
Abstract
To compare different interventional strategies for patients with 4b-AMI because of very late stent thrombosis (VLST) in real world. 316 patients with VLST-4bAMI were enrolled and divided into Re-stent group, drug coated balloon (DCB) group and plain old balloon angioplasty(POBA) group. The MACE was observed at 1 year follow up including cardiac death, recurrent AMI(re-AMI), target lesion revascularization (TLR) and recurrent ST(RST). The Kaplan-Meier survival curves were used to compare the survival of free-MACE events, and the propensity score matching was used for further analysis. 66 MACEs were observed at 1 year follow-up. There was no significant difference in the MACE between the three groups (P > 0.05), but TLR in the POBA group was the highest (P = 0.023). Kaplan-Meier survival analysis showed that there was no significant difference in the survival of 1-year cumulative free-MACE events between the three groups (P > 0.05), the survival of free-TLR in the POBA group was the lowest (P = 0.015). There was no significant difference in the incidence of MACE after propensity score matching. There is no significant difference in prognosis between the three interventional treatment strategies of VLST-4bAMI. DCB did not have less favorable clinical outcomes than Re-stent or POBA.The treatment of VLST-4bAMI is still a major clinical challenge.
Similar content being viewed by others

Introduction
Stent thrombosis (ST) is a rare but highly fatal complication after percutaneous coronary intervention (PCI)1, and acute myocardial infarction (AMI) due to ST is defined as 4bAMI2. With the popularity of PCI, 4bAMI is increasing. The American Academic Research Association (ARC) categorizes ST according to the time of ST onset into acute stent thrombosis (< 24 h), subacute stent thrombosis (1–30 days), late stent thrombosis (> 30 days to 1 year), and very late stent thrombosis (> 1 year)(VLST)3. The incidence, treatment and prognosis of ST in different stages is different, among which VLST-4b AMI has the highest incidence4. Currently, there is no guideline or consensus on the interventional treatment strategy of VLST-4bAMI, there are few reports on the treatment of VLST-4bAM with DCB. and this study is a single-center cohort study aimed at observing and comparing the prognosis of different interventional treatment strategies for patients with VLST-4bAMI.
Methods
Study population
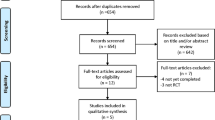
From January 2018 to June 2022, we screened 519 patients with acute myocardial infarction (AMI) who had a history of coronary stent implantation ≥ 1 year in the coronary care unit of Tianjin Chest Hospital. Among these, 339 patients were confirmed to have very late stent thrombosis (VLST) in the culprit vessel by coronary angiography and thus diagnosed as VLST-4b AMI. We further excluded 10 patients who received medication-only treatment and 13 patients who underwent coronary artery bypass grafting (CABG). Finally, 316 patients with VLST-4b AMI who underwent interventional therapy were enrolled in the study. The patients were divided into three groups: Re-stent group, drug coated balloon (DCB) group, and plain old balloon angioplasty (POBA) group according to the type of interventional therapy in the real world, which are based on clinical characteristics(such as age, comorbidity, high bleeding patients, etc.) and characteristics of culprit vessel(such as stent underexpansion, in-stent restenosis, bifurcation lession, etc.).Interventional therapy is carried out according to the PCI guidelines5, and the strategy is decided by two independent operators after discussion. If there is a disagreement, the opinion of a third operator needs to be sought. Inclusion criteria: (1) Previous history of coronary stent implantation and ≧ 1 year. (2) This admission meets the diagnostic criteria of AMI2, and coronary angiography confirms that the patient’s culprit vessel has VLST.(3) Coronary angiography confirms that the thrombus is located in the stent or 5 mm proximal and distal margins of the stent in patients with VLST. Exclusion criteria: (1) patients with non-AMI and type 2 AMI, including patients with unstable angina pectoris (UAP) and type 2 AMI due to coronary artery spasm, spontaneous dissection, and embolism; (2) ST that was not confirmed by coronary angiography, including probable in-stent thrombosis such as sudden death; (3) patients with acute ST, subacute ST, late ST. The study flow chart was shown in Fig. 1. The study was approved by the Ethics Committee of Tianjin Chest Hospital (Ethics No. 2018KY 010 − 01), and the patients signed an informed consent form. We confirm that all experiments were performed in accordance with relevant guidelines and regulations.

