
Abstract
To evaluate the relationship of diabetes duration and glycemic control with risk of stroke and its major subtypes using data from the UK Biobank, a large population-based cohort of UK adults. We included 23,401 UK adult residents with diabetes who had no known stroke at baseline (2006–2010). Diabetes duration was self-reported and glycemic control was assessed by glycated hemoglobin (HbA1c) levels. Their associations with incident stroke were assessed using multivariate Cox models. During a median follow-up of 11.6 years, 982 incident cases of stroke were identified. A longer diabetes duration was associated with higher risk of total stroke, ischemic stroke (IS), and hemorrhagic stroke (HS) (≥ 15 vs. <5 years: HRs [95% CI] were 1.81 [1.50, 2.19], 1.80 [1.47, 2.20], and 2.17 [1.46, 3.23], respectively), while higher levels of HbA1c were associated with higher risk of total stroke and IS but not HS (≥ 8.0% vs. <7.0%: HRs [95% CI] were 1.78 [1.52, 2.09], 1.93 [1.63, 2.28], and 0.97 [0.67, 1.41], respectively). Diabetes duration interacted with glycemic status on total stroke and IS (both P-for-interaction values < 0.01). Individuals who had the longest diabetes duration (≥ 15 years) and poorer glycemic control (≥ 8.0%) had particularly higher risk of total stroke (HR = 3.21; 95% CI: 2.55, 4.04) and IS (HR = 3.47; 95% CI: 2.73, 4.40) as compared with those who had a duration of < 5 years with HbA1c < 8%. A longer diabetes duration and poorer glycemic control were both associated with higher risk of total stroke and IS, and the risk may be further exacerbated with the coexistence of both risk factors.
Similar content being viewed by others
Introduction
Stroke is the second leading cause of death and the third leading cause of disability worldwide1,2. There were 12.2 million incident cases, 101 million prevalent cases, 6.55 million deaths, and 143 million DALYs of stroke worldwide in 2019. Stroke costs more than 721 billion dollars or 0.66% of the global GDP3. Although age-standardised mortality rates for stroke decreased sharply, the decrease in age-standardised incidence was much less steep4, suggesting that prevention efforts have been less successful than treatment efforts.
Individuals with diabetes are at higher risk of developing stroke5,6. Thus, identification of disease-progression markers in diabetes is relevant for diabetes management and stroke prevention. Duration of diagnosis of diabetes(both type 1 and type 2), which is a proxy of diabetes progression, has been positively associated with adverse cardiovascular outcomes7,8,9,10,11,12. The relationship between diabetes duration and risk of stroke is less clear, and the majority of previous studies on this topic have been focused on total stroke13 or ischemic stroke (IS) only14. On the other hand, cumulative evidence has demonstrated that poorer glycemic control in type 1 diabetes is associated with higher risk of stroke and other macrovascular complications15,16. Similar to the studies on diabetes duration and stroke, there are very few studies that have explored the relationship between glycemic control and major subtypes of stroke (i.e., IS and hemorrhagic stroke [HS]), with inconsistent findings5,15,17.
An additional open issue relates to whether there are potential interplays between diabetes duration and glycemic control on the incidence of stroke or its subtypes. Indeed, in the guidelines for diabetes, it has been pointed out that the control targets of glycemic control need to be tailored according to the duration of diabetes18,19. Chronic hyperglycemia in diabetes leads to vascular damage, including endothelial dysfunction, atherosclerosis, and increased arterial stiffness, which are key pathophysiological mechanisms linking diabetes to both IS and HS11,20. Our previous studies have also revealed that both glycemic control and diabetes duration were important predictive indices for cardiovascular disease (CVD) and mortality among individuals with diabetes21,22. However, because of the limited epidemiological evidence for stroke, neither the Guidelines for the Primary Prevention of Stroke from the American Heart Association, nor the European Stroke Initiative have highlighted the importance of diabetes duration and glycemic control among individuals with diabetes23,24,25. It would be clinically relevant to elucidate the influences of diabetes duration, glycemic control, and their potential interplays on the development of stroke and its major subtypes.
To fill these knowledge gaps, we used data collected for participants in the UK Biobank, a large-scale population-based prospective cohort study, to investigate the relationship of diabetes duration, glycemic control, and their interplays with risk of stroke and its major subtypes among individuals with diabetes.
