
Abstract
Artificial intelligence (AI) offers opportunities to enhance breast cancer screening by improving diagnostic accuracy and reducing radiologist workload, yet its successful adoption depends on public trust and acceptability. This cross-sectional survey of 562 Emirati women aged 18 years and older in Abu Dhabi explored knowledge, perceptions, and willingness to participate in AI-supported screening. Using a structured, culturally adapted questionnaire, descriptive statistics summarized attitudes and concerns, and logistic regression identified predictors of AI-related knowledge. Most participants (69%) believed AI could improve diagnostic accuracy, although only 11% fully trusted AI without human oversight. Human clinicians remained central to decision-making, with 86% of women preferring physician judgment in cases of conflict between AI and radiologist findings. Willingness to undergo AI-supported screening was high (74%), though concerns about false results (59%) and data misuse (36%) were prevalent. Being a health professional (aOR = 2.76, 95% CI: 1.23–6.43) and having higher knowledge of breast screening methods (aOR = 8.29, 95% CI: 3.98–18.6) were significantly associated with awareness of AI use in breast cancer screening. These findings indicate that while Emirati women show cautious support for AI in breast cancer screening, trust, cultural values, and baseline knowledge are key determinants of acceptance. Public health strategies that emphasize transparent communication, robust data protection, and education on both conventional and AI-assisted screening are essential to promote equitable and ethical integration of AI technologies into cancer control programs.
Similar content being viewed by others

Introduction
Breast cancer (BC) remains the most frequently diagnosed cancer among women globally, with 2.3 million new cases and 670,000 deaths in 2022. In the United Arab Emirates (UAE), BC accounts for 21.4% of all cancers, with 1,030 new cases reported in 2020, and incidence among women under 50 is rising1,2.
Early detection through screening is central to BC control. Mammography is widely used, with high specificity but only moderate sensitivity, particularly in women with dense breast tissue3,4. Despite availability, BC screening uptake is low, as only 13.9% of women aged 40–75 in the UAE reported participation, compared with < 15% in neighboring Gulf countries and > 80% in parts of Europe5,6.
Amidst these challenges, artificial intelligence (AI) has emerged as a promising adjunct to mammography7. AI systems have demonstrated accuracy comparable to radiologists and can reduce false positives/negatives while alleviating workload8,9,10,11,12. Regionally, the Department of Health (DOH) in Abu Dhabi, in partnership with New York University (NYU) and NYU Abu Dhabi, developed an AI tool for breast ultrasound with performance comparable to that of experts13.
Despite these technological advances, public trust and acceptance remain pivotal for the successful implementation of AI in BC screening14. Studies from Europe suggest that women value AI as a supportive tool, but not as a replacement for radiologists, with concerns about accountability and the final decision-making process15,16. Evidence on women’s perceptions regarding use of AI in BC screening in the UAE remains limited. This study, therefore, aims to assess Emirati women’s perspectives on integrating AI into BC screening, focusing on trust, perceived accuracy, and acceptability.
Results
Participants’ characteristics
A total of 562 women participated in the study, of whom 7% reported working in health-related professions. Most participants were aged 18–29 years (43%), followed by those aged 40–49 years (25%). Over half (54%) resided in the Emirate of Abu Dhabi (including Abu Dhabi city and Al Ain), and the majority (65%) held a bachelor’s degree. Additionally, 39% reported having previously undergone BC screening, and 4% had received a cancer diagnosis. A family history of cancer was reported by 41% of participants, with BC being the most frequently cited type (47%) (Table 1).
Attitudes toward the use of AI in BC screening
Overall, participants expressed cautious optimism toward the integration of AI in BC screening. A majority (69%) believed that AI has the potential to enhance the accuracy of BC detection. However, only 11% indicated full trust in an AI-generated diagnosis without human oversight, while most (86%) preferred to defer to a human doctor in cases where AI and physician diagnoses diverged. Personalized diagnosis was cited as a key advantage of human doctors in such scenarios (Fig. 1). In terms of acceptability, 74% expressed willingness to undergo BC screening if it involved AI technologies, and 63% believed AI could support early-stage detection. Nonetheless, concerns were evident: 59% were apprehensive about the risk of false positives or false negatives, and over one-third (36%) expressed unease regarding potential secondary use of their personal data by AI systems. More than half (59%) agreed that AI-based screening is culturally and ethically acceptable within the UAE context (Supplementary Table S1).
Bars represent the percentage of respondents who preferred AI over human doctors (blue, n = 97) for attributes such as accuracy, objectivity, and consistency; and those who preferred human doctors over AI (n = 483) for attributes such as personalized care, complex case analysis, and comprehensive disease assessment.

Comparison of perceived strengths of AI and human doctors in BC screening
Knowledge of AI in BC screening
More than a third (35%) of participants reported knowledge of the usability of AI in the medical field, including BC screening (BCS). Specifically, about 8% self-reported having good knowledge, while 27% indicated having some general knowledge of the topic. The remaining 65%, which constitutes the majority, indicated that they had never heard of AI being used in the medical field, including BC screening.