The study flow chart.
Procedure
Selective coronary angiography was performed by Judkin’s method using an angiography machine (Philips), and coronary lesions and reference vessel diameters were determined using a quantitative coronary angiography system. The culprit vessel associated with VLST was identified by the operator based on the patient’s medical history, electrocardiogram, angiographic results, etc. PCI was performed in accordance with the interventional therapy standard. 100 U/kg of heparin was given to the patients before PCI, and heparin was supplemented according to the results of activated clotting time of whole blood (ACT) during the operation to maintain ACT at 250–300 s. Aspirin 300 mg, clopidogrel 300 mg, or ticagrelor 180 mg were given to the patients before the operation.The operator performed interventional treatment for the culprit vessel based on clinical characteristics and coronary characteristics, including Re-stent, DCB, and POBA.The operator applied a aspiration catheter and the Glycoprotein IIb/IIIa inhibitor according to the characteristics of the thrombus. Hemodynamically unstable patients were implanted with intra-aortic balloon pump (IABP) for supportive therapy. Success criteria for the procedure: angiographic demonstration of residual stenosis < 20% and antegrade flow to Thrombolysis in Myocardial Infarction (TIMI) grade 3. VLST images and the PCI procedure should be analyzed independently by at least 2 experienced cardiologists. Postoperatively, all PCI-treated patients were administered dual antiplatelet drugs and admitted to the coronary care unit for monitoring and treatment.
Clinical information
(1) General information: patients’ gender, age, history of smoking, history of drinking, diabetes, hypertension and hypercholesterolemia, etc. (2) Laboratory data: white blood cells (WBC), hemoglobin (Hb), platelets (PLT), creatine kinase isoenzyme (CK-MB), troponin T (TNT), low-density lipoprotein cholesterol (LDL-C), and fasting blood glucose(FBG), etc. at the time of the patient’s admission. (3) Clinical data: Killip’s cardiac function classification, left ventricular ejection fraction (LVEF), and medication etc. at admission. (4) Coronary angiography and interventional therapy data: ST time, first stent implantation for AMI, first intervention stent type [bare metal stent(BMS), first-generation drug-eluting stent (DES), second-generation DES], review of coronary angiography (CAG), target vessel, interventional therapy, and intravascular imaging.
Follow-up and study endpoints
MACE events at 1 year follow up were recorded by inpatient data, telephone or outpatient follow-up. MACE events included cardiac death, recurrent AMI(re-AMI), target lesion revascularization (TLR), and recurrent ST(RST). cardiac death was defined as cardiac disease-related death. re-AMI was defined as (1) in-hospital: recurrence of ischemic symptoms within 28 d, recurrence of ST-segment elevation ≥ 1 mm on the ECG or new pathologic Q waves in at least 2 contiguous leads, and re-elevation of biomarkers of myocardial injury by 20% for 3 to 6 h after stabilization or decline. (2) follow-up: Acute myocardial infarction was characterized after 28 d of the first myocardial infarction. TLR was defined as repeat intervention or coronary artery bypass grafting based on restenosis of the target lesion or other complications. RST was defined as recurrent thrombus according to the definition published by the ARC, and the thrombus was located within the stent or 5 mm proximal and distal margins of the stent.
Statistical methods
Statistical analyses were performed using SPSS 25.0 software. Normally distributed continuous variables were expressed as mean ± standard deviation, comparisons between groups were conducted using the t-test. Non-normally distributed continuous variables were presented as median (interquartile range, P25, P75), intergroup comparisons were performed using the rank-sum test. Categorical data were compared between groups using theχ²test or Fisher’s exact probability test, as appropriate. Survival curves were plotted using the Kaplan-Meier method, differences among the three groups were compared using the Log-rank test. A two-tailed P value < 0.05 was considered statistically significant. Propensity score matching (PSM) comparisons were used to determine whether there was a difference in MACE among the three treatment groups for VLST-4b AMI patients. The three groups of cases with different treatment were matched 1:1:1 using the nearest neighbor matching method with a caliper value set at 0.25, and the balance of control variables before and after matching was tested.
