
Abstract
Local anesthetic minimally invasive liposuction (LAMS) is a liposuction technique that uses tumescent fluid and involves connecting a syringe to a tiny blunt catheter to remove fat at low pressure. The clinical outcomes of LAMS were compared based on the type of tumescent fluid. This study aim to compare the efficacy and safety of LAMS using half saline and normal saline. A retrospective cohort study was conducted at the 365mc Gangnam LAMS center from August 2023 to February 2024. A total of 147 patients who underwent LAMS for abdominal fat reduction were divided into two groups based on the type of tumescent fluid used. Clinical outcomes including changes in waist circumference were compared while adjusting various covariates. The study included 46 patients in the normal saline group and 101 patients in the half saline group. After adjusting multiple covariates, statistically significant greater reduction in waist circumference and weight change per extracted fat were observed in the half saline group compared to the normal saline group. LAMS using half saline appears to be more effective than using normal saline for reducing waist circumference and achieving greater weight loss per extracted fat.
IRB approval status: (IRB No. P01-202,410–01-046).
Similar content being viewed by others
Introduction
Liposuction is a cosmetic surgical procedure aimed at removing excess fat from various parts of the body, such as the abdomen, thighs, buttocks, and arms, to reshape these areas and improve their aesthetic appearance1. Indicated primarily for patients who have stable body weight but struggle with fat deposits that are resistant to diet and exercise, liposuction is not a weight-loss solution but rather a body contouring method2,3. According to Aesthetic Plastic Surgery National Databank Statistics 2022, approximately 405,328 liposuction procedures have been performed, accounting for about 13% of all plastic surgeries4.
Although generally effective at reducing localized fat deposits and enhancing body contours, liposuction can lead to various adverse events. The most common complications include bruising, swelling, pain, and temporary numbness3,5. More severe risks, although rare, include infections, hematoma, and contour irregularities2,5. Each patient’s outcomes can vary based on factors like age, skin quality, and overall health1,3.
Local anesthetic minimally invasive liposuction (LAMS) is a tumescent fluid liposuction technique that involves connecting a syringe to a small-gauge blunt catheter to extract fat at low pressure, which was named by our clinic. LAMS, unlike traditional liposuction, does not require sedation and leaves almost no scars.
Conventionally, low pressure tumescent fluid liposuction was performed using normal saline in combination with lidocaine, epinephrine, and sodium bicarbonate6,7. However, we hypothesized that if half saline is used as the tumescent fluid for liposuction, an osmotic difference between the tumescent fluid and fat cells might be created, potentially allowing for more effective fat removal. Therefore, we conducted a study comparing the efficacy and safety of using normal saline versus half saline as the tumescent fluid.
Methods
Study design
This was a retrospective cohort study to compare the efficacy of LAMS using normal saline and half saline. From August 2023 to February 2024, the study was conducted on patients who received LAMS on the abdomen at the single center. The allocation to either the normal saline group or the half saline group was not randomized but determined at the clinician’s discretion based on clinical judgment and experience. We measured the waist circumference of the patients before the procedure and about one month after receiving LAMS. Additionally, we measured the weight, body fat, and height before and after the procedure and number of bottles of extracted fat during the procedure. The precise volume of one bottle was 50 ml. This volume represented the aspirate, including fat as well as the mixed blood and tumescent fluid. We evaluated the efficacy by comparing the waist circumference before and after the procedure between two groups, while adjusting covariates. In addition, we compare secondary clinical outcomes including waist circumference change per extracted fat, weight change, and weight change per extracted fat before and after the procedure between two groups. The covariates include age, sex, height, weight, number of bottles of extracted fat, location (anterior abdomen/lateral abdomen), method of liposuction, and surgeon performing LAMS. Patients can choose between limited LAMS and unlimited LAMS as method of liposuction. In limited LAMS, both areas for fat removal and number of bottles of fat to be extracted are determined during the planning stage. On the other hand, in unlimited LAMS, areas for fat extraction are decided during the planning stage, but exact number of bottles of fat to be extracted is not determined. All methods were carried out in accordance with relevant guidelines and regulations. This study was reviewed and approved by the Public Institutional Review Board (IRB) (IRB No. P01-202,410–01-046). Due to the retrospective nature of the study, the Public Institutional Review Board waived the need of obtaining informed consent.
