
Abstract
Fear of disease progression is a common problem among patients with chronic disease. However, to the authors’ knowledge, it was not studied in Ethiopia. Thus, this study aimed to assess fear of disease progression and related factors among patients with chronic disease attending South Wollo zone government hospitals, Northeast Ethiopia. Institution-based cross-sectional study design was conducted among 411 patients with chronic disease for quantitative data. For qualitative data in-depth interview were done until information saturation. The total sample size was allocated proportionally based on the number of patients in selected government hospitals. Finally, from each selected hospital, patients were selected using systematic random sampling technique. Fear of disease progression was measured using fear of progression questionnaire. A significant association was declared at p-value of < 0.05 in multivariable analysis. In this study, 40.9% (95% CI = 36.3–45.7) of patients had high fear of disease progression. Patients with heart failure, presence of comorbidities, not attending health education, poor social support, current chat use, severe depression, moderate anxiety and severe anxiety were significantly associated with high fear of disease progression. Eating sweet foods, heavy work, improper use of medication, afraid of death, stressful living conditions, shortness of breath and fatigue manifestations, afraid of comorbidity, absence of social support, drug resistance, thinking about children and depression were explained as the reasons for fear of disease progression in qualitative part of this study. Significant numbers of patients had high fear of disease progression. Therefore, policy makers, health professionals and community should give more attentions especially for those patients with the identified significant associated factors to reduce high fear of disease progression. Researchers should focus to get clear information about fear of disease progression for patients with a particular disease.
Similar content being viewed by others


Background
Fear of disease progression (FoDP) defined as a re-active, consciously perceived fear that develops from a serious, life-threatening, disabling disease or its treatment and consequences1,2. When patients realize that they have a severe disease that threatens their life, they start thinking of the development of the disease and its possible progression in the future3. FoDP is an appropriate response to the real threats of diagnosis, treatments and course of illness. However, the level of fear can range between functional and dysfunctional ends. Elevated fear of progression becomes dysfunctional, affecting wellbeing, quality of life, and social functioning are in need for treatment4,5,6.
With regard to quality of life, moderate significant correlations were found between FoDP and physical functioning, social functioning, general health status, pain and fatigue7. In previous studies, FoDP was evident in patients with cancer, rheumatoid arthritis, diabetes, parkinson’s disease, crohn’s disease, and multiple sclerosis1,8. The experiences of fears, symptoms returning or progression are common undiagnosed and untreated problem among patients who live with chronic illness9,10.
Patients can experience long lasting and exaggerated realistic fears that affect their well-being and quality of life. This is a reactive, non-neurotic fear response patients are fully aware of4. While there were variations, the biggest worries for respondents with regard to having long-term illnesses were become a burden to their family and a concern of dying. The survey found that respondents had fear of chronic disease and recommended educational program to adopt a healthy lifestyle11,12. Attitudes towards chronic illness, such as fears of memory loss, losing independence, afraid of suffering again, afraid of the spread of disease to other body part, afraid of disease consequences and burdening on family members and society are deeply embedded in people’s cultural biographies and life experiences13,14,15.
FoDP does not only have a profound impact on patients, but also on their spouses. A study on partners of chronically ill patients in Germany showed that significant positive correlations were found for anxiety and depression16. A study done in Netherland showed that 18% reported high FoDP. Fear of progression was moderately correlated with feelings of depression and anxiety7. Similarly, significant positive relationships were found between FoDP and anxiety, stress and depression17. In other study, a high level of fear of cancer progression was revealed in 26.07% of patients18.
In Malaysia respondents were asked what they feared most in relation to having long-term illness. About 66% of respondents feared being burden on family, fear of exhausting their savings (13.7%), dying (9.5%), and ending up in nursing home (6.0%)11.
To the investigators’ knowledge, there has not been similar study conducted on FoDP among chronic disease patients in Ethiopia. However, FoDP is a common health problem in our clinical experience which is often unreported. Due to non-reportable of the problem, FoDP is not identified as a problem in the planning of health in Ethiopia. Thus, this study aimed to assess FoDP and related factors among patients with chronic disease attending South Wollo zone government hospitals, Ethiopia. The findings of this study will be useful evidence to design interventions for FoDP. The finding could also add to the existing base of knowledge on FoDP in the study region.
Methods and materials
Study area, design and period
The study was conducted in South Wollo zone government hospitals. Institution-based cross-sectional study design with mixed quantitative and qualitative approaches was conducted from April 1–30, 2024.
