
Abstract
Patients with head and neck cancer (HNC) frequently encounter symptom clusters following radiotherapy, which substantially affect their quality of life. This study aims to identify distinct symptom clusters in undergoing radiotherapy HNC patients and examine how self-perceived burden and social support mediate the relationship between symptom clusters and quality of life. A cross-sectional survey of 409 HNC patients (Jun–Dec 2024) was conducted. Symptoms were assessed using the M.D. Anderson Symptom Inventory-Head and Neck, self-perceived burden using the Self-Perceived Burden Scale for Cancer Patients, social support using the Medical Outcomes Study Social Support Survey, and quality of life using the Functional Assessment of Cancer Therapy-General. Exploratory factor analysis identified symptom clusters, structural equation modeling (SEM) tested mediation paths. Four distinct symptom clusters were identified in HNC patients undergoing radiation therapy: oropharyngeal, neurosensory, psychological, and gastrointestinal. Symptom clusters negatively predicted social support (β= − 0.449, p < 0.05, explaining 20.2% variance). Symptom clusters and social support jointly predicted self-perceived burden (Symptom clusters:β = 0.490, Social support:β = − 0.131; p < 0.05, explaining 31.6% variance). Symptom clusters, social support, and self-perceived burden collectively predicted quality of life (Symptom clusters:β= − 0.396, Social support:β = 0.150, Self-perceived burden:β= − 0.198; p < 0.05, explaining 37.9% variance). Self-perceived burden significantly mediated the relationship between symptom clusters and quality of life(indirect effect = − 0.041, 95% CI − 0.256 to − 0.007), social support mediation was non-significant, and no chain mediation existed. It was found that symptom clusters in HNC patients receiving radiation therapy have a direct negative impact on their quality of life. These symptoms also indirectly affect quality of life through self-perceived burden mediation. Future interventions should focus on reducing patient’s burden and improving Social support. Additionally, exploring the relationship between symptoms, psychological factors, and social factors, and creating a comprehensive care system that addresses symptom management, psychological empowerment, and social support enhancement could help improve patients’ quality of life.
Similar content being viewed by others

Introduction
Head and neck cancer (HNC) ranks as the sixth most prevalent malignant tumors worldwide, impacting different anatomical locations like the nasopharynx, oropharynx, larynx, and thyroid1. In 2020, around 878,000 new cases were reported worldwide2, with higher incidence rates in China compared to Western countries3. To date, radiotherapy is the main treatment for HNC, but it also leads to symptoms like fatigue, dry mouth, anorexia, skin pain, dysphagia, and hoarseness, which can impact treatment effectiveness and patients’quality of life (QOL)4. QOL is a key outcome indicator in cancer treatment encompassing various dimensions like physiological function, psychological state, social adaptation, and environmental interaction. Moreover, studies have found that symptoms due to shared pathological mechanisms forms various symptom clusters (SC)5, such as RT-specific SC (pain, dysphagia, mucositis), gastrointestinal SC (nausea, anorexia), and psychosocial SC (depression, anxiety)6, which have a more significant impact on QOL than individual symptoms in HNC patients receiving radiotherapy7. However, while the relationship between HNC’s SC and QOL is known, the underlying mechanisms remain unclear, underscoring the importance of further research to establish a theoretical model for clinical intervention.
This study adopted the Theory of Unpleasant Symptoms (TOUS) as the theoretical framework. which includes three core concepts: symptom experience, influencing factors, and functional performance8. TOUS has been used in cancer-related studies to explain how multiple co-occurring symptoms interact to affect patients’ health outcomes9. However, its use in HNC patients during radiotherapy remains limited. HNC patients often experience co-occurring symptoms during radiotherapy, including pain, dysphagia, and fatigue.The complex interactions between these symptoms align with the multidimensional and interactive characteristics emphasized by TOUS, providing a theoretical basis for this study. TOUS posits that physiological, psychological, and situational factors influence symptom experiences, which in turn affect patients’ functional performance and overall health10. Guided by this theory, this study conceptualizes SC as core symptom experiences, self-perceived burden(SPB) as a psychological factor, and social support (SS) as an environmental factor-elements that contribute to functional outcomes reflected in QOL. Integrating these elements into a unified theoretical model, this study advances evidence-based supportive care strategies combining nursing, psychological, and social interventions to enhance the overall health of head and neck cancer patients during radiotherapy.