Study population
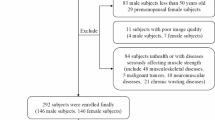
147 patients underwent LAMS at the center between August 2023 and February 2024. Among them, 46 patients underwent LAMS using normal saline and 101 patients underwent LAMS using half saline. All patients were 19 years old or older, with a BMI of 17.5 or higher. Patients with uncontrolled bleeding disorder, uncontrolled psychiatric disorder, BMI less than 17.5 did not receive liposuction. Patients who had used weight loss medication or oral corticosteroids within one month before visiting the hospital also did not receive liposuction.
Procedure of LAMS
We designated the insertion point, either the central lower abdomen or lateral upper abdomen, to avoid superficial epigastric artery. An 18G needle is used at the insertion point to make a hole. Through the hole, a blunt catheter with a diameter of 1.6 mm is inserted and tumescent fluid is sufficiently injected into the hypodermis. The conventional tumescent fluid using normal saline consists of 1 L of 0.9% sodium chloride, 16 ml of 2% lidocaine hydrochloride, 20 ml of 8.4% sodium bicarbonate, and 1 ml of epinephrine. The tumescent fluid using half saline consists of 1 L of 0.45% sodium chloride, 16 ml of 2% lidocaine hydrochloride, 20 ml of 8.4% sodium bicarbonate, and 1 ml of epinephrine (Table 1). After waiting 10–15 min for the fat cells to break down, the fluid mixture containing fat cells, blood, connective tissue, and tumescent fluid is extracted using a blunt catheter with a diameter ranged from 1.6 to 2.5 mm connected to a suction or a syringe. Repeat the procedure 2–3 times to ensure sufficient removal of abdominal fat.
Evaluation of clinical outcomes
Our primary clinical outcome was waist circumference change and secondary clinical outcomes include waist circumference change per extracted fat, weight change, and weight change per extracted fat.
Waist circumference was measured as follows: The nurse assistant locates the top of the patient’s hip bone and the bottom of the ribs, placing the tape measure midway between these points, aligned with the belly button. The tape is wrapped around the waist loosely enough to allow a finger to fit between the tape and the patient’s body.
Waist circumference change per extracted fat and weight change per extracted fat were defined as the difference in waist circumference and weight before and approximately 1 month after the procedure, respectively, divided by the volume of 50 ml per bottle of extracted fat. The number of bottles of extracted fat was recorded during procedure.
All patients underwent InBody test (InBody Co., Ltd., Seoul, Korea) before and approximately 1 month after the procedure to measure weight, body fat, and height. They revisited the clinic approximately 4 weeks (± 2 weeks) after receiving LAMS, and weight, body fat, height, and waist circumference were measured again. The InBody device uses bioelectrical impedance analysis to measure the resistance of body tissues to a small electrical current8,9. By analyzing how different tissues like muscle, fat, and water conduct electricity, it estimates body composition8,9. Esco et al. assessed the validity of the InBody and found it to be comparable with dual-energy X-ray absorptiometry (DXA), which is often considered the gold standard for body composition analysis8.
Assessment of safety
Based on medical records, we investigated the incidence of common adverse events following LAMS, such as bruising, nodularity, swelling, pain, erythema, and skin infection. We also examined the treatments received by patients for each adverse event and their outcomes.
Statistical analysis
Continuous variables are presented as mean and standard deviation. Categorical variables were presented as number and percentage. We utilized Analysis of Covariance (ANCOVA) to compare clinical outcomes between two groups while adjusting covariates. The sample circumference required to achieve a sufficient level of statistical power was calculated using the G*Power software10,11. Statistical analysis was processed with Python statsmodels.
