
Abstract
The objective of this study was to assess the knowledge, attitudes, and practices (KAP) related to the functional status of arteriovenous fistulas (AVF) among patients undergoing hemodialysis. This cross-sectional study was conducted from April to May 2025 at the First Affiliated Hospital of Nanchang University, employing a self-developed questionnaire for data collection. Among 536 respondents (62.1% male), the mean scores for knowledge, attitude, and practice were 14.74 ± 4.89 (possible range: 0–20), 42.84 ± 4.87 (possible range: 10–50), and 40.75 ± 7.89 (possible range: 10–50), respectively. Statistically significant positive correlations were identified between knowledge and attitude (r = 0.682, P < 0.001), knowledge and practice (r = 0.711, P < 0.001), and attitude and practice (r = 0.622, P = 0.001). Structural equation modeling analysis revealed that knowledge directly influenced both attitude (β = 0.752, P < 0.001) and practice (β = 0.388, P < 0.001), while attitude also had a direct effect on practice (β = 0.449, P < 0.001). Furthermore, knowledge exerted an indirect effect on practice through attitude (β = 0.337, P < 0.001). These findings underscore the necessity for structured and continuous patient education interventions to enhance AVF maintenance and improve long-term dialysis outcomes.
Similar content being viewed by others

Introduction
End-stage renal disease (ESRD) presents a considerable global public health challenge, with maintenance hemodialysis (HD) serving as one of the primary therapeutic interventions for affected individuals1. Within the population of HD patients, the arteriovenous fistula (AVF) is the most prevalent form of vascular access, often characterized as the patient’s “lifeline” due to its pivotal role in ensuring adequate dialysis and enhancing overall survival outcomes2. Current global epidemiological data indicate that approximately four million individuals require renal replacement therapy, with HD constituting nearly 69% of this demographic and representing approximately 89% of all patients receiving dialysis treatment3. In China, recent national surveillance data indicate that by 2021, the number of patients undergoing maintenance HD reached an estimated 735,000, reflecting a significant expansion of the country’s dialysis infrastructure and services4.
Given the essential role of AVF in HD therapy, maintaining its functional integrity is crucial, as it directly impacts treatment efficacy, complication rates, and overall patient quality of life5. International clinical practice guidelines consistently endorse AVF as the preferred method of vascular access due to its lower infection rates, superior long-term patency, and fewer complications in comparison to alternative access methods6,7. However, utilization rates of AVF vary considerably across the globe, with Japan exhibiting the highest prevalence (exceeding 90%), followed by Europe and Australia (60–80%)8. China also reports a relatively high AVF usage rate surpassing 75%, significantly higher than the rates observed in the United States (64%) and several other Western countries9. Despite these encouraging utilization figures, managing AVF presents substantial clinical challenges, with primary patency rates falling to only 60%–70% after one year and continuing to decline thereafter10. Common complications, such as primary failure, stenosis, and thrombosis, significantly contribute to patient morbidity and healthcare resource utilization11.
The Knowledge, Attitude, and Practice (KAP) theoretical framework posits that knowledge serves as a foundational prerequisite for behavioral change, while attitudes and beliefs act as key drivers of this transformation12. This model delineates behavioral change as occurring in three sequential phases: acquiring knowledge, developing corresponding attitudes and beliefs, and establishing sustained practices or behaviors13,14. In the context of HD care, patients’ knowledge, attitudes, and practices are critical determinants of AVF patency and long-term functional outcomes15. Although existing literature indicates that many patients recognize the importance of AVF care, a significant gap often exists between their perceived knowledge and actual clinical practices16. Specifically, patients frequently lack a clear understanding of daily care protocols and evidence-based strategies for preventing complications17. Additionally, maladaptive attitudes—ranging from negligence to excessive concern—can result in poor self-care behaviors, delayed recognition of complications, or unnecessary clinical interventions, ultimately undermining AVF outcomes17. Despite the established clinical significance of AVF functionality in HD patients, comprehensive investigations examining KAP dimensions within the Chinese patient population remain limited.
This study aimed to systematically assess the knowledge, attitudes, and practices of Chinese HD patients regarding AVF functionality while identifying key factors that influence patient behavior. The findings will offer evidence-based insights for developing targeted educational interventions and personalized care strategies, thereby enhancing patient self-management capabilities and ultimately improving long-term dialysis outcomes and quality of life.