Research design and methods
The UK Biobank is a large-scale, population-based cohort study of over 500,000 participants. Between 2006 and 2010, participants visited 22 assessment centres in England, Scotland and Wales for baseline assessments26,27. A wide range of information was collected for the study participants at baseline, including sociodemographic, lifestyle, anthropometric, and clinical factors28,29. The study was approved by the National Health Service (NHS) National Research Ethics Service (REC reference: 11/NW/03820) and all participants provided written informed consent to participate in the study. All procedures were performed in accordance with the relevant guidelines and regulations, including the Declaration of Helsinki and the UK Biobank Ethics and Governance Framework.
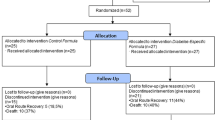
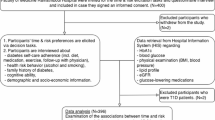
Of the initial 502,442 participants, 30,912 had diabetes. Among these, we excluded 1194 participants who had a history of stroke at baseline, 4628 participants without measurement of HbA1c or age of diabetes onset, 1689 participants with missing covariates. Finally, 23,401 participants with diabetes were included in the present analysis (Fig. S1).
Assessment of diabetes duration and glycemic control
We identified participants with diabetes according to the following predefined criteria30: (1) a history of diabetes in the medical record (International Classification of Diseases ICD-9 codes 250 and 6480 or ICD-10 codes E10 to E14)30; (2) self-reported history of diabetes; (3) self-reported diabetes medication use; or (4) HbA1c level ≥ 48 mmol/mol (6.5%). The age at diabetes onset was determined by the question “What was your age when diabetes was first diagnosed?”. Undiagnosed diabetes was defined if a participant was not previously diagnosed with diabetes but had HbA1c level that exceeded the diabetes threshold (≥ 6.5%, 48 mmol/mol). The duration of undiagnosed diabetes was designated as 0 years. In the UK Biobank, HbA1c levels were measured in a central laboratory from November 5rd, 2014 to October 3rd, 2017 and were adjusted for the variables by the UK Biobank before analysis31. HbA1c was used as a stable indicator of glycemic control because it reflects the average glycemic concentration over the previous 3 months32.
According to the European Society of Cardiology guidelines33, glycemic control can be categorized into near-normal targets (HbA1c < 7.0%) and less-rigorous targets (HbA1c < 8.0%). We grouped the participants with diabetes based on duration of the diagnosis of diabetes (< 5, 5 to < 15, and ≥ 15 years) and by HbA1c levels (< 7.0% [< 53.0 mmol/mol], 7.0 to < 8.0% [53.0 to < 64.0 mmol/mol], and ≥ 8.0% [64.0 mmol/mol]). We categorized diabetes duration into three groups (< 5 y, 5 to < 15 y, and ≥ 15 y) based on clinical relevance and to ensure sufficient sample sizes for robust statistical analyses. In comparison to our previous studies22,34, where diabetes duration was divided into four groups (< 5 y, 5 to < 10 y, 10 to < 15 y, and ≥ 15 y), we combined the intermediate categories (5 to < 10 y and 10 to < 15 y) into a single group (5 to < 15 y) to address the issue of smaller sample sizes, especially for rare outcomes like hemorrhagic stroke.
Covariates
Information about baseline socio-demographic characteristics, lifestyle factors (smoking, alcohol consumption, and diet), and other clinical risk factors in the UK Biobank was collected through a touchscreen questionnaire. A Townsend deprivation index (TDI) was derived using participants’ postal codes and information from the national census output area. A food frequency questionnaire was used to evaluate regular dietary habits and alcohol consumption. A healthy diet score (from 0 to 6 points) and the amounts of alcohol consumption were calculated according to the methods reported previously21,34. Daily sedentary time (hours) was obtained by integrating the time participants spent watching TV, using computers, and driving every day35. Other clinical risk factors such as height, weight, and systolic blood pressure (SBP) were obtained by trained nurses. Height and weight were used to calculate body mass index (BMI, kg/m2). The history of coronary heart disease (CHD) was determined by self-report and hospital diagnosis. More details about the measurements can be found in the UK Biobank Data Display and Agreement (http://www.ukbiobank.ac.uk).