Building on theoretical and empirical evidence, we posits the following hypotheses: Hypothesis 1 (H1): SC can significantly and negatively predict QOL in HNC patients undergoing radiotherapy. Although previous studies have demonstrated an inverse association between SC and QOL11,12,13,14,15, there is limited evidence in patients undergoing radiotherapy for HNC, particularly within the framework of the TOUS. Hypothesis 2 (H2): SS mediates the relationship between SC and QOL. Social support (SS) is an important component of an individual’s external resources in the Conservation of Resources (COR) theory16. Medical social support involves support from healthcare professionals, family, friends, and other social networks in medical settings. Research has shown that SS can positively impact QOL through resource gain mechanisms17. However, it was also reported that SC hinders patients’ access to SS15. Thus, it is plausible to suggest that SS partially mediates the SC-QOL relationship.Hypothesis 3 (H3): SPB mediates the relationship between SC and QOL. Self-perceived burden (SPB) is defined as “a complex psychological experience characterized by empathic concern for the impact of illness and caregiving demands on others, leading to feelings of guilt, distress, responsibility, and diminished self-awareness“18. Studies have shown that SPB is a crucial factor in determining QOL19,20. Moreover, research has suggested that reducing SPB can help lessen the effects of SC on QOL21, suggesting that SPB may partially mediates the SC-QOL relationship. Hypothesis 4 (H4): a chain mediation path via SS and SPB exists between SC and QOL. Studies have shown that SS significantly reduces the perceived burden of patients after lung cancer surgery through multiple mechanisms such as emotional buffering, cognitive reconstruction, behavioral empowerment, and social capital accumulation22. Combined with H2 and H3, it suggests that the severity of SC could impact SS acquisition, leading to changes in SPB levels and ultimately affecting QOL.
The objective of this study is to uncover the connection between SC, SS, SPB and QOL in HNC patients. Theoretically, it demonstrated a dual-pathway conceptual model where SC impact QOL through SPB and SS. Practically, it provides insights for creating comprehensive interventions that combine symptom management, psychological support, and social resource integration.
Methods
Study design and participants
A cross-sectional study was carried out to examine how Social Support (SS) and self-perceived burden (SPB) mediate the relationship between symptom clusters (SC) and quality of life (QOL) in head and neck cancer (HNC) patients undergoing radiotherapy.
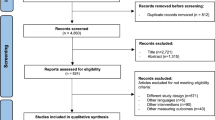
A cross-sectional survey was carried out from May to December 2024, using convenience sampling at the radiotherapy departments of three tertiary general hospitals in Zhengzhou, Henan Province. Inclusion criteria included: (1) pathologically confirmed HNC; (2) age≥ 18 years; (3) undergoing radiotherapy; (4) awareness of diagnosis and treatment plan; (5) adequate literacy to complete self-reported measures; and (6) provision of informed consent. Exclusion criteria were: (1) malignant tumors outside the head and neck region; (2) communication or cognitive dysfunction; and (3) poor physical condition with a Karnofsky Performance Status (KPS) score≤ 30. This study was approved by the Institutional Review Board of Henan Cancer Hospital (No. 2021-KY-0165-002) and performed in accordance with the Declaration of Helsinki and relevant institutional guidelines. Written informed consent was obtained from all participants prior to study procedures. With 409 valid questionnaires retained after quality control, the valid response rate was 93.17%. Invalid questionnaires (6.83%) were excluded due to incomplete responses, logical inconsistencies, or failure to meet inclusion criteria (e.g., patients who did not complete radiotherapy or provided duplicate answers).
Measures
Demographic and disease information questionnaire
A researcher-designed data collection form was developed based on relevant literature and clinical experience. It consists of two sections: demographic information (such as gender, age, and educational level) and disease-related information (including type of HNC, disease stage, illness duration, treatment methods, and presence of nasogastric tube).
Independent variable
The M. D. Anderson Symptom Inventory-Head and Neck (MDASI-H&N) was originally developed in 200723 and consists of three parts:13 core items, 9 head and neck cancer-specific items, and the 6 interference items, respectively. The scoring scale range is from 0 to 10, with 0, 10 representing no symptoms, and the most severe symptoms, respectively. The scale was translated, culturally adapted, revised, and validated, showing good reliability and validity. The Cronbach’s αcoefficient for the symptom distress section is 0.91 for the first 13 items, 0.85 for the last 9 items, and 0.88 for the daily life distress section24. In this study, only the symptom distress section was used, with a Cronbach’s αcoefficient of 0.894.
