
Abstract
Oral health is a significant contributor to public health and a basic determinant of general health. As Egypt shows high prevalence of oral diseases, the aim of this study is to assess the oral health knowledge, attitudes and behaviors (KAB) among Egyptian adults. The study also correlates the KAB of the participants with their dental habits, caries experience and sociodemographic characteristics. A cross-sectional survey with non-probability convenience sampling was performed in a dental school hospital in Egypt. The Hiroshima University - Dental Behavioral Inventory (HU-DBI) by Kawamura was used to assess the KAB, the survey also included questions about sociodemographic data and dental habits of the participants. In addition, a DMFT index was used to assess the caries experience. Continuous data was explored for normality using Kolmogrov Smirnov test and Shapiro Wilktest. Correlation between age, DMF, KAB and HU-DBI index was performed using spearman’s correlation. Association between categorical data and HU-DBI index was performed using the Chi-Square test. Significance level was set at P ≤ 0.05 and all tests were two tailed. The study participants demonstrated fair HU-DBI score. Knowledge (r = 0.70), attitudes (r = 0.59) and behaviors (r = 0.47) had strong positive correlation with the HU-DBI score. The DMFT score showed a moderate negative correlation (r=-0.35) with the overall HU DBI score. In addition, age showed a weak negative correlation (r=-0.29) with HU DBI score. The dental habits and sociodemographic characteristics showed statistically significant effect on the overall HU-DBI score, with the exception for mouth wash use, gender, health status and smoking status which showed no significant effect. Adult patients in Egypt demonstrate fair oral health knowledge and attitude and poor oral health behaviors, in addition to high caries index. We recommend planning and implementing oral health programs to enhance the oral health of adults in Egypt.
Clinical trial number: The protocol of the study is registered with ClinicalTrials.gov Identifier: NCT06689202.
Similar content being viewed by others

Introduction
Oral health is a significant contributor to public health, and a basic determinant of an individual’s general health and quality of life1,2. Moreover, oral health is classified by the World Health Organization (WHO) as a major global health concern3. Notably, one in two adults suffer from dental decay, with oral diseases ranking among the most prevalent non-communicable diseases (NCDs)4. The global oral health status report shows that Egypt is among the countries with the highest prevalence of oral diseases in the Middle East and North Africa5.
Oral health professionals have a crucial role in influencing the behaviours of their patients and preventing oral diseases6. Thus, public health programs focus on prevention rather than treatment of dental diseases through modifying the lifestyle factors of the individuals such as improving their oral hygiene practices and promoting better dietary habits7,8. Also, effective prevention depends on enhancing oral health knowledge which is essential for positive health behaviours and better oral health outcomes9.
Oral health education and promotion programs have successfully improved oral health outcomes, positively influencing dental visits, attitudes, and oral hygiene practices such as brushing and flossing10. However, public health programs require a thorough assessment of the target population’s oral health knowledge, attitudes and behaviours. In addition, those programs must consider the sociodemographic factors of the individuals, along with their dental visiting habits which affect their oral health11,12.
To the best of our knowledge there is a research gap in the assessment of the oral health knowledge, attitudes and behaviours (KAB) of adult patients in Egypt. Thus, the aim of this study is to assess the KAB of adult patients attending the diagnostic center at a dental school in Egypt. The study will also assess dental habits and measure the mean number of decayed, missing, and filled Permanent Teeth (DMFT scores) to assess the participants’ caries experience. Finally, the KAB scores will be correlated with the dental habits, DMFT scores and sociodemographic variables of the participants.
Methods
Study design and recruitment of participants
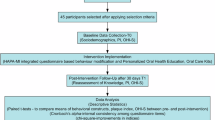
A cross-sectional survey with non-probability convenience sampling was conducted in the diagnostic center of the School of Dentistry in one of the Egyptian universities. The research protocol was approved by the Research Ethics Committee of School of Dentistry, Newgiza University (approval date: 17 December 2024). All research was performed in accordance with the ethical principles outlined in the 2013 revision of the Declaration of Helsinki. The protocol of the study is registered with ClinicalTrials.gov Identifier: NCT06689202. The study included adult patients (18 years or older) with adequate cognitive ability who agreed to participate in the study and signed an informed consent.