Source population and study population
The source population were chronic disease patients who attended government hospitals found in South Wollo zone and the study population were chronic disease patients who attended selected government hospitals found in South Wollo zone during the study period.
Inclusion and exclusion criteria
Patients with chronic disease including diabetes mellitus, heart failure, hypertension, kidney disease and asthma patients whose age ≥ 18 years and patients attending outpatient clinics were included in the study. However, critical ill patients and who have hearing impairments in the study period were excluded in the study.
Sample size determination
For quantitative data, using single population proportion formula [n = (Z a/2)2P(1-P)/d2]. The assumptions were 95% level of confidence which yields Z α/2 = 1.96, 5% margin of error (d), and estimated prevalence (P) of FoDP. Prevalence of 50% was taken because to the authors’ knowledge there was no similar study done in Ethiopia. Adding 10% non-respondent rate, the final sample size was 423 chronic disease patients.
For qualitative data, the sample size was until information saturation. In-depth interview were done among 17 chronic disease patients who were not participating in quantitative data to prevent data contamination.
Sampling technique and procedure
South Wollo zone has 14 government hospitals from which 5 hospitals were selected by simple random sampling technique. Based on the number of chronic disease patients per month in each selected hospitals, the total sample size was allocated proportionally (Boru Meda hospital = 58, Akesta hospital = 84, Queen Zewditu hospital = 106, Tenta hospital = 82, Mekane Selam hospital = 93). Then, from each selected hospital, participants were selected using systematic random sampling technique every 5 interval. The first study subject was selected by lottery method.
Data collection tools
The data were collected using interviewer administered questionnaire which had six parts.
-
1.
Socio-demographic characteristics: Age, sex, marital status, residency, educational level, occupation, role in family, ethnicity and religion.
-
2.
Clinical profiles: Types of chronic disease, duration of chronic disease, presence of comorbidities, family history of chronic disease, member of community health insurance and attending chronic disease education.
-
3.
Psychosocial factors: Depression, Anxiety and Stress Scale-21 (DASS-21) were used to measure the level of depression, anxiety and stress. Each subscale has seven items. Each item has 0 to 3 responses (0 = did not apply to me at all, 1 = applied to me to some degree or some of the time, 2 = applied to me to a considerable degree or a good part of time, 3 = applied to me very much or most of the time). The scores of depression, anxiety and stress were calculated by summing each subscale items. Each subscale of DASS-21 score was multiplied by 2 to get the final each subscale score of Depression, Anxiety and Stress Scale-42 (DASS-42)19,20,21,22. Social support was measured using Oslo Social Support Scale-3 (OSSS-3) tools23,24,25.
-
4.
Behavioural factors: Current cigarettes, alcohol and chat use were assessed by preparing tools from literatures26,27,28.
-
5.
Fear of disease progression: was measured using Fear of Progression Questionnaire (FoP-Q). The FoP-Q consists of 43 items with 5 point Likert scale (1 = Never, 2 = Seldom, 3 = Sometimes, 4 = Often, 5 = Very often). The responses of positive items were reversed to sum up FoDP. The tool was reliable and valid; its internal consistency was Cronbach’s alpha > 0.72.
-
6.
In-depth interview questionnaire: For qualitative part of the study, questions were used to guide the in-depth interview.
Data collection procedure and quality control
To assure the quality of data, properly designed data collection instrument was used. English versions of instruments were translated to Amharic (local language). Five nurses as data collectors (one for each hospital) and one nurse as supervisor were selected for data collection and one day training were given for them. Pre-test was done on 5% of the total sample size at Dessie comprehensive specialized referral hospital.
Operational definitions
-
Low fear of disease progression: Patients who scored below the mean overall FoP-Q.
-
High fear of disease progression: Patients who scored the mean and above the overall FoP-Q.
-
Good social support: Patients who scored 12–14 of the total OSSS-3.
-
Moderate social support: Patients who scored 9–11 of the total OSSS-3.
-
Poor social support: Patients who scored 3–8 of the total OSSS-323,25.
-
Normal depression: Patients who scored 0–13 of the total depression subscale of DASS-21.
-
Moderate depression: Patients who scored 14–20 of the total depression subscale of DASS-21.
-
Severe depression: Patients who scored 21–42 of the total depression subscale of DASS-21.
-
Normal anxiety: Patients who scored 0–9 of the total anxiety subscale of DASS-21.
-
Moderate anxiety: Patients who scored 10–14 of the total anxiety subscale of DASS-21.