Mediating variables
The Self-perceived Burden Scale for Cancer Patients (SPBS-CP) was developed by Ren et al. based on Cousineau et al.‘s scale25, assesses the degree of self-perceived burden among cancer patients. It consists of four dimensions: economic/family burden, psychological/emotional burden, caregiving burden, and treatment burden, with a total of 21 items. Each item is rated on a 5-point Likert scale, resulting in a total score range of 21–105. Scores below 30 indicate no significant burden, 30–49 indicate mild burden, 50–69 indicates moderate burden, and 70 or above indicate severe burden.The SPBS-CP has been shown to possess good reliability and validity in previous studies26. In the present study, it exhibited excellent internal consistency (Cronbach’s α = 0.946).
Medical Outcomes Study Social Support Survey (MOS-SSS) was originally developed by Sherbourne and Stewart27 to assess social support in individuals with chronic diseases. It was translated and culturally adapted by Doris et, showing strong reliability and validity28.The scale consists of 19 items grouped into four dimensions: emotional-informational support, instrumental support, affectionate support, and positive social interaction. Participants rate each item on a 5-point Likert scale, with higher scores indicating higher perceived social support. The Cronbach’s αcoefficient for the MOS-SSS in this study was 0.981.
Dependent variable
Cella et al. developed the Functional Assessment of Cancer Therapy-General (FACT-G) to evaluate the functional status of cancer patients29.Wan et al. translated and evaluated the FACT-G in 2007 for use Chinese cancer populations, demonstrating good reliability, validity, and responsiveness30.It includes 27 items measuring physical well-being, social/family well-being, emotional well-being, and functional well-being. Patients rate their feelings over the past week on a scale of 0 ~ 4. Higher scores reflect better quality of life (QOL). In this study, the FACT-G demonstrated a Cronbach’s αcoefficient of 0.918.
Data collection methods
The first author sought support from the head of the radiotherapy department and the head nurse before the survey. Data collectors were trained on the study objectives, patient consent procedures, questionnaire administration, and related precautions. They recorded general and disease-related information from electronic medical records. During the mid-to-late stages of radiotherapy, when symptoms stabilize and become more pronounced31.patients completed the scales themselves, with assistance available for those who needed it. This period was chosen for data collection as it provides a comprehensive reflection of symptom cluster (SC) characteristics and their impact on quality of life (QOL). Patients with severe comorbidities or unstable conditions were excluded to ensure independent questionnaire completion. All participants successfully completed the questionnaires without refusal or interruption due to physical discomfort. Questionnaires were filled out within 20–30 min, checked for accuracy, and promptly collected after completion.
Statistical analysis
Statistical analyses were conducted using SPSS 24.0 and Amos 24.0. Descriptive statistics were used to describe demographic variables and disease characteristics. The factor structure of SC was determined through principal component analysis with varimax rotation. Factors and items were selected based on eigenvalues > 1 and factor loadings>0.5. Pearson correlation analysis was used to examine the relationship between SC, SS, SPB, and QOL. Structural equation modeling (SEM) was applied to assess the model’s convergent validity, discriminant validity, overall fit, and to analyze path relationships and mediating effects.The evaluation of the model was based on established SEM guidelines.Convergent validity was examined using factor loadings, composite reliability (CR), and average variance extracted (AVE), following the criterion that standardized loadings should exceed 0.50, CR > 0.70, and AVE > 0.5032,33. Regression analysis based on a path model within a structural equation modeling framework was performed to examine the direct and indirect effects.
Results
Basic demographic and disease information
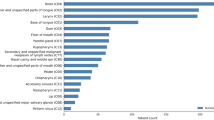
Among the 409 patients, 71.39% were aged 50 or older, and 77.51% patients were male. Moreover, 57.7% had junior high school education or below. The primary tumor site for most patients was the nasal cavity and paranasal sinuses (38.88%). A majority of patients (52.32%) had a disease duration of 1–3 months since diagnosis (see Table 1).