Sample size calculation
According to the results of Al-wesabi et al. 201913, the standard deviation of HU-DBI index in Egypt was 1.73. Based on the equation \(\:\frac{{{Z}_{1-\alpha\:/2}}^{2}\:{SD}^{2}}{{d}^{2}}\:\)by Charan et al. in 201314, precision of 0.2 and by adopting an alpha (α) level of 0.05 (5%), power = 80%, the predicted sample size (n) was a total of 288 participants. The sample size was calculated using statistics kingdom sample size calculator (https://www.statskingdom.com/50_ci_sample_size.html).
Methods of assessment
The Hiroshima University - Dental Behavioral Inventory (HU-DBI) by Kawamura was used as a validated instrument to assess oral health-related knowledge, attitudes, and behaviours (KAB) among participants (Table 1)15,16. The Arabic version of the HU-DBI questionnaire was validated and cross-culturally adapted, showing almost perfect reliability and validity17. The assessment included 20 HU-DBI items, which employed a dichotomous response format (agree/disagree) and related to oral and dental health, as well as tooth brushing habits. However, only 12 items in bold font (Questions 2, 4, 6, 8, 9, 10, 11, 12, 14, 15, 16, and 19) were used to calculate the overall KAB score. The scores ranged from 0 to 12, with higher scores indicating better oral health KAB13,18.
The knowledge (K) index score, is derived from items 2, 8, 10, 15, and 19, the attitude (A) index score is derived from items 6, 11, and 14, and the behavior (B) index score is determined from items 4, 9, 12, and 16. One point was given for answering “Agree” to items 4, 9, 11, 12, 16, and 19, while one point was given for answering “Disagree” to items 2, 6, 8, 10, 14, and 15. Questions 1, 3, 5, 7, 13, 17, 18, and 20 are considered dummy items and are not included in the KAB score. These dummy items serve as a strategic tool in questionnaire design to enhance the quality and reliability of the collected data by mitigating biases and encouraging more accurate and authentic responses13,18.
The overall HU-DBI score can be interpreted as follows: a score of 0–4 (poor), 5–8 (fair), and 9–12 (good), with 12 being the maximum possible score. In addition, the Knowledge (K) index score, can be interpreted as follows: a score of 0–1 (poor), 2–3 (fair), and 4–5 (good), with 5 being the maximum possible score. Furthermore, the attitude (A) index score can be interpreted as follows: a score of 0 (poor), 1–2 (fair), and 3 (good), with 3 being the maximum possible score. Finally, the behavior (B) index score can be interpreted as follows: a score of 0–1 (poor), 2–3 (fair), and 4 (good), with 4 being the maximum possible score.
Additionally, the questionnaire included questions about sociodemographic data and dental habits to correlate these factors with other outcomes (Appendix 1). DMFT index19 was used to clinically determine the number of decayed (D), missed (M), filled (F) teeth (T) of the participants on the same day of the questionnaire (Appendix 2).
Statistical analysis
The identity of the patients was kept anonymous, and the data was saved and tabulated on shared folders for back up. Statistical analysis was performed using Medcalc software, version 22 for windows (MedCalc Software Ltd, Ostend, Belgium). Continuous data were tested for normality using the Kolmogrov Smirnov and Shapiro Wilk tests and since the distribution was non-parametric, the results were presented as mean, standard deviation (SD), median, minimum and maximum. Categorical and binary data were presented as frequency and percentage. Correlation between age, DMFT, KAB and HU-DBI score was performed using spearman’s correlation. Association between categorical data and HU-DBI score was performed using the Chi-Square test. Significance level was set at P ≤ 0.05 and all tests were two tailed.