Methods
Study design and participants
This cross-sectional study was conducted among hemodialysis patients at the First Affiliated Hospital of Nanchang University from April to May 2025. Data were collected utilizing a self-developed questionnaire. Ethical approval was obtained from the Ethics Committee of the First Affiliated Hospital of Nanchang University (Approval No: IIT (2025) Interim Ethics Review Document No. 359), and informed consent was secured from all participants prior to their enrollment in the study. The inclusion criteria were as follows: (1) patients undergoing maintenance hemodialysis at the study site for a duration exceeding three months; (2) the ability to communicate effectively; (3) intact cognitive function; and (4) the capacity to comprehend and respond to the questionnaire. The exclusion criteria included: (1) refusal to participate; (2) cognitive impairment or psychiatric disorders that could impede questionnaire completion; and (3) recent serious arteriovenous fistula-related complications within the preceding three months that had not achieved subsequent clinical stabilization. This study adhered to the STROBE guidelines for cross-sectional studies and considered relevant items from the CHERRIES checklist for online surveys (Supplementary materials).
Procedures
The questionnaire employed in this study was meticulously developed through a comprehensive process that involved an extensive review of pertinent domestic and international literature, clinical practice guidelines, and insights derived from routine hemodialysis care18,19,20,21,22. Members of the research team, including nephrologists and dialysis nurses, discussed and refined the draft items. To evaluate the instrument’s reliability and validity, a pilot study was conducted involving 39 patients undergoing maintenance hemodialysis. The results indicated satisfactory internal consistency, with a total Cronbach’s alpha coefficient of 0.925. The reliability coefficients for the dimensions of knowledge, attitude, and practice were 0.901, 0.909, and 0.829, respectively, signifying acceptable psychometric properties for this population. In response to participant feedback regarding item clarity, relevance, and comprehensibility, the questionnaire underwent three iterative rounds of revisions. The finalized version, developed in Chinese (a version translated into English was attached as an Appendix 1), encompassed four dimensions: demographic and clinical characteristics (13 items), knowledge of AVF function (10 items), attitudes toward AVF maintenance (10 items), and self-reported practices related to AVF care and monitoring (10 items). No structured or regular AVF educational sessions were organized by the research team or the participating center. The questionnaire included an item asking whether patients had ever participated in any form of AVF-related education or training (such as hospital sessions, community programs, or online lectures) to capture their previous exposure to patient education. The demographics and clinical characteristics section included variables such as age, gender, duration of dialysis, comorbidities, etc.
The knowledge section comprises 10 items, each scored on a scale where participants receive 2 points for “very familiar,” 1 point for “heard of,” and 0 points for “unclear,” resulting in a total score range of 0 to 20 points. The attitude section similarly contains 10 items, employing a five-point Likert scale ranging from “strongly agree” to “strongly disagree,” with scores varying from 5 to 1, yielding a total score range of 10 to 50 points. The practice dimension encompasses 10 items, scored from 5 to 1 based on responses ranging from “always” to “never,” resulting in a score range of 10 to 50 points. Scores exceeding 70% of the maximum possible in each dimension indicate adequate knowledge, a positive attitude, and proactive practices. Scores falling between 50 and 70% of the maximum reflect moderate knowledge, a neutral attitude, and moderate practices23. In the formal survey, the questionnaire consistently demonstrated robust psychometric properties, with an overall Cronbach’s alpha coefficient of 0.9373. The scale coefficients were 0.8821 for knowledge, 0.8315 for attitude, and 0.9267 for practice. The Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy for the overall scale was 0.9701, thereby confirming the appropriateness of the data for factor analysis and validating the instrument’s structural integrity. Construct validity was examined using confirmatory factor analysis (CFA) for the three latent dimensions (Knowledge, Attitude, Practice). The CFA showed acceptable fit to the intended three-factor structure (CFI = 0.916, TLI = 0.910, RMSEA = 0.065, SRMR = 0.047), consistent with commonly used thresholds for good fit (e.g., CFI/TLI ≥ 0.90, RMSEA/SRMR ≤ 0.08). Standardized factor loadings for all retained items were ≥ 0.70. These results support the structural integrity of the instrument.
Questionnaire distribution and quality control
Participants were recruited by a convenience sampling method. Data collection was conducted via an online platform, utilizing the Wenjuanxing applet (https://www.wjx.cn/) integrated into WeChat. Dialysis nurses were available to help patients who were not familiar with smartphone-based questionnaires to ensure that all participants could complete the survey accurately. A QR code was generated and distributed to potential participants, who accessed and completed the questionnaire by scanning the code with their mobile devices. To ensure data integrity, each IP address was restricted to a single submission, and all questionnaire items were set as mandatory.
Three trained research assistants were responsible for initial data screening. They reviewed all submissions for completeness, consistency, and logical coherence. Questionnaires were excluded if they met any of the following criteria: completion time of less than 90 s; response patterns indicating a lack of engagement, such as identical answers across an entire KAP domain; or internal logical contradictions within the responses.
Sample size estimation
Sample size was calculated using the formula for cross-sectional studies24: α = 0.05, \({\text{n}}={\left( {\frac{{{Z_{1 - \alpha /2}}}}{\delta }} \right)^2} \times p \times \left( {1 - p} \right)\) where \({Z_{1 - \alpha /2}}\)=1.96 when α = 0.05, the assumed degree of variability of p=0.5 maximises the required sample size, and δ is admissible error (which was 5% here). The theoretical sample size was 480 which includes an extra 20% to allow for subjects lost during the study.