-
Severe anxiety: Patients who scored 15–42 of the total anxiety subscale of DASS-21.
-
Normal stress: Patients who scored 0–18 of the total stress subscale of DASS-21.
-
Moderate stress: Patients who scored 19–25 of the total stress subscale of DASS-21.
-
Severe stressed: Patients who scored 26–42 of the total stress subscale of DASS-21.
-
Current Cigarettes use: Patients who consumed cigarettes at least once in the past 30 days26,28.
-
Current alcohol use: Patients who consumed any alcohol at least once in the past 30 days26,27,28.
-
Current chat use: Patients who consumed chat at least once in the past 30 days26,27,28.
-
Comorbidities: Presence of additional disease other than the current illness.
Data processing and analysis
The collected data were entered into epidata 3.1 and export to SPSS version 23 for analysis. Frequencies, percentages, mean and standard deviation (SD) were done and displayed in the form of texts, tables and graphs. Bivariable logistic regression analysis was done to see the crude association between independent and outcome variables. Then, multivariable logistic regression analysis was conducted by selecting variables with p-value of < 0.2 in bivariable analysis. In multivariable analysis, significant association was declared at p-value of < 0.05. The qualitative data were gathered through an in-depth interview and it was recorded. The Amharic recorded data were translated to English text and the results were presented in narration form under selected themes.
Results
Socio-demographic characteristics
In quantitative study, out of the total sample size (n = 423), 411 patients with chronic disease participated in the interview that gave 97.16% response rate. Among 411 patients, more than half of the participants 223(54.3%) were males. The mean age of respondents was 48.10 ± 16.214 SD with minimum and maximum age of 18 and 87 years, respectively. Two third of the participants, 283(68.9%) were married and 225(54.7%) live in the rural area (Table 1).
Clinical profile of respondents
Of all patients, 155(37.7%), 122(29.7%) and 72(17.5%) were hypertension, diabetes mellitus and hear failure, respectively. Among participants, 56(13.6%) patients have been living with their disease for more than ten years and majority of the participants, 236(57.4%) had duration of their chronic disease less than or equal to 5 years. One fourth of participants, 99(24.1%) had other co-morbidities in addition to their current disease (Table 2).
Psychosocial and behavioural characteristics of respondents
With regard to psychosocial characteristics of the participants, 55(13.4%) and 60(14.6%) of patients had severe and moderate depression, respectively. Furthermore, 70(17.0%) and 40(9.7%) of patients had severe anxiety and stress, respectively. One third, 143(34.8%) of patients had good social support whereas 149(36.3%) of them had poor social support. On the other hand with regard to behavioural characteristics, 15(3.6%), 47(11.4%) and 133(32.4%) of patients were use cigarettes, alcohol and chat, respectively (Table 3).
Fear of disease progression
In the FoP-Q, the minimum and maximum score were 72 and 172 out of 215 respectively with the mean score of 110.06 (SD: 19.069). Regarding to the item that I am worried that at some point in time, because of my illness I will no longer be able to pursue my hobbies, 168(40.9%) participants respond sometimes while none of them respond very often. To that of I am successful in dealing with my fears, 30(7.3%), 93(22.6%), 152(37.0%), 121(29.4%) and 15(3.6%) found being never, seldom, sometimes, often and very often, respectively.
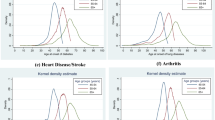
Over one third of patients, 151(36.7%) said sometimes and 122(29.7%) said often to the item of that I am afraid of pain. One hundred sixteen patients (28.2%) said often with the statement that due to worrying about my health I have a sleep disturbance (Supplementary Table S1). Overall, in this study 168(40.9%) (95% CI = 36.3–45.7) of patients with chronic disease had high FoDP and 243(59.1%) (95% CI = 54.3–63.7) of them had low FoDP (Fig. 1).

Overall Fear of Disease Progression of respondents.
Factors associated with fear of disease progression
Among 20 variables in bivariable logistic regression analysis, 15 variables namely age, sex, residency, role in family, type of patients’ chronic disease, duration of chronic disease, presence of comorbidities, family history of chronic disease, member of community health insurance, attending health education, social support, current chat use, depression, anxiety and stress were candidate variables for multivariable logistic regression at a p-value < 0.2. Among 15 variables which were entered to multivariable logistic regression analysis, 7 variables namely type of patients’ chronic disease, presence of comorbidities, attending health education, social support, current chat use, depression and anxiety were significantly associated with outcome variable at p-value of < 0.05.