Results
Sociodemographic characteristics of the participants
Data were collected from 288 participants with a response rate of 90%. The mean age of the participants was 32.6 years ± 11.62 ranging from 17 to 72 years. As presented in Table 2 most of the participants (75%) were females while 25% were males. In addition, about half of the participants (45.8%) received higher education, while about 11% did not receive any form of education. Also, more than 60% of the participants resided in urban areas and almost half of the participants were employed (51.2%), 38.5% were unemployed or retired and the rest of the participants (10.1%) were students. Additionally, most of the participants demonstrated no systemic diseases and never smoked, however more than half of the participants (56.6%) did not have any form of insurance (private or public).
Dental habits and oral hygiene practices
Table 2 shows that most participants (77.8%) reported visiting the dental clinic only when experiencing pain. However, the remaining participants visited the dentist every six months (12.2%), annually (5.5%) or had their first dental visit on the day of the questionnaire (4.5%). In addition, on the day of the questionnaire, half of the participants (50.7%) visited the dental clinics for a dental checkup, while the remaining participants attended due to pain (36.5%) or were undergoing treatment (12.8%). More than half of the participants (55.9%) reported using fluoride toothpaste daily, however only a third (30.2%) reported brushing their teeth twice a day. On the other hand, daily flossing and mouthwash use were uncommon among the participants with 85.4% not flossing and 91% not using mouthwash.
Correlations between KAB (HU-DBI) scores and DMFT, dental habits, and sociodemographic variables
The HU-DBI scores among the participants ranged from 1 to 12, with a mean of 5.69 ± 1.80 showing a fair overall score. Additionally, the individual components knowledge and attitudes showed fair mean scores of 2.18 ± 1.09, 1.55 ± 0.96 respectively, while behaviors showed poor mean score of 1.95 ± 0.81 (Table 3). Table 3 also demonstrates the positive correlations between these components and the overall HU-DBI score, where knowledge had the strongest correlation (r = 0.70), followed by attitudes (r = 0.59) and behaviors (r = 0.47) all indicating strong positive correlation20. These correlations are illustrated in Fig. 1, which visually displays the strength of association between the HU-DBI components and the overall score. Furthermore, the mean DMFT score of the participants was 6.40 ± 5.30 indicating a high caries index21 and the DMFT score showed a moderate negative correlation (r=-0.35) with the overall HU-DBI score (Table 3).

Box plot of HU-DBI total scores and subcomponents (knowledge, attitude, and behavior).
In terms of oral hygiene and dental habits, several factors demonstrated a statistically significant association with HU-DBI scores as presented in Table 2. Participants who reported visiting the dentist regularly every six months had higher median HU-DBI scores (7(4–12)) than those who visited annually (6.5 (5–9)), only when on pain (5(1–10)) or never (6 (4–9)). Similarly, those who visited the clinic on the day of the questionnaire for a routine checkup (50.7%) had higher median scores compared to those who came for ongoing treatment or due to pain. Additionally, participants who used fluoride toothpaste daily (55.9%) and those who practiced daily flossing (14.6%) demonstrated higher median HU-DBI scores compared to those who did not use fluoride toothpaste daily or floss respectively. However, the use of mouth wash (P = 0.51) did not demonstrate a statistically significant effect.
Age showed a weak negative correlation (r = −0.29) with the overall HU DBI score (Table 3). As shown in Table 2, most sociodemographic variables were significantly associated with HU-DBI score. Participants with higher levels of education (45.8%) had the highest median HU-DBI scores among the different education categories. Similarly, participants who lived in urban areas (63.9%) had higher median HU-DBI scores compared to those who lived in rural areas, reflecting higher knowledge, attitude and behavior towards oral health. Among the different occupation groups, participants working in education and research, as well as those in technology and IT jobs had higher median HU-DBI scores, students also showed high scores. In addition, participants with private insurance had higher median HU DBI scores compared to those with public or with no insurance suggesting better oral health awareness and behaviors. In contrast, gender (P = 0.17), health status (P = 0.06), and smoking status (P = 0.96) showed statistically insignificant effect on the HU-DBI score.
