
Abstract
To compare survival outcomes between surgery and chemoradiotherapy in patients with stage T1bN0M0 esophageal cancer. Stage T1bN0M0 esophageal cancer patients treated with either surgery or chemoradiotherapy were extracted from the Surveillance, Epidemiology, and End Results database between 2000 and 2020. Included patients were divided into two groups: surgery and chemoradiotherapy. Cancer-specific survival (CSS) and overall survival (OS) were compared between the two groups. Among the 515 patients included in the study, 55 (10.7%) underwent chemoradiotherapy and 460 (89.3%) received surgery. Surgery showed better 5-year CSS (73.2% vs. 31.0%; hazard ratio [HR] = 0.27, 95% confidence interval [CI] 0.19–0.39; P < 0.001) and OS (60.0% vs. 21.5%; HR = 0.35, 95% CI 0.25–0.48; P < 0.001) compared to chemoradiotherapy. Subgroup analysis indicated that surgery remained associated with superior 5-year CSS (61.3% vs. 40.6%; HR = 0.51, 95% CI 0.26–0.99; P = 0.049) and OS (48.9% vs. 23.8%; HR = 0.52, 95% CI 0.29–0.91; P = 0.021) compared to chemoradiotherapy in squamous cell carcinoma patients. Similarly, surgery showed better 5-year CSS (76.0% vs. 27.1%; HR = 0.22, 95% CI 0.14–0.34; P < 0.001) and OS (62.7% vs. 20.6%; HR = 0.31, 95% CI 0.21–0.46; P < 0.001) compared to chemoradiotherapy in adenocarcinoma patients. Surgery is associated with superior survival outcomes compared to chemoradiotherapy in stage T1bN0M0 esophageal cancer and should be considered the preferred treatment for eligible patients, particularly in settings where consistent follow-up and salvage therapy may be limited.
Similar content being viewed by others
Introduction
Esophageal cancer is the sixth leading cause of cancer-related mortality worldwide, accounting for approximately 4.3% of all annual cancer deaths1. Advances in diagnostic techniques, such as endoscopic ultrasonography and high-resolution imaging, have improved the detection of early-stage lesions, significantly enhancing long-term survival outcomes2. For patients with stage T1bN0M0 esophageal cancer, radical esophagectomy is currently the recommended treatment, achieving 5-year survival rates exceeding 85% in high-volume centers with multidisciplinary care teams3. However, approximately 15–25% of these patients are ineligible for surgical intervention, necessitating alternative therapeutic strategies4,5.
Although chemoradiotherapy has been established as a curative modality for locally advanced esophageal cancer6, its role in stage T1bN0M0 disease remains inadequately investigated. A recent study suggested non-inferior overall survival (OS) for chemoradiotherapy versus surgery in T1bN0M0 squamous cell carcinoma7. However, this evidence was limited by the exclusion of adenocarcinoma patients and a small randomized cohort, highlighting a critical gap in understanding the efficacy of chemoradiotherapy across histological subtypes.
To address these knowledge gaps, we hypothesized that chemoradiotherapy may achieve comparable survival outcomes to surgery in T1bN0M0 esophageal cancer patients. Using the Surveillance, Epidemiology, and End Results (SEER) database, we conducted a multicenter propensity score-matched cohort analysis to evaluate this hypothesis. This study aims to provide robust evidence to inform clinical decision-making for the management of stage T1bN0M0 esophageal cancer.
Materials and methods
Patients
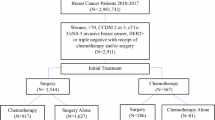
This retrospective cohort study analyzed data from the SEER program (2000 to 2020). We included patients with histologically confirmed stage T1bN0M0 esophageal cancer, comprising both adenocarcinoma (International Classification of Diseases for Oncology, 3rd Edition [ICD-O-3] codes: 8140-8389) and squamous cell carcinoma (ICD-O-3 codes: 8050-8089). To focus on curative-intent treatments, we excluded patients who received radiotherapy alone, chemotherapy alone, or no treatments.
Demographic and clinical characteristics, including age, sex, race, primary tumor location, histological subtype, and tumor grade, were extracted. Patients were classified into two groups according to treatment received: surgery or chemoradiotherapy.