Patients with heart failure were 4 times more likely to have high FoDP than those patients with asthma disease (AOR = 3.950; 95% CI = 1.139–13.697; P-value = 0.030). Patients with other comorbidity in addition to the current chronic disease were 2.4 times more likely to have high FoDP than those with no comorbidity (AOR = 2.411; 95% CI = 1.270–4.575, P-value = 0.007). Patients who did not attend health education about their chronic disease were 4 times more likely to have high FoDP than those who attended health education (AOR = 4.147; 95% CI = 12.438–7.052; P-value = 0.000). Patients having poor social support were 2.3 times more likely to have high FoDP than those having good social support (AOR = 2.339; 95% CI = 1.272–4.300.272.300; P-value = 0.006).
Patients with chronic disease who use chat currently were 3 times more likely to have high FoDP than those who do not use chat (AOR = 3.166; 95% CI = 1.813–5.530; P-value = 0.000). Patients with severe depression were 4 times more likely to have high FoDP than patients with normal depression (AOR = 4.043; 95% CI = 1.602–10.202; P-value = 0.003). In the same way, patients with severe anxiety (AOR = 2.440; 95% CI = 1.082–5.504; P-value = 0.032) and moderate anxiety (AOR = 2.417; 95% CI = 1.119–5.218; P-value = 0.025) were 2.4 times more likely to have high FoDP than patients with normal anxiety (Table 4).
The result of In-depth interviews
Qualitative data were conducted from 17 patients with chronic disease using in-depth interview. Among these, six of them were hypertension and four of them were diabetes mellitus patients. Regarding sex, 9 of them were males. (Table 5).
Organization of themes
The data were organized into 3 themes.
Theme one: factors related to fear of disease progression
Depending on the type of chronic diseases, the participants explained that sweet foods, heavy work, improper use of medication, afraid of death, stress of living conditions, shortness of breath and fatigue manifestation, afraid of comorbidities, absence of social support, drug resistance, thinking about children and depression were considered as factors related to FoDP.
Informant 1 stated about the factors related to FoDP was that “I use sweet foods which increase my blood glucose level. On the other hand, when I do heavy work my blood glucose level decreased; manifested by excessive sweating and blurred vision. Due to these increased and decreased blood glucose levels, I fear my diabetes going on bad progression”. Informant 4 also stated that “I do not take my medication properly as physician order because I do not hold my drug when I go to another place. When I think this improper uses of medication, I fear my disease progression”.
Informant 2 stated that “I have shortness of breath and cough when my asthma aggravates by cold environment and other factors like animal dander, dust and pollen. When I think the exacerbations of my asthma, I feel fear of my disease progression or recurrence”. Informant 3 said that “I highly fear my disease progression because I have children who are depending on me. When I think about my children, I fear the progression of my disease. For me I don’t fear either the disease killed me or not”.
Informant 5 stated that “Increasing of my blood pressure, cost of living conditions and afraid of death make me to fear the progression of my disease. My blood pressure fluctuation meaning sometime I have a raised blood pressure and sometimes I have normal level of blood pressure, again a raised level of blood pressure. I am poor in my living so that I have difficulty to buy my hypertensive drug and educate my children because my income and cost of living is unbalanced. All these uncomfortable conditions make me to have stress and to fear the progression of my hypertension disease”.
Informant 6 said that “I did not take care for myself and I develop infected wound in my right foot after little trauma. I took wound medication orally but my wound could not be cured. The wound become big and the doctor told me that the reason why the wound does not heal is that I can’t control my blood glucose because I do not take my diabetes medications correctly. The doctor told me that unless I control my blood glucose and the wound heals, the probability of my leg amputation will be high. Recently, I fear the bad progression of my wound that leads to amputation”.
Informant 7 said that “I am living with hypertension for the last nine years with treatment. In this week, I was investigated for kidney disease because my doctor suspects kidney disease because I have low level of urine output and drowsiness. After the investigation, the doctor told me that I have renal failure but he said that it needs further investigation. This additional comorbid disease makes me to fear my disease progression of both hypertension and the new kidney disease. Especially, I fear my kidney disease because I know a person who is on dialysis three times per week for renal failure”.
Informant 9 stated that “I heard from other asthmatic patient about drug resistance. One person told me that his medication was treating him properly when he started the treatment. However, he said that through time his medication not treat him properly. He said that this is due drug resistance. Due to this, I fear the progression of my asthma disease to severe stage after a time like other person”.