Outcome assessment
The primary outcome was total stroke and the secondary outcomes were the two major subtypes of stroke including IS and HS. The adjudication of stroke events was performed by the UK Biobank Outcome Adjudication Group through linkage with hospital admissions data and the national death register. The ICD codes were used to define the incident cases. The codes for IS included ICD-9: 434. X, 434.0, 434.1, 434.9, and 436. X; ICD-10: I63-I64; and the codes for HS included ICD-9: 430. X and 431. X; ICD-10: I60-I60.9. Previous validation study has demonstrated high diagnostic accuracy for identifying incident stroke cases in UK Biobank and the data are sufficient for research36.
Statistical analysis
Baseline participant characteristics were reported according to the categories for diabetes duration and HbA1c levels. We used Cox proportional hazards model to estimate hazard ratio (HR) and 95% confidence interval (CI) of stroke according to the categories for duration of diabetes or HbA1c levels, using age as the potential time scale. At the time of data analyses, the mortality data of Scotland were updated to April 20th, 2020, the mortality data of England and Wales were updated to April 26th, 2020, and the hospital inpatient records were updated to November 30th, 2020. These dates were used as the end of follow-up where appropriate. Person-time of follow-up was calculated from the date of baseline assessment to the date of diagnosis of the event, death, loss to follow-up, or end of follow-up, whichever occurred first. These analyses were conducted using the shortest-duration (< 5 years) or the lowest-HbA1c category (< 7.0%) as the reference. Multivariable adjustments were made to account for age, sex, ethnicity, socioeconomic status (TDI), diet-quality score, alcohol consumption, smoking status, sedentary time, BMI, SBP, antihypertensive medication use, statin use, and history of CHD. Additionally, diabetes duration and HbA1c levels were included in the same model and thus were mutually adjusted for each other.
We also evaluated the potential interaction between diabetes duration and glycemic control on risk of stroke and its subtypes. In this analysis, the relationship between diabetes duration (< 5, 5 to < 15, and ≥ 15 years) and risk of stroke was examined by participants’ HbA1c levels (< 8.0%, and ≥ 8.0%). The P values for interaction between diabetes duration and glycemic control were estimated by including their product term in the aforementioned multivariable regression model. Adjustments were made for age, sex, ethnicity, TDI, BMI, smoking status, alcohol consumption, sedentary time, healthy diet score, SBP, antihypertensive medication use, and history of CHD.
In addition, we explored the joint associations of diabetes duration and glycemic control with risk of stroke and stroke subtypes, using those with the shortest duration (< 5 years) and the lower HbA1c levels (< 8.0%) as the reference. We further examined these joint associations within different subgroups of population defined by sex, age (< 60 or ≥ 60 years), TDI (< or ≥ median), ethnicity (White or other), and BMI (< 30 or ≥ 30 kg/m2). Additionally, we acknowledge that diabetes duration was determined by self-reported data, which may introduce recall bias. To assess the robustness of our findings, we conducted several sensitivity analyses: (1) excluding participants with undiagnosed diabetes; (2) excluding participants with type 1 diabetes; (3) additionally adjusted for psychological stress (depression and anxiety), healthy sleep traits (chronotype, sleep duration, insomnia, snoring, and daytime sleepiness), regular exercise, and microalbuminuria (albumin-to-creatinine ratio, ACR); (4) additionally adjusted for low-density lipoprotein cholesterol as well as the use of statin, aspirin, specific antihyperglycemic drugs (metformin and insulin), and specific antihypertensive drugs (angiotensin-converting enzyme inhibitor, angiotensin II receptor blocker, beta blocker, and calcium channel blocker); (5) to assess the potential impact of missing data, we performed multiple imputation using the mice package in R, generating five imputed datasets and combining estimates across datasets using Rubin’s rules.
All data were analysed using R software (version 4.0.1) or STATA 14.0 (StataCorp LP, College Station, Texas). A two-sided P-value < 0.05 was considered to be statistically significant.
Results
Baseline characteristics
Participants with a longer diabetes duration were slightly older, were more likely to be male and antihypertensive drug users, had lower BMI, had higher likelihood of having CHD, and were less likely to be current smokers (Table 1). Supplementary Table S1 shows the baseline characteristics of the participants according to their HbA1c levels.
Associations of diabetes duration and glycemic control with risk of stroke
During a median follow-up of 11.6 years, 982 incident cases of stroke were identified, including 863 IS and 227 HS cases. After multivariable adjustment, a longer duration of diabetes was associated with a higher risk of stroke and its subtypes (P for trend < 0.001) (Table 2). The adjusted HRs (95% CIs) for total stroke associated with diabetes durations of 5 to < 15 years and ≥ 15 years were 1.30 (1.12, 1.50) and 1.81 (1.50, 2.19), respectively (vs. diabetes duration < 5 years). The corresponding estimates were 1.26 (1.08, 1.47) and 1.80 (1.47, 2.20) for IS and 1.38 (1.02, 1.87) and 2.17 (1.46, 3.23) for HS.
