage, which is useful to guide future care coordination programmes. Identification of patients at risk of poorer RTW, for proactive occupational rehabilitation, may help to reduce the economic burden of stroke.
Similar content being viewed by others

Introduction
Stroke is the second-leading cause of death and third-leading cause of disability-adjusted life-years lost (DALYs) globally, with stroke incidence rising by 70% from 1990 to 20191. There is an alarming trend of increasing ischemic stroke incidence in the 35–39 age group, who form part of the working age population2, rising from 22.1 per 100,000 in 1990 to 22.7 per 100,000 in 20193. Upward trends in ischemic stroke incidence were observed particularly in the lower-middle and high sociodemographic index (SDI) groups3. Coinciding with the rise in global incidence, the rising number of stroke cases in Singapore has also increased from 6,143 episodes in 2011 to 9,680 episodes in 20214 due to the ageing population and a growing prevalence of chronic diseases. If current trends were to continue, the economic cost of stroke could surpass US$1 trillion by 20305.
Part of this economic cost is attributed to the range of long-term physical, cognitive, emotional, and psychological complications stroke patients face during recovery6. Cognition impairment in domains like memory, executive function, and attention occurs in up to 60% of survivors one year after stroke7 and post stroke depression prevalence ranged from 31% to 45%8. These unmet post-stroke needs hinder the ability of individuals to return to work (RTW)9, further contributing to rising healthcare costs and productivity loss. Findings from systematic reviews among stroke patients revealed reasons for unmet post-stroke care needs amongst stroke survivors, including the inability of patients to accurately identify and articulate needs to health care professionals10, and insufficient information on post-discharge healthcare services and scheduling appointments11. Additionally, despite international guidelines recommending follow-up reviews with stroke survivors post-discharge, this is still not routinely practiced12. Therefore, early identification of post stroke complications paired with timely follow-up interventions is critical.
Exacerbating the unmet needs of stroke survivors is the large number of different healthcare providers involved in the patient’s recovery journey, with multiple handoffs along the way, potentially complicating or lengthening the process for both patients and providers. Improving the efficiency of stroke care and management of patients through better care coordination has hence become increasingly imperative.
In Singapore, the Stroke Life Support Central Health Alliance, Registry and Technology Enabled Care (SLS CHARTER) Programme was conceived in 2022 to address the evolving rehabilitation needs of stroke survivors residing in central Singapore through a structured screening process and the appropriate right-siting for further intervention aimed at improving their standard of care and quality of life. This programme was anchored in a restructured hospital, Tan Tock Seng Hospital (TTSH), which is where many stroke patients seek care due to the hospital’s multidisciplinary approach, specialised acute care, and comprehensive rehabilitation expertise13. The programme aims to empower patients and caregivers on the usage of the post-stroke checklist (PSC)14, and improve care coordination of care by Central Health Alliance in Stroke Enablement (CHASE) coordinators within the CHASE network of stroke care providers. Although there are existing studies on transitional care interventions15 and studies on PSC usage16,17, these have been presented separately. The SLS CHARTER Programme combined both aspects to allow for better care coordination using the long-term problems identified using the PSC, which is understood by all relevant stakeholders involved in the patient recovery journey. There is limited evidence on the effectiveness of such models in the context of stroke care, which is crucial in providing insights to refine the patient recovery journey. Hence, the primary aim study was to examine the PSC usage and the secondary aim was to compare (1) healthcare utilisation and (2) RTW 6 months post-stroke between SLS and control participants. Subgroup analysis was also conducted to examine healthcare utilisation at specific rehabilitation institution settings. Additional analyses were conducted to examine the association between socioeconomic variables and RTW.
Methods
Study design and population
Eligible patients with a first incidence of stroke and admitted to TTSH were recruited to this prospective cohort study from November 2022 to July 2023. In a staggered recruitment approach, patients were recruited to the control group between November 2022 to January 2023, until the target number of 65 was reached. Thereafter, patient recruitment in the SLS group began in January 2023, till July 2023, until a target number of 250 was reached. The sample sizes were predetermined based on availability of the clinical team within the project period, especially considering the significant logistics requirements to follow up patients with only 2 CHASE coordinators. As the primary aim of the study was to examine the usage of PSC, based on the predetermined numbers, is sufficient to detect a 30% increase in PSC usage with 80% power. Patients who passed away, went to a nursing home, were uncontactable, and withdrew from the study were excluded from the final analysis.