Informant 8 said that “My husband died in last year and I have only one son who is living in far area and it is difficult to get support from neighbours. No one support me when I become ill. Because of this lack of social support, I fear the progression of my disease because no one helps me when I have severe manifestation of my disease”.
Similarly, informant 10 stated that “After the death of my wife I live alone and the cost of living as well as buying medication is very expensive. In addition, I fear the progression of my disease because I experience shortness of breath and fatigue when my illness becomes worse. So now, I feel depression due to the stated problems. I do not feel any positive feeling at all and I feel that life is meaningless”.
Theme two: solutions for fear of disease progression
The study participants explained that the solutions to reduce FoDP were taking medication correctly, reduce salt and alcohol, do exercise, eat fruits and keeping from cold weather. Others said that avoid factors like bad odour, dust and harmful substances such as chat and cigarettes. However, other participants didn’t know the solutions and another also had misconceptions.
Informant 4 said that “to reduce fear of disease progression, it is better to reduce salt intake because nurse educate me to reduce my salt intake in order to control raised blood pressure level”. Informant 5 also explained that “Avoid or reducing dietary salt intake and limit alcohol consumption are important. The health professionals advised me to eat fruits, vegetables and low-fat dietary products. They also educated me the importance of regular exercise to decrease my hypertension”.
In contrast, Informant 11 had misconception practice; he stated that “By using sharp material like blade the traditional healer penetrates my head blood vessel when I have severe headache to remove blood from the body in order to decrease my blood pressure and headache”. Informant 12 also stated that “I don’t know the solutions to solve fear of disease progression, I came to your health facility so that please tell me the solutions”.
Informant 6 stated that “To decrease fear of disease progression, it is better to take ordered medication properly. If we take diabetes medication correctly the disease progression will be delayed. The health professional educated us by saying if we are not taking medications properly, complication will be present recently like kidney disease, blindness, heart disease and nerve disease”.
Informant 2 elaborates that “The solutions for fear of disease progression are keeping from animal dander smell, flower pollen and dusts. As much as possible wear clothes which prevents from cold weather condition. Stay at home in the morning and evening time also prevents from coughing”. On the other hand informant 13 stated that “To reduce fear of disease progression it is better to avoid harmful substance like chat, tobacco and large amount of alcohol consumptions. Taking of harmful substances is not good for any person health”.
Theme three: challenges to solve fear of disease progression
With regard to the challenges to solve FoDP, the study participants explained that distance of living areas from the hospitals, disease management is not comfortable with farm work, difficulty of getting medication when there is war and absence of medication in the government hospitals.
Informant 11 stated that “I am living in far areas from the hospital. For me it is challenge to attend my follow up in the health facility and it is impossible to get frequent counselling from the health care professionals. In addition, I am a farmer so that it is difficult to manage my disease with my farm work”.
Informant 9 said that “When there is war due to political issues in our country, it is very challenge to get medications. Example when there was war between federal government of Ethiopia and Tigray defence force, it was very difficult for me to get my asthmatic medications. If that war continued, I would be died and you cannot get me now”.
Informant 10 explained that “In this government hospital, there is no medication. Mostly, health professionals in this hospital said that we have no drugs and they sent me to buy my heart disease medication in private pharmacy. In private pharmacy the cost of drugs are very expensive. Sometimes, I went to my house without buying my medication when I have not enough money. Due to this, I worried because my disease becomes severe and severe from day to day. So this is the great challenge for me to solve my fear of disease progression”. Similarly, informant 15 said that “I buy medication in private pharmacy which is found in front of this hospital because my medication does not found in this government hospital”.
Discussion
FoDP is a crucial concern health problem. Investigating FoDP and associated factors among patients with chronic disease are needed to design appropriate plan and interventions. In this study, the overall finding revealed that 40.9% (95% CI = 36.3–45.7) of patients with chronic disease had high FoDP. This finding was higher than studies done in Netherland (18%)7 and among cancer patients (26.07%)18. The possible explanation for this difference may be due to the difference in the study design used, variation in socio-demographic characteristics, presence of variation in data collection periods and difference in level of patients’ care across various settings.
Among factors patients with heart failure, presence of comorbidities, not attending health education, poor social support, current chat use, severe depression, moderate anxiety and severer anxiety were significantly associated with high FoDP. Patients with heart failure were more likely to have high FoDP than those patients with asthma disease. This might be explained by heart is the main organ of our body where its disease is characterized by the inability of the myocardium to pump enough blood to meet the needs of the body for oxygen and nutrients. When oxygen and nutrient shortage are present, overall body system will be disturbed which may end up with high FoDP for patients with heart disease29,30.
