
Abstract
Attention-Deficit/Hyperactivity Disorder (ADHD) and Developmental Coordination Disorder (DCD) are two prevalent neurodevelopmental disorders among children. Both of these diseases, occurring independently or in combination, can result in significant motor skill deficits. The purpose of this study was to observe the improvement in motor performance and skill acquisition of children with ADHD + DCD in comparison with their peers with ADHD or DCD, through repeated practice in the MTSI game. A total of 139 children (37 ADHD, 33 ADHD + DCD, 34 DCD, 35 TD: Typically Developing) participated in the MTSI (Multi-task Sensorimotor Intervention), which involved five sensorimotor intervention tasks. The change of motor performance scores provided by the MTSI system was assessed with repeated measurements, and the skill acquisition in gross & fine motor skills before and after intervention was analyzed with a mixed-design repeated measures ANOVA with post hoc analysis. All groups of children demonstrated a significant increase in motor performance during repeated practice in MTSI and displayed great improvements in gross and fine motor skills, with ADHD + DCD children benefiting more in the magnitude. Multi-task sensorimotor intervention (MTSI) can effectively improve gross and fine motor skills for children with ADHD or DCD, and particularly for those with ADHD and DCD comorbidity, with tailored, multidimensional intervention strategies.
Similar content being viewed by others

Introduction
Neurodevelopmental disorders (NDDs) affect millions of children worldwide, typically manifesting early in life and encompassing a broad spectrum of symptoms across multiple functional domains1. Different types of NDD have their unique clinical features, but sometimes, they often occur in combination and result in more serious or complex problems in motor development, presenting a great challenge for family caretaking and clinical treatment2. Attention-deficit/hyperactivity disorder (ADHD) and developmental coordination disorder (DCD) are two of the most common neurodevelopmental disorders, which affect approximately 7% and 6% of school-age children, respectively3,4. Children with ADHD or DCD both face higher risks of anxiety, depression, academic underachievement, and social psychological issues5, but they displayed different features in motor performance. ADHD is mainly characterized by inattention, hyperactivity, and impulsivity, while DCD primarily manifests as clumsiness and poor coordination6.
Notably, the comorbidity rate of ADHD and DCD reaches up to 50%3,4 as they have highly relevant pathogenesis as neurological impairment7,89. The motor difficulties of children with comorbid ADHD and DCD are often neglected or underrecognized since the clinical examination may be terminated once the main problem is identified. Usually, the behavioral problems, including attention deficits and behavioral regulation issues caused by ADHD, receive more attention and are often prioritized in assessment, thereby overshadowing the manifestations of motor problems in DCD10. Moreover, some children with ADHD may develop avoidance strategies, such as refusing to participate in exercises or sports, which are mistaken as a preference for the issue of interest rather than motor ability11,12. Abnormal sensory information processing and disordered sensorimotor coupling are two important factors that affect motor performance in children with both DCD and ADHD, although the influencing pathways and symptom manifestations are different13. Gillberg et al. introduced the concept of “Attention, Motor Control, and Perceptual Deficits” (DAMP), which described the symptom overlap between ADHD and DCD, highlighting the intrinsic connection between sensory integration dysfunction and motor difficulties in these children14. Furthermore, two studies enlightened that ADHD and DCD share high comorbidity with other NDDs involving impairments in sensory processing15,16.
Compared to those with only one of the disorders, children with comorbid ADHD and DCD perform worse and face more significant challenges in action execution, because of the combination or overlap of the attention deficit and incoordinated movements. The comorbidity predisposes this group of children to be at the risk of slow information processing, inaccurate sensory integration, and ineffective motor skill learning & control, as well as a lower level of gross and fine motor skills17,18. Although pharmacological treatments19 and cognitive training20 have a good therapeutic effect on motor behavior regulations in children with ADHD, they may still leave their motor difficulty unimproved, as they focus mainly on attention deficits rather than movement coordination problems. In recent decades, balance training, ball manipulation, and rhythmic movements, as the methods of Kinesitherapy, have been widely used in the field of treatment of NDDs, and they have been evidenced to be effective in improving the problems of motor ability and coordination, not only for DCD21, but also for ADHD22, and even for DCD + ADHD23. Actually, exercise-based interventions could be broadly classified into two categories: process-oriented interventions that help cure motor defects and shape standardized movements, and task-oriented interventions, which may increase movement function through goal-driven enhancement of task engagement24,25. Comparatively, task-oriented interventions were recommended by the International Clinical Practice Guidelines for DCD as the first-choice intervention for children with DCD26, based on its superiority over the process-oriented25,27.