This study adhered to the Declaration of Helsinki and was approved by National Healthcare Group (NHG) Domain Specific Review Board (DSRB) (Reference Number: (2021/01059)). Written informed consent was obtained from all individual participants after they were being informed about the study objectives and the safeguards put in place so that confidentiality of the collected data is maintained.
Study intervention
A comparison of the SLS CHARTER Programme model and the traditional model is shown in Figure S1 (Additional File 1). As part of the SLS CHARTER pilot programme, an alliance named CHASE was formed to foster closer collaboration and coordination in managing care for stroke survivors in the Central Singapore community. The CHASE network is made up of various stroke care providers from tertiary healthcare institutions down to community-level services.
Two care coordinators (CHASE coordinators) that were recruited for this study helped to engage stroke patients within the acute stroke unit early in their journey. They educated the SLS participants and their families on how to self-administer the PSC. The PSC is an 11-item checklist that was identified by the Global Stroke Community Advisory Panel as a tool to identify long-term post stroke problems and facilitate appropriate referrals for treatment14. The CHASE coordinators played a central role in coordinating referrals and appropriately right-siting care within the CHASE network. They served as the point of contact for participants, caregivers and different healthcare providers, facilitating the transition of care to the optimal levels of support and treatment across the CHASE network.
Outcome measures
The primary objective was to measure the number of participants who had used the PSC and the number of PSC used per patient, at 1-month, 3-month, and 6-month intervals. Participants were asked to self-report the number of PSC used at 1-month, 3-month, 6-month, from day 1 to the end of each month.
The secondary objective was to measure economic outcomes, namely healthcare utilisation and RTW outcomes 6 months post-stroke. Post-stroke recovery processes are time-dependent, with most of the significant improvements usually reaching a plateau after 3 months and spontaneous recovery is often at its limit after 6 months post-stroke18.
For healthcare utilisation, the length of stay (LOS) (acute stroke unit, rehabilitation institutions (Table S1, Additional File 1), and whole stroke episode), stroke-related emergency department (ED) visits and readmissions at TTSH, outpatient visits at TTSH Specialist Outpatient Centres (SOCs) (Table S2, Additional File 1) and community-based visits at selected day centres (Table S3, Additional File 1) within the 6 months post-enrolment, were evaluated. Whole stroke episode encompasses the entire continuum of stroke care, including both the acute stroke unit and rehabilitation institutions, which together help ensure comprehensive stroke management and recovery.
RTW outcomes, were self-reported, with participants indicating whether they had returned to work and the corresponding RTW date, if applicable. The proportion of participants who returned to work and the time taken from initial admission to return to work were measured at the 6-month mark, for participants who were employed at the baseline.
Baseline characteristics
Socio-demographic information that were collected included age, gender, ethnicity (Chinese, Malay, Indian, others, missing), living arrangement (alone, spouse, spouse and/or children, other family members, unrelated caregiver, others, missing), marital status (single, married, divorced, widowed, missing), occupation class (legislators, senior officials, managers; professionals; associate professionals, technicians; clerical support workers; service & sales workers; agricultural & fishery workers; craftsmen & related trades workers; plant & machine operators, & assemblers; cleaners, labourers & related workers), employment status (unemployed, employed full-time, employed part-time, self-employed, including own account worker, contributing family member, and employer, retired, not applicable (NA)), (NA, monthly income level (<$2000, $2000 - $3999, $4000 - $5999, $6000 - $9999, $10000 - $14999, >$15000, NA, missing), and highest educational level (no formal education, primary, secondary, pre-university, tertiary, postgraduate, missing), and premorbid caregiver status (independent, family (informal) caregiver, formal caregiver).
Clinical information collected included type of stroke (ischemic or hemorrhagic), any hyperacute stroke intervention, any surgical treatment for acute stroke, initial stroke severity indicated by the National Institutes of Health Stroke Scale (NIHSS) (mild (0–4), moderate (5–15), severe (16–42))19, predefined risk factors for stroke (diabetes mellitus, hypertension, dyslipidemia, ischemic heart disease, atrial fibrillation, and smoker), predefined medical complications (pulmonary embolism (PE), deep vein thrombosis (DVT), pneumonia, urinary tract infection (UTI)), hyperacute intervention (no hyperacute intervention, recombinant tissue plasminogen activator (rTPA), endovascular treatments (EVT), rTPA and EVT) and the functional status measured using Premorbid Modified Ranking Score (MRS) (no symptoms (0), no significant disability (1), slight disability (2), moderate disability (3), moderate to severe disability (4), and severe disability (5))20, and Modified Barthel Index (MBI) (severe (0–20), moderate (21–60), mild (61–100))21.