Discussion
The results of the study showed that the participants demonstrated fair knowledge, attitudes and poor behaviors towards oral health, reflected by an overall fair HU-DBI score. Knowledge (r = 0.70), attitude (r = 0.59) and behavior (r = 0.47) had a strong positive correlation with the HU-DBI scores. Knowledge exhibited the strongest positive correlation and made the greatest contribution to the overall score. Additionally, the participants had a high caries index as indicated by their mean DMF score (6.40 ± 5.30), which is comparable to the national average DMFT score (5.5 ± 5.7) reported in a population-based survey of Egyptian adults22. The sociodemographic and behavioral factors showed statistically significant effect on the overall HU-DBI score, with the exception of gender, health status and smoking status and the use of mouthwash which showed no significant effect.
The fair level of oral health knowledge among the participants is consistent with previous studies among Egyptian parents23 and older adults24. In addition, consistent with our results, unsatisfactory oral health behaviors were reported among Egyptian mothers25 and older adults24. These unsatisfactory findings highlight the need for oral health education initiatives that promote preventive practices of oral diseases26. On the other hand, satisfactory levels of oral health knowledge and behaviors among Egyptian parents were reported in another study27. This discrepancy can be explained by the different background and sociodemographic characteristics of the participants in both studies.
More acceptable levels of oral health knowledge and behaviors were reported by a study conducted among adults in the United Arab Emirates (UAE)28.This can be explained by the lower rates of daily oral hygiene practices in our study, where only 30.2% of the participants brushed their teeth twice daily compared to 79% of the UAE study. Additionally, only 14.6% of our participants reported daily flossing compared to 45% in the other study. Furthermore, UAE is a high-income country whereas Egypt is a middle lower income country, which explains the role of the income as an enabler to oral health29.This observation aligns with previous research which indicates the association between lower-income levels and inadequate levels of oral health knowledge due to limited access to dental education30.
In addition, receiving higher levels of education was associated with higher HU-DBI scores, which aligns with the literature indicating that oral health literacy and behaviors are positively correlated with higher education levels28,31,32. This relationship highlights the crucial role of education in improving the oral health awareness33. Similarly, younger participants, particularly students, demonstrated better KAB, explaining the weak negative correlation between age and HU-DBI scores. The negative correlation suggests that younger participants tend to have higher scores. This reflects increased awareness among younger educated groups, as indicated in another study34,35.
The results also indicated that living in rural areas was associated with lower levels of oral health KAB, this is consistent with the results of a study conducted among pregnant Egyptian women32. Lower levels of KAB among participants living in rural areas can be attributed to their increased vulnerability to geographical isolation, limited access to oral health services and more financial stresses36. Additionally, consistent with existing literature, having health insurance was significantly associated with better oral health behaviors28. Most of the participants (77.8%) reported visiting the dentist only when they experienced pain. This finding aligns with another study, which suggests that such behavior may stem from lower levels of oral health awareness and financial constraints35.These findings highlight the need for expanded health insurance coverage to promote better oral health behaviors and increase the affordability of dental services37.
On the other hand, the effect of gender on oral health knowledge is statistically insignificant (P = 0.17), this finding is consistent with existing literature38. However, studies in other Arab countries, reported that females showed statistically significant higher scores of oral health knowledge28,39,40. Additionally, the health status and smoking status of the participants exhibited no statistically significant effect on the overall HU-DBI score. This contrasts with findings from another study reporting that non-smokers have better oral health knowledge and behaviors compared to smokers28.This can be due to the variable sample size, study population and the reliance of our study on self-reported data. Also, among the various oral health habits, the use of mouth wash did not have a statistically significant effect on the overall HUD-DBI score.