Results
Baseline characteristics
A total of 316 patients were included, with a mean age of (65.76 ± 9.74) years, 249 (78.8%) were male. There were 203 cases in the Re-stent group, 42 cases in the DCB group and 71 cases in the POBA group. Differences in hypercholesterolemia, atrial fibrillation, family history of CAD, plateletcrit, creatine kinase, and creatine kinase isoenzyme were statistically significant among the three groups (P < 0.05). The differences in other baseline data among the three groups were not statistically significant (P > 0.05), as shown in Tables 1 and 2.
Table 3
Comparison of imaging and hospitalization in the three groups
The differences in low molecular heparin anticoagulation therapy, Killip classification, ST time, proportion of first stent implantation for AMI, B2/C lesion, and IABP use were statistically significant in the three groups (P < 0.05), and the differences in the comparison of other coronary angiographic and hospitalization period data were not statistically significant (P > 0.05), as shown in Table 3.
Comparison of MACE events at follow-up in the three groups
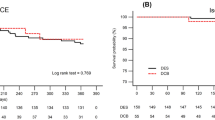
Of the 316 patients, 302 (95.6%) completed the 1-year follow-up, and a total of 66 MACE events were recorded, including 42 cases in the Re-stent group, 9 cases in the DCB group, and 15 cases in the POBA group. The difference in MACE among the three groups was not statistically significant (P > 0.05), but the difference in TLR was statistically significant, with the highest incidence of TLR in the POBA group (P = 0.023), as shown in Table 4.The Kaplan-Meier survival analysis showed that the difference in the cumulative survival of free-MACE events at 1 year among the three groups was not statistically significant (P > 0.05), but there was a significant difference in the survival of free-TLR, with the lowest survival of free-TLR in the POBA group (P = 0.015), and the other differences in the survival of free-cardiac death, free re-AMI, and free-RST were not statistically significant (P>0.05), as shown in Fig. 2.

Kaplan Meier survival curve of three groups of MACE events.

Kaplan Meier survival curve of three groups of MACE events after propensity score matching.
Comparison of baseline information and prognosis among the three groups using propensity score matching
The propensity score nearest neighbor matching method was used to match the three groups of patients 1:1:1, with a caliper value set at 0.25, and to test the balance of control variables before and after matching. Matching variables included baseline characteristics (such as age, male, smoking, etc.) and angiographic characteristics (such as bifurcation lesion, left main artery lesion, occlusive lesion, etc.). The three groups of patients after matching were 36 patients in the Re-stent group, 36 patients in the DCB group, and 36 patients in the POBA group. After matching, except for family history of CAD, diabetes and first stent implantation for AMI, the differences in the above mentioned matching variables among the three groups were not statistically significant and the distribution was balanced (P > 0.05 SMD < 0.2). A total of 22 MACE events occurred in the three groups after matching, including 7 cases in the re-stent group, 8 cases in the DCB group, and 7 cases in the POBA group. The difference in MACE among the three groups was not statistically significant (P > 0.05), but the difference in TLR was statistically significant, with the highest incidence of TLR in the POBA group (P = 0.034), as shown in Table 5. Kaplan-Meier survival analysis showed that the difference in 1-year cumulative survival free-MACE event among the three groups was not statistically significant (P > 0.05), but there was a significant difference in the survival of free-TLR, with the lowest survival of free-TLR in the POBA group (P = 0.028), and the other differences in the survival of free-cardiac death, free re-AMI, and free-RST were not statistically significant (P>0.05), as shown in Fig. 3.
Discussions
VLST-4b AMI is quite different from Denovo myocardial infarction in terms of mechanism of occurrence, diagnosis and treatment and prognosis. Regarding its interventional treatment strategy, previous studies have some contradictory findings, and there is still a lack of evidence from large-sample multi-centre RCT studies and guidelines6,7,8.