Virtual reality (VR), as a method of modern technology, has increasingly been applied in neuro-rehabilitation, and a growing body of research supports the use of VR in the treatment of motor deficiency for children with ADHD and/or DCD28,29. For example, Schena et al. (2021) conducted a 6-month VR gaming intervention in children with ADHD and reported significant improvements in hyperactivity symptoms, conflict behavior, and executive function30. Jelsma et al. (2014) conducted a 6-week Wii Fit intervention for children with DCD and found improvements in their motor performance, especially in dynamic balance31. And further, some active video games (AVGs) with task-oriented intervention have been certified to be positive in enhancing sensorimotor function for children, and improving movement abilities in motor learning28,2930.
Thus, this study designed a task-oriented enhanced multi-sensorimotor intervention system (MTSI) based on VR, and investigated its effects on motor performance and skill acquisition in children with ADHD, DCD, and ADHD + DCD. This study hypothesized that children with ADHD, DCD, and ADHD + DCD children could all adapt to the intervention tasks and improve their motor performance during repeated practice in MTSI, as their TD peers, and resultantly, their gross and fine motor skills would also be improved. And further, children with ADHD + DCD were expected to get the most substantial gains in benefit. Hopefully, this study will provide new evidence and intervention strategies for motor intervention in children with ADHD or DCD, and particularly for those with ADHD + DCD.
Methods
Participants
137 participants were recruited from two special education schools and one normal elementary school in the city of Shijiazhuang, Hebei Province, China. They were classified into four groups, including ADHD, DCD, ADHD + DCD, and TD groups, with 37, 34, 33, and 35 children, respectively. The ratio of the participants by sex was determined by the natural characteristics of the real-world clinical demographics, which consists of the higher clinical prevalence of ADHD or DCD in males32,33.
Inclusion criteria were as follows: (1) Children aged 6–8 years. (2) ADHD was diagnosed by using the Conners Rating Scale and the Vanderbilt ADHD Diagnostic Parent Rating Scale. (3) DCD was diagnosed with the Developmental Coordination Disorder Questionnaire (DCDQ) completed by parents and performance on the Movement Assessment Battery for Children – Second Edition (MABC-2), with ADHD symptoms excluded using the Conners Rating Scale to rule out comorbidity. (4) Full-scale IQ ≥ 70. (5) No use of medication in the past 3 months, or a stable dose maintained; (6) Children in the ADHD + DCD group met all above criteria (1–5). (7) ADHD + DCD comorbidity was confirmed by two experienced pediatric neurologists through structured interviews and neurological examinations, following the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria.
Exclusion criteria included: (1) comorbid diagnoses of autism spectrum disorder, intellectual disability, or other neurodevelopmental conditions. (2) the presence of cerebral palsy, epilepsy, or other severe neurological or organic motor disorders. (3) severe psychiatric disorders, such as schizophrenia. (4) significant sensory impairments, including visual or auditory deficits that would prevent cooperation with VR-based tasks. (5) participating in other motor intervention programs. (6) using psychiatric or neurological medications, other than stable doses of ADHD treatment drugs. The research team contacted 171 families, of which 139 consented to participate, and 32 refused for lack of interest, academic workload, or long travel distances. Among the enrolled participants, only 7 children were taking ADHD medications (all short-acting stimulants), and their parents were instructed to suspend the use of medication 48 h before each assessment. Demographic characteristics of participants across groups are presented in Table 1.
The study protocol and intervention design were approved by the Medical Ethics Committee of Hebei Normal University (Approval No. 2023LLSC015) and conducted according to the Declaration of Helsinki. Written informed consent was obtained from the legal guardians of all participants, and assent was also provided by the children. And they were informed of their right to withdraw from the study at any time without any negative consequences.
MTSI design
This study utilized a custom-designed Multi-Task Sensorimotor Intervention (MTSI) system, which enabled skeletal tracking and motion recognition by integrating Kinect motion sensing technology with an RGB camera and a depth sensor to simultaneously capture color and depth information34. The MTSI system comprises two core modules: (1) the Motion Task Module, (2) the Data Processing Module. The Motion Task Module was designed based on the theoretical foundations of the DAMP model (Deficits in Attention, Motor control, and Perception) and expert consultation. It includes five sensorimotor tasks targeting multi-sensory integration and progressive training not only for gross but also for fine motor skills. The MTSI system included five interactive tasks, including Tennis Ball Hitting (Task 1), Obstacle Run (Task 2), Rapid Reaction (Task 3), Obstacle Skiing (Task 4), and Human-shaped Wall Traversal (Task 5). Task difficulty was incrementally adjusted every 4 weeks through backend-controlled parameters, such as the presenting frequency and movement speed of the obstacle, time constraints, and action complexity, like multi-step actions. The Data Processing Module gives scores automatically and provides real-time feedback on movement accuracy. Each successful action will be awarded with 1 point (e.g., passing one obstacle); incomplete or incorrect actions will get no points, i.e., 0 points. Cumulative scores were displayed in real time, and total scores were automatically recorded and stored by the system after each session. See Table 2.