Symptom clusters
Symptom clusters(SC) were derived from the MDASI-HN using exploratory factor analysis (EFA). The aim of this analysis was to identify groups of co-occurring symptoms that represent distinct but interrelated dimensions of symptom experience among patients receiving radiotherapy. Principal component extraction with varimax rotation was applied to determine the underlying factor structure.Exploratory factor analysis identified four SC in this study: oropharyngeal (eigenvalue = 3.601), neurosensory(eigenvalue = 3.350), psychological state (eigenvalue = 3.321) and the gastrointestinal (eigenvalue = 2.585). These factors explained a total of 58.443% of the variance. In subsequent analyses, these SC scores served as independent variables to examine effects on patients’quality of life(QOL) within the structural equation model.In subsequent analyses, these symptom cluster scores served as independent variables to examine effects on patients’quality of life within the structural equation model. (see Table 2)
Correlation analysis of study variables
Correlation analyses among the main study variables were conducted using Pearson’s correlation coefficients computed in SPSS to examine bivariate associations. A negative correlation was observed between SC and social support(SS) (r = −0.347, P < 0.001), as well as QOL (r = −0.349, p < 0.001), while a positive correlation was noted between SC and self-perceived burden (SPB) (r = 0.453, p < 0.001). SS exhibited a negative correlation with SPB (r = −0.364, p < 0.001),but a positive correlation with QOL(r = 0.358, p < 0.001). Moreover, SPB showed a negative correlation with QOL(r = −0.457, p < 0.001) (see Table 3).
Measurement model
Maximum likelihood estimation was used to estimate the measurement model, assessing reliability and convergent validity, as well as discriminant validity( See Fig. 1).

Structural equation modeling diagram.
Convergent validity
The standardized factor loadings fell between 0.500 and 0.993, with composite reliability ranging from 0.711 to 0.987, and AVE from 0.382 to 0.949, thus satisfying the recommended criteria for reliability and convergent validity (see Fig. 1).Although some AVE values were slightly below the 0.50 threshold, the corresponding CR values all exceeded 0.70, indicating that the constructs still demonstrated adequate internal consistency and convergent validity32,33. In such cases, higher CR values can compensate for marginally low AVE, suggesting that the latent constructs explain sufficient shared variance among their indicators to be considered reliable (Fig. 2).

Structural equation modeling diagram-simple version. SC, Symptom clusters; SCRO, Symptom clusters-ropharyngeal; SCNE, Symptom clusters-neurosensory; SCPS, Symptom clusters-psychological; SCGA, Symptom clusters-gastrointestinal; SS, Social support; SSFL, Social support-flexible; SSIN, Social support-emotional information; SSEM, Social support-emotional; SSSO, Social support-social interaction features; SPB, Self-perceived burden; SPBCA, Self-perceived burden-care; SPBEF, Self-perceived burden-economic/family; SPBTR, Self-perceived burden-treatment; QOL, Quality of life; QOLPH, Quality of life-physical; QOLSO, Quality of life-social family; QOLEM, Quality of life-emotional; QOLFU, Quality of life-function.
Discriminant validity
This study assessed the measurement model’s discriminant validity using the AVE method. A model has discriminant validity when the square root of the AVE for each construct exceeds its correlations with others.In this study, the square roots of the AVE for most constructs exceeded their corresponding correlation coefficients. Specifically, the AVE square roots for SC, SS, SPB, and QOL were 0.572, 0.949, 0.660, and 0.486, respectively.The correlation coefficients between SC and SS, SC and SPB, SC and QOL, SS and SPB, SS and QOL, and SPB and QOL are − 0.449, 0.549, − 0.572, − 0.352, 0.398, and − 0.468, respectively.These results show that each construct in this study has good discriminant validity (See Table 3).
Structural model analysis
This study used the maximum likelihood method for structural equation modeling (SEM) analysis.Following Kenny’s recommendationto exclude GFI and AGFI due to sample size sensitivity34, we assessed the model’s fit.The original MLχ2 was 7235.559, but after using the Bollen-Stine p-value correction method to address potential chi-square inflation from non-multivariate normality, the corrected chi-square value was 3334.345.We recalculated all fit indices.The recalculated indices indicated that, except for SRMR (0.105), which was slightly above the standard, other indices such asχ2/DF (1.393), RMSEA (0.031), TLI (0.964), and CFI (0.966) met the conventional SEM criteria, indicating acceptable model fit.
Regression analysis
SC was found to have a significant negative impact on SS (b = − 0.340, p < 0.05), explaining 20.2% of the variance in SS. Both SS (b = − 0.139, p < 0.05) and SC (b = 0.392, p < 0.05) significantly influenced SPB, explaining 31.6% of the variance in SPB. Furthermore, SC (b = − 0.166, p < 0.05), SS (b = 0.083, p < 0.05), and SPB (b = − 0.104, p < 0.05) were found to significantly impact QOL, explaining 37.9% of the variance in QOL (see Table 4).