A poorer glycemic control was also associated with higher risk of stroke (P for trend < 0.001) (Table 3). The adjusted HRs (95% CI) for total stroke associated with HbA1c levels of 7.0 to < 8.0% and ≥ 8.0% were 1.20 (1.03, 1.40) and 1.78 (1.52, 2.09), respectively. The corresponding estimates for IS were 1.22 (1.03, 1.44) and 1.93 (1.63, 2.28), respectively. Poor glycemic control was not significantly associated with risk of HS.
We found significant interactions between diabetes duration and HbA1c levels on the risk of total stroke and IS (all P-interaction < 0.05). The duration-stroke associations were more pronounced among those with HbA1c levels ≥ 8.0% than among those with HbA1c levels < 8.0%. Compared with those with a shorter diabetes duration (< 5 years) and better glycemic control (HbA1c < 8%), individuals who had the longest duration of diabetes (≥ 15 years) and higher HbA1c level (≥ 8%) had multivariable HRs (95% CIs) of 3.21 (2.55, 4.04) for total stroke and 3.47 (2.73, 4.40) for IS (Fig. 1). However, regarding HS, the duration-stroke association was significant among those with HbA1c < 8.0% only, while no evidence of an interaction was observed (Fig. 1 and Supplemental Table S2).

Hazard ratios (95% CIs) for the combined effect of diabetes duration and glycemic control on the risk of incident stroke and stroke subtypes among participants with diabetes. Adjustments were made for age, sex, ethnicity, TDI, BMI, smoking status, alcohol consumption, sedentary time, healthy diet score, SBP, antihypertensive medication use, and history of CHD. Abbreviations: CI, confidence interval; HbA1c, glycated hemoglobin; HR, hazard ratio; HS, hemorrhagic stroke; IS, ischaemic stroke. *The conversion of an HbA1c level of 8.0% is 64.0 mmol/mol.
Subgroup analysis and sensitivity analysis
Subgroup analysis showed that the joint associations of diabetes duration and glycemic control with the risk of total stroke were consistent across age, sex, ethnicity, socioeconomic status, and overall obesity subgroups (both P-interaction > 0.10) (Supplementary Table S3). The results were not substantially changed after excluding participants with undiagnosed diabetes or those with type 1 diabetes, after additional adjustment for psychological stress, sleep traits, physical activity, and microalbuminuria, after additional adjustment for low-density lipoprotein cholesterol and the use of statins, aspirin, specific antihyperglycemic agents (e.g., metformin and insulin), and antihypertensive medications (angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, beta blockers, and calcium channel blockers), or after applying multiple imputation for missing data (Supplementary Table S4).
Discussion
Our analysis used data from the UK Biobank study and systematically investigated the independent and joint associations of diabetes duration and glycemic control with incident stroke and its major subtypes among 23,401 adults with diabetes. We found that a longer diabetes duration was associated with higher risk of total stroke, IS, and HS in a dose-response manner, while worse glycemic control, as reflected by elevated HbA1c, was associated with higher risk of total stroke and IS but not HS. Moreover, diabetes duration interacted significantly with glycemic status on total stroke and IS. Individuals who had the longest diabetes duration and poorer glycemic control had particularly higher risk of total stroke and IS.
The relationship between duration of diabetes and risk of stroke has been evaluated in a few previously studies using relatively small sample sizes, and the findings have been inconsistent14. A previous prospective study involving 3298 participants from Northern Manhattan found that diabetes duration was independently associated with an increased risk of IS, with the risk tripling for those with diabetes duration of ≥ 10 years compared to nondiabetic participants14. In another prospective study of 11,069 nurses with diabetes, risk of total stroke and IS were 3.3- and 4.1-fold higher, respectively, for participants with diabetes duration ≥ 20 years (vs. those without diabetes)5. This previous study did not found diabetes duration to be associated with HS5, but there were only 31 HS cases among the participants with diabetes. A study conducted in an East Asian population reported that the associations of diabetes duration and glycemic control with stroke risk became non-significant after multivariable adjustment37. This is in contrast to our study that enrolled ethnicities mainly of white people (nearly 90%) from the UK Biobank and supported that diabetes duration and glycemic control are independent risk factors of stroke even after extensive adjustment for various sets of covariates. Such discrepancies may reflect differences in ethnic composition, genetic susceptibility, or residual confounding between populations. Indeed, a previous study demonstrated that the angiotensin-converting enzyme gene DD genotype was linked to higher stroke risk, underscoring that population-specific genetic and environmental factors could modulate the diabetes–stroke relationship38. Compared to these earlier studies, our study benefits from a significantly larger sample size with hospital inpatient-confirmed incident cases, providing more robust evidence for the association between diabetes duration and stroke risk.