Before this research, the system validation of the MTSI was tested and verified with a cohort of studies on 24 ADHD + DCD children, 25 DCD children, and 25 TD children. Internal consistency was assessed using Cronbach’s alpha and Intraclass Correlation Coefficient (ICC) based on 12 repeated practice scores of the DCD group. Content validity was evaluated through expert interviews, yielding a high Content Validity Index (CVI > 0.90). Calibration validity was tested by comparing task scores between the DCD and TD groups by using independent-samples t-tests and Levene’s test, confirming homogeneity of variance (p > 0.05) and significant between-group differences (p < 0.05). Pearson correlation analyses between task scores (1st and 12th sessions) and MABC-2 sub-test scores confirmed moderate-to-strong associations, which support concurrent validity. In terms of reliability, practice scores significantly improved across all tasks for children with ADHD + DCD (p < 0.05, η² > 0.14), with high internal consistency (Cronbach’s α > 0.80, ICC > 0.60).
Practice intervention
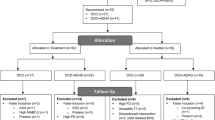
The intervention was conducted at community centers or schools to ensure convenient accessibility and engagement for the participants. The duration of the intervention lasted 12 weeks, and it was divided into three stages, with four weeks for each. Each trial lasted 35 min, and there were a total of 12 trials for each stage, with three trials scheduled for each week. The time duration and practice frequency were arranged based on age-appropriate attention spans for children aged 6 to 8 years, which were supported by validated parameters from similar pediatric exercise intervention studies35. A fixed session duration was employed to minimize confounding effects related to differences in intervention dosage. At the end of each phase, the task difficulty would be adjusted if the participants achieved an average completion rate of ≥ 80% for the task, and still maintained a safe heart rate (120 and 150 bpm), which was monitored by a Xiaomi REDMI Kids Watch (Xiaomi Corporation, Beijing, China) worn on the wrist To ensure task familiarity, two practice sessions were given before the formal intervention. The entire program was supervised by a team of rehabilitation therapists and trained research staff. During the period of intervention, participants were instructed to maintain their usual routines and were asked to refrain from any engagement in extracurricular sports activities. All the participants completed the full protocol of the 12-week intervention program except for one participant who withdrew from the ADHD group, and another from the TD group. The overall study flow is illustrated in Fig. 1.

Flow diagram outlining participant recruitment, grouping, experimental design, exercise intervention, and data collection and processing.
Measures of gross and fine motor skills
Gross and fine motor skills were assessed immediately before and after the intervention. Gross motor skills were evaluated by using the Test of Gross Motor Development, Third Edition (TGMD-3) in two domains of locomotor skills (e.g., running, hopping, side-sliding) and ball skills (e.g., overhand throwing, kicking, dribbling, two-hand catching). Scores were recorded as raw scores and standardized scores (based on Chinese normative data), with higher scores indicating better performance. Fine motor skills were assessed by using the Movement Assessment Battery for Children, Second Edition (MABC-2), which consists of three components of manual dexterity (e.g., coin posting, threading beads), aiming and catching (ball catching and throwing), and static & dynamic balance. In the present study, the participants aged 6 and 7 years were assessed with the evaluation sessions for 3ཞ6 and 7ཞ10 years old children, respectively. Standardized scores for each item were compared with Chinese normative data to ensure validity.
Statistical methods
All data were analyzed with IBM SPSS Statistics 27.0 (IBM Corp., Chicago, IL). Descriptive statistics (mean ± standard deviation) were calculated for all variables; the Shapiro–Wilk test and Levene’s test were used for the assessment of the normality and homogeneity of all the continuous variables, respectively (both p > 0.05). A Repeated Measures ANOVA was conducted to evaluate the changes in the motor performance scores across each phase of the interventions for each skill. A 2 (Time: pre-test vs. post-test) × 4 (Group: ADHD, DCD, ADHD + DCD, TD) Mixed-design Repeated Measures ANOVA was employed to examine the main effect of time and group and their interaction on gross and fine motor skills, and post hoc comparison was performed with the Bonferroni test to explore the between-group differences if necessary. Significance levels were set at p < 0.05, with p < 0.01 considered highly significant.
Results
Sample characteristics
There is no significant difference in the demographic characteristics, such as age, gender, body height, and weight (p > 0.05), but there are significant between-group differences at the baseline of the total scores of TGMD-3 and MABC-2 (p < 0.05). See Table 2.