Statistical analysis
Continuous outcomes (age, NIHSS score, MBI score) were described using unadjusted means and standard deviations, while categorical outcomes (gender, ethnicity, living arrangement, marital status, occupation, employment status, monthly income level, highest educational level, premorbid caregiver status, predefined risk factors for stroke, and predefined medical complications) were described as percentages. T-tests for continuous outcomes and chi-squared tests for categorical variables, were conducted to assess between-group differences at baseline.
Poisson models were used to examine the association between intervention status and healthcare utilisation. Logistic and cox regressions were employed for examining the association between intervention status and RTW status and days to RTW, respectively. These regression analyses were adjusted for age, gender, race, stroke type and baseline MBI severity category.
As exploratory analyses, to investigate different health utilisation pathways of stroke care, subgroup analysis stratified by rehabilitation institution (rehabilitation institution A, rehabilitation institution B, rehabilitation institution C, and rehabilitation institution D) was performed to examine healthcare utilisation across each rehabilitation institution. Additional exploratory analyses by occupation type (white-collar, blue-collar), and income level (low (≤ $3,999), high (≥ $4,000)) were also performed to examine the association between socioeconomic status and RTW outcomes. These additional analyses were conducted to examine the association between socioeconomic status and RTW, because no significant associations were observed between intervention status and RTW.
All the analyses were conducted using Stata (v15 and v18) (StataCorp, College Station, Tx) and a p value of 0.05 was set as the level of significance for all tests.
Results
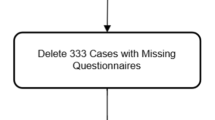
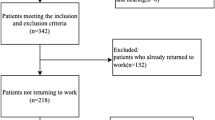
315 patients were recruited at baseline. After excluding participants who passed away, went to a nursing home, were uncontactable, and withdrew from the study (SLS n = 44; Control n = 10), 206 SLS participants and 55 control participants were included in the final analysis (Fig. 1).

Number of participants included in the final analysis.
Characteristics of the participants
The baseline characteristics of the participants included in the final analysis are described in Table 1. There were no significant differences in socio-demographic or clinical factors between groups.
Usage of PSC
Among the intervention group, despite reminders, 13 (0.49%) participants in the intervention group did not use PSC during the study period. Participants who used PSC were more likely to be younger, single or married, and less likely to be widowed than those who did not. There were no differences in gender, highest education status SLS participants who used PSC and those who did not (Table S4, Additional File 1).
Table 2 shows the usage of PSC over 6 months. The percentage of SLS participants using PSC increased from 50.5% (n = 104) 1-month post stroke to 86.9% (n = 179) 6-month post stroke. The number of PSC used per patient also increased across the 6-month period (mean ± SD: 1.76 ± 1.09 to 4.25 ± 1.09).
Figure 2 shows the issues raised and received by CHASE coordinators according to the PSC items. 30% of the issues could not be categorised into PSC items and were hence placed under ‘Other challenges’. The next three most common long-term post stroke issues were related to secondary stroke prevention (12.1%), returning to work (11.3%), and mobility (7.8%). The ‘Other challenges’ faced was further broken down (Fig. 2). The most common issues were related to community care plan (20%) and SOC appointments (20%), followed by finance (12%), insurance (12%), and medical (12%), then hospital leave (10%).

Issues raised and received by CHASE coordinators by PSC items. PSC: Post-stroke checklist; ADL: Activities of daily living; NOK: Next of kin; DRC: Day rehabilitation centre; SOC: Specialist outpatient clinic.