An observational study included 19 patients with VLST who had undergone prior DES implantation, 7 patients were treated with balloon dilatation alone while the other 12 patients were treated with reimplantation of stents, and both groups were followed up for 6–8 months, the results of the study showed that all MACE events occurred in the balloon dilatation alone population, suggesting that reimplantation of stents may improve the prognosis9. However, due to the small sample size and the inclusion of many patients with unstable angina, the results of this study do not truly reflect the safety and efficacy of different treatment strategies for type 4b AMI caused by VLST. 431 patients with ST were enrolled in the Dutch Registry Study, 203 (48.2%) patients were treated with balloon angioplasty, 214 (50.8%) patients underwent balloon angioplasty followed by implantation of an additional stent.The primary end point including cardiac death and definite recurrent ST occurred in 111 patients after a median follow-up of 27.1 months. And the results of Multivariate Cox Proportional Hazard Analysis demonstrated that re-implantation of a stent was an independent risk factor for the primary end point (HR: 1.73, 1.14–2.61, p < 0.001)10. A total of 106 ST patients were included in the study conducted by Almalla et al. The frequency and predictors of adverse events (death, myocardial infarction, and recurrent ST) during long-term follow-up (mean 65 ± 30 months) were evaluated.They were divided into event group and event-free group. Of these, 33(31.1%) patients were treated with balloon angioplasty, 73(68.9%) patients were implanted additional stents. The results of the study showed that re-implantation of stents did not increase the risk of MACE events11. A total of 221 ST patients were enrolled in the UCST study, procedural characteristics were compared between those with and those without MACE, defined as all-cause mortality, myocardial infarction and stroke. 64% (141/221) of patients received re-implantation of the stent.The findings demonstrated that re-implantation of the stent did not increase or decrease the risk of MACE events(HR: 1.21, 0.68–2.15, p = 0.5)12. A Japanese study of patients with ST-induced ACS suggested that more than half of ST patients were treated with thrombus aspiration and/or balloon dilatation only, suggesting that PCI operators intentionally avoided implantation of new stents. And only 35.1% of ST patients underwent new stent implantation, which was significantly lower than that of Denovo-ACS patients (35.1% vs. 75.3%), and the investigators suggested that this could be one of the potential reasons for the higher incidence of recurrent ST in ST- ACS patients13. A Dutch study on ST suggested that additional stent was performed in 59.8% of patients and DES was used in 90.8% of patients. POBA was performed in 34.4% and POBA was more common in patients with early ST14. Based on the results of the above studies, the relationship between reimplantation of stents and better clinical prognosis of ST patients cannot be confirmed, and the conclusions still need to be further explored in multicenter, large-sample randomized controlled trials. Moreover, the above studies mainly focused on the ST-ACS population, including acute ST, subacute ST, and late ST patients, and included many patients with unstable angina pectoris, while few studies were conducted on the special population of type 4b AMI caused by VLST. In this study, for the population of patients with VLST-4bAMI, 203 casesreceived re-stent treatment, 71 cases received POBA,, and 42 cases received DCB. the difference in the 1-year free-MACE event survival among the three groups was not statistically significant, the survival of free-TLR in the POBA group is lowest. These conclusions do not prove that the re-stent has more advantages.
Different types of re-stent may also differ in the prognosis of VLST-4bAMI. A multicenter study conducted by Kimura et al. reported that the 1-year mortality in patients with definite VLST after implantation of a first-generation sirolimus stent was 10.5%, whereas the mortality in patients with early ST and those with late ST were 22.4% and 23.5%, respectively15. Another single-center study showed a 5-year mortality of 39.0% in ST patients, most of whom received first-generation drug-eluting stents16. A study conducted by Xu L. et al. included 62 patients with AMI who presented with VLST. it was found that although reimplantation of a stent was not associated with the development of MACE, reimplantation of a first-generation drug-coated stent was a risk factor for the development of MACE17. Another retrospective study included 608 patients with STEMI (50 VLST, 558 in Denovo lesions), all of whom were treated with second-generation DES, and it was found that the second-generation DES did not increase hospitalization and long-term MACE events in patients with VLST-STEMI compared to STEMI caused by Denovo lesions. The investigator analyzed that the possible mechanism is more rapid and complete endothelialization after second-generation DES implantation14. The ESTHIR study, which enrolled 131 ST patients, showed that re-implantation of second-generation drug-eluting stents significantly reduced long-term mortality18. Therefore, we speculated that second-generation DES might be a better choice for this particular type of STEMI caused by VLST compared with balloon dilatation alone and first-generation DES. However, in this study, considering that coronary stents have been subjected to national consistency evaluation and centralized purchasing, the type of re-implanted stent was not clearly differentiated.