Patients may also have high fear when they think about their family as their disease become worse18,31. This finding was supported by the qualitative component of this study where heart failure female patient had fear of disease progression because she had children who are depend on her. This indicates that health professionals should be able to identify patients need suffered by heart disease to provide counselling services for fears of cardiac disease progression and related consequences32.
Patients with comorbidities were more likely to have high FoDP than those with no comorbidities. This might be due to the fact that when the patients had more than one chronic disease, the burden of the diseases including deterioration of quality of life, money expense, inability to work and disability will be high on the patients33,34. This high burden will have high FoDP on the patients’ side.
Patients who did not attend health education about their chronic disease were more likely to have high FoDP than those who attended health education. This indicates that not attending health education about chronic disease may contribute for high FoDP because they do not get psychological support from heath care workers.
On the other hand, those patients who took health education can get advices how they control their disease, importance of taking medication properly and life style modifications35,36. This was supported in the qualitative part of the study; where taking ordered medication properly is important to decrease FoDP which was recognised by a known diabetes patient. She understands the importance of education for patients by health professionals to decrease complications of the disease like kidney disease, blindness, heart disease and nerve disease. A hypertension patient also explained the importance of fruits, vegetables, low-fat dietary products, regular exercise, salt restriction and limit alcohol consumption to decrease raised blood pressure.
Patients having poor social support were more likely to have high FoDP than those having good social support. This was supported with qualitative finding, a kidney disease female patient knows the importance of social support to decrease FoDP by stating no one support her when she became ill after her husband was died and she has only one son who is not living with her so that she has FoDP when she has sever manifestation of her disease.
Patients with chronic disease who chew chat currently were more likely to have high FoDP than those who did not practice chat chewing. The qualitative part of this study also revealed that avoiding harmful substance like chat, tobacco and large amount of alcohol consumptions are necessary to decrease FoDP. However, tobacco and alcohol consumptions were not significantly associated with high FoDP in quantitative part of this study.
Patients with severe depression and anxiety were significantly associated with high FoDP by comparing patients with normal depression and normal anxiety, respectively. This was congruent with other studies where FoDP had significant relation with depression and anxiety7,16,17,37. Other study also revealed that higher depression was significant predictors for fear of cancer recurrence38. The qualitative part of the study also showed that patient developed depression due to death of loved ones, cost of living and expensiveness of buying medications which end ups with fear of disease progression especially when the patient experienced shortness of breath and fatigue.
In this study, various variables had no significantly associated with high FoDP. Age, sex, marital status, educational level and occupation had no significantly associated with high FoDP. This was similar with other study7. However, in other study being married and female gender were significantly associated with fear of cancer recurrence38. Another study also showed that the fear of having a long-term illness had not significant association with sex, residency and age11. Similarly, in this study stress level of patients had no significant association with FoDP. This was contradicts with other studies where significant relationships were found between FoDP and stress17,37.
Strengths of the study
-
Conducted by using mixed quantitative and qualitative approach.
-
Used standardized questionnaires to assess FoDP.
-
High response rate.
-
To the authors’ knowledge, since there was no similar study conducted in Ethiopia, it can contribute a lot as baseline information.
Limitations of the study
-
Face-to-face interview which may lead to social desirability bias by overestimate or under estimate of the results.
-
Since the study design was cross-sectional, the direction of relationship between variables could not always be determined.
Conclusion
Significant proportion of patients with chronic disease had high FoDP. Patients with heart failure, presence of comorbidities, not attending health education, poor social support, current chat use, severe depression, moderate anxiety and severe anxiety were significantly associated with high FoDP. In qualitative part of this study, participants were explained that sweet foods, heavy work, improper use of medication, afraid of death, stress living conditions, shortness of breath and fatigue manifestation, afraid of comorbidities, absence of social support, drug resistance, thinking about children and depression were considered as reasons for FoDP.
Therefore, policy makers, hospital managers, health professionals and community need to give more attentions especially for those patients with the identified significant associated factors to reduce high fear of disease progression. Next researchers need to focus to get clear information about FoDP for a particular disease.