Healthcare utilisation
There were no differences in LOS between the SLS participants and control participants for their whole stroke episode and across all rehabilitation institution settings (Table S5, Additional File 1). Additionally, in the exploratory subgroup analysis by rehabilitation institution setting (Table S5, Additional File 1), it was observed that SLS participants had a significantly longer LOS than control participants at rehabilitation institution B and D, after adjusting for age, gender, ethnicity, stroke type, and baseline MBI severity category (Rehabilitation institution B Incidence Risk Ratio (IRR) = 2.1, 95% Confidence Interval (CI) = 1.6–2.8; Rehabilitation institution D IRR = 1.7, 95% CI = 1.4–2.2), or baseline NIHSS severity category (Rehabilitation institution B IRR = 3.1, 95% CI = 2.4–4.2, p-value < 0.001; Rehabilitation institution D IRR = 1.4, 95% CI = 1.2–1.9, p-value = 0.001). On the other hand, SLS participants had shorter LOS compared to control participants at rehabilitation institution C after adjustments for age, gender, ethnicity, stroke type, and baseline MBI severity category (IRR = 0.4, 95% CI = 0.2–0.7).
Outpatient visits
Among SLS participants, 35.9% visited Neurology (NL) and 32.0% visited Rehabilitation department, while 36.4% of control participants visited Neurology and Rehabilitation department (Fig. 3). More SLS participants (28.2%) attended Neurosurgery (NS) compared to control participants (16.4%) and less SLS participants (10.7%) attended Speech Therapy (ST) compared to control participants (20.0%).

Number of SLS and control participants that visited (a) various TTSH Specialist Outpatient Clinics, and (b) various Day Care service providers. *≥10% of patients. Following clinics not reflected due to small numbers (< 10%): Consultation-Liaison Interventions for the Mind and Brain (CLIMB), Home-based Case Management, Home-based Medical Social Worker, Home-based Nursing, Home-based Occupational Therapy, Home-based Psychology, Home-based Physiotherapy, Home-based Speech Therapy, Psychiatry, Psychology, Medical Social Worker, Neurology Radiology, Sex Clinic. PT: Physiotherapy; OT: Occupational Therapy; ST: Speech Therapy; NL: Neurology; NS: Neurosurgery.
Day care visits
The percentage of participants who visited day care were similar in both groups [SLS: 9.7% (n = 20) and Controls: 10.9% (n = 6)]. The mean number of day care visits is lower for SLS than controls (Table 3).
Post-stroke acute healthcare utilisation
The percentage of participants who visited ED within 6 months of the index stroke visit were similar in both groups [SLS: 13 (6.3%) and controls: 3 (5.5%)] (Table 4). There was no difference observed in the number of SLS participants who had ED visitss compared to control participants, after adjusting for age, gender, ethnicity, stroke type, and baseline MBI severity category (OR = 1.2; 95%CI = 0.3–4.3; p = 0.817) For SLS participants, 68.8% and 31.3% of the reasons for ED visits were due to new stroke and stroke-related falls, respectively (Fig. 4). For control participants, 75% and 25% of the reasons for ED visits were due to a UTI and stroke-related falls, respectively.
Among the SLS participants, 16 (7.8%) had readmissions while 3 (5.5%) control participants had readmissions within 6 months of the index stroke visit (Table 4). There was no difference observed in the number of SLS participants who had readmissions compared to control participants, after adjusting for age, gender, ethnicity, stroke type, and baseline MBI severity category (OR = 1.3 (95%CI = 0.4–4.9); p = 0.659). For SLS participants, 55.6% and 22.2% of the reasons for readmissions were due to new stroke and stroke-related falls, respectively (Fig. 4). For control participants, 40% of the reasons for readmissions were due to a UTI and a cardiovascular condition.

Number of patients with specified reasons for (a) ED visits and (b) readmissions, by SLS and control groups. *Not shown due to no counts: SLS: pain, pneumonia, mood, cardiovascular condition. Control: pain, pneumonia. ED: Emergency department.
Return to work
The percentage of participants employed at baseline who returned to work were similar in both groups [SLS RTW: 58.3% (n = 67) and controls: 54.3% (n = 19)]. There were no differences in RTW status (OR = 1.2, 95% CI = 0.5–2.9) and RTW time (HR = 0.8, 95% CI = 0.4–1.5, p = 0.478) between SLS and control participants after adjusting for age, gender, ethnicity, stroke type, baseline MBI severity category.
Additional analysis for RTW outcomes – occupation and income level
An additional analysis was conducted to identify potential demographic factors that is associated with RTW, to better support RTW in these groups of patients. Figure 5 shows the stratification done on RTW outcomes by occupation type and income level. White collar workers were four times more likely to RTW compared to blue collar workers (95% CI: 1.6–10.1) and workers with income of more than or equal to $4000 were 6.5 times more likely to RTW than workers with income of less than $4000 (95% CI: 1.9–22.6) when adjusted for age, gender, ethnicity, stroke type, and baseline MBI severity category.