Results
Patient characteristics
147 patients were enrolled in this study. Of these, 46 patients received LAMS using normal saline, and 101 patients received LAMS using half saline. The proportion of females in each group was higher, at 91.30% and 88.12%, respectively. Weight and height were comparable between both groups. Body fat and extracted fat were slightly higher in the half saline group, but no statistically significant differences were observed (Table 2). The proportion of patients with the procedure area being the anterior abdomen was higher in the half saline group at 78.22%, compared to 65.22% in the normal saline group. The rate of unlimited LAMS was slightly higher in the half saline group at 67.33% compared to 58.7% in the normal saline group. A total of 5 surgeons participated in the study. Detailed patient characteristics are described in Table 2.
Primary clinical outcome
The adjusted mean waist circumference reduction for LAMS using normal saline was 2.039 cm (95% CI: [1.580, 2.324]), while for LAMS using half saline, it was 2.382 cm (95% CI: [2.174, 2.669]). LAMS using half saline statistically significantly reduces the waist circumference more than LAMS using normal saline. (p-value 0.043) (Table 3, Figs. 1, 2) Images taken before, 1 month after, and 3 months after LAMS are presented in Fig. 3.

Comparison of waist circumference between patients receiving LAMS with normal saline and patients receiving LAMS with half saline.

Comparison of secondary outcomes between patients receiving LAMS with normal saline and patients receiving LAMS with half saline. (a) Waist circumference change per extracted fat. (b) Weight change. (c) Weight change per extracted fat.

Images taken (a) before LAMS with half saline, (b) 1 month after, and (c) 3 months after the procedure.
Secondary clinical outcomes
The adjusted mean waist circumference change per extracted fat for LAMS using normal saline was 0.00756 (95% CI: [0.00470, 0.00816]), while for LAMS using half saline, it was 0.00796 (95% CI: [0.00732, 0.00962]). The adjusted mean weight change for LAMS using normal saline was 1.085 kg (95% CI: [0.582, 1.657]), while for LAMS using half saline, it was 1.568 kg (95% CI: [1.195, 1.910]). The adjusted mean weight change per extracted fat for LAMS using normal saline was 0.00246 (95% CI: [0.00018, 0.00398]), while for LAMS using half saline, it was 0.00424 (95% CI: [0.00314, 0.00566]). The adjusted waist circumference change, and weight change per extracted fat for LAMS using half saline was higher than for LAMS using normal saline, but the difference was statistically insignificant. The weight change per extracted fat is statistically significantly higher in the half saline group compared to the normal saline group. (p-value 0.048) (Table 3, Fig. 2).
Subgroup analysis
The adjusted mean waist circumference reduction for unlimited LAMS using normal saline was 2.330 cm (95% CI: [1.969, 2.664]), while for LAMS using half saline, it was 2.280 cm (95% CI: [1.990, 2.589]). However, the difference was not statistically significant (Table 3). The adjusted mean waist circumference reduction for limited LAMS using normal saline was 2.148 cm (95% CI: [1.616, 2.587]), while for LAMS using half saline, it was 2.594 cm (95% CI: [2.208, 3.050]). However, the difference was not statistically significant (Table 3) Except for the finding that weight change was significantly higher in the normal saline group than in the half-saline group (1.067 kg [95% CI: 0.663–1.502] vs 0.424 kg [95% CI: − 0.081–0.887], p-value = 0.040) in limited LAMS, all other statistical results in subgroup analysis were insignificant.
Safety
There was no significant difference in adverse events between the two groups. Detailed information about adverse event is described in Table 4. The most common adverse event following LAMS was bruising, occurring in 73.9% of the normal saline group and 75.2% of the half saline group. This was followed by nodularity, swelling, pain, and erythema in order of frequency. There were no other adverse events, including skin infections.