Data availability
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AOR:
-
Adjusted Odds Ratio
- CI:
-
Confidence Interval
- COR:
-
Crude Odds Ratio
- DASS-21:
-
Depression, Anxiety and Stress Scale − 21
- DASS-42:
-
Depression, Anxiety and Stress Scale − 42
- FoDP:
-
Fear of Disease Progression
- FoP-Q:
-
Fear of Progression Questionnaire
- OSSS-3:
-
Oslo Social Support Scale − 3
- SD:
-
standard deviation
- SPSS:
-
Statistical Package for Social Sciences
References
Dankert, A. et al. Progredienzangst Bei patienten Mit Tumorerkrankungen, diabetes mellitus und entzündlich-rheumatischen erkrankungen. Die Rehabilit. 42 (03), 155–163 (2003).
Herschbach, P. et al. Fear of progression in chronic diseases: psychometric properties of the fear of progression questionnaire. J. Psychosom. Res. 58 (6), 505–511 (2005).
Maheu, C., Lebel, S., Tomei, C., Singh, M. & Esplen, M. J. Breast and ovarian cancer survivors’ experience of participating in a cognitive-existential group intervention addressing fear of cancer recurrence. Eur. J. Oncol. Nurs. 19 (4), 433–440 (2015).
Herschbach, P. & Dinkel, A. Fear of progression. Recent Results Cancer Res 197, 11–29 https://doi.org/10.1007/978-3-642-40187-9_2 (2014).
Dinkel, A. & Herschbach, P. Fear of progression in cancer patients and survivors. Recent Results Cancer Res. 210, 13–33. https://doi.org/10.1007/978-3-319-64310-6_2. (2018).
Herschbach, P. et al. Group psychotherapy of dysfunctional fear of progression in patients with chronic arthritis or cancer. Psychother. Psychosom. 79 (1), 31–38 (2009).
Custers, J. A. et al. Fear of disease progression in carriers of the m. 3243A > G mutation. Orphanet J. Rare Dis. 13 (1), 1–6 (2018).
Berg, P. et al. Fear of progression in chronic diseases. Psychother. Psychosom. Med. Psychol. 61 (1), 32–37 (2010).
Lebel, S. et al. Health anxiety and illness-related fears across diverse chronic illnesses: a systematic review on conceptualization, measurement, prevalence, course, and correlates. Plos One. 15 (7), e0234124 (2020).
Nielsen, J. et al. The role of wisdom and self-management skills for coping with fear of progression among patients with multiple sclerosis with moderate disability: results from a cross-sectional study. J. Affect. Disorders Rep. 8, 100311 (2022).
Awang, H., Mansor, N., Nai Peng, T. & Nik Osman, N. A. Understanding ageing: fear of chronic diseases later in life. J. Int. Med. Res. 46 (1), 175–184 (2018).
Ponikowski, P. et al. Heart failure: preventing disease and death worldwide. ESC Heart Fail. 1 (1), 4–25 (2014).
Laditka, J. N. et al. Older adults’ concerns about cognitive health: commonalities and differences among six united States ethnic groups. Ageing Soc. 31 (7), 1202–1228 (2011).
Laditka, S. B. et al. How do older people describe others with cognitive impairment? A multiethnic study in the united States. Ageing Soc. 33 (3), 369–392 (2013).
Gossec, L. et al. THU0575 the Most Frequent Fears and Beliefs of 226 Patients with Rheumatoid Arthritis or Spondyloarthritis, Using a Novel Questionnaire (BMJ Publishing Group Ltd, 2015).
Zimmermann, T., Herschbach, P., Wessarges, M. & Heinrichs, N. Fear of progression in partners of chronically ill patients. Behav. Med. 37 (3), 95–104 (2011).
Manafi, S. F. & Dehshiri, G. Fear of disease progression in patients with cancer and multiple sclerosis and its relation to emotional problems. Health Psychol. 6 (22), 115–130 (2017).
Bonkalo, T. I., Veprentsova, S. Y., Nikitina, N., Gardanova, Z. R. & Ilgov, V. I. Factors of the development of fear of disease progression in patients with breast cancer. Open. Access. Macedonian J. Med. Sci. 8 (E), 74–80 (2020).
Lovibond, P. F. & Lovibond, S. H. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav. Res. Ther. 33 (3), 335–343 (1995).
Antony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W. & Swinson, R. P. Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychol. Assess. 10 (2), 176 (1998).
Ho, C. S., Tan, E. L., Ho, R. C. & Chiu, M. Y. Relationship of anxiety and depression with respiratory symptoms: comparison between depressed and non-depressed smokers in Singapore. Int. J. Environ. Res. Public Health. 16 (1), 163 (2019).
Addis, S. G., Nega, A. D. & Miretu, D. G. Depression, anxiety and stress levels among chronic disease patients during COVID-19 pandemic in Dessie town hospitals, Ethiopia. Open. Psychol. J. ;14(1), 249–57. (2021).