Additional group baseline employment, RTW outcomes, and the relationship between socioeconomic variables and RTW outcomes. RTW: Return to work.
Discussion
In this prospective case-control study, we evaluated the implementation of the Stroke Life Support Central Health Alliance, Registry & Technology Enabled Care (SLS CHARTER) program over a six-month period. We found that stroke survivors were willing and able to use the Post Stroke Checklist (PSC) to self-monitor symptoms at home, with increased uptake over time. Contrary to expectations, SLS participants had less day care visits compared to control participants. Clinical outcomes such as hospital length of stay (LOS) also varied across rehabilitation institutions, possibly due to differing care protocols. While intervention status did not influence whether patients RTW, socioeconomic factors were associated with the ability to RTW.
The study demonstrated that stroke survivors found the PSC feasible and easy to use, with self-reported usage increasing from 50.5% at one month to 86.9% at six months. This rising trend was accompanied by a higher number of PSCs completed per patient over time, indicating sustained engagement. Lower usage in the first month was likely attributable to participants still in inpatient or rehabilitation. Importantly, approximately 30% of issues raised by participants fell outside the PSC’s predefined items, including administrative queries, insurance concerns, and care planning. This mirrors findings from a UK pilot study, where patients similarly reported needs beyond the scope of the PSC16. A global comparative study involving seven countries also found significant variability in PSC item reporting across populations12, further underscoring the need to tailor the checklist to local contexts.
Although the PSC has shown utility in identifying post-stroke problems, its use alone may be insufficient to drive long-term outcomes. A Swedish study reported that while the PSC was feasible for problem identification, it did not on its own lead to achievement of treatment goals17. Similarly, pilot studies in Singapore and the UK highlighted that the PSC primarily functions as a referral tool and lacks the mechanisms to enforce follow-up care16. The SLS CHARTER Programme was designed to address this limitation by embedding the PSC within a coordinated care model that supports completion of the checklist and facilitates timely referrals to a multidisciplinary network of stroke care providers. While we observed that SLS participants were willing to use PSC to self-monitor post-stroke symptoms, further studies with longer follow-up will be required to observe if tangible follow-up actions or care adjustments were implemented and sustained.
To the best of our knowledge, there are no studies examining the effect of post stroke care coordination on day care utilisation. The fewer day care visits amongst SLS participants, however, may reflect a variety of situations, such as better self-management, access issues, or service mismatch. To further investigate this, we could explore following-up with the patients for a longer period to track their journey across various healthcare providers, along with qualitative explorations.
The mean LOS varied at different rehabilitations for the SLS and control groups. While previous studies have identified predictors of LOS in rehabilitation institutions in general22,23, there is a paucity of research examining factors contributing to differences in LOS across different rehabilitation institution settings. Echoing a prior Singapore study that reported ward class and pre-stroke living arrangements as significant predictors of rehabilitation LOS24, it is plausible that differences in patients’ socioeconomic backgrounds and family support structures may have contributed to the observed variation. Additionally, variations in institutional care protocols, such as discharge planning processes and resource availability, could potentially influence LOS25. Individual rehabilitation settings may also prioritise different aspects of care, such as high-quality care or cost-efficient care. These factors were not captured in our dataset. As this was a preliminary study with a relatively small sample size and limited covariate data, future research should explore these contextual and institutional variables more comprehensively to better understand LOS differences between intervention and control groups across different rehabilitation settings, and to further validate these exploratory findings.
Previous studies from Western populations have consistently shown that white-collar workers and individuals with higher income are more likely to return to work after stroke26,27. This trend is often attributed to less physically demanding job roles, greater workplace flexibility, and better access to resources compared to blue-collar workers and individuals with lower income27. A systematic review of 16 studies reported that white-collar workers had significantly higher odds of returning to work (OR: 1.84)28. Patients with lower income (69.9%) were also less likely to RTW compared to those with higher income (79.9%), as a 2016 Swedish study had found26. However, few previous studies have examined social demographics status with RTW status in an Asian population. Our exploratory findings potentially add on to this narrative from an Asian context and supports the need for interventions globally to target blue collar workers with lower educational levels and incomes to facilitate the process of returning to work after stroke. Such interventions can entail workplace modifications, support from employers, and vocational rehabilitation29. We acknowledge that the RTW exploratory analysis is limited by the study’s sample size, and further exploration needs to be done to further validate the associations between RTW and the various subgroups.