Statistical analysis
Statistical analysis was performed using Stata version 17.0 (StataCorp, College Station, TX, USA). Continuous variables were summarized as means and standard deviations (SD), and categorical variables were presented as frequencies and percentages (n, %). For continuous variables exhibiting a normal distribution, comparisons were conducted using independent sample t-tests or analysis of variance (ANOVA). In contrast, variables characterized by skewed distributions were analyzed using the Wilcoxon-Mann-Whitney test or Kruskal-Wallis ANOVA. Multivariable logistic regression analysis was executed to investigate associations between demographic variables and levels of proactive practices. The correlations between KAP dimension scores were assessed using Spearman correlation analysis. Structural equation modeling (SEM) was utilized to investigate the interrelationships among the constructs of knowledge (K), attitudes (A), and practices (P). The hypotheses posited by the SEM framework were as follows: (1) knowledge directly influences attitude, (2) attitude directly influences practice, and (3) knowledge influences practice both directly and indirectly. These pathways are theoretically grounded in the KAP model, which suggests that knowledge shapes attitudes and subsequently influences behaviors25. An acceptable model fit was established in accordance with established criteria. The evaluation of the factor structure encompassed standardized factor loadings, critical ratios (C.R.), and fit indices, including the Root Mean Square Error of Approximation (RMSEA Reference: < 0.08 good), Standardized Root Mean Square Residual (SRMR Reference: < 0.08 good), Tucker-Lewis Index (TLI Reference > 0.08 good), and Comparative Fit Index (CFI Reference: > 0.8 good). All statistical tests were two-sided, and P-values < 0.05 were considered statistically significant.
Results
Questionnaires quality verification
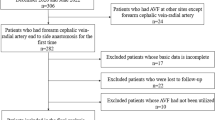
Initially, a total of 565 samples were collected. The following were excluded: 23 responses with abnormal completion times (less than 90 s or more than 3000 s); 3 responses without informed consent;1 response with abnormal gender information༛2 responses with abnormal age entries. The final valid sample size was 536 cases, with a valid rate of 94.87%.
Demographic characteristics on participants and KAP scores
The study included 536 hemodialysis patients (62.1% male; mean age: 51.7% aged 45–64 years), predominantly married (84.9%), Han Chinese (98.9%), and from rural/urban settings (94%). The mean knowledge, attitude, and practice scores were 14.74 ± 4.89 (possible range: 0–20), 42.84 ± 4.87 (possible range: 10–50), and 40.75 ± 7.89 (possible range: 10–50), respectively. Ethnic minority participants scored substantially lower in knowledge (9.33 ± 5.05 vs. 14.81 ± 4.86 for Han, P = 0.007), attitude (32.67 ± 9.00 vs. 42.96 ± 4.69, P = 0.006), and practice (31.67 ± 7.99 vs. 40.85 ± 7.84, P = 0.011). Suburban residents demonstrated the poorest knowledge (P = 0.030) and practice scores (P = 0.091). Patients with longer dialysis duration (> 2 years) exhibited superior knowledge (P < 0.001), attitude (P < 0.001), and practice scores (P = 0.044). Regular post-hemodialysis check-ups strongly correlated with enhanced KAP outcomes: participants with check-ups scored higher in knowledge, attitude, and practice (all P < 0.001). Those with family members undergoing hemodialysis achieved better knowledge (P < 0.001) and practice scores (P = 0.007). Patients with “other” causes of renal failure (e.g., polycystic kidney disease) showed the highest knowledge and attitude scores (P = 0.001), while diabetic nephropathy patients scored lowest in knowledge (Table 1).
Distribution of knowledge, attitude, and practice dimension
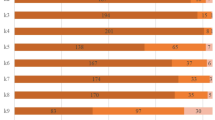
The distribution of knowledge dimensions showed that the three questions with the lowest number of participants choosing the ‘Very familiar’ option were ‘PTA is currently the main surgical method for treating AVF stenosis.’ (K10) with 44.4%, ‘AVF stenosis is mainly caused by postoperative venous intimal hyperplasia.’ (K9) with 44.96%, and ‘There are currently three main types of vascular access for hemodialysis: native AVF, prosthetic graft AVF, and central venous catheter, with native AVF being the first choice for patients.’ (K3) with 50% (Supplementary Table S1). For most of the attitude dimension items, more than 90% of the participants were quite positive (choosing either ‘strongly agree’ or ‘agree’), except for A2, where 23.32% firmly believed and 15.67% also endorsed that AVF surgery has many complications and is therefore unnecessary (Supplementary Table S2). Responses to the practice dimension showed that only 33.77% always try to elevate the limb with the fistula to promote venous return and reduce swelling in their daily activities (P2), only 35.63% always actively seek to learn about AVF surgery-related knowledge (P1), only 37.87% always participate in educational sessions on how to maintain AVF function and consistently perform AVF function exercises as recommended (P8) (Supplementary Table S3).