Statistical analysis
Age was dichotomized based on the median value. Categorical variables (age group, race, sex, histology, tumor site, and grade) were compared between treatment groups using the χ2 test or Fisher’s exact test, depending on the distribution of the data.
Survival outcomes were evaluated with Kaplan–Meier curves for both cancer-specific survival (CSS) and OS, and compared using the log-rank test. Multivariable Cox proportional hazards models were applied to identify independent prognostic factors of CSS and OS, adjusting for all baseline characteristics. Subgroup analyses were conducted separately for adenocarcinoma and squamous cell carcinoma.
To mitigate selection bias between the chemoradiotherapy and surgery groups, we performed a 1:1 propensity score matching (PSM) using nearest-neighbor matching without replacement. Matching covariates included age, sex, race, tumor location, histology, and grade. A caliper width of 0.1 was selected to balance bias reduction and matching feasibility. Sensitivity analyses were conducted using calipers of 0.05 and 0.15 to assess result robustness.
After matching, covariate balance was assessed using standardized mean differences, with standardized mean differences < 0.1 considered acceptable. All analyses were repeated with inverse probability weighting as a sensitivity check to confirm consistency.
All analyses were performed using SPSS version 26.0 (IBM Corp.) and R software (version 4.4.0). A two-sided P-value < 0.05 was considered statistically significant.
Results
Patient characteristics
This study included 515 patients, among whom 55 (10.7%) received chemoradiotherapy and 460 (89.3%) underwent surgery. In the surgical group, the median number of examined lymph nodes was 9 (interquartile range: 0–18). Table 1 summarizes baseline characteristics before and after PSM.
Before matching, significant differences were observed between the two groups in race (P = 0.014), tumor location (P = 0.001), histological subtype (P = 0.002), and tumor grade (P = 0.030). After matching, all covariates were well balanced, with standardized mean differences < 0.1.
Factors associated with treatment selection
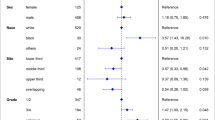
Logistic regression identified lower esophageal tumor location as a factor positively associated with surgical treatment (odds ratio [OR] = 3.35, 95% confidence interval [CI]: 1.06–9.86; P = 0.032) (Fig. 1). In contrast, patients with unknown tumor grade were more likely to receive chemoradiotherapy (OR = 0.30, 95% CI 0.12–0.79; P = 0.010).

Logistic regression analysis for factors associated with surgery in patients with stage T1bN0M0 esophageal cancer. The analysis identifies significant predictors for choosing surgery over chemoradiotherapy.
Survival outcomes before PSM
The surgery group demonstrated superior 5-year CSS than the chemoradiotherapy group (73.2% vs. 31.0%; hazard ratio [HR] = 0.27, 95% CI 0.19–0.39; P < 0.001) (Fig. 2A). Multivariable proportional hazards regression confirmed surgery as an independent prognostic factor for CSS (HR = 0.28, 95% CI 0.19–0.42; P < 0.001) (Fig. re 2B).

Survival outcomes in the unmatched cohort of patients. (A) Comparison of cancer-specific survival between chemoradiotherapy and surgery. (B) Multivariable proportional hazards regression analysis of cancer-specific survival. (C) Comparison of overall survival between chemoradiotherapy and surgery. (D) Multivariable proportional hazards regression analysis of overall survival.
Similarly, surgery was associated with superior 5-year OS compared to chemoradiotherapy (60.0% vs. 21.5%; HR = 0.35, 95% CI 0.25–0.48; P < 0.001) (Fig. 2C). Multivariable analysis also identified surgery as independently predictive of better OS (HR = 0.39, 95% CI 0.28–0.55; P < 0.001) (Fig. 2D).
Causes of death
Cumulative incidence analysis revealed significantly higher 5-year esophageal cancer-specific mortality in the chemoradiotherapy group (60.3% vs. 24.5%, P < 0.001, Fig. 3A). Non-cancer mortality rates at 5 years were comparable between groups (18.2% vs. 15.5%, P = 0.843). Subgroup analysis showed no significant differences in lung-related mortality (3.6% vs. 4.2%, P = 0.604, Fig. 3B) or cardiovascular mortality (5.5% vs. 5.0%, P = 0.922, Fig. 3C).