One of the key strengths of this study is its prospective design, which allowed us to follow up with the stroke survivors over time. We were able to compare baseline and post-intervention outcomes to evaluate the impact of the SLS CHARTER Programme, as well as enhance our understanding of temporal changes at different time points across a 6-month period. Another strength is the low attrition rate, 17.1%, of the study. This reduced the risk of selection bias and increased the reliability of our study. Moreover, we conducted a comprehensive assessment of economic outcomes of this novel care model that included both PSC usage and follow-up care coordination, examining both healthcare utilisation in visits and LOS, and RTW outcomes. However, our study has some limitations. Firstly, only ischemic and haemorrhagic stroke patients were included, hence limiting the generalisability of our findings to patients with other less common stroke types. However, ischemic and haemorrhagic stroke patients constitute a majority of Singapore’s stroke patient30. Secondly, our study was conducted in Singapore, an Asian country, which limits the transferability of the results to countries with vastly different healthcare systems. Future study designs should account for localised contexts for post-stroke needs, to develop tailored patient care coordination. Additionally, participants were only recruited from TTSH, and hence findings cannot be generalised to the entire stroke survivor population in Singapore. However, to our knowledge, this is the first study which explored care coordination, PSC and economic outcomes in Singapore. Thirdly, while our study demonstrated the potential that stroke patients are willing to self-monitor using the PSC, we did not measure the adherence to medical appointments or referred services. This is critical as it helps them address their post-stroke needs, hence future evaluation will need to consider collecting adherence outcomes. Fourth, participants self-reported the number of PSC completed, which may result in recall bias where participants might under or over-report. Fifth, the sample sizes were predetermined based on availability of the clinical team within the project period, especially considering the manpower constraints of only 2 CHASE coordinators over a 6-month period. As such, this resulted in a substantial difference in sample size between the intervention (n = 206) and control (n = 55) groups, and a relatively modest follow-up period. Future studies with equal sample sizes in intervention and control group and a longer follow-up period should be conducted to confirm the findings in our study. Lastly, the non-contemporaneous recruitment approach, where the control group (November 2022 to January 2023) was recruited prior to the intervention group (January 2023 to July 2023), could potentially introduce temporal bias. However, there were no changes to the care model during this period and the relatively short overall recruitment period likely minimised the time-based confounding effects.
Conclusion
The study measured PSC usage and the economic outcomes of the SLS CHARTER Programme. Our findings suggest that the SLS CHARTER Programme can help increase PSC usage among stroke survivors and can be useful to guide future care coordination programmes that uses PSC, to support stroke survivors in accessing the appropriate care services for their post-stroke needs. Patients with lower socioeconomic status might also require more pro-active interventions to support their RTW. For future studies, it might be beneficial to follow the patients through a longer timeline, especially for RTW outcomes, which might take longer to actualise. We should also explore ways to increase SLS adoption across the CHASE network and healthcare professionals, so that more referrals are being made to the right care providers.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and its Supplementary material. Raw data that supports the findings in this study are available from the corresponding author, upon reasonable request.
References
Feigin, V. L. et al. World stroke organization (WSO): global stroke fact sheet 2022. Int. J. Stroke. 17(1), 18–29 (2022).
Organization for Economic Co-operation and Development (OECD). Employment rate by age group. [Online] (2022). https://www.oecd.org/en/data/indicators/employment-rate-by-age-group.html
Ma Z, et al. Global burden of stroke in adolescents and young adults (aged 15-39 years) from 1990 to 2019: a comprehensive trend analysis based on the global burden of disease study 2019. BMC Public Health. 24(1), 1–15 (2024).
National Registry of Diseases Office. Singapore Stroke Registry. Singapore : s.n., (2020).
World Stroke Organization. Impact of Stroke. [Online] (2024). https://www.world-stroke.org/world-stroke-day-campaign/about-stroke/impact-of-stroke
van Dongen L, et al. Stroke survivors’ experiences with rebuilding life in the community and exercising at home: A qualitative study. Nurs Open. 8(5), 2567–2577 (2021).
Husseini, N. E. et al. Cognitive impairment after ischemic and hemorrhagic stroke: a scientific statement from the American heart association/american stroke association. J. Stroke. 54, 272–291 (2023).