Game-based outcomes
ADHD (p < 0.001, η² = 0.73–0.91), ADHD + DCD (p < 0.001, η² = 0.72–0.95), DCD (p < 0.001, η² = 0.68–0.91), and TD (p < 0.001, η² = 0.28–0.90) groups all demonstrated significant improvements in motor performance across the three intervention phases. However, the three groups of ADHD, ADHD + DCD, and DCD showed lower scores compared to the TD group. ADHD + DCD and ADHD groups exhibited higher gain but obviouly greater intra-group variability compared to the DCD group, and the DCD group demonstrated a slower and more gradual improvement in learning curves. See Table 3; Fig. 2.
Standardized test outcomes
There was a significant interactive effect of time and group on the total scores of gross motor skills, including locomotion and ball skills, and fine motor skills. In more detail, the significant improvements are manifested in all the movements except for the items of run, underhand throw, and one-hand forehand strike. Besides this interaction, both group and time have a notable influence on all the motor skill measures, separately (all p < 0.001). Further observation on effect size (η² and Cohen’d) revealed that the movements of slide, catch, and most of the fine motor skills, such as manual dexterity and balance, benefited more than others from the MTSI practice.

The change of scores in each stage of intervention among ADHD+DCD, ADHD, DCD, and TD groups. Fig. a: Task 1 performance across groups. Fig. b: Task 2 performance across groups. Fig. c: Task 3 performance across groups. Fig. d: Task 4 performance across groups. Fig. e: Task 5 performance across groups.
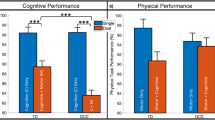
In benefit magnitude, the ADHD + DCD group made the largest progress among the three clinical groups, followed by the DCD and ADHD group in all the overall abilities and most of their sub-categories. According to the post hoc analysis, the children in the ADHD + DCD group showed better performance than those in the DCD group in all the tested fine motor skills and the gross motor skills of gallop, skip, hop, catch, ball strikes and underhand throw, and outperformed ADHD group only in aiming and catching, and balance after intervention. ADHD vs. DCD comparison revealed no significant differences in all the motor skills. In addition, compared with the TD group, the ADHD, DCD, and ADHD + DCD groups all demonstrated lower levels of abilities in all the tested motor skills, not only in pre- but also in post-test. However, it could be seen from the effect size (Cohen’d) that they all showed relatively larger improvements in the total scores of gross motor skills, locomotion skills, and ball skills, as well as fine motor skills. See Table 4.
Discussion
The primary objective of this study was to assess the effect of a Virtual Reality (VR)-based, multitasking sensorimotor intervention (MTSI) on motor skill acquisition in children diagnosed with Attention-Deficit/Hyperactivity Disorder (ADHD), Developmental Coordination Disorder (DCD), and ADHD + DCD comorbidity. The findings of this study agree with our hypotheses that MTSI may not only improve motor performance for children with ADHD or DCD, but also for those with ADHD + DCD, by goal-targeted repeated practice. Furthermore, as expected, the enhancement of motor abilities can result in the promotion of the development of their motor skills, especially for the fine motor skills and some of the gross motor skills, such as sliding and catching. And more importantly, all three clinical groups made a greater improvement than the TD group, and the ADHD + DCD group had the greatest benefit, followed by the DCD and ADHD group in sequence, in most of the fine motor skills and all the gross motor skills, especially in slide and catch.
These findings underscore the potential of virtual reality (VR)-based multisensory feedback systems to enhance motor abilities and skill acquisition in children with neurodevelopmental disorders. In the mechanism, the clinical intervention effects of the MTSI may be attributed to the task-oriented intervention with repeated practice assignment, immediate feedback, and ecological simulation of daily scenarios, etc. Firstly, the MTSI system is designed potentially to improve the children’s attention concentration and increase their motivation and engagement since it could influence reward-related circuits by real-time feedback in an interactive and gamified environment39. A systematic review proposed that instant or concurrent feedback via technology would be popular due to its ability to provide enhanced multisensory feedback46. Secondly, VR is designed with the purpose of integrating different types of sensory information, including visual, auditory, and proprioceptive signals, and further facilitating sensorimotor coupling40. Thirdly, the MTSI games combine several state-of-the-art evidence-based strategies, including high dosage, active learning, and environmental enrichment, as proposed by a study protocol about early therapeutic intervention on infants at risk of neuro-motor delay41. In this study, greater improvements in gross and fine motor skills were observed in all three clinical groups compared to the TD group. One reason is that children with sensorimotor deficits may gain more from the interventions targeting both attentional and perceptual–motor pathways simultaneously. The other may be related to the “ceiling effect” that leaves limited room for further improvement for TD children.