Cumulative incidence functions of death between the chemoradiotherapy and surgery groups. (A) Non-tumor death. (B) Death due to lung disease. (C) Death due to heart disease.
Survival outcomes after PSM
After PSM, surgery maintained superior CSS (69.8% vs. 30.9%; HR = 0.28, 95% CI 0.15–0.52; P < 0.001; Fig. 4A) and OS (59.2% vs. 20.4%; HR = 0.38, 95% CI 0.23–0.63; P < 0.001; Fig. 4C) compared to chemoradiotherapy. Multivariable analyses confirmed surgery as an independent predictor for both CSS (HR = 0.27, 95% CI 0.14–0.51; P < 0.001; Fig. 4B) and OS (HR = 0.37, 95% CI 0.22–0.61; P < 0.001; Fig. 4D).

Survival outcomes in the propensity-matched cohort of patients. (A) Comparison of cancer-specific survival between chemoradiotherapy and surgery. (B) Multivariable proportional hazards regression analysis of cancer-specific survival. (C) Comparison of overall survival between chemoradiotherapy and surgery. (D) Multivariable proportional hazards regression analysis of overall survival.
Subgroup analysis of patients with squamous cell carcinoma
Surgery was associated with significantly improved 5-year CSS (61.3% vs. 40.6%; HR = 0.51, 95% CI 0.26–0.99; P = 0.049; Fig. 5A) and OS (48.9% vs. 23.8%; HR = 0.52, 95% CI 0.29–0.91; P = 0.021; Fig. 5C). Multivariable analyses consistently showed surgery as an independent prognostic factor for CSS (HR = 0.40, 95% CI 0.19–0.89; P = 0.024; Fig. 5B) and OS (HR = 0.53, 95% CI 0.28–0.99; P = 0.046; Fig. 5D).

Survival outcomes of patients with esophageal squamous cell carcinoma. (A) Comparison of cancer-specific survival between chemoradiotherapy and surgery. (B) Multivariable proportional hazards regression analysis of cancer-specific survival. (C) Comparison of overall survival between chemoradiotherapy and surgery. (D) Multivariable proportional hazards regression analysis of overall survival.
Subgroup analysis of patients with adenocarcinoma
Surgery yielded superior 5-year CSS (76.0% vs. 27.1%; HR = 0.22, 95% CI 0.14–0.34; P < 0.001; Fig. 6A)) and OS (62.7% vs. 20.6%; HR = 0.31, 95% CI 0.21–0.46; P < 0.001; Fig. 6C). Multivariable models confirmed the independent prognostic value of surgery for both CSS (HR = 0.21, 95% CI 0.13–0.34; P < 0.001; Fig. 6B) and OS (HR = 0.31, 95% CI 0.20–0.47; P < 0.001; Fig. 6D).

Survival outcomes of patients with esophageal adenocarcinoma. (A) Comparison of cancer-specific survival between chemoradiotherapy and surgery. (B) Multivariable proportional hazards regression analysis of cancer-specific survival. (C) Comparison of overall survival between chemoradiotherapy and surgery. (D) Multivariable proportional hazards regression analysis of overall survival.
Discussion
This study demonstrates that surgery is associated with significantly improved CSS and OS in patients with stage T1bN0M0 esophageal cancer, irrespective of histological subtype. These findings support the current recommendation of surgery as the standard treatment for eligible patients.
Although surgery appears to be the optimal approach, a notable proportion of patients (15–25%) who are candidates for surgery instead receive chemoradiotherapy in real-world practice. While advanced age is a commonly cited reason for non-surgical management, our data showed no significant age difference between treatment groups (P = 0.377), and logistic regression indicated that age ≥ 67 years was not associated with increased likelihood of receiving chemoradiotherapy. Furthermore, comorbidities are also cited reasons. Although detail of comorbidities was not available in our study, the comparable rates of lung-related death and heart-related mortality between groups suggested that baseline comorbidities might not have differed substantially. The survival benefit observed in the surgical group thus appears to derive primarily from improved tumor control, as evidenced by the significantly lower esophageal cancer-specific mortality in this group. At last, performance status undoubtedly influences treatment selection. However, patients with T1b disease are less likely to have tumor-related performance impairment compared to those with advanced stages. The low utilization of chemoradiotherapy in our cohort is therefore unlikely to be attributable solely to performance status.