High HbA1c levels have been widely associated with higher risk of stroke, especially IS17,39. For example, in a prospective study of 33,453 participants from Sweden, as compared with matched control participants without diabetes, risk of stroke increased from 75% in the lowest HbA1c category to nearly 8-fold in the highest category40, which is generally consistent with findings of the current study.
The evidence has been more limited and inconsistent regarding the association between HbA1c levels and HS risk. In the abovementioned Swedish cohort, participants with type 1 diabetes were found to have higher risk of HS when their HbA1c levels were high40. In another study of 406,271 Swedish participants with type 2 diabetes, risk of HS increased by nearly 1.5-fold when comparing participants with HbA1c > 87 mmol/mol with participants who had HbA1c ≤ 53 mmol/mol41. Conversely, in a prospective study of 4083 Finnish participants, glycemic control was not associated with HS among participants with diabetes16, which is consistent with our null results regarding the HbA1c-HS association. Mechanistically, poor glycemic control primarily contributes to macrovascular and microvascular damage leading to IS, whereas HS is more strongly associated with hypertension, endothelial dysfunction, and vessel fragility-pathways less directly driven by chronic hyperglycemia42. Additionally, the absence of significant HbA1c-HS associations in our study may be due to several factors: our highest HbA1c category (≥ 8.0% [64 mmol/mol]) does not capture more extreme hyperglycemia, and the number of HS events was relatively low (yielding limited statistical power).
To the best of our knowledge, the joint influence of diabetes duration and glycemic control on stroke risk has not been explored previously. In this study, we found that a longer diabetes duration and higher HbA1c levels were both associated with higher of total stroke and IS. We further found that a coexistence of long-standing diabetes and poor glycemic control conferred substantially higher risk of total stroke and IS. Several potential mechanisms can explain this association of long diabetes duration and poor glycemic control. First, there is evidence of an association between long-term poor glycemic control, which leads to cumulative vascular damage and chronic inflammation, and atherosclerotic lesions11,20, and carotid plaque thickness has been shown to predict stroke43. In addition, the risk of microalbuminuria has been shown to increase with the diabetes duration44,45, and it has been reported that microalbuminuria is an important and independent risk factor for stroke in diabetic patients46.
Our these findings may have public health significance. At present, stroke is still a serious complication in diabetes population14. The age of diabetes onset tends to be younger47, leading to an increasing number of people suffering from long-standing diabetes48. The guidelines for diabetes has pointed out that the control targets of glycemic control need to be tailored according to the duration of diabetes18,19. However, neither the Guidelines for the Primary Prevention of Stroke from the American Heart Association, nor the European Stroke Initiative have emphasized the role of diabetes duration and glycemic control for stroke prevention among individuals with diabetes23,24,25. Findings from the present study highlighted the paramount role of jointly considering diabetes duration and glycemic control in the management of diabetes and prevention of stroke. Thus, our findings may contribute to the early detection and management of modifiable risk factors that reduce the number of individuals developing stroke.