ADHD + DCD children exhibited the greatest improvements in both fine and gross motor skills in the three clinical groups. These findings can be explained on two levels. From a clinical phenotype perspective, ADHD + DCD children present with both attention regulation deficits and sensory–motor integration impairments, leading to the lowest baseline performance and thus the largest potential for improvement42. In terms of intervention mechanism, the tasks of MTSI may realize the dual-pathway activation of attention & motivation engagement and sensorimotor correction. One is the motivation-attentional pathway associated with ADHD’s attention deficits. It was considered to be associated with arousal levels and excitation-inhibition control within the frontostriatal circuit for motor skill acquisition, by using the mesolimbic dopamine reward system, which is highly sensitive to immediate feedback43. The other is the sensory-motor pathway linked to DCD’s motor coordination impairments. Because multisensory feedback could compensate for their deficits in constructing internal motor models for predictive control of movement44, and the virtual reality could strengthen the formation of sensory-motor mapping by triggering the use of the mirror neuron system and inducing the participation of the action observation network45. However, the interplay between ADHD related deficits in attention and DCD’s core impairment in sensorimotor integration46 may render ADHD + DCD comorbid children prone to have short-term intense drive in the gamified, high-motivation tasks, so they were struggling to maintain consistent output due to the ADHD’s compromised ability to regulate cognitive resources47. The mechanisms could also be manifested by the “high-gain yet unstable” trajectory of learning curves in ADHD + DCD children during the MTSI practice. In contrast, both ADHD and DCD children showed lower beneficial gain in motor skills. Children with ADHD alone often show relatively preserved performance in gross motor skills, but the deficits in attention would negatively affect their continuous motor learning47, which could also be seen from the unstable line for motor learning within MTSI. DCD children, although improving steadily, remain limited by deficits in feed-forward prediction48 and internal motor modeling49, which might slow their error-based adaptation50, although the enriched visual-proprioceptive cues likely enable progressive error reduction and postural recalibration21. That’s also why DCD exhibited a “steady but slow” learning curve in practice.
Sliding and catching showed marked improvements in all three clinical groups of children. It may be due to the close match between task demands and neurofunctional deficits. Sliding is a locomotor skill with more requirements of dynamic postural control than forward rhythmic movements like walking and running, so it gives more pressure on visuospatial perception, proprioceptive integration, and cerebellar-cortical circuits51. Coincidentally, similar to most of the traditional VR games, all five tasks in this MTSI need participants to control posture and adjust movement only in the frontal plane, i.e., move up and down, or left and right. Catching is a ball skill that relies more on visual tracking, timing prediction, and visuomotor coordination52. In the MTSI, Task 1 of tennis ball hitting is a typical movement of object manipulation, and all the other four tasks also require participants to deal with flying objects or approaching environments ahead. Besides that, all the movements of the tasks need higher demand of attention on postural control. And further, a structured gross motor training could also lead to parallel improvement in their fine motor abilities and produce moderate positive effects on fine motor skills, like visuomotor and manual dexterity, for children. Therefore, aiming and catching, balance, and manual dexterity, as the three main categories of fine motor skills measured in M-ABC, all greatly improved during MTSI exercise.
Taken together, this study enlightened that a VR-based multi-task sensorimotor intervention (MTSI) may offer benefits for children with ADHD or DCD, and particularly for those with ADHD + DCD comorbidity, and underscores the need for tailored, multidimensional intervention strategies in neurodevelopmental disorders.
Limitations and future work
Although this study systematically evaluated the process and outcomes of long-term motor skill learning in children with Attention-Deficit/Hyperactivity Disorder (ADHD), Developmental Coordination Disorder (DCD), and their comorbidity, several limitations should be acknowledged. One is the limited number of participants; future research needs to expand the sample size to cover a broader range of population diversity to enhance the generalization of the results, and even to make subtype classifications. The other is that this study lacks long-term practice follow-up of the intervention and retention/transfer test; future studies are recommended to explore the long-term effects of Multitask Sensorimotor Intervention (MTSI) and observe the retention and transfer effect over an extended period. Thirdly, this is a kinematic study focusing on the children’s behavior, not including direct measures of attention engagement and brain activity. Future trials should include eye-tracking, pupillometry, event-related EEG, or functional Magnetic Resonance Imaging (fMRI) as planned objective measures in follow-up work. In addition, the two-dimensional virtual reality technology is also a limitation; an upgraded three-dimensional design will be more effective to enhance environmental immersion and ecological validity, and give full-dimensional intervention stimulation, including forward and diagonal movements.
Conclusion
The task-oriented Multi-task sensorimotor intervention (MTSI) can effectively increase motor ability with repeated practice, and improve the gross and fine motor skills for children with ADHD or DCD, and particularly for those with ADHD and DCD comorbidity.
Data availability
All data supporting the findings of this study are available at https://doi.org/10.57760/sciencedb.29768.