Potential reasons for selecting chemoradiotherapy include concerns over surgical complications, such as pneumonia, vocal cord palsy, and anastomotic leakage, which can prolong hospitalization and increased perioperative mortality risk8. Additionally, many patients experience lasting alterations in dietary habits and quality of life after esophagectomy9,10,11. Furthermore, in regions with limited access to high-volume surgical centers, chemoradiotherapy may also represent a more feasible and widely available alternative12,13,14,15,16. Thus, a range of factors, including patient preference, physician bias, geographic accessibility, and economic considerations, may influence treatment selection. Multidisciplinary evaluation involving surgeons, medical oncologists, radiation oncologists, and endoscopists is essential to tailor treatment recommendations to individual patient values, potential toxicities, and expected outcomes.
A previous clinical trial reported non-inferior 5-year OS with chemoradiotherapy versus surgery in squamous cell carcinoma (86.5% vs. 85.5%; adjusted HR = 1.052, 95% CI 0.674–1.640)7. However, that study also identified worse 5-year progression-free survival with chemoradiotherapy (81.7% vs. 71.6%; adjusted HR = 1.478, 95% CI 1.010–2.162), suggesting that more intensive follow-up and timely salvage treatment in the trial setting may have mitigated survival differences17,18,19. As the SEER database does not capture recurrence data or detailed follow-up protocols, this bias cannot be assessed in our study. Instead, we analyzed cause-specific mortality and found comparable non-cancer death rates between groups, implying that patients receiving chemoradiotherapy may not have consistently received salvage therapy upon progression. The high cancer-specific mortality in the chemoradiotherapy group may reflect real-world limitations in consistent follow-up and access to salvage therapies, which could narrow the survival gap in settings with rigorous surveillance protocols. This supports the recommendation of surgery for patients who may lack access to regular follow-up.
As a non-surgical option, radiotherapy for stage T1bN0M0 esophageal cancer must be considered in light of a 20–40% risk of lymph node metastasis20,21, underscoring the necessity of combining chemotherapy with radiotherapy. The efficacy of chemoradiotherapy (CRT) is evidenced by long-term follow-up, showing an 87.5% complete response rate and 5-year overall, disease-free, and locoregional failure-free survival rates of 86%, 59%, and 90%, respectively22,23. Consistent with this, comparative studies demonstrate a significant survival benefit for chemoradiotherapy over radiotherapy alone24,25.
Technical advances in radiotherapy delivery are also vital. Involved-field irradiation, while associated with excellent long-term survival, still fails to prevent locoregional recurrence in approximately 20% of patients26,27. Combining chemoradiotherapy with elective nodal irradiation has been proposed to address this limitation. The definitive influence of irradiation volume on patient outcomes is expected to be clarified by an ongoing phase III clinical trial28.
Our study addresses an important evidence gap by including both histological subtypes, employing propensity score matching to minimize confounding, and analyzing real-world outcomes from a large national database. However, several limitations should be acknowledged. First, detailed treatment parameters, such as surgical techniques, chemotherapy regimens, radiation doses, and toxicities, were unavailable. These factors are critical in influencing treatment outcomes17,29,30. Second, accurate staging of early esophageal cancer remains challenging, and misclassification of T1b lesions is possible, particularly in non-surgically treated patients31,32,33,34,35. Third, the small sample size in the chemoradiotherapy group may affect the statistical power and generalizability of our findings. Future prospective studies or randomized trials incorporating more precise staging and treatment details are needed to validate these results. Furthermore, future research should aim to evaluate the impact of follow-up intensity and salvage therapy accessibility on long-term outcomes in patients receiving non-surgical treatments.
In conclusion, our analysis suggests that surgery is associated with superior survival compared to chemoradiotherapy in stage T1bN0M0 esophageal cancer, especially when rigorous follow-up and salvage therapy cannot be assured. Individualized treatment decisions should consider patient preferences, comorbidities, and access to multidisciplinary care.
Data availability
The data are available from the corresponding author upon request.
Abbreviations
- OS:
-
Overall survival
- SEER:
-
The Surveillance, Epidemiology, and End Results
- ICD-O-3:
-
International Classification of Diseases for Oncology, 3rd Edition
- CSS:
-
Cancer-specific survival
- PSM:
-
Propensity score matching
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- HR:
-
Hazard ratio
References
Sung, H. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 71(3), 209–249 (2021).