This study is one of the first to examine the oral health knowledge, attitudes and behaviors among a group of Egyptian adults. The study also provided insights into the correlation of these factors with the participants’ dental habits, DMFT scores and sociodemographic characteristics. Additionally, the sample included a diverse range of sociodemographic characteristics, making it representative of the population. Moreover, the study included clinical examinations, which provided an objective assessment of the participants’ oral health.
However, this study may have several limitations. First, using convenience non-probability sampling from a single institution may introduce selection bias and limit the generalizability of the results. However, data collection from a single institution was essential due to limited funding and time, which are common constraints in developing countries. Additionally, despite its limitations, convenience sampling is suitable to identify patterns and trends by providing a snapshot of the KAB of the study population. Moreover, the dental school is in Greater Cairo, a metropolitan area, which may serve as a reasonably representative sample of the Egyptian population. In addition, some subgroup sizes, such as certain occupation categories, included very few participants, which may limit the statistical validity of subgroup comparisons. Furthermore, as a cross-sectional study, it lacks the ability to establish temporality and causality; however, it serves as a valuable foundation for future studies. Lastly, the use of close-ended questions limits the ability to capture all the dimensions of oral health knowledge, attitudes, and behaviors among the participants. Self-reported data may also introduce social desirability bias, where participants may have over-reported positive oral hygiene practices and underreported negative ones.
The findings suggest designing focused oral health awareness targeting the populations with lower education levels, and those living in rural areas to tackle the observed disparities. The programs must reinforce the adoption of healthier oral habits such as daily brushing and flossing. In addition, we recommend that governmental efforts focus on expanding medical insurance coverage to vulnerable and uninsured groups. The insurance coverage should include routine dental examinations and preventive measures, which are essential for improving individuals’ oral health41. Furthermore, conducting multi-center studies, with larger representative samples using probability sampling, is recommended to enhance the generalizability of the results. Also, longitudinal studies are needed to assess changes in oral health knowledge, attitudes and behaviors over time. Interventional studies are also recommended to detect causal relationships and to assess the effectiveness of health promotion programs.
Conclusion
Adult patients in Egypt demonstrate fair oral health knowledge and attitudes while their oral health behaviors are poor. In addition, the participants demonstrate high caries index. Participants with higher education levels, urban residence, regular dental visits, and positive oral hygiene practices such as daily use of fluoride toothpaste and flossing showed higher HU-DBI scores, implying better oral health knowledge, attitudes, and behaviors. These findings indicate a substantial need for coordinated oral health promotion programs targeting different population segments.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to participant consent limiting data use to research purposes under conditions that ensure anonymity. Public sharing may compromise confidentiality and privacy. However, the data are available from the corresponding author on reasonable request.
Abbreviations
- HU-DBI:
-
The Hiroshima University–Dental Behavioral Inventory
- DMFT:
-
Decayed, missing and filled teeth
- KAB:
-
Knowledge, attitude and behavior
References
Karimbux, N. et al. Measuring patient experience of oral health care: A call to action. J. Evidence-Based Dent. Pract. 23, 101788 (2023).
Sischo, L. & Broder, H. Oral health-related quality of life: what, why, how, and future implications. J. Dent. Res. 90, 1264–1270 (2011).
Moradi, G. et al. Evaluation of oral health status based on the decayed, missing and filled teeth (DMFT) index. Iran. J. Public Health 48, 2050 (2019).
Peres, M. A. et al. Oral diseases: a global public health challenge. Lancet 394, 249–260 (2019).
Organization, W. H. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030 (World Health Organization, 2022).
Oberg, E. & Frank, E. Physicians’ health practices strongly influence patient health practices. J. Royal Coll. Physicians. Edinb. 39, 290 (2009).
Wijtzes, A. I. et al. Effectiveness of interventions to improve lifestyle behaviors among socially disadvantaged children in Europe. Eur. J. Public. Health. 27, 240–247 (2017).
Mishra, S. R., Neupane, D., Shakya, A., Adhikari, S. & Kallestrup, P. Modifiable risk factors for major non-communicable diseases among medical students in Nepal. J. Community Health. 40, 863–868 (2015).