Liu, L. et al. Natural History of Depression Up To 18 Years after Stroke: a population-based South London Stroke Register Study (The Lancet Regional Health – Europe, 2024).
Torre, G. L. et al. Factors that Facilitate and Hinder the Return To Work after Stroke: an Overview of Systematic Reviews (La Medicina del Lavoro, 2022).
Lin, B. et al. Unmet Care Needs of community-dwelling Stroke Survivors: a Systematic Review of Quantitative Studies (BMJ Open, 2021).
Kass B, et al. Cost-effectiveness of patient navigation programs for stroke patients-A systematic review. PLoS One. 16(10), 1–21 (2021).
Olver J, et al. Post Stroke Outcome: Global Insight into Persisting Sequelae Using the Post Stroke Checklist. J Stroke Cerebrovasc Dis. 30(4), 1–7 (2021).
Tan Tock Seng Hospital. Your Health Journey (Tan Tock Seng Hospital. [Online], 2025).
Philp I, et al. Global Stroke Community Advisory Panel. Development of a poststroke checklist to standardize follow-up care for stroke survivors. J Stroke Cerebrovasc Dis. 22(7), e173-80 (2013).
Markle-Reid M, et al. An integrated hospital-to-home transitional care intervention for older adults with stroke and multimorbidity: A feasibility study. J Comorb. 10, 1–21 (2020).
Ward, A. B. et al. Evaluation of the post stroke checklist: a pilot study in the united Kingdom and Singapore. Int. J. Stroke.9 Suppl A100, 76–84 (2014).
Månsson, K. et al. The post-stroke Checklist: Longitudinal Use in Routine Clinical Practice during First Year after Stroke (BMC Cardiovascular Disorders, 2024).
Grefkes, C. & Fink, G. R. Recovery from Stroke: Current Concepts and Future Perspectives (Neurological Research and Practice, 2020).
Brott, T. et al. Measurements of acute cerebral infarction: a clnical examination scale. Am. Heart Association J. 20(7), 864–870 (1989).
Joint Commission. Specifications Manual for Joint Commission National Quality Measures (v2018B). (2019).
Shah, S., Vanclay, F. & Cooper, B. Improving the sensitivity of the Barthel index for stroke rehabilitation. J. Clin. Epidemiol. 42(8), 703–709 (1989).
Lin, K-H., Lin, H-J. & Yeh, P-S. Determinants of prolonged length of hospital stay in patients with severe acute ischemic stroke. J. Clin. Med. 11(12), 1–8 (2022).
Bijl, T. & Mudzi, W. & Comley-White, N. Predictor of patient length of stay post stroke rehabilitation. Afr. Health Sci. 23(2), 543–552 (2023).
Tan, W. S. et al. Factors predicting inpatient rehabilitation length of stay of acute stroke patients in Singapore. Arch Phys Med Rehabil. 90, 1202–1207 (2009).
Brosseau, L. et al. Post-stroke inpatient rehabilitation. I. Predicting length of stay. Am. J. Phys. Med. Rehabil. 75, 422–430 (1996).
Glader, E. L. et al. Socioeconomic factors’ effect on return to work after first stroke. Acta Neurilogica Scand. 135(6), 608–613 (2016).
Brey, J. K. & Wolf, T. J. Socioeconomic disparities in work performance following mild stroke. Disabil. Rehabilitation. 37(2), 106–112 (2016).
Orange, C. et al. Determinants of return to work after a stroke: a systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 105(2), 359–368 (2024).
Mascarenhas, R. et al. Predictors of return to work after a year since stroke: A systematic review. Clin. Epidemiol. Global Health, 27, 1–10 (2024).
Venketasubramanian, N. Stroke demographics, risk factors, subtypes, syndromes, mechanisms and inter-ethnic differences between Chinese, Malays and Indians in Singapore—a hospital-based study. Journal of Cardiovascular Development and Disease, 11. (2024).
Author information
Authors and Affiliations
Contributions
All authors contributed to the intellectual development of this paper. The TTSH and NNI teams designed the study and collected the data. P.M.J., H.J.W.Y., and W.F.Y. performed the analysis. F.E.J.W. and W.F.Y. wrote the first draft. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wei, E.F., Yip, W.F., Yee, J.H.W. et al. Evaluation of the SLS CHARTER care model to support post-stroke care continuity and employment. Sci Rep 15, 43142 (2025). https://doi.org/10.1038/s41598-025-27343-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27343-9