Univariate and multivariable logistic regression analysis
Multivariable logistic regression showed that living in suburban (OR = 0.378, 95% CI: [0.163,0.878], P = 0.024), with associate / bachelor’s degree (OR = 2.737, 95% CI: [1.204,6.225], P = 0.016), unsure if family member underwent haemodialysis (OR = 0.065, 95% CI: [0.008,0.559], P = 0.013), dialysis for more than 2 years (OR = 2.123, 95% CI: [1.317,3.422], P = 0.002), and without regular check-ups after hemodialysis treatment (OR = 0.493, 95% CI: [0.295,0.823], P = 0.007) were independently associated with knowledge. Meanwhile, knowledge score (OR = 1.468, 95% CI: [1.376,1.566], P < 0.001) was independently associated with positive attitude. Furthermore, knowledge (OR = 1.278, 95% CI: [1.193,1.370], P < 0.001), attitude (OR = 1.223, 95% CI: [1.137,1.316], P < 0.001), aged 45–64 years (OR = 2.121, 95% CI: [1.178,3.820], P = 0.012), aged more than 65 years (OR = 2.487, 95% CI: [1.151,5.373], P = 0.020), with monthly income per capita (OR = 0.218, 95% CI: [0.090,0.528], P = 0.001), and with hypertensive renal damage (OR = 2.071, 95% CI: [1.099,3.901], P = 0.024) were independently associated with practice (Table 2, Supplementary table S4).
Spearman correlation analysis and structural equation model analysis
Significant positive correlations between knowledge and attitude (r = 0.682, P < 0.001) as well as practice (r = 0.711, P < 0.001). Also, there was a correlation between attitude and practice (r = 0.622, P < 0.001) (Table 3). The SEM demonstrated highly favorable model fit indices: RMSEA value of 0,071 (Reference: < 0.08), SRMR value of 0.048 (Reference: < 0.08), TLI value of 0.910 (Reference > 0.08 good), CFI value of 0.910 (Reference: > 0.8 good), suggesting a well-fitting model (Supplementary Table S5). The SEM analysis showed that knowledge directly affected both attitude (β = 0.752, P < 0.001) and practice (β = 0.388, P < 0.001), as well as of attitude on practice (β = 0.449, P < 0.001), furthermore, knowledge indirectly affected practice through attitude (β = 0.337, P < 0.001) (Supplementary Table S6, Table 4; Fig. 1).

SEM model.
Discussion
Hemodialysis patients demonstrated moderate levels of knowledge, generally positive attitudes, and relatively active practices regarding the functional status of arteriovenous fistulas. These findings highlight the need for targeted, knowledge-based educational interventions that can simultaneously enhance attitudes and promote evidence-based self-care behaviors to optimize AVF maintenance and dialysis outcomes.
The current findings elucidate the knowledge, attitudes, and practices of hemodialysis patients concerning the management of AVF. While a majority of participants in this study demonstrated elevated scores in their attitudes toward AVF and attained an overall practice score of 40.75 out of 50—significantly exceeding the ‘high level’ threshold of 30—a detailed analysis of the practice dimension revealed specific challenges. Certain proactive behaviors, such as attending educational sessions and conducting regular, comprehensive assessments of their fistulas, were reported less frequently than fundamental adherence behaviors. This discrepancy within the practice dimension highlights a barrier to the transition from knowledge and positive attitudes to sustained, proactive self-care actions. Such phenomena are not uncommon in health behavior research. According to the Health Belief Model (HBM), even when patients possess adequate knowledge and a favorable attitude, uncertainties regarding procedures, perceived risks, and low self-efficacy can obstruct the initiation of health-related behaviors26,27. Therefore, in AVF health education, it is crucial not only to convey knowledge but also to apply behavioral intervention techniques—such as motivational interviewing and scenario-based simulation training—to enhance patients’ self-efficacy and willingness to act28,29. A central feature of the data is the strong predictive role of knowledge across the model. In both correlation and structural equation analyses, knowledge was not only associated with attitude and practice but exerted a substantial total effect on each. The observed pathways suggest that the internalization of key clinical information is not merely a parallel factor, but a core component shaping behavioral participation and attitudinal stance30,31. Furthermore, the SEM results in this study revealed that attitude mediates the relationship between knowledge and behavior, with the indirect path knowledge → attitude → behavior having a stronger effect than the direct knowledge → behavior path. This finding underscores the importance of focusing on the cognitive-to-intentional process in educational interventions. Improving knowledge alone may not directly translate into behavior change; rather, it is essential to strengthen the cognitive foundation, cultivate positive attitudes, and build behavioral intention to facilitate the transformation from “knowing” to “believing” and ultimately to “acting”32,33,34.