Discussion
For all clinical outcomes, the efficacy of half saline LAMS consistently appeared to be higher than the efficacy of normal saline LAMS. After adjusting the covariates, there was a statistically significant higher waist circumference change in half saline LAMS compared to normal saline LAMS. Although, the data did not show a significant difference in waist circumference change per extracted fat, there was still a trend suggesting that the efficacy of half saline LAMS was superior. Given that the p-value was close to 0.05, a study with a larger population might have yielded statistically significant results.
Half saline LAMS showed a significantly greater weight change per extracted fat compared to normal saline LAMS after adjusting covariates. This indicates that half saline LAMS achieved greater weight reduction per bottle of fat extracted during liposuction.
The lack of a significant difference in weight change between half saline LAMS and normal saline LAMS can be explained by previous studies showing that liposuction does not result in substantial weight loss. Mohammed et al. found that body composition and weight remained the same after liposuction12. In addition, according to Rohrich et al., it has been reported that a significant number of individuals actually experience weight gain after liposuction13.
The precise mechanism behind the higher efficacy observed when using half saline as tumescent fluid in LAMS has not yet been identified. Unlike normal saline, half saline can cause osmotic lysis14 due to the osmotic pressure difference between fat cell and tumescent fluid, therefore, it is believed to be more effective in removing fat.
When extracted fat is subjected to centrifugation, it separates the fat into distinct layers based on their density15. (Supplementary Fig. 1) The layers of centrifuged extracted fat consist of an oil and liquid fat fraction at the top, adipocytes in the middle, and blood, water, and other cellular debris at the bottom. When centrifuged, the fraction of fat is higher in half saline compared to normal saline. Although these are preliminary, illustrative findings from two cases showing the potential effect difference between normal saline and half saline due to osmotic variation, they are not considered statistically significant.
In this study, we included the methods for performing LAMS—classified as limited or unlimited LAMS—as covariates in the statistical analysis, as these methods could influence the outcomes of liposuction. In limited LAMS, the number of bottles of fat to be extracted is determined before the procedure while the number is not fixed in unlimited LAMS. Instead, the goal for surgeon performing unlimited LAMS is to remove fat as much as possible. Therefore, as unlimited LAMS tends to remove a larger amount of fat compared to limited LAMS, the method used can have impact on the outcomes of liposuction.
In terms of safety, LAMS is considered generally safe procedure. After performing LAMS, adverse events such as bruise, nodularity, pain, erythema, and edema were observed. Most of adverse event were mild to moderate and either improved spontaneously or were controlled with medication such as analgesics. Swelling and bruising were slightly higher in the half saline group, while nodularity was slightly higher in the normal saline group. However, there were no statistically significant differences, and most of these effects were transient. In contrast to traditional liposuction, LAMS did not result in any severe adverse events such as vascular complications, abdominal wall puncture, or nerve damage. If a 14G-16G cannula is gently approached to the hypodermis, it is difficult for a blunt cannula to pierce an artery or abdominal wall. If the cannula is inserted into the hypodermis with too much force, it tends to bend rather than pierce an artery or the abdominal wall.
Even though there is a limitation of this study, such as being conducted at a single institution with a small patient group, a relatively wide window in the follow-up period among patients, and lack of long term follow up, low pressure tumescent fluid liposuction using half saline were more effective compared to those using normal saline.
Conclusion
In conclusion, the clinical outcomes of tumescent fluid liposuction using half saline were superior compared to those using normal saline while no significant differences were observed between the two groups regarding safety. When performing fat extraction during LAMS procedures, it is advisable to consider using half saline over normal saline.
Data availability
The datasets used and analyzed during this study are available from the corresponding author on reasonable request.
Abbreviations
- LAMS:
-
Local anesthetic minimally-invasive liposuction
References
Mendez, B. M., Coleman, J. E. & Kenkel, J. M. Optimizing patient outcomes and safety with liposuction. Aesthet. Surg. J. 39, 66–82. https://doi.org/10.1093/asj/sjy151 (2019).