The strengths of the present study include the large sample size with a long-term follow-up. The link to hospital registration and death registers ensures complete information about incident cases. Additionally, a wealth of information about classic risk factors, such as comorbidities and lifestyle factors, enabled us to comprehensively adjust for confounding factors. This study still has some limitations. First, the observational nature of the UK Biobank makes it impossible to exclude the possibility of residual confounding. However, after adjusting for a variety of traditional risk factors, the results of the present study were robust. Second, although HbA1c can reflect glycemic control levels over a few weeks, a single baseline measurement may not be sufficiently reflective of long-term glycemic status. This may underestimate the association between poor glycemic control and stroke risk. Future prospective studies with repeated measurements of HbA1c are needed to more accurately evaluate the long-term effects of glycemic control on stroke risk. Third, the use of self-reported age at diabetes diagnosis to estimate diabetes duration may be subject to recall bias, especially given the typical lag between diabetes onset and clinical diagnosis49. However, our sensitivity analyses indicated that excluding individuals with uncertain diagnosis did not alter the primary results, suggesting that our conclusions are robust to potential recall bias. Fourth, the included participants were mostly of White European descent which may limit the generalization of our findings to other ethnic populations. Fifth, although we did not apply formal multiple-testing corrections, our analyses were based on prespecified outcomes and hypotheses, and the consistency of findings across sensitivity and subgroup analyses suggests that the risk of false positives is low. Sixth, the potential for misclassification of stroke subtypes and undiagnosed early cerebrovascular damage could have affected the accuracy of our outcome assessment. Seventh, there is a possibility of selection bias due to loss to follow-up, which may have influenced our findings. Eighth, although stroke and ischemic stroke outcomes in UK Biobank have demonstrated high diagnostic accuracy in prior validation studies, some misclassification (particularly of hemorrhagic stroke) is still possible. Finally, because of the limited sample size, we were not able to conduct an independent analysis for type 1 diabetes, and further large cohorts of type 1 diabetes are still needed.
Conclusion
Among adults with diabetes, a longer diabetes duration and poorer glycemic control were both associated with higher risk of total stroke and IS, and the risk may be further exacerbated by the coexistence of both risk factors. Clinicians should prioritize regular monitoring of glycemic control and be particularly vigilant in patients with long-standing diabetes to mitigate the risk of stroke. Future studies with diverse populations and repeated glycemic measurements are needed to confirm these findings and guide the development of tailored stroke prevention strategies for individuals with diabetes.
Data availability
Data from the UK Biobank are publicly available and can be accessed at https://www.ukbiobank.ac.uk/.
Abbreviations
- BMI:
-
Body mass index
- CHD:
-
Coronary heart disease
- CI:
-
Confidential interval
- DALYs:
-
Disability-adjusted life years
- HR:
-
Hazard ratio
- HbA1c:
-
Glycated hemoglobin
- ICD:
-
International Classification of Diseases
- NHS:
-
National Health Service
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviation
- TDI:
-
Townsend deprivation index
References
Roth, G. A. et al. Global burden of cardiovascular diseases and risk factors, 1990–2019 update from the GBD 2019 study. J. Am. Coll. Cardiol. 76 (25), 2982–3021 (2020).
Feigin, V. L. et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. 20 (10), 795–820 (2021).
Feigin, V. L. et al. World stroke organization (WSO): global stroke fact sheet 2022. Int. J. Stroke. 17 (1), 18–29 (2022).
Krishnamurthi, R. V., Ikeda, T. & Feigin, V. L. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology 54 (2), 171–179 (2020).
Janghorbani, M. et al. Prospective study of type 1 and type 2 diabetes and risk of stroke subtypes—the nurses’ health study. Diabetes Care. 30 (7), 1730–1735 (2007).
Kissela, B. M. et al. Epidemiology of ischemic stroke in patients with diabetes—the greater Cincinnati/Northern Kentucky stroke study. Diabetes Care. 28 (2), 355–359 (2005).
Emanuele, N. V. Duration of diabetes, glucose control and cardiovascular risk. Diabetologia 53 (1), 214–215 (2010).
Spijkerman, A. M. W. et al. Impact of diabetes duration and cardiovascular risk factors on mortality in type 2 diabetes: the Hoorn study. Eur. J. Clin. Invest. 32 (12), 924–930 (2002).
Natarajan, S. et al. Sex differences in the effect of diabetes duration on coronary heart disease mortality. Arch. Intern. Med. 165 (4), 430–435 (2005).
Brun, E. et al. Diabetes duration and cause-specific mortality in the Verona diabetes study. Diabetes Care. 23 (8), 1119–1123 (2000).
Wagenknecht, L. E. et al. Duration of diabetes and carotid wall thickness—the insulin resistance atherosclerosis study (IRAS). Stroke 28 (5), 999–1005 (1997).
Fox, C. S., Sullivan, L., D’Agostino, R. B. & Wilson, P. W. F. The significant effect of diabetes duration on coronary heart disease morality—the Framingham heart study. Diabetes Care. 27 (3), 704–708 (2004).