Havigerová, J. M., Dosedlová, J. & Burešová, I. One health behavior or many health-related behaviors? Psychol. Res. Behav. Manage. 12, 23–30. https://doi.org/10.2147/PRBM.S173692 (2018).
Ghaffari, M., Rakhshanderou, S., Ramezankhani, A., Noroozi, M. & Armoon, B. Oral health education and promotion programmes: meta-analysis of 17‐year intervention. Int. J. Dental Hygiene. 16, 59–67 (2018).
Lian, C. W. et al. Oral health knowledge, attitude and practice among secondary school students in Kuching, Sarawak. Archives Orofac. Sci. 5, 9–16 (2010).
Organization, W. H. Advocacy, Communication and Social Mobilization for TB Control: a Guide To Developing knowledge, Attitude and Practice surveys. Report No. 9241596171 (World Health Organization, 2008).
Al-Wesabi, A. A., Abdelgawad, F. & Sasahara, H. El Motayam, K. Oral health knowledge, attitude and behaviour of dental students in a private university. BDJ open. 5, 16 (2019).
Charan, J. & Biswas, T. How to calculate sample size for different study designs in medical research? Indian J. Psychol. Med. 35, 121–126 (2013).
Kawamura, M. Dental behavioral science. The relationship between perceptions of oral health and oral status in adults. Hiroshima Daigaku Shigaku Zasshi J. Hiroshima Univ. Dent. Soc. 20, 273–286 (1988).
Kawamura, M. et al. Relationship between CPITN and oral health behaviour in Japanese adults. Aust. Dent. J. 38, 381–388 (1993).
Daou, D., Rifai, K., Doughan, B. & Doumit, M. Development of an Arabic version of the Hiroshima University-dental behavioral inventory: Cross-cultural adaptation, reliability, and validity. J. Epidemiol. Global Health. 8, 48–53 (2018).
Riad, A. et al. Oral health knowledge, attitudes, and behaviors (KAB) of German dental students: descriptive cross-sectional study. Front. Med. 9, 852660 (2022).
Klein, H., Palmer, C. E. & Knutson, J. W. Studies on dental caries: I. Dental status and dental needs of elementary school children. Public Health Reports (1896–1970), 751–765 (2013).
Dancey, C. P. & Reidy, J. Statistics without maths for psychology. Pearson education (2007).
Cancio, V., Faker, K., Bendo, C. B., Paiva, S. M. & Tostes, M. A. Individuals with special needs and their families’ oral health-related quality of life. Brazilian Oral Res. 32, e39 (2018).
Abdel Fattah, M. A. et al. Epidemiology of dental caries in permanent dentition: evidence from a population-based survey in Egypt. BMC Public. Health. 22, 2438 (2022).
Mohamed, Y. S. Assessment of the knowledge and awareness among Egyptian parents in relation to oral health status of their children. Egypt. Dent. J. 66, 737–746 (2020).
Ghayth, E. I., Fahmy, H. D. & El-moghrab, N. M. Abd El-Aziz, N. M. Knowledge and reported practice among elderly with oral and dental problems at Assiut City, Egypt. Assiut Sci. Nurs. J. 7, 102–112 (2019).
Mohamed, A. Y., Hassan, S. A. A. & Ali, A. A. E. Mothers’ Awareness, attitude and practices regarding oral health of preschool children. Zagazig Nurs. J. 20, 58–76 (2024).
De Abreu, M. H. N. G., Cruz, A. J. S., Borges-Oliveira, A. C., Martins, R. C. & Mattos, F. d. F. Perspectives on social and environmental determinants of oral health. Int. J. Environ. Res. Public Health. 18, 13429 (2021).
Helal, M., Moneim, S. A. & Foad, M. Parents’ knowledge, attitude and practices toward oral health of their children with primary dentition: A cross sectional study. J. Med. Sci. Res. 5 (2022).