A Meta-analysis on DCB application targeting non-small-vessel PCI therapy included three randomized controlled trials and two observational studies involving a total of 520 patients19. In terms of cardiac death (RR 0.33, 95% CI [0.01, 8.29], p = 0.50), myocardial infarction (RR 0.49, 95% CI [0.09,2.50], p = 0.39), target lesion revascularization (RR 0.64, 95% CI [0.19, 2.18], p = 0.47), and late lumen loss (RR 0.48, the 95% CI [-1.32, 0.36], p = 0.26), DCB did not show an advantage over stenting and the minimum lumen diameter was smaller in the DCB group. For in-stent restenosis, it has been shown that DCB is as effective as DES, whereas the recently European guidelines for myocardial revascularization have recommended DCB as class I, with a level of evidence A20. For stent thrombosis, there are fewer DCB studies, and 13.3% (42/316) of VLST-4b AMI patients were treated with DCB in this study. The difference in the incidence of MACE among the three groups was not statistically significant.DCB did not have less favorable clinical outcomes than Re-stent or POBA.
The Bern, PESTO and PRESTIGE registry studies are three largest studies of the use of intravascular imaging techniques for STto date, demonstrated that OCT was able to detect the underlying cause of ST in the majority of cases at the time of ST event. In these studies, poor image quality was found in only 5.5% of cases, whereas in interpretable OCT, the cause of ST was detected in 98.2% of cases in the Bern study, 87% of cases in the PESTO study, and all cases in the PRESTIGE study. these etiologic analyses are extremely important in guiding the treatment strategies of ST patients21,22,23. Intravascular imaging means can be used to detect causes of stent failure such as stent thrombosis and to guide individualized treatment, and have a class IIa indication in the European Society of Cardiology guidelines24. OCT is superior to IVUS in guiding ST treatment because it allows for accurate assessment of luminal pathologic features and allows for a more detailed understanding of stent structure and stent apposition as well as reliable morphologic characterization of the endothelium25. In order to better prevent the occurrence of VLST, it is necessary to assess the risk of VLST as early as possible. For high-risk patients, intravascular imaging techniques such as IVUS or OCT should be applied as much as possible during PCI to optimize the operation process and select appropriate stents according to the actual situation of the coronary lesion, so as to avoid the occurrence of events such as stent malapposition and stent coverage incompleteness.
VLST-4bAMI is a rare but severe type of AMI, and our study compared different interventional treatment strategies and provided new evidence for the treatment of this particular type AMI. But it is a retrospective study with a small sample size. Moreover, some variables in the propensity score matching can not be completely matched, which weakens its persuasiveness.Therefore, the evidence require validation in more prospective trials.