Mediation analyses
Bootstrapping is commonly used to test indirect effects of mediating variables by resampling with replacement from the original sample, and bias-corrected bootstrapping is especially powerful for this purpose. The total effect of SC on QOL is significant, with a confidence interval of − 0.384 to − 0.135. The indirect effect of SC on QOL via SS is non-significant, with a confidence interval of − 0.064 to 0.010. By contrast, the indirect effect of SC on QOL via SPB is significant, with a confidence interval of − 0.256 to − 0.007. Additionally, the indirect effect of SC on QOL via SS and SPB together is non-significant, with a confidence interval of − 0.053 to 0.000 (see Table 5).
Discussion
Symptom clusters in head and neck cancer patients undergoing radiotherapy
Four clinically significant symptom clusters(SC)were identified in this study: the oropharyngeal cluster (oral and pharyngeal mucus, dry mouth, oral or pharyngeal pain, swallowing/choking, taste abnormalities), the neurosensory cluster (choking, skin pain, dental or gum pain, numbness and tingling), the psychological state cluster (distressing, sorrow, sleeplessness, shortness of breath, fatigue), and the gastrointestinal cluster (nausea, vomiting, appetite loss). The SC identified in head and neck cancer (HNC) patients undergoing radiotherapy support the core proposition of the Theory of Unpleasant Symptoms (TOUS), which posits that symptoms often co-occur and share common mechanisms10. Among the oropharyngeal cluster, dry mouth was the most prominent symptom, closely associated with radiation-induced salivary gland damage35. The neurosensory cluster primarily reflected alterations in sensory function and motor coordination, such as coughing during swallowing. The psychological state cluster was characterized by emotional distress and fatigue, aligning with prior research emphasizing the psychological burden of radiotherapy in HNC patients36. The gastrointestinal cluster emerged as an independent cluster, highlighting the close link between treatment toxicity and nutritional status. Notably, oral or pharyngeal pain was classified within thethe oropharyngeal cluster rather than the neurosensory cluster. This may relate to the physiological connections among symptoms such as mucositis, xerostomia, and dysphagia. the oropharyngeal cluster reflects local symptom experiences directly associated with mucosal and glandular damage, rather than systemic neurosensory changes. Overall, these findings shed light on the complex interplay between physical and psychological symptoms in HNC patients undergoing radiotherapy, providing a theoretical foundation for multidisciplinary symptom management.
Correlations among symptom clusters, social support, self-perceived burden, and quality of life
The Pearson correlation analysis revealed strong interrelationships among various variables in HNC patients undergoing radiotherapy. Consistent with previous research37, SC was to be found positively correlated with self-perceived burden (SPB), indicating that a higher SC burden leads to increased perception of symptom burden. SC was negatively correlated with social support (SS) and quality of life(QOL), suggesting that symptoms may deplete social energy, reduce support resources utilization, and lower QOL11,15,38. SPB was negatively correlated with both QOL and SS, in line with prior studies19,39, indicating a bidirectional weakening effect on QOL and SS through an emotional withdrawal mechanism. In addition, the positive correlation between SS and QOL was also observed in patients with oral cancer40, highlighting the universal applicability of SS in improving QOL across different cancer types. These findings suggest that symptom burden may impact QOL through direct physical function weakening and indirect effects on SS utilization and SPB.
Mediating role of SPB between SC and QOL
The structural equation model in this study showed a good fit after the Bollen-Stine correction, although the SRMR slightly exceeded the ideal threshold at 0.15.This suggests that the model accurately captured the relationships among variables. Through the mediation analysis, it was found that the SC had both a direct and an indirect effect on QOL, the latter being through SPB. This supports the idea that SC affects QOL in two ways: (1) directly through physiological symptoms like pain and fatigue, which can decrease daily functioning and comfort; (2) indirectly through psychosocial factors such as increased psychological stress from SPB, where more severe SC leads to the higher SPB and a decline QOL. These findings align with the TOUS framework, which highlights the interconnectedness of symptoms, influencing factors, and outcomes in patients’experiences10. The bidirectional mechanism suggests that clinical interventions should target both symptom management and psychosocial support. Therefore, recommendations include implementing precision case like wallowing function training and mucosal protection programs41, and establishing a dyadic intervention model for patients and caregivers to reduce patients’ SPB through psychoeducation and family support42. This combined strategy offers hope for personalized symptom relief in HNC cancer patients undergoing radiotherapy.