Zhu, H. et al. Esophageal cancer in China: Practice and research in the new era. Int. J. Cancer. 152(9), 1741–1751 (2023).
Kanie, Y. et al. Additional treatment following noncurative endoscopic resection for esophageal squamous cell carcinoma: A comparison of outcomes between esophagectomy and chemoradiotherapy. Ann. Surg. Oncol. 28(13), 8428–8435 (2021).
Kitagawa, Y. et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: Part 1. Esophagus 16(1), 1–24 (2019).
Lordick, F. et al. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 27(suppl 5), v50–v57 (2016).
Cooper, J. S. et al. Chemoradiotherapy of locally advanced esophageal cancer: Long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA 281(17), 1623–1627 (1999).
Kato, K. et al. Parallel-group controlled trial of surgery versus chemoradiotherapy in patients with stage I esophageal squamous cell carcinoma. Gastroenterology. 161(6), 1878–1886 (2021).
Fabbi, M., Hagens, E. R. C., van Berge Henegouwen, M. I. & Gisbertz, S. S. Anastomotic leakage after esophagectomy for esophageal cancer: definitions, diagnostics, and treatment. Dis. Esophagus. 34(1), doaa039 (2021).
Smyth, E. C. et al. Oesophageal cancer. Nat. Rev. Dis. Primers 3, 17048 (2017).
Noordman, B. J. et al. Quality of life during and after completion of neoadjuvant chemoradiotherapy for esophageal and junctional cancer. Ann. Surg. Oncol. 26(13), 4765–4772 (2019).
Derogar, M., Orsini, N., Sadr-Azodi, O. & Lagergren, P. Influence of major postoperative complications on health-related quality of life among long-term survivors of esophageal cancer surgery. J. Clin. Oncol. 30(14), 1615–1619 (2012).
Merritt, R. E., Abdel-Rasoul, M., Fitzgerald, M., D’Souza, D. M. & Kneuertz, P. J. The academic facility is associated with higher utilization of esophagectomy and improved overall survival for esophageal carcinoma. J. Gastrointest. Surg. 25(7), 1677–1689 (2021).
Muslim, Z. et al. Impact of facility type and volume in locally advanced esophageal cancer. Asian Cardiovasc. Thorac. Ann. 32(1), 19–26 (2024).
Wouters, M. W., Gooiker, G. A., van Sandick, J. W. & Tollenaar, R. A. The volume-outcome relation in the surgical treatment of esophageal cancer: A systematic review and meta-analysis. Cancer 118(7), 1754–1763 (2012).
Di, J., Lu, X. S., Sun, M., Zhao, Z. M. & Zhang, C. D. Hospital volume-mortality association after esophagectomy for cancer: A systematic review and meta-analysis. Int. J. Surg. 110(5), 3021–3029 (2024).
Kim, B. R. et al. The association between hospital case-volume and postoperative outcomes after esophageal cancer surgery: A population-based retrospective cohort study. Thorac. Cancer 12(18), 2487–2493 (2021).
Kato, K. et al. Phase II study of concurrent chemoradiotherapy at the dose of 50.4 Gy with elective nodal irradiation for Stage II–III esophageal carcinoma. Jpn. J. Clin. Oncol. 43(6), 608–615 (2013).
Tachimori, Y. et al. Salvage esophagectomy after high-dose chemoradiotherapy for esophageal squamous cell carcinoma. J. Thorac. Cardiovasc. Surg. 137(1), 49–54 (2009).
Takeuchi, H. et al. Factors influencing the long-term survival in patients with esophageal cancer who underwent esophagectomy after chemoradiotherapy. World J. Surg. 34(2), 277–284 (2010).
Eguchi, T. et al. Histopathological criteria for additional treatment after endoscopic mucosal resection for esophageal cancer: Analysis of 464 surgically resected cases. Mod. Pathol. 19(3), 475–480 (2006).
Kim, D. U. et al. Risk factors of lymph node metastasis in T1 esophageal squamous cell carcinoma. J. Gastroenterol. Hepatol. 23(4), 619–625 (2008).