Conclusions
There is no significant difference in prognosis between the three interventional treatment strategies of VLST-4bAMI. DCB did not have less favorable clinical outcomes than Re-stent or POBA, which suggests it may be a potential option for VLST-4bAMI.The treatment of VLST-4bAMI is still a major clinical challenge and needs to be explored in multi-center randomized controlled trials with large samples.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- MI:
-
Myocardial infarction
- CABG:
-
Coronary artery bypass grafting
- AF:
-
Atrial fibrillation
- CAD:
-
Coronary artery disease
- HR:
-
Heart rate
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- LVEF:
-
Left ventricular ejection fraction
- NSTEMI:
-
Non-ST-segment elevation myocardial infarction
- STEMI:
-
ST-segment elevation myocardial infarction
- DAPT:
-
Dual antiplatelet therapy
- ACEI:
-
Angiotensin-converting enzyme inhibitor
- ARB:
-
Angiotensin II receptor blocker
- ARNI:
-
Angiotensin receptor neprilysin inhibitor
- WBC:
-
White blood cells
- PLT:
-
Platelet
- PDW:
-
Platelet distribution width
- P-LCR:
-
Platelet-large cell ratio
- PCT:
-
Plateletcrit
- Hb:
-
Hemoglobin
- RDW:
-
Red blood cell distribution width
- FBG:
-
Fasting blood glucose
- HbA1c:
-
Glycosylated hemoglobin
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- Apo A1:
-
Apolipoprotein A1
- Apo B:
-
Apolipoprotein B
- Lp(a):
-
Lipoprotein(a)
- Cr:
-
Creatinine
- UA:
-
Uric acid
- CK:
-
Creatine kinase
- CK-MB:
-
Creatine kinase MB
- TnT:
-
Troponin T
- BNP:
-
B-type natriuretic peptide
- HCY:
-
Homocysteine
- CRP:
-
C-reactive protein
- ST:
-
Stent thrombosis
- TIMI:
-
Thrombolysis in myocardial infarction
- LAD:
-
Left anterior descending artery
- LCX:
-
Left circumflex artery
- RCA:
-
Right coronary artery
- LM:
-
Left main coronary artery
- SVG:
-
Saphenous vein graft
- IABP:
-
Intra-aortic balloon pump
- OCT:
-
Optical coherence tomography
- IVUS:
-
Intravascular ultrasound
- LMWH:
-
Low molecular weight heparin
- MACE:
-
Major adverse cardiovascular events
- TLR:
-
Target lesion revascularization
References
Kuramitsu, S. et al. Drug-eluting stent thrombosis: current and future perspectives. Cardiovasc. Interv Ther. 36 (2), 158–168 (2021).
Thygesen, K. et al. Fourth universal definition of myocardial infarction (2018). J. Am. Coll. Cardiol. 72 (18), 2231–2264 (2018).
Ullrich, H., Munzel, T. & Gori, T. Coronary stent Thrombosis- predictors and Prevention. Dtsch. Arztebl Int. 117 (18), 320–326 (2020).
Courtney, B. K. Very late stent thrombosis in japan: A look into the Future?. Can. J. Cardiol. 40 (4), 705–706 (2024).
Lawton, J. S. et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: A report of the American college of Cardiology/American heart association joint committee on clinical practice guidelines. J. Am. Coll. Cardiol. 79 (2), e21–e129 (2022).
Muntane-Carol, G., Gomez-Lara, J. & Romaguera, R. Stent thrombosis with new-generation drug-eluting stents: a decade of reassuring evidence. Rev. Esp. Cardiol. (Engl Ed). 75 (11), 861–863 (2022).
Polimeni, A. et al. Stent thrombosis after percutaneous coronary intervention: from Bare-Metal to the last generation of Drug-Eluting Stents. Cardiol. Clin. 38 (4), 639–647 (2020).
Kumar, M. et al. The outcome of primary percutaneous coronary intervention in patients with stent thrombosis. Indian Heart J. 74 (6), 464–468 (2022).
Kim, M. C. et al. Incidence of cardiac death and recurrent stent thrombosis after treatment for angiographically confirmed stent thrombosis. J. Cardiol. 74 (3), 267–272 (2019).
van Werkum, J. W. et al. Long-term clinical outcome after a first angiographically confirmed coronary stent thrombosis: an analysis of 431 cases. Circulation 119 (6), 828–834 (2009).
Almalla, M. et al. Long-term outcome after angiographically proven coronary stent thrombosis. Am. J. Cardiol. 111 (9), 1289–1294 (2013).
Yeo, K. K. et al. Long-term outcomes of angiographically confirmed coronary stent thrombosis: results from a multicentre California registry. EuroIntervention 11 (2), 188–195 (2015).
Chechi, T. et al. ST-segment elevation myocardial infarction due to early and late stent thrombosis a new group of high-risk patients. J. Am. Coll. Cardiol. 51 (25), 2396–2402 (2008).