Knowledge of AI use in BC screening is associated with the participants’ job category and their familiarity with BC screening methods (Table 2). Individuals in health professions were nearly three times more likely to have knowledge of AI use in BC screening compared to those in non-health professions (aOR = 2.76, 95% CI = 1.23–6.43, p = 0.015). Similarly, those with very good (aOR = 8.29, 95% CI = 3.98–18.6, p < 0.001) and intermediate (aOR = 3.40, 95% CI = 1.68–7.41, p = 0.001) knowledge of BSC methods were significantly more likely to have knowledge of AI use in BC screening than those who lacked such knowledge.
Perceptions and expectations of AI in BC screening
Most participants viewed AI either as a tool to improve the accuracy of BC screening (68%) or as a technology for medical image analysis (43%). When asked about the potential advantages of AI in BC screening (Fig. 2), the most frequently mentioned advantages were promoting early detection (58%), reducing the rate of missed and misdiagnosed diagnoses (44%), and improving the accuracy of doctors’ advice (42%). As per drawbacks, the most frequently cited were lack of human care (56%), inability to cope with complex disorders (49%), and concerns about excessive reliance on AI without human oversight (48%). When asked whether they would expect a human physician to be present in an AI clinic for BC screening, the majority of the participants (68%) preferred having a human physician present.

Perceived advantages and drawbacks of AI in BC screenings.
Discussion
This study demonstrates cautious support for AI integration into BC screening services among Emirati women, coupled with a clear desire to retain the human element in healthcare. A large majority believed AI could improve screening accuracy (69%) and aid early detection (63%), reflecting international trends of generally positive attitudes toward AI’s diagnostic potential16. For instance, in a recent survey of screening-eligible women in Europe, 88% viewed medical AI favorably and acknowledged its utility in mammography17. Our participants’ high willingness to undergo AI-based screening (74% ready or very ready) in line with such global optimism. However, trust in AI as an independent diagnostician remains limited. Consistently, an overwhelming 86% of participants in our study reported that they would seek a human doctor’s advice if an AI’s assessment conflicted with a physician’s finding, aligning with international data showing 94% of women insist radiologists should always provide their own mammography report16. These patterns underscore a common perception of AI as a useful adjunct but not a replacement for human expertise in BC screening18. In line with this, 77% of European screening participants agreed that AI should be used at least as a second reader, rather than a stand-alone tool,16 and only 4% of women were comfortable with AI serving as the sole reader of mammograms19. Together, these findings highlight that while patients appreciate AI’s potential benefits, they fundamentally trust the human touch, valuing the reassurance, personalized judgment, and accountability that human doctors provide.
Participants’ concerns further emphasize the need for a human-centered approach to AI integration. Over half (59%) expressed worry about false-positive or false-negative results with AI. This caution is well-founded and resonates with themes from qualitative studies in England and Australia, where women emphasized the high stakes of accuracy in screening and demanded that new technologies be virtually infallible before adoption20,21. In addition, more than one-third of participants (36%) in our study were concerned about how AI might use their personal health data a reflection of growing global apprehension regarding data privacy and misuse in healthcare AI. Such concerns in our Emirati sample suggest that transparency in how AI systems use and protect patient data will be pivotal for building trust. A recent study on the use of AI in medical imaging among UAE patients reported that 80.5% of patients have concerns about data security22. Findings from focus group discussions in the UK have similarly reported wariness about data sharing and ownership, with women querying who controls their medical data, how securely it is stored, and whether companies might profit from it without patient benefit21. Indeed, literature emphasizes that trust in AI is tightly linked to assurances of privacy, security, and transparency in algorithmic decision-making15. Participants in multiple settings have voiced fears of “black box” AI errors, potential bias, and loss of control, indicating that explainable and ethically governed AI is necessary to gain public confidence17,23.
An intriguing finding in our study is the relatively high proportion of women willing to participate in AI-based screening (74%), which compares favorably to acceptability rates reported in other countries16,24. This suggests that with proper implementation, AI-driven screening could achieve public support in the UAE. However, it must be noted that willingness coexists with caution: many participants, as in other regions, view AI as an adjunct that improves coverage and accuracy, such as reducing missed cancers, rather than a magic solution. The perceived advantages our respondents cited; early detection, fewer missed diagnoses, and improved accuracy of doctors’ decisions, match well with expectations reported in the literature21.
Importantly, the drawbacks noted (lack of human care, inability to handle complex cases, over-reliance on technology) highlight a fear that medicine could become dehumanized if AI eclipses clinician involvement. This reflects the broader theme of “humanization of healthcare in the era of AI”: patients fear losing the compassionate, context-sensitive care that only humans can provide. Indeed, international research emphasizes that patients place great value on human empathy, two-way communication, and the intuition of experienced physicians, none of which they want sacrificed to automation18,21. Moreover, cultural values emerged as a relevant consideration in this study. While 59% of respondents felt that AI screening aligned with the UAE’s cultural and ethical values, a minority expressed uncertainty or disagreement. In the UAE, where healthcare interactions are strongly shaped by trust, family involvement, and respect for cultural norms, acceptance of AI may depend on whether technologies are implemented in ways that reinforce these values. For example, participants may expect AI to support, but not replace, the interpersonal role of physicians, particularly in sensitive discussions of cancer risk and treatment. This is documented in the literature that most patients in the UAE do not see a fundamental conflict between AI technology and local norms, with 81% expressing comfort with AI-based technology22.