Abbreviations
- ADHD:
-
Attention-Deficit Hyperactivity Disorder
- DCD:
-
Developmental Coordination Disorder
- TD:
-
Typically Developing
- MTSI:
-
Multi-task Sensorimotor Intervention
- VR:
-
Virtual Reality
- AVG:
-
Active Video Game
- MABC-2:
-
Movement Assessment Battery for Children – Second Edition
- TGMD-3:
-
Test of Gross Motor Development – Third Edition
- fMRI:
-
Functional Magnetic Resonance Imaging
- EEG:
-
Electroencephalography
- Motor Skill:
-
A learned ability to cause predetermined movement outcomes with accuracy and efficiency
- Motor Learning:
-
The process of acquiring and refining motor skills through practice is often reflected in long-term retention and transfer to new tasks
- Motor Performance:
-
The observable execution of a motor task at a given moment, which may fluctuate due to attention, fatigue, or motivation
- Sensory Integration:
-
The neurological process of organizing input from multiple sensory modalities (e.g., visual, auditory, proprioceptive) to produce coherent motor output
- Sensorimotor Coupling Function:
-
The coordination between sensory inputs and motor commands allows real-time adjustment and control of movement
- Task-Oriented Training:
-
An intervention strategy that uses meaningful, goal-directed activities to improve functional skills in real-life contexts
- Executive Function:
-
A set of cognitive processes (e.g., attention, planning, inhibition) is involved in goal-directed behaviors and is essential to motor control
- Multimodal Feedback:
-
The simultaneous provision of information through different sensory channels (e.g., visual + auditory) to support learning
References
Thapar, A., Cooper, M. & Rutter, M. Neurodevelopmental disorders. The lancet. Psychiatry 4 (4), 339–346 (2017).
First, M. B. Diagnostic and statistical manual of mental disorders, 5th edition, and clinical utility. The Journal of nervous and mental disease 201 (9), 727–729 (2013).
Sayal, K., Prasad, V., Daley, D., Ford, T. & Coghill, D. ADHD in children and young people: prevalence, care pathways, and service provision. Lancet Psychiatry. 5 (2), 175–186 (2018). (2018).
Zwicker, J. G., Missiuna, C., Harris, S. R. & Boyd, L. A. Developmental coordination disorder: a review and update. Eur. J. Pediatr. Neurology: EJPN : Official J. Eur. Pediatr. Neurol. Soc. 16 (6), 573–581 (2012).
Biotteau, M. et al. Developmental coordination disorder and dysgraphia: signs and symptoms, diagnosis, and rehabilitation. Neuropsychiatr. Dis. Treat. 15, 1873–1885 (2019).
World Health Organization. International statistical classification of diseases and related health problems (11th ed.). (2019).
Shephard, E. et al. Shepard and Zuccolo are co-first authors of this work. Systematic review and Meta-analysis: the science of Early-Life precursors and interventions for Attention-Deficit/Hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry. 61 (2), 187–226 (2022).
Lee, J. et al. The relationship between motor milestone achievement and childhood motor deficits in children with attention deficit hyperactivity disorder (ADHD) and children with developmental coordination disorder. Res. Dev. Disabil. 113, 103920 (2021).
Blank, R., Smits-Engelsman, B., Polatajko, H. & Wilson, P. European academy for childhood disability. European academy for childhood disability (EACD): recommendations on the definition, diagnosis and intervention of developmental coordination disorder (long version). Dev. Med. Child Neurol. 54 (1), 54–93 (2012).
Sergeant, J. A., Piek, J. P. & Oosterlaan, J. ADHD and DCD: a relationship in need of research. Hum. Mov. Sci. 25 (1), 76–89 (2006).
Kleeren, L. et al. A critical view on motor-based interventions to improve motor skill performance in children with ADHD: A systematic review and Meta-analysis. J. Atten. Disord. 27 (4), 354–367 (2023).
Athanasiadou, A. et al. Early motor signs of attention-deficit hyperactivity disorder: a systematic review. Eur. Child Adolesc. Psychiatry. 29 (7), 903–916 (2020).
Kofler, M. J. et al. Executive function deficits in attention-deficit/hyperactivity disorder and autism spectrum disorder. Nat. Rev. Psychol. 3, 701–719 (2024).
Gillberg, C. Deficits in attention, motor control, and perception: a brief review. Arch. Dis. Child. 88 (10), 904–910 (2003).
Tervo, R. C., Azuma, S., Fogas, B. & Fiechtner, H. Children with ADHD and motor dysfunction compared with children with ADHD only. Dev. Med. Child Neurol. 44 (6), 383–390 (2002).