He, C. et al. Long-term outcomes of primary percutaneous coronary intervention with Second-generation Drug-eluting stents in ST-elevation myocardial infarction patients caused by very late stent Thrombosis. Chin. Med. J. (Engl). 130 (8), 929–935 (2017).
Kimura, T. et al. Comparisons of baseline demographics, clinical presentation, and long-term outcome among patients with early, late, and very late stent thrombosis of sirolimus-eluting stents: observations from the registry of stent thrombosis for review and Reevaluation (RESTART). Circulation 122 (1), 52–61 (2010).
Kubo, S. et al. Comparison of long-term outcome after percutaneous coronary intervention for stent thrombosis between early, late, and very late stent thrombosis. Circ. J. 78 (1), 101–109 (2014).
Xu, L. et al. Long-term outcomes following very late stent thrombosis of drug-eluting stent. J. Cardiol. 66 (6), 496–501 (2015).
Katsikis, A. et al. Contemporary management of stent thrombosis: predictors of mortality and the role of new-generation drug-eluting stents. Catheter Cardiovasc. Interv. 96 (1), E8–E16 (2020).
Sun, K., Liu, Z. & Wang, H. Drug-Coated balloon vs. Stent for de Novo Non-small coronary artery disease: A systematic review and Meta-Analysis. Front. Cardiovasc. Med. 8, 700235 (2021).
Giacoppo, D. et al. Paclitaxel-coated balloon angioplasty vs. drug-eluting stenting for the treatment of coronary in-stent restenosis: a comprehensive, collaborative, individual patient data meta-analysis of 10 randomized clinical trials (DAEDALUS study). Eur. Heart J. 41 (38), 3715–3728 (2020).
Adriaenssens, T. et al. Optical coherence tomography findings in patients with coronary stent thrombosis: A report of the PRESTIGE consortium (Prevention of late stent thrombosis by an interdisciplinary global European Effort). Circulation 136 (11), 1007–1021 (2017).
Taniwaki, M. et al. Mechanisms of very late Drug-Eluting stent thrombosis assessed by optical coherence Tomography. Circulation 133 (7), 650–660 (2016).
Souteyrand, G. et al. Mechanisms of stent thrombosis analysed by optical coherence tomography: insights from the National PESTO French registry. Eur. Heart J. 37 (15), 1208–1216 (2016).
Neumann, F. J. et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. Heart J. 40 (2), 87–165 (2019).
Rai, H. et al. Stent optimization using optical coherence tomography and its prognostic implications after percutaneous coronary Intervention. J. Am. Heart Assoc. 11 (9), e023493 (2022).
Funding
This study was supported by the Key Project of Scientific and Technological Support Plan of Tianjin in 2020 (No. 20YFZCSY00820), the Key Disciplines of Tianjin Health Research Project (No. TJWJ2022XK032), the Tianjin Health Research Youth Project (No. TJWJ2021QN058), the Key Projects of Tianjin Natural Science Foundation (No. 22JCZDJC00130), the Science and Technology Fund Project of Tianjin Municipal Health Commission (No. TJWJ2021MS027), and the Tianjin Medical Key Construction Discipline Project (No. TJYXZDXK-055B).
Author information
Authors and Affiliations
Contributions
YL and JG were the principal investigators for managing the protocol and developed the protocol for this project. XWL, MDG, JYX, JXW, NZ, PJL, and YHW were responsible for data collection, analysis and management. XWL, MDG, JYX, and JXW were responsible for epidemiological investigations and laboratory testing. XWL and MDG performed all statistical analyses. XWL contributed to writing the first draft of the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study protocol was approved by the Internal Review Board of Tianjin Chest Hospital (No. 2018KY-010-01), and all included patients provided signed informed consent before participating in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, X., Gao, M., Xiao, J. et al. Comparison of different interventional treatment strategies for patients with type 4b acute myocardial infarction caused by very late stent thrombosis. Sci Rep 15, 44290 (2025). https://doi.org/10.1038/s41598-025-27987-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27987-7