Beyond these patient-centered perspectives, it is important to recognize the broader limitations of AI in BC screening. AI systems are vulnerable to algorithmic bias, as training datasets may not adequately represent diverse populations, leading to unequal performance across demographic groups. The explainability of AI models remains a challenge, with many functioning as “black boxes” that provide outputs without transparent reasoning. This opacity can undermine the trust between clinicians and patients, particularly in contexts where accountability is crucial. Furthermore, there are significant ethical concerns, including questions of liability in the event of errors, equitable access to AI-enhanced services, and the risk of exacerbating health disparities if implementation favors technologically advanced settings. These limitations highlight the necessity for ongoing oversight, robust ethical frameworks, and continued evaluation before large-scale deployment.
Finally, our analysis showed that knowledge of AI use in BC screening was significantly associated with professional background and familiarity with conventional screening methods. Health professionals were nearly three times more likely to report AI awareness compared to those outside the sector, while women with very good knowledge of breast screening methods were more than eight times more likely to be aware of AI compared to those with poor knowledge. These findings underscore the need for broad-based education campaigns to extend AI and cancer screening literacy beyond health professionals to the general population. Embedding AI literacy into national awareness programs could promote equitable knowledge, reduce disparities, and ensure that future implementation is inclusive.
Limitations
Our study has important limitations. The cross-sectional survey design captures opinions at one point in time and cannot establish causality or track how attitudes might change as AI becomes more common. Also, the use of convenience and snowball sampling may introduce selection bias, limiting the representativeness of the sample. For example, participants recruited from clinical settings may differ systematically from those not engaged in healthcare, potentially overestimating awareness of AI. Similarly, snowball sampling may cluster participants with similar sociodemographic profiles. While the sample size was adequate, findings should be interpreted with caution, and generalisability to all Emirati women may be limited. Future studies should consider probability sampling strategies to enhance representativeness. Furthermore, responses were self-reported, which can introduce recall or social desirability biases; for instance, some may overstate trust in doctors or AI to appear prudent or tech-savvy. Moreover, our sample skewed toward younger, well-educated women (nearly half were under 30, and two-thirds held a bachelor’s degree), which may over-represent positive attitudes and knowledge levels. The general female population, especially older or less educated individuals, might have lower awareness or greater scepticism than observed here.
Conclusion
This study assessed Emirati women’s perspectives on the integration of AI into BC screening. Findings indicate cautious support for AI, with a strong preference for human oversight. Awareness of AI was significantly influenced by professional background and knowledge of breast screening methods, underscoring the importance of health literacy. For effective and equitable adoption, implementation strategies should prioritize transparent communication, robust data protection, and culturally sensitive public education. Embedding AI literacy into national cancer awareness campaigns and positioning AI as a supportive tool, rather than a replacement for physicians, may enhance trust and acceptance in the UAE context.
Materials and methods
Study design
This study employed a cross-sectional quantitative design to assess Emirati women’s knowledge, attitudes, and perceptions regarding the use of AI in BC screening to provide a snapshot of public awareness, trust, and accuracy in emerging technologies. The study adhered to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES)25 to ensure transparency and quality in online survey design and reporting.
Study setting
The study was conducted in the Emirate of Abu Dhabi one of the largest seven Emirates of the UAE. According to recent statistical reports the UAE has an estimated population of 9.5 million in 2023, of which approximately 69% are males and 31% are females. Emirati nationals comprise around 11% of the total population, while expatriates represent the majority. Women aged 40 years and above, who are the primary target group for BC screening programs, account for nearly 18% of the female population. Data collection took place in clinical settings (BC screening and treatment centers), public recreational spaces, and through online platforms. This multi-modal strategy was designed to maximize reach and inclusiveness across demographic subgroups.
Study population and sampling
The target population comprised Emirati women aged 18 years and older residing in Abu Dhabi. A combination of convenience sampling and snowball sampling was utilized. Initial recruitment occurred at BC screening and treatment centers, where eligible participants were approached in the waiting areas. Convenience sampling was also extended to recreational venues and social media platforms. To further enhance diversity and reach potentially underrepresented or hard-to-reach groups, snowball sampling was employed, and participants were encouraged to refer to others from their social networks who met eligibility criteria.
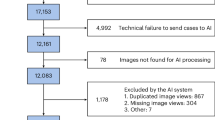
Sample size was calculated using Raosoft sample size calculator, assuming maximum variability at 50% proportion, 95% confidence level, and 5% margin of error, yielding an optimal required sample of 377 participants. To account for a projected