Social support did not mediate between symptom clusters and quality of life, and no chain mediation effect was found
Despite our initial hypothesis, SS did not act as a mediator between SC and QOL in undergoing-radiotherapy patients with HNC cancer. This could be due to the majority of patients being over 50 years old (71.39%), and a significant portion being diagnosed with the disease for only 1 ~ 3 months (52.32%). Older patients may have different needs and perceptions regarding SS43 and those with shorter disease durations may not have experienced depletion of long-term support44, explaining why SS did not mediate the association between SC and QOL. The sequential mediation effect of SS and SPB between SC and QOLwas not statistically significant in our study. Two potential explanations for this finding: (1) sample characteristics and data distribution may have contributed to this result. While the Bollen-Stine Bootstrap correction improved model fit indices in our structural equation modeling (SEM) analysis, it’s noteworthy that this correction primarily addresses issues of small sample size or violations of multivariate normality assumptions. This methodological consideration may explain the discrepancy between significant individual path coefficients in our regression analyses and non-significant sequential mediation effects in mediation analyses. (2) Second, effect size considerations warrant attention. The current sample size may have been insufficient to achieve adequate statistical power, particularly given the complexity of examining this specific sequential mediation pathway. However, given that no prior studies have reported effect sizes for this particular mediation chain and that the non-significant paths may reflect limited statistical power rather than the true absence of effects45, a formal post-hoc power analysis is recommended to better evaluate whether sample size constraints influenced these findings46. In conclusion, despite the lack of significant sequential mediation in our study, these initial results need to be validated in larger samples. The theoretical framework suggesting that SS could boost coping strategies by providing emotional support, informational guidance, and practical assistance, and potentially leading to improved QOL47 remains clinically plausible and warrants further investigation with more robust methodologies.
Limitations and future directions
The study found no significant mediating effect of social support (SS) between symptom clusters (SC) and quality of life (QOL) in HNC patients. No chain-mediation was observed where SC influenced QOLthrough SS and SPB. The study has the following limitations: First, the cross-sectional research design restricts causal inferences between SC, SS, SPB, and QOL. Second, the study sample, drawn from three hospitals within the same region, limits the representativeness and generalizability of the findings. Additionally, the small sample size reduces statistical power and weakens the significance of some effects. Future studies should use longitudinal research designs to track the trajectories of SC, SS, SPB, and QOL, thereby deepening understanding of their underlying mechanisms. Multi-center or cross-regional study designs can include more diverse populations and improve the generalizability of the results.Incorporating neurobiological indicators (such as inflammation markers and stress hormones) can uncover the biological mechanisms through which SC affects QOL. These findings support integrating precision strategies for symptom management, psychological interventions, and biomedical measures to optimize individualized clinical decision-making and improve the quality of life for HNC patients.
Clinical implications and innovations
This study introduces a fresh structural equation model to explore the connection between QOL and SC in undergoing radiotherapy patients with HNC cancer, going beyond traditional research methods. The study proposes a dual-intervention approach: (1) incorporating SPB screening tools in regular symptom assessments; and (2) implementing interdisciplinary intervention programs for high-risk patients, such as mindfulness-based stress reduction and cognitive restructuring.
Data availability
The datasets generated and/or analyzed during this study are available from the corresponding author upon reasonable request.
Abbreviations
- QOL:
-
Quality of life
- SC:
-
Symptom clusters
- HNC:
-
Head and neck cancer
- SS:
-
Social support
- SPB:
-
Self-perceived burden
- TOUS:
-
The theory of unpleasant symptoms
- MDASI-H&N:
-
M.D. Anderson symptom inventory-head and neck
- SPBS-CP:
-
Self-perceived burden scale for cancer patients
- MOS-SSS:
-
Medical outcomes study social support survey
- FACT-G:
-
Functional assessment of cancer therapy-general
- KPS:
-
Karnofsky performance status
References
Bhat, G. R., Hyole, R. G. & Li, J. Head and neck cancer: current challenges and future perspectives. Adv. Cancer Res. 152, 67–102 (2021).
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71 (3), 209–249 (2021).
Cao, W. et al. Changing profiles of cancer burden worldwide and in china: a secondary analysis of the global cancer statistics 2020. Chin. Med. J. 134 (7), 783–791 (2021).
Crowder, S. L. et al. Head and neck cancer survivors’ experiences with chronic nutrition impact symptom burden after radiation: a qualitative study. J. Acad. Nutr. Diet. 120 (10), 1643–1653 (2020).
Lopes-Júnior, L. C., Ferrarini, T. F., Pires, L. B. & Pereira-da-Silva, G. Cancer symptom clusters in adult patients undergoing chemotherapy: a systematic review and meta-analysis protocol. PLOS One. 17 (7), e0273411 (2022).