Differences in knowledge scores were particularly evident across educational levels and dialysis duration. Patients with higher formal education tended to perform better in knowledge assessments. This outcome is consistent with observations in chronic disease management where literacy and comprehension are closely linked to formal educational exposure35,36. Longer dialysis duration was also associated with higher knowledge scores, a trend potentially attributable to repeated clinical encounters and gradual assimilation of disease-related information over time. Such time-linked increases in procedural understanding have been described in cohorts managing conditions that require ongoing self-care37,38.
The lower scores observed among suburban patients raise specific concerns. Compared to both rural and urban residents, this subgroup demonstrated reduced knowledge levels, a disparity that persisted even after adjusting for socioeconomic and clinical covariates. It is possible that suburban patients occupy a structural blind spot within current health service delivery models. Unlike rural patients who may benefit from targeted outreach, and urban residents who typically access higher-tier services, suburban populations often lack both proximity and prioritization in resource allocation39,40.
Examination of individual knowledge items reveals variation in content-specific familiarity. While basic concepts, such as the surgical nature of AVF and general care precautions, were widely recognized, responses to more specialized items—particularly those involving AVF complications and interventional procedures—were less encouraging. Items related to PTA, stenosis mechanisms, and long-term fistula function received lower recognition. This divergence between foundational and procedural knowledge has been reported in other chronic care contexts, often resulting from inadequate reinforcement of advanced topics during standard consultations41,42. The limited familiarity with interventional aspects may reflect both the complexity of these topics and a lack of tailored education following initial surgery. These observations are consistent with recommendations in the Vascular Access Handbook for People with Kidney Disease, which emphasizes structured patient education on access maintenance and early recognition of complications. Incorporating such practical guidance into routine care may help close the gap between foundational knowledge and procedure-specific understanding43.
Attitudinal responses were generally favorable, with most patients acknowledging the importance of shared responsibility in AVF maintenance and expressing trust in clinical processes. However, some items revealed uncertainty. A notable proportion of participants expressed ambivalence regarding the necessity of AVF surgery or its associated risks. While such concerns may partially stem from personal experiences or procedural anxiety, they may also indicate gaps in communication or insufficient contextualization of clinical information. Research in chronic disease patient populations has shown that even when basic understanding is present, incomplete or one-way communication about treatment risks often leads to hesitant or neutral attitudes30,44.
Multivariable analysis showed that, beyond knowledge, few demographic or economic variables consistently predicted attitudinal stance. Regular check-ups initially appeared linked to more favorable attitudes but did not retain predictive power when knowledge was accounted for. This may suggest that continuity of care alone does not necessarily alter beliefs unless supported by substantive educational interactions. Some previous studies in primary care settings have similarly highlighted that routine follow-up without structured communication fails to modify patient expectations or concerns meaningfully45,46.
As for practice, patients generally reported active involvement in AVF-related behaviors. The model confirmed that both knowledge and attitude contributed to practice, with the indirect effect of knowledge through attitude being particularly prominent. However, certain behaviors—such as attending educational sessions or conducting regular fistula assessments—showed relatively lower frequencies. While most patients adhered to basic physical protection and monitoring, actions that required proactive initiative or long-term consistency were reported less often. This gap may reflect a broader challenge in chronic care, where initial engagement with self-management often declines over time without reinforcement structures or practical scaffolds47,48.
Practice variation by income level and age introduces further complexity. A noteworthy finding of this study is that patients in the middle-income group exhibited lower behavior scores compared to the low-income group. This counterintuitive result may reflect real-world constraints related to work pressure, time availability, and limited access to healthcare services. Previous research has shown that some middle-income hemodialysis patients, lacking flexible time or caregiving resources, often fall into a “blind spot” in healthcare utilization—neither qualifying for subsidies nor having enough disposable time or support to engage in sustained self-management49,50,51. These structural challenges suggest that future interventions should adopt more targeted and accessible strategies to support this population, ensuring feasible and sustainable behavior change. Patients in mid-income brackets showed lower engagement than expected, suggesting that financial status alone does not uniformly predict adherence. In some cases, individuals with moderate income may experience higher occupational burden or time constraints, reducing their capacity to implement recommended behaviors. In other health domains, such as cardiovascular risk management, similar inverted trends have been observed, where moderate-income individuals face both limited public support and insufficient private health coverage, creating a structural disadvantage52,53.
These findings support the need for context-sensitive interventions. Educational materials should not only be simplified for low-literacy groups but also adapted to address the procedural gaps identified in higher-educated patients. Follow-up visits could include structured behavioral feedback, focusing not only on clinical outcomes but also on patients’ engagement with recommended practices. For patients with longer dialysis histories, individualized education refreshers might be introduced to maintain long-term adherence and prevent information decay54,55.