Yeap, B. B. et al. Diabetes, myocardial infarction and stroke are distinct and duration-dependent predictors of subsequent cardiovascular events and all-cause mortality in older men. J. Clin. Endocrinol. Metabolism. 100 (3), 1038–1047 (2015).
Banerjee, C. et al. Duration of diabetes and risk of ischemic stroke the Northern Manhattan study. Stroke 43 (5), 1212–1217 (2012).
Nathan, D. M. et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N. Engl. J. Med. 353 (25), 2643–2653 (2005).
Hagg, S. et al. Different risk factor profiles for ischemic and hemorrhagic stroke in type 1 diabetes mellitus. Stroke 45 (9), 2558– (2014).
Davis, T. M. E., Bruce, D. G. & Davis, W. A. Predictors of first stroke in type 1 diabetes: the fremantle diabetes study. Diabet. Med. 22 (5), 551–553 (2005).
Qaseem, A. et al. Hemoglobin A(1c) targets for glycemic control with pharmacologic therapy for nonpregnant adults with type 2 diabetes mellitus: a guidance statement update from the American college of physicians. Ann. Intern. Med. 168 (8), 569– (2018).
Inzucchi, S. E. et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach update to a position statement of the American diabetes association and the European association for the study of diabetes. Diabetes Care. 38 (1), 140–149 (2015).
Lindsey, J. B., House, J. A., Kennedy, K. F. & Marso, S. P. Diabetes duration is associated with increased thin-cap fibroatheroma detected by intravascular ultrasound with virtual histology. Circ.-Cardiovasc. Intervent.. 2 (6), 543–548 (2009).
Li, F-R. et al. Diabetes duration and glycaemic control as predictors of cardiovascular disease and mortality. Diabetes Obes. Metab. 23 (6), 1361–1370 (2021).
Yang, H-H. et al. Duration of diabetes, glycemic Control, and risk of heart failure among adults with diabetes: a cohort study. J. Clin. Endocrinol. Metab. 108 (5), 1166–1172 (2022).
Hacke, W., Kaste, M., Olsen, T. S., Orgogozo, J. M. & Bogousslavsky, J. European stroke initiative (EUSI) recommendations for stroke Management - The European stroke initiative writing committee. Eur. J. Neurol. 7 (6), 607–623 (2000).
Goldstein, L. B. et al. Guidelines for the primary prevention of stroke a guideline for healthcare professionals from the American heart association/American stroke association. Stroke 42 (2), 517–584 (2011).
Meschia, J. F. et al. Guidelines for the primary prevention of stroke a statement for healthcare professionals from the American Heart Association/American Stroke Association the American Academy of neurology affirms the value of these guidelines as an educational tool for neurologists. Stroke 45 (12), 3754– (2014).
Yates, T. et al. Association of walking Pace and handgrip strength with all-cause, cardiovascular, and cancer mortality: a UK biobank observational study. Eur. Heart J. 38 (43), 3232–3240 (2017).
Celis-Morales, C. A. et al. The association between physical activity and risk of mortality is modulated by grip strength and cardiorespiratory fitness: evidence from 498 135 UK-Biobank participants. Eur. Heart J. 38 (2), 116–122 (2017).
Collins, R. What makes UK biobank special? Lancet 379 (9822), 1173–1174 (2012).
Sudlow, C. et al. UK biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 12 (3), e1001779 (2015).
Eastwood, S. V. M. R. et al. Algorithms for the capture and adjudication of prevalent and incident diabetes in UK biobank. PLoS One. 11 (9), e0162388 (2016).
Elliott, P., Peakman, T. C. & Biobank, U. K. The UK biobank sample handling and storage protocol for the collection, processing and archiving of human blood and urine. Int. J. Epidemiol. 37 (2), 234–244 (2008).
Di Angelantonio, E. et al. Glycated hemoglobin measurement and prediction of cardiovascular disease. Jama-J. Am. Med. Assoc. 311 (12), 1225–1233 (2014).
Cosentino, F. et al. 2019 ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 41 (2), 255–323 (2020).
Li, F-R. et al. Influence of diabetes duration and glycemic control on dementia: a cohort study. J. Gerontol. A Biol. Sci. Med. Sci. 76 (11), 2062–2070 (2021).
Pazoki, R. et al. Genetic predisposition to high blood pressure and lifestyle factors associations with midlife blood pressure levels and cardiovascular events. Circulation 137 (7), 653–661 (2018).
Rannikmäe, K. N. K. et al. Accuracy of identifying incident stroke cases from linked health care data in UK biobank. Neurology 95 (6), e697–e707 (2020).