Murakami, Y. et al. Long-term results of definitive concurrent chemoradiotherapy for patients with esophageal submucosal cancer (T1bN0M0). Int. J. Clin. Oncol. 20(5), 897–904 (2015).
Kato, H. et al. A phase II trial of chemoradiotherapy for stage I esophageal squamous cell carcinoma: Japan Clinical Oncology Group Study (JCOG9708). Jpn. J. Clin. Oncol. 39(10), 638–643 (2009).
Li, J., Jia, Y., Cheng, Y. & Wang, J. Chemoradiotherapy vs radiotherapy for nonoperative early stage esophageal cancer: A seer data analysis. Cancer Med. 9(14), 5025–5034 (2020).
Wang, R. Z., Liang, H. W., Liu, Y., Huang, W. & Pan, X. B. Chemoradiotherapy versus radiotherapy in patients with stage T1N0M0 esophageal cancer: A retrospective cohort study. J. Gastroenterol. Hepatol. 40, 2705–2713 (2025).
Nakatani, Y. et al. Comparison of involved field radiotherapy and elective nodal irradiation in combination with concurrent chemotherapy for T1bN0M0 esophageal cancer. Int. J. Clin. Oncol. 25(6), 1098–1104 (2020).
Kawamoto, T., Shikama, N., Mine, S. & Sasai, K. Comparison of recurrence patterns and salvage treatments after definitive radiotherapy for cT1a and cT1bN0M0 esophageal cancer. Front. Oncol. 12, 857881 (2022).
Sasaki, K. et al. A phase III randomized controlled trial comparing local field with additional prophylactic irradiation in chemoradiotherapy for clinical-T1bN0M0 esophageal cancer: ARMADILLO trial (JCOG1904). Jpn. J. Clin. Oncol. 54(1), 103–107 (2024).
Kato, K. et al. Phase II study of chemoradiotherapy with 5-fluorouracil and cisplatin for Stage II-III esophageal squamous cell carcinoma: JCOG trial (JCOG 9906). Int. J. Radiat. Oncol. Biol. Phys. 81(3), 684–690 (2011).
Onozawa, M. et al. Elective nodal irradiation (ENI) in definitive chemoradiotherapy (CRT) for squamous cell carcinoma of the thoracic esophagus. Radiother. Oncol. 92(2), 266–269 (2009).
Katada, C. et al. Curative management after endoscopic resection for esophageal squamous cell carcinoma invading muscularis mucosa or shallow submucosal layer-multicenter real-world survey in Japan. Am. J. Gastroenterol. 118(7), 1175–1183 (2023).
Minashi, K. et al. Efficacy of endoscopic resection and selective chemoradiotherapy for stage I esophageal squamous cell carcinoma. Gastroenterology. 157(2), 382–390 (2019).
Nihei, K. et al. Final analysis of diagnostic endoscopic resection followed by selective chemoradiotherapy for stage I esophageal cancer: JCOG0508. Gastroenterology 164(2), 296–299 (2023).
Yang, X. et al. Radiotherapy improves survival of patients with lymphovascular invasion in pT1b esophageal squamous cell cancer after endoscopic submucosal dissection. Am. J. Gastroenterol. 118(8), 1344–1352 (2023).
Ishihara, R. et al. Endoscopic submucosal dissection/endoscopic mucosal resection guidelines for esophageal cancer. Dig. Endosc. 32(4), 452–493 (2020).
Acknowledgements
The authors thank the Surveillance, Epidemiology, and End Results program for providing the data used in this study.
Author information
Authors and Affiliations
Contributions
Conceptualization: Zu-Yi Chen; Methodology: Huan-Wei Liang and Yang Liu; Formal analysis: Shou-Feng Wang and Huan-Wei Liang; Investigation: Zu-Yi Chen; Resources: Shou-Feng Wang and Huan-Wei Liang; Validation: Wei Huang; Writing—original draft preparation: Zu-Yi Chen; Writing—review and editing: Xin-Bin Pan.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, ZY., Wang, SF., Liang, HW. et al. Surgery versus chemoradiotherapy in patients with stage T1bN0M0 esophageal cancer: a retrospective cohort study. Sci Rep 15, 43364 (2025). https://doi.org/10.1038/s41598-025-27430-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27430-x