Suburban populations may benefit from mobile educational outreach or region-specific digital platforms, especially if conventional health education resources remain centralized. Clinics could consider brief, structured learning components integrated into dialysis sessions, allowing patients to review one procedural topic at a time. For behavioral practices that require sustained effort, such as exercise adherence or at-home monitoring, pairing patients with peer mentors who model and reinforce these behaviors has shown positive results in other chronic disease models56,57.
This study has several limitations. First, the use of self-reported data may introduce recall or social desirability bias, potentially affecting the accuracy of responses on knowledge, attitudes, and practices. Second, psychological or behavioral factors such as health literacy, self-efficacy, and behavioral intention were not assessed, although previous research has identified health literacy as an important determinant of self-management among hemodialysis patients58. Future studies should incorporate validated instruments such as the HeLP-CKD health literacy scale and adopt larger, stratified, and longitudinal designs to enhance generalisability and explanatory power59. Mixed-method approaches combining quantitative data with qualitative interviews or behavioral observations may further improve the depth and authenticity of findings60. In addition, the study was conducted in a single center with a convenience sample, limiting the generalisability of results to other regions. Because the survey was conducted online, patients needed to be familiar with digital devices, which may have introduced selection bias. Not all potentially relevant characteristics were included as covariates in the SEM, which may leave residual confounding. As this was a cross-sectional study, the observed associations cannot be interpreted as causal. Finally, some questionnaire items included more than one related concept to reflect clinical practice, which may have influenced item clarity and interpretation.
Conclusion
In conclusion, hemodialysis patients demonstrated varying degrees of knowledge, attitudes, and practices concerning the functional status of AVF, with significant interrelationships observed among these dimensions. Targeted educational interventions that enhance patients’ understanding and attitudes may facilitate more consistent and effective self-care practices, ultimately contributing to improved AVF maintenance and dialysis outcomes.
Data availability
All data generated or analysed during this study are included in this published article.
References
Thurlow, J. S. et al. Global epidemiology of End-Stage kidney disease and disparities in kidney replacement therapy. Am. J. Nephrol. 52, 98–107 (2021).
Lawson, J. H., Niklason, L. E. & Roy-Chaudhury, P. Challenges and novel therapies for vascular access in haemodialysis. Nat. Rev. Nephrol. 16, 586–602 (2020).
Bello, A. K. et al. Epidemiology of haemodialysis outcomes. Nat. Rev. Nephrol. 18, 378–395 (2022).
Liu, J. et al. Epidemiological analysis of death among patients on maintenance hemodialysis: results from the Beijing blood purification quality control and improvement center. BMC Nephrol. 24, 236 (2023).
Yeh, L. M., Chiu, S. Y. & Lai, P. C. The impact of vascular access types on Hemodialysis patient Long-term survival. Sci. Rep. 9, 10708 (2019).
Sequeira, A., Naljayan, M. & Vachharajani, T. J. Vascular access guidelines: summary, rationale, and controversies. Tech. Vasc. Interv. Radiol. 20, 2–8 (2017).
Venegas-Ramírez, J. et al. Vascular access type and survival outcomes in hemodialysis patients: a seven-year cohort study. Med. (Kaunas) 2025, 61 (2025).
Pisoni, R. L. et al. International differences in the location and use of arteriovenous accesses created for hemodialysis: results from the Dialysis outcomes and practice patterns study (DOPPS). Am. J. Kidney Dis. 71, 469–478 (2018).
Ghimire, A. et al. Global variations in funding and use of Hemodialysis accesses: an international report using the ISN global kidney health atlas. BMC Nephrol. 25, 159 (2024).
Bylsma, L. C., Gage, S. M., Reichert, H., Dahl, S. L. M. & Lawson, J. H. Arteriovenous fistulae for haemodialysis: a systematic review and Meta-analysis of efficacy and safety outcomes. Eur. J. Vasc Endovasc Surg. 54, 513–522 (2017).
MacRae, J. M. et al. Arteriovenous access Failure, Stenosis, and thrombosis. Can. J. Kidney Health Dis. 3, 2054358116669126 (2016).
Zhao, F. Y. et al. Knowledge about, attitude toward, and practice of complementary and alternative medicine among nursing students: a systematic review of cross-sectional studies. Front. Public. Health. 10, 946874 (2022).
Wang, J., Chen, L., Yu, M. & He, J. Impact of knowledge, attitude, and practice (KAP)-based rehabilitation education on the KAP of patients with intervertebral disc herniation. Ann. Palliat. Med. 9, 388–393 (2020).