Tseng, C. H., Chong, C. K., Sheu, J. J., Wu, T. H. & Tseng, C. P. Prevalence and risk factors for stroke in type 2 diabetic patients in taiwan: a cross-sectional survey of a National sample by telephone interview. Diabet. Med. 22 (4), 477–482 (2005).
Tseng, C. H., Tseng, C. P., Chong, C. K., Sheu, J. J. & Cheng, J. C. Angiotensin-converting enzyme gene polymorphism and stroke in type 2 diabetic patients in Taiwan. Eur. J. Clin. Invest. 37 (6), 483–491 (2007).
Soedamah-Muthu, S. S. et al. Predicting major outcomes in type 1 diabetes: a model development and validation study. Diabetologia 57 (11), 2304–2314 (2014).
Stahl, C. H. et al. Glycaemic control and excess risk of ischaemic and haemorrhagic stroke in patients with type 1 diabetes: a cohort study of 33 453 patients. J. Intern. Med. 281 (3), 261–272 (2017).
Zabala, A. et al. Risk of first stroke in people with type 2 diabetes and its relation to glycaemic control: a nationwide observational study. Diabetes Obes. Metab. 22 (2), 182–190 (2020).
Mosenzon, O., Cheng, A. Y. Y., Rabinstein, A. A. & Sacco, S. Diabetes and stroke: what are the connections? J. Stroke. 25 (1), 26–38 (2023).
Rundek, T. et al. Carotid plaque, a subclinical precursor of vascular events—the Northern Manhattan study. Neurology 70 (14), 1200–1207 (2008).
Orchard, T. J. et al. Prevalence of complications in IDDM by sex and duration. Pittsburgh epidemiology of diabetes complications study II. Diabetes 39 (9), 1116–1124 (1990).
Tuomilehto, J. et al. Incidence of cardiovascular disease in type 1 (insulin-dependent) diabetic subjects with and without diabetic nephropathy in Finland. Diabetologia 41 (7), 784–790 (1998).
Guerrero-Romero, F. & Rodriguez-Moran, M. Proteinuria is an independent risk factor for ischemic stroke in non-insulin-dependent diabetes mellitus. Stroke 30 (9), 1787–1791 (1999).
Koopman, R. J., Mainous, A. G., Diaz, V. A. & Geesey, M. E. Changes in age at diagnosis of type 2 diabetes mellitus in the United States, 1988 to 2000. Ann. Fam. Med. 3 (1), 60–69 (2005).
Booth, G. L., Kapral, M. K., Fung, K. & Tu, J. V. Recent trends in cardiovascular complications among men and women with and without diabetes. Diabetes Care. 29 (1), 32–37 (2006).
Harris, M. I., Klein, R., Welborn, T. A. & Knuiman, M. W. Onset of NIDDM occurs at least 4–7 year before clinical diagnosis. Diabetes Care. 15 (7), 815–819 (1992).
Acknowledgements
The authors acknowledge the participants and staff of the UK Biobank for their dedication and contribution to the research. This research has been conducted using the UK Biobank Resource under application number 55794.
Funding
Xiang Gao is supported by grants from the Fundamental Research Funds for the Central Universities (YG2025QNB01), the National Natural Science Foundation of China (72004032) and Startup Fund for Young Faculty at Shanghai Jiao Tong University (Grant Number: KJ3-0221-22-6333). Fu-Rong Li is supported by grants from Science, Technology and Innovation Commission of Shenzhen Municipality (ZDSYS20200810171403013).
Author information
Authors and Affiliations
Contributions
Xiang Gao and Fu-Rong Li wrote the manuscript and researched data. Guo-Chong Chen, Xu Wang and Li-Qiang Qin reviewed and edited the manuscript. Huan-Huan Yang, Fei Xie and Hai-Peng Wang contributed to the discussion and reviewed the manuscript. Li-Hua Chen and Zheng-Bao Zhu researched data and contributed to discussion.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
The study was approved by the National Health Service (NHS) National Research Ethics Service (REC reference: 11/NW/03820) and all participants provided written informed consent to participate in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gao, X., Yang, HH., Xie, F. et al. Diabetes duration, glycemic control, and risk of stroke and stroke subtypes: a nationwide prospective cohort study. Sci Rep 15, 43633 (2025). https://doi.org/10.1038/s41598-025-27547-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27547-z