Kaoutzanis, C. et al. Cosmetic liposuction: Preoperative risk factors, major complication rates, and safety of combined procedures. Aesthet. Surg. J. 37, 680–694. https://doi.org/10.1093/asj/sjw243 (2017).
Costagliola, M., Atiyeh, B., Rampillon, F., Illouz, Y. G. & Dibo, S. Aesthetic or functional indications for liposuction. Aesthet. Surg. J. 33, 1212–1213. https://doi.org/10.1177/1090820X13511454 (2013).
Aesthetic plastic surgery national databank statistics 2022. Aesthet. Surg. J 43, 1-19, https://doi.org/10.1093/asj/sjad354 (2023)
Villanueva, N. L. & Kenkel, J. M. Commentary on: Cosmetic liposuction—preoperative risk factors, major complication rates, and safety of combined procedures. Aesthet. Surg. J. 37, 695–697. https://doi.org/10.1093/asj/sjw283 (2017).
Venkataram, J. Tumescent liposuction: A review. J. Cutan. Aesthet. Surg. 1, 49–57. https://doi.org/10.4103/0974-2077.44159 (2008).
Boschert, M. T. & Puckett, C. L. Tumescent infusion for liposuction: A practical method and pressure delivery system. Aesthet. Surg. J. 18, 266–268. https://doi.org/10.1016/s1090-820x(98)70055-x (1998).
Esco, M. R. et al. Comparison of total and segmental body composition using DXA and multifrequency bioimpedance in collegiate female athletes. J. Strength Cond. Res. 29, 918–925. https://doi.org/10.1519/JSC.0000000000000732 (2015).
Antonio, J. et al. Comparison of dual-energy x-ray absorptiometry (DXA) versus a multi-frequency bioelectrical impedance (InBody 770) device for body composition assessment after a 4-week hypoenergetic diet. J. Funct. Morphol. Kinesiol. https://doi.org/10.3390/jfmk4020023 (2019).
Faul, F., Erdfelder, E., Lang, A. G. & Buchner, A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. https://doi.org/10.3758/bf03193146 (2007).
Faul, F., Erdfelder, E., Buchner, A. & Lang, A. G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 41, 1149–1160. https://doi.org/10.3758/BRM.41.4.1149 (2009).
Mohammed, B. S., Cohen, S., Reeds, D., Young, V. L. & Klein, S. Long-term effects of large-volume liposuction on metabolic risk factors for coronary heart disease. Obesity (Silver Spring) 16, 2648–2651. https://doi.org/10.1038/oby.2008.418 (2008).
Rohrich, R. J. et al. The key to long-term success in liposuction: a guide for plastic surgeons and patients. Plast Reconstr Surg 114, 1945–1952. https://doi.org/10.1097/01.prs.0000143002.01231.3d (2004).
Goodhead, L. K. & MacMillan, F. M. Measuring osmosis and hemolysis of red blood cells. Adv. Physiol. Educ. 41, 298–305. https://doi.org/10.1152/advan.00083.2016 (2017).
Shauly, O., Gould, D. J. & Ghavami, A. Fat grafting: Basic science, techniques, and patient management. Plast. Reconstr. Surg. Glob. Open 10, e3987. https://doi.org/10.1097/GOX.0000000000003987 (2022).
Funding
No funding sources.
Author information
Authors and Affiliations
Contributions
K. Paik and C. Huh contributed to the study concept, research methodology, and analysis methods. K. Paik performed the statistical analysis. N. Kim, J. Kim, and J. Jeong provided resources. J. Na, J. Shin, and C. Huh reviewed and edited the manuscript. K. Paik drafted the initial manuscript. C. Huh supervised the study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Paik, K., Kim, N.C., Kim, J.E. et al. The efficacy of half saline in tumescent liposuction. Sci Rep 15, 44287 (2025). https://doi.org/10.1038/s41598-025-27904-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27904-y

{kind=link}