Zhou, H., Zhao, R. & Yang, Y. A qualitative study on Knowledge, Attitude, and practice of nursing students in the early stage of the COVID-19 epidemic and inspiration for nursing education in Mainland China. Front. Public. Health. 10, 845588 (2022).
Xu, F. et al. Knowledge, attitude, and practice of patients receiving maintenance Hemodialysis regarding Hemodialysis and its complications: a single-center, cross-sectional study in Nanjing. BMC Nephrol. 24, 275 (2023).
Huang, S., Liu, X., Liu, Y. & Liu, D. Knowledge, attitudes and practices regarding arteriovenous fistulas among uremic patients undergoing haemodialysis in china: a cross-sectional study. BMJ Open. 15, e089844 (2025).
Dev, S. et al. Knowledge, Attitude, and practice on arteriovenous fistula care among End-Stage kidney disease patients receiving maintenance hemodialysis: a Single-Center, prospective cohort study in Nepal. Health Sci. Rep. 8, e70823 (2025).
Expert Consensus Working Group of Nephrology and Blood Purification Branch of Beijing Perioperative Medical Research Society, Zhang, D. & Yang, T. Expert consensus on perioperative management of newly established autologous arteriovenous fistula. Blood Purif. China. 22, 881–890 (2023).
Li, M., Xu, J. & Peng, J. Summary of the best evidence for self-care of autologous arteriovenous fistulas in maintenance Hemodialysis patients. Int. J. Nurs. Sci. 31, 56–63 (2024).
Shen, P., Li, H. & Guo, J. Summary of the best evidence for the prevention of autologous arteriovenous fistula thrombosis in Hemodialysis patients. Chin. J. Nurs. 57, 1634–1640 (2022).
Grafts., C. E. C., Xiao, G. & Xia, J. W. G. Chinese expert consensus on the nursing of arteriovenous Fistulas in Hemodialysis grafts (1st Edition). Blood Purific. China 24, 89–107 (2025).
Gallieni, M. et al. Clinical practice guideline on peri- and postoperative care of arteriovenous fistulas and grafts for haemodialysis in adults. Nephrol. Dial Transplant. 4 (12), 2203 (2020).
Lee, F. & Suryohusodo, A. A. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, indonesia: a cross-sectional study. Front. Public. Health. 10, 957630 (2022).
Charan, J. A. T. B. How to calculate sample size for different study designs in medical research? Indian J. Psychol. Med. 35 (2), 121–126 (2013).
Andrade, C. Designing and conducting Knowledge, Attitude, and practice surveys in psychiatry: practical guidance. Indian J. Psychol. Med. 42 (5), 478–481 (2020).
Glanz, K. & Viswanath, R. B. K. Health Behavior: Theory, Research, and Practice (Jossey-Bass, 2015).
IM, R. Historical origins of the health belief model. Health Educ. Monogr. 2 (4), 328–335 (1974).
Butler, A. Self-Efficacy: The Exercise of Control (Freeman, 1997).
Miller, W. R. R. S. Motivational Interviewing: Helping People Change (Guilford Press, 2012).
Luo, Y. et al. Construction and validation of a scale to assess knowledge, attitude, and practice regarding vascular protection anticipatory to the creation of an arteriovenous fistula. J. Vasc. Access 2024, 11297298241258793 (2024).
Natti Krishna, V. et al. Knowledge of arteriovenous fistula care in patients with end-stage kidney disease in South Asian countries: a systematic review and meta-analysis. Chronic Illn. 20, 23–36 (2024).
D, N. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 15 (3), 259–267 (2000).
Yang, F. Health literacy and self-management behavior among maintenance Hemodialysis patients: a structural equation modeling approach. Int. J. Nurs. Sci. 8 (1), 52–59 (2021).
Zhang, H. The mediation effect of attitude on knowledge and self-management behaviors in Hemodialysis patients. Patient Educ. Couns. 103 (6), 1141–1147 (2020).
Li, C., Lin, Y., Cheng, J., Xu, D. & Zhang, L. Psychometric properties of the Chinese version of scales of knowledge, attitude, and practice of self-care for patients with arteriovenous fistula: a translation and verification study. Front. Public. Health. 13, 1588271 (2025).
Pessoa, N. R. C. et al. Development and psychometric testing of scales of Knowledge, Attitude, and practice of Self-Care for patients with arteriovenous fistula. J. Nurs. Meas. (2024).
Alsolami, E. & Alobaidi, S. Hemodialysis nurses’ knowledge, attitude, and practices in managing vascular access: a cross-sectional study in Saudi Arabia. Med. (Baltim). 103, e37310 (2024).
Shamasneh, A. O., Atieh, A. S., Gharaibeh, K. A. & Hamadah, A. Perceived barriers and attitudes toward arteriovenous fistula creation and use in Hemodialysis patients in Palestine. Ren. Fail. 42, 343–349 (2020).