Bøen, H., Dalgard, O. S. & Bjertness, E. The importance of social support in the associations between psychological distress and somatic health problems and socio-economic factors among older adults living at home: a cross sectional study. BMC Geriatr. 12 (1), 1–12 (2012).
Dalgard, O. S. et al. Negative life events, social support and gender difference in depression: a multinational community survey with data from the ODIN study. Soc. Psychiatry Psychiatr. Epidemiol. 41, 444–451 (2006).
Kocalevent, R-D. et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. 6 (1), 1–8 (2018).
Tesfaye, G., Derese, A. & Hambisa, M. T. Substance use and associated factors among university students in ethiopia: a cross-sectional study. J. Addict. ;2014, 969837 https://doi.org/10.1155/2014/969837 (2014).
Kassa, A., Wakgari, N. & Taddesse, F. Determinants of alcohol use and Khat chewing among Hawassa university students, ethiopia: a cross sectional study. Afr. Health Sci. 16 (3), 822–830 (2016).
Aklog, T., Tiruneh, G. & Tsegay, G. Assessment of substance abuse and associated factors among students of Debre Markos Poly technique college in Debre Markos town, East Gojjam Zone, Amhara regional State, Ethiopia, 2013. Global J. Med. Res. 13 (4), 1 (2013).
Amran, M. S., Bahar, N. B. & Akash, S. Physiology and Pathology of the Cardiovascular System (IntechOpen, 2022).
Zhou, Z. et al. Cardiovascular Disease p. 583–594 (Springer, 2021).
Pattenden, J., Roberts, H. & Lewin, R. Living with heart failure; patient and carer perspectives. Eur. J. Cardiovasc. Nurs. 6 (4), 273–279 (2007).
Clarke, S. T., Le Grande, M., Murphy, B. M., Hester, R. & Jackson, A. C. Protocol for the Development and Validation of a Clinical Measurement Tool for Fear of Disease Progression and Recurrence in Cardiac Patients (Chronic Diseases and Translational Medicine, 2024).
Hajat, C. & Stein, E. The global burden of multiple chronic conditions: a narrative review. Prev. Med. Rep. 12, 284–293 (2018).
Klijs, B., Nusselder, W. J., Looman, C. W. & Mackenbach, J. P. Contribution of chronic disease to the burden of disability. PLoS One. 6 (9), e25325 (2011).
Farley, H. Promoting self-efficacy in patients with chronic disease beyond traditional education: A literature review. Nurs. open. 7 (1), 30–41 (2020).
Fortin, M., Chouinard, M-C., Diallo, B. B. & Bouhali, T. Integration of chronic disease prevention and management services into primary care (PR1MaC): findings from an embedded qualitative study. BMC Fam. Pract. 20 (1), 1–8 (2019).
Yang, Y. et al. Factors associated with fear of progression in Chinese cancer patients: sociodemographic, clinical and psychological variables. J. Psychosom. Res. 114, 18–24 (2018).
Sarkar, S. et al. Fear of recurrence and its impact on quality of life in patients with hematological cancers in the course of allogeneic hematopoietic SCT. Bone Marrow Transplant. 49 (9), 1217–1222 (2014).
Acknowledgements
Authors would like to acknowledge Wollo University for financial support of this research. We would also acknowledge hospital administrators, data collectors, supervisors and the study participants for their valuable contribution in the study.
Funding
The study was financially supported by Wollo University. This University reviewed and approved the concept of the study to be conducted but had no role in the study design, data collection, analysis and interpretations of data.
Author information
Authors and Affiliations
Contributions
SGA contributed to conceptualization, formal analysis, interpretation of data and writing original draft. AD and DG contributed to data collection, interpretation of data, and review and editing. MG and MZ contributed to interpretation of data and review and editing. DH, ABN and ATA participated in the formal analysis, conducted literature review and supervision. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethical clearance was obtained from Wollo University College of medicine and health science research ethical review committee and its reference number was CMHS 712/20/15. The study was performed in accordance with principles of the Declaration of Helsinki. Written informed consent was obtained from all eligible study participants after information was provided about the purpose of the study, confidentiality of the data and non-invasiveness of the data collection procedure.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Addis, S.G., Dires, A., Goshiye, D. et al. Fear of disease progression and related factors among chronic disease patients attending South Wollo zone government hospitals. Sci Rep 16, 140 (2026). https://doi.org/10.1038/s41598-025-28868-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-28868-9