Licari, M., Larkin, D. & Miyahara, M. The influence of developmental coordination disorder and attention deficits on associated movements in children. Hum. Mov. Sci. 25 (1), 90–99 (2006).
Alloway, T. P., Rajendran, G. & Archibald, L. M.Working memory in children with developmental disorders. J. Learn. Disabil. 42 (4), 372–382 (2009).
Alloway, T. P. & Temple, K. J. A comparison of working memory skills and learning in children with developmental coordination disorder and moderate learning difficulties. Appl. Cogn. Psychol. 21 (4), 473–487 (2007).
Kaiser, M. L., Schoemaker, M. M., Albaret, J. M. & Geuze, R. H. What is the evidence of impaired motor skills and motor control among children with attention deficit hyperactivity disorder (ADHD)? Systematic review of the literature. Res. Dev. Disabil. 36, 338–357 (2015).
Wilson, A. C. Cognitive profile in autism and ADHD: A Meta-Analysis of performance on the WAIS-IV and WISC-V. Archives of clinical neuropsychology: the. Official J. Natl. Acad. Neuropsychologists. 39 (4), 498–515 (2024).
Smits-Engelsman, B. et al. Evaluating the evidence for motor-based interventions in developmental coordination disorder: A systematic review and meta-analysis. Res. Dev. Disabil. 74, 72–102 (2018).
Kanevski, M., Booth, J. N., Stewart, T. M. & Rhodes, S. M. Cognition and maths in children with Attention-Deficit/Hyperactivity disorder with and without co-occurring movement difficulties. Res. Dev. Disabil. 136, 104471 (2023).
Pranjić, M. et al. A systematic review of behavioral and Neurobiological profiles associated with coexisting attention-deficit/hyperactivity disorder and developmental coordination disorder. Neurosci. Biobehav. Rev. 153, 105389 (2023).
Straker, L. et al. A crossover randomised and controlled trial of the impact of active video games on motor coordination and perceptions of physical ability in children at risk of developmental coordination disorder. Hum. Mov. Sci. 42, 146–160 (2015).
Miyahara, M., Lagisz, M., Nakagawa, S. & Henderson S intervention for children with developmental coordination disorder: how robust is our recent evidence? Child Care Health Dev. 46 (4), 397–406 (2020).
Blank, R. et al. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev. Med. Child Neurol. 61 (3), 242–285 (2019).
Blank, R. & European Academy of Childhood Disability (EACD). Recommendations on the definition, diagnosis and intervention of developmental coordination disorder (pocket version). German-Swiss interdisciplinary clinical practice guideline S3-standard according to the association of the scientific medical societies in Germany. Pocket version. Definition, diagnosis, assessment, and intervention of developmental coordination disorder (DCD). Dev. Med. Child Neurol. 54 (11), e1–e7 (2012).
Yu, C., Wang, C., Xie, Q. & Wang, C. Effect of virtual reality technology on attention and motor ability in children with attention-Deficit/Hyperactivity disorder: systematic review and Meta-Analysis. JMIR Serious Games. 12, e56918 (2024).
Bioulac, S. et al. Qu’apportent les outils de réalité Virtuelle En psychiatrie de l’enfant et l’adolescent ? [What do virtual reality tools bring to child and adolescent psychiatry?]. L’Encephale 44 (3), 280–285 (2018).
Schena, A. et al. Preliminary findings of an experimental study to evaluate the statistical significance of an intervention for ADHD conducted through the use of serious games in virtual reality. Int. J. Environ. Res. Public Health. 20 (4), 3414 (2023).
Jelsma, D., Geuze, R. H., Mombarg, R. & Smits-Engelsman, B. C. The impact of Wii fit intervention on dynamic balance control in children with probable developmental coordination disorder and balance problems. Hum. Mov. Sci. 33, 404–418 (2014).
Mowlem, F. D. et al. Sex differences in predicting ADHD clinical diagnosis and Pharmacological treatment. Eur. Child Adolesc. Psychiatry. 28 (4), 481–489 (2019).
Slobodin, O. & Davidovitch, M. Gender differences in objective and subjective measures of ADHD among Clinic-Referred children. Front. Hum. Neurosci. 13, 441 (2019).
Xu, M., Zhai, Y., Guo, Y. et al. Personalized training through Kinect-based games for physical educaiton. J. Vis. Commun. Image. Represent. 62, 394-401(2019)
Petancevski, E. L. et al. The Effect of Augmented Feedback on the Performance and Learning of Gross Motor and sport-specific Skills: A Systematic review[J] (Psychology of Sport and Exercise, 2022).
Glaziera, P. S., Davids, K. & Bartlett, R. M. Dynamical systems theory: A relevant framework for performance-oriented sports biomechanics research. Sportscience 7, 8 (2003).