Wang, Y. et al. Nutrition impact symptom clusters in patients with head and neck cancer receiving concurrent chemoradiotherapy. J. Pain Symptom Manag. 62 (2), 277–285 (2021).
Lin, Y. et al. A network analysis of self-reported psychoneurological symptoms in patients with head and neck cancer undergoing intensity-modulated radiotherapy. Cancer 128 (20), 3734–3743 (2022).
Lenz, E. R., Pugh, L. C., Milligan, R. A., Gift, A. & Suppe, F. The middle-range theory of unpleasant symptoms: an update. Adv. Nurs. Sci. 19 (1), 14–27 (1997).
Ren, X. et al. The relationships between symptom clusters and contributing factors in patients with esophageal cancer: structural equation modelling based on theory of unpleasant symptoms. BMC Gastroenterol. 25 (1), 544 (2025).
Lenz, E. R. Application of the theory of unpleasant symptoms in practice: a challenge for nursing. Investig. Educ. Enferm. 20 (1), e20 (2018).
Li, Y. et al. Symptom clusters in head and neck cancer patients with endotracheal tube: which symptom clusters are independently associated with health-related quality of life. Eur. J. Oncol. Nurs. 48, 101819 (2020).
Chen, K. et al. Changes in the symptom clusters of elderly patients with lung cancer over the course of postoperative rehabilitation and their correlation with frailty and quality of life: a longitudinal study. Eur. J. Oncol. Nurs. 67, 102388 (2023).
Luo, Y. et al. Symptom clusters and impact on quality of life in lung cancer patients undergoing chemotherapy. Qual. Life Res. 33 (12), 3363–3375 (2024).
Fei, F. et al. Symptom clusters, associated factors and health-related quality of life in patients with chronic obstructive pulmonary disease: a structural equation modelling analysis. J. Clin. Nurs. 32 (1–2), 298–310 (2022).
Zhong, Y. Z. Exploration of Symptom Clusters in Frail Elderly in Nursing Homes and Verification of the Mediating Role of Social Support between Symptom Clusters and Quality of Life (Chengdu University of Traditional Chinese Medicine, 2021).
Egozi, F. H. et al. Conservation of resources, psychological distress, and resilience during the COVID-19 pandemic. Int. J. Public. Health. 67, 1604567 (2022).
Chen, Z. et al. Sleep quality mediates the effect of medical social support on depression symptoms in patients with HIV/AIDS. BMC Public. Health. 24 (1), 1429 (2024).
McPherson, C. J., Wilson, K. G. & Murray, M. A. Feeling like a burden: exploring the perspectives of patients at the end of life. Soc. Sci. Med. 64, 417–427 (2007).
Lin, X. et al. Self-perceived burden predicts lower quality of life in advanced cancer patients: the mediating role of existential distress and anxiety. BMC Geriatr. 22 (1), 803 (2022).
Xu, J. et al. Relationship between psychological resilience and quality of life in cancer patients and the multiple mediating roles of stigma and self perceived burden. Sci. Rep. 15 (1), 12375 (2025).
Zhang, N. et al. Illness uncertainty, self-perceived burden and quality of life in patients with chronic myeloid leukaemia: a cross-sectional study. J. Clin. Nurs. 31 (19–20), 2935–2942 (2021).
Ren, N. et al. The relationship between facilitation of patient involvement and self-perceived burden in postoperative lung cancer patients: the mediating role of social support. Patient Prefer Adherence. 18, 1979–1989 (2024).
Rosenthal, D. I. et al. Measuring head and neck cancer symptom burden: the development and validation of the M. D. Anderson symptom inventory, head and neck module. Head Neck. 29 (10), 923–931 (2007).
Xiao, W. et al. Psychometric validation of the Chinese version of the M.D. Anderson symptom Inventory-Head and neck module (MDASI-HN-C) in patients with head and neck cancer. Support Care Cancer. 30 (1), 219–229 (2022).
Cousineau, N., McDowell, I., Hotz, S. & Hébert, P. Measuring chronic patients’ feelings of being a burden to their caregivers: development and preliminary validation of a scale. Med. Care. 41 (1), 110–118 (2003).
Ren, Y. Development and Preliminary Clinical Application of the Self-Perceived Burden Scale for Cancer Patients (Taishan Medical University, 2012).
Sherbourne, C. D. & Stewart, A. L. The MOS social support survey. Soc. Sci. Med. 32 (5), 705–714 (1991).