Cao, M. C., Jia, R. F., Wang, Y. F., Pan, K. L. & Hu, J. The effects of health education and exercise style changes on the maturation of autologous arteriovenous fistula in Hemodialysis patients: a randomized controlled trial. J. Vasc Access. 26, 271–279 (2025).
Fielding, C. A. et al. Managing access by generating improvements in cannulation: a National quality improvement project. J. Vasc Access. 22, 450–456 (2021).
Alaridah, N. et al. Knowledge, attitude, and practices toward hepatitis B infection among Hemodialysis patients: a nationwide study in Jordan. PLoS One. 19, e0312226 (2024).
Hu, X. et al. Knowledge, attitude, and practice of nephrologists on the decision for renal replacement therapy. BMC Public. Health. 23, 654 (2023).
Roca-Tey, R. et al. Vascular access handbook for people with kidney disease. ISBN: 978-84-09-28494-8; e-ISBN: 978-84-09-28498-6. Available at: www.gemav.org (2021).
Medeiros, L. P. et al. Knowledge of and adherence to standard precautions in a Hemodialysis unit: a cross-sectional study. Sao Paulo Med. J. 140, 297–304 (2022).
Chen, Z. et al. Dietary knowledge-attitude-practice status in Hemodialysis patients: a latent profile analysis. BMC Public. Health. 24, 836 (2024).
Kilic, E. & Kavurmaci, M. Hemodialysis patients’ knowledge of, beliefs about, and practices in using complementary and alternative medicine: an exploratory study. Altern. Ther. Health Med. 28, 30–34 (2022).
Prevyzi, E. et al. Perceptions of teamwork and knowledge attitudes of Hemodialysis unit nurses on infection prevention. Adv. Exp. Med. Biol. 1425, 555–565 (2023).
Wu, R. et al. Effect of self-determination theory on knowledge, treatment adherence, and self-management of patients with maintenance hemodialysis. Contrast Media Mol Imaging 2022, 1416404 (2022).
Liu, L. Barriers to healthcare access among middle-income patients with chronic diseases in urban China. BMC Health Serv. Res. 20, 874 (2020).
Marmot, M. Social determinants of health inequalities. Lancet 365 (9464), 1099–1104 (2024).
Wang, Y. Socioeconomic disparities in chronic disease outcomes: a review of evidence from China. Lancet Public. Health. 6 (6), e327–e338 (2021).
Chen, J., Lu, J., Fu, X. & Zhou, H. The knowledge, attitudes, and practices of arteriovenous access assessment among Hemodialysis nurses: a multicenter cross-sectional survey. Hemodial. Int. 28, 278–289 (2024).
Smith, K. & Ayars, C. Improving vascular access knowledge and assessment skill of Hemodialysis staff. J. Osteopath. Med. 125, 321–327 (2025).
Cashmore, B. A. et al. Education programmes for people with chronic kidney disease and diabetes. Cochrane Database Syst. Rev. 8, Cd007374 (2024).
Dandamudi, R., Twombley, K., Flynn, J. T., Kakajiwala, A. & Chand, D. H. Physician knowledge, attitudes, and practices regarding physical activity restrictions in pediatric Hemodialysis patients. Hemodial. Int. 27, 345–351 (2023).
Inanaga, R. et al. Multidimensional health Literacy, and medication adherence among patients undergoing Long-Term Hemodialysis. Clin. J. Am. Soc. Nephrol. 19, 463–471 (2024). Trust.
Song, Y., Wang, J., Liu, H., Chen, X. & Zhan, M. Diet and culture among Chinese patients undergoing hemodialysis: a qualitative study. Front. Nutr. 9, 876179 (2022).
Green, J. Health literacy and outcomes among patients with chronic kidney disease. Kidney Int. 80 (3), 250–256 (2011).
Polit, D. F. B. C. Nursing Research: Generating and Assessing Evidence for Nursing Practice (Wolters Kluwer, 2016).
Tong, A. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care. 19 (6), 349–357 (2007).
Funding
This work was supported by National Natural Science Foundation of China (82360152).
Author information
Authors and Affiliations
Contributions
Yan Yan and Chengfa Ren carried out the studies, participated in collecting data, and drafted the manuscript. Jiao Huang, Dehui Liu and Xiaoxia Su performed the statistical analysis and participated in its design. Xia Guo, Yanchun Li, Hongyan Peng, Lu Yin, Jun Xiao, Yan Zeng and Yujuan Yang participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by The First Affiliated Hospital of Nanchang University Medical Ethics Committee (Approval No.: IIT [2025] Clinical Ethics Review No. 359). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ren, C., Huang, J., Liu, D. et al. Knowledge, attitudes, and practices regarding the functional status of arteriovenous fistulas among hemodialysis patients. Sci Rep 15, 45622 (2025). https://doi.org/10.1038/s41598-025-30097-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30097-z