Ossmy, O. & Mukamel, R. Perception as a route for motor skill learning: perspectives from neuroscience. Neuroscience 382, 144–153 (2018).
Ducrocq, E., Wilson, M., Vine, S. & Derakshan, N. Training attentional control improves cognitive and motor task performance. J. Sport Exerc. Psychol. 38 (5), 521–533 (2016).
Ali, S. G. et al. B. A systematic review: Virtual-reality-based techniques for human exercises and health improvement. Front. public. Health. 11, 1143947 (2023).
Butler, A. J., James, T. W. & James, K. H. Enhanced multisensory integration and motor reactivation after active motor learning of audiovisual associations. J. Cogn. Neurosci. 23 (11), 3515–3528 (2011).
Deng, W. et al. Protocol for a randomized controlled trial to evaluate a year-long (NICU-to-home) evidence-based, high dose physical therapy intervention in infants at risk of neuromotor delay. PloS One. 18 (9), e0291408 (2023).
Fliers, E. et al. ADHD and poor motor performance from a family genetic perspective. J. Am. Acad. Child Adolesc. Psychiatry. 48 (1), 25–34 (2009).
Dutta, C. N., Christov-Moore, L., Ombao, H. & Douglas, P. K. Neuroprotection in late life attention-deficit/hyperactivity disorder: A review of pharmacotherapy and phenotype across the lifespan. Front. Hum. Neurosci. 16, 938501 (2022).
Wilson, P. H., Ruddock, S., Smits-Engelsman, B., Polatajko, H. & Blank, R. Understanding performance deficits in developmental coordination disorder: a meta-analysis of recent research. Dev. Med. Child Neurol. 55 (3), 217–228 (2013).
Rizzolatti, G. & Sinigaglia, C. The functional role of the parieto-frontal mirror circuit: interpretations and misinterpretations. Nat. Rev. Neurosci. 11 (4), 264–274 (2010).
Xu, S., Li, C. & Duan, Y. Action observation and mirror neuron activation in VR-mediated rehabilitation. NeuroRehabilitation 49 (2), 155–165 (2021).
Antshel, K. M. & Russo, N. Executive functioning in children with ADHD. Child Adolesc. Psychiatr. Clin. N. Am. 28 (3), 393–410 (2019).
Adams, I. L., Lust, J. M., Wilson, P. H. & Steenbergen, B. Compromised motor control in children with DCD: a deficit in the internal model?—A systematic review. Neurosci. Biobehav. Rev. 47, 225–244 (2014).
Zwicker, J. G., Missiuna, C., Harris, S. R. & Boyd, L. A. Brain activation associated with motor skill practice in children with developmental coordination disorder: an fMRI study. Int. J. Dev. Neuroscience: Official J. Int. Soc. Dev. Neurosci. 29 (2), 145–152 (2011).
Kagerer, F. A., Bo, J., Contreras-Vidal, J. L. & Clark, J. E. Visuomotor adaptation in children with developmental coordination disorder. Mot. Control. 8 (4), 450–460 (2004).
Gowen, E. & Miall, R. C. The cerebellum and motor dysfunction in neuropsychiatric disorders. Cerebellum 6 (3), 268–279 (2007).
Cameron, C. E., Brocki, K. C. & Zelazo, P. D. Visuomotor control and executive function: A developmental perspective. Dev. Psychol. 48 (1), 56–68 (2012).
Acknowledgements
We sincerely thank all the participants and their parents for their invaluable contributions to this study. Special thanks are due to the leaders and teachers at the Education Bureau of Qiaoxi District in Shijiazhuang, the Special Education School, and Zhonglu Primary School in Shijiazhuang, for their support in participant recruitment and throughout the course of the experiment.
Funding
This study was supported by the National Key Research and Development Program of the Ministry of Health and Family Planning, China [grant numbers No. 2024YFC2707903], the National Social Science Fund of China [grant numbers No. 19BTY045], and the Hebei Province Overseas Returnee Talent Program [grant numbers No. C2023034].
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collectioiand analysis were performed by H.L., L.Z., Y.Z., and J.W. were responsible for recruiting and data collection. T.W., Y.G. were responsible for patient selection. C.J., K.L., K.W., Y.Z., and Y.Z. contributed advice during the study in their specific fields. The first draft ofthemanuscript was written by Z.L. and all authors commented on previousversions ofthemanuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was conducted by the principles of the Declaration of Helsinki. Ethical approval was granted by the Ethics Committee of Hebei Normal University (Approval No. 2023LLSC015).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cai, Y., Li, Z., Liu, H. et al. The effects of VR-based multi-task sensorimotor intervention on motor performance in children with ADHD and DCD comorbidity. Sci Rep 15, 43960 (2025). https://doi.org/10.1038/s41598-025-27613-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27613-6