Doris, S. F., Yu, D. T. F., Lee, D. & Woo, J. Psychometric testing of the Chinese version of the medical outcomes study social support survey (MOS-SSS-C). Res. Nurs. Health. 27 (2), 135–143 (2004).
Cella, D. F. et al. The functional assessment of cancer therapy scale: development and validation of the general measure. J. Clin. Oncol. 11 (3), 570–579 (1993).
Wan, C., Meng, Q., Tang, X., Zhang, X. & Yang, Z. A review of the Chinese version of the functional assessment of cancer Therapy-General (FACT-G) scale for cancer patients. Pract. J. Cancer. 21 (1), 77–80 (2006).
Rocha, P. H. P. et al. Adverse radiation therapy effects in the treatment of head and neck tumors. Radiographics. 42 (3), 806–821 (2022).
Fornell, C. & Larcker, D. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 18 (1), 39–50 (1981).
Hair, J. F., Black, W. C., Babin, B. J. & Anderson, R. E. Multivariate Data Analysis, 8th edn (Cengage Learning, 2019).
Kenny, D. A. Measuring model fit. http://www.davidakenny.net/cm/fit.htm (accessed 09 Jun 2025).
Schulz, R. E. et al. Prevalence of hyposalivation and associated factors in survivors of head and neck cancer treated with radiotherapy. J. Appl. Oral Sci. 29, e20200854 (2021).
Bao, R. Z. et al. Analysis of psychological distress status in elderly head and neck malignant tumor patients before and after radiotherapy. Chin. J. Radiat. Oncol. 30 (2), 109–113 (2021).
Pan, H. Y. The Mediating Effect of self-perceived Burden between Symptom Clusters and Quality of Life in Patients with Primary Brain Tumors (North Sichuan Medical College, 2023).
Wang, Y. et al. Symptom clusters and impact on quality of life in esophageal cancer patients. Health Qual. Life Outcomes. 20 (1), 168 (2022).
Chang, Y. et al. Influence of self-perceived burden on quality of life in patients with urostomy based on structural equation model: the mediating effects of resilience and social support. Biomed. Res. Int. 2022, 9724751 (2022).
Zhang, Y. et al. Effects of stigma, hope and social support on quality of life among Chinese patients diagnosed with oral cancer: a cross-sectional study. Health Qual. Life Outcomes. 18 (1), 112 (2020).
Lanzetti, J. et al. Management of oral hygiene in head-neck cancer patients undergoing oncological surgery and radiotherapy: a systematic review. Dent. J. 11 (3), 83 (2023).
Chen, X. et al. Intervention and coping strategies for self-perceived burden of patients with cancer: a systematic review. Asia Pac. J. Oncol. Nurs. 10 (6), 100231 (2023).
Won, M. Relationship between perceived social support and physical frailty among older patients with coronary artery disease: a dual mediation model. J. Clin. Med. 14 (5), 1744 (2025).
Shokrgozar, S., Rouzbehan, V., Zare, R. & Abdollahi, E. Evaluation of patient social support, caregiver burden, and their relationship with the course of the disease in patients with bipolar disorder. Int. J. Soc. Psychiatry. 68 (8), 1815–1823 (2022).
Kenny, D. A. Mediation. In The Kenny Handbook of Structural Equation Modeling (online). (2018).
Hayes, A. F. Introduction To Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach (Guilford Press, 2013).
Ruiz-Rodríguez, I., Hombrados-Mendieta, I., Melguizo-Garín, A. & Martos-Méndez, M. J. The importance of social support, optimism and resilience on the quality of life of cancer patients. Front. Psychol. 13, 833176 (2022).
Acknowledgements
We extend our sincere gratitude to all study participants for their dedication and contributions.
Funding
This research was supported by the Henan Provincial Academy of Medical Sciences (Grant No. QNYJ2023005).
Author information
Authors and Affiliations
Contributions
R.Z.: Conceptualization, supervision, formal analysis, writing-original draft, writing-review and editing; T.D., H.M., Y.M., A.H.: Data curation; J.K.: Supervision, writing-review and editing; Y.Z.: Writing-review and editing, resources.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
The study protocol was approved by the Ethics Committee of Henan Cancer Hospital (Approval No.2021-KY-0165-002). Written informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhao, R., Ding, T., Ma, H. et al. Effect of symptom clusters on quality of life in patients with head and neck cancer treated with radiotherapy: a cross-sectional study. Sci Rep 15, 44929 (2025). https://doi.org/10.1038/s41598-025-29275-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-29275-w