Abu-Gharbieh, E., Saddik, B., El-Faramawi, M., Hamidi, S. & Basheti, M. Oral health knowledge and behavior among adults in the united Arab Emirates. Biomed. Res. Int. 2019 (7568679). https://doi.org/10.1155/2019/7568679 (2019).
Aida, J. et al. Income inequality, social capital and self-rated health and dental status in older Japanese. Soc. Sci. Med. 73, 1561–1568 (2011).
Islam, M. N. et al. Oral health knowledge, attitudes, and practices among university students in bangladesh: a cross-sectional study. Discover Public. Health. 22, 242 (2025).
Elrashid, A. H. et al. Correlation of sociodemographic factors and oral health knowledge among residents in Riyadh City, Kingdom of Saudi Arabia. Journal Oral Health & Community Dentistry 12 (2018).
Khalaf, S. A., Osman, S. R., Abbas, A. M. & Ismail, T. Knowledge, attitude and practice of oral healthcare among pregnant women in Assiut, Egypt. Int. J. Community Med. Public. Health. 5, 890–900 (2018).
Rajeh, M. T. Gender differences in oral health knowledge and practices among adults in Jeddah, Saudi Arabia. Clinical Cosmet. Invest. Dentistry, 235–244 (2022).
Tadin, A. & Badrov, M. Oral health Knowledge, Self-Assessed oral health Behavior, and oral hygiene practices among the adult general population in Croatia. Healthcare 12, 88 (2024).
Kango, H., Jha, N. A., Masoodi, P., Naz, A. & Chowdhury, A. Oral health and hygiene practices from Baramulla District, Jammu and Kashmir, india: A Questionnaire-Based Cross-Sectional observational survey. Healthcare 13, 458 (2025).
Smokowski, P. R., Bacallao, M. L., Cotter, K. L. & Evans, C. B. The effects of positive and negative parenting practices on adolescent mental health outcomes in a multicultural sample of rural youth. Child. Psychiatry Hum. Dev. 46, 333–345 (2015).
Jang, Y. E., Kim, C. B. & Kim, N. H. Utilization of preventive dental services before and after health insurance covered dental scaling in korea: 2009 to 2014 community health survey. Asia Pac. J. Public. Health. 29, 70–80 (2017).
Tadin, A., Poljak Guberina, R., Domazet, J. & Gavic, L. Oral hygiene practices and oral health knowledge among students in Split, Croatia. Healthcare 10, 406 (2022).
Abdulrahim, M., AlKandari, M., Alomari, Q. & Baskaradoss, J. K. Oral health knowledge, attitude and practice among adolescents in Kuwait. Int. J. Adolesc. Med. Health. 34, 437–442 (2022).
Miluska, E. A. K., Dulanto-Vargas, J. A. & Maynor, C. S. K. Factors influencing adolescents’ Knowledge, Practices, and attitudes towards oral health in the Rupa-Rupa District, Peru. J. Int. Soc. Prev. Community Dentistry. 14, 469–478 (2024).
Go, H., Kuboniwa, M. & Choi, Y. H. Effect of the oral examinations in the National health screening program on preventive oral health care and treatments: a 19-year follow-up study. BMC Oral Health. 24, 1447 (2024).
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
Mennatollah Nagy Sharkawy (MNS) contributed to the collection and interpretation of data, drafting and revising the manuscript. Omar Shaalan (OS) contributed to the conception and design of the study, contributed to data interpretation and revised the full manuscript draft. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The research protocol was approved by the Research Ethics Committee of School of Dentistry, Newgiza University. The study included adult patients (18 years or older) with adequate cognitive ability who agreed to participate in the study and signed an informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sharkawy, M.N., Shaalan, O. Oral health knowledge, attitudes, and behaviors of adult patients attending a dental school hospital in Egypt: a cross-sectional study. Sci Rep 15, 43274 (2025). https://doi.org/10.1038/s41598-025-29251-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-29251-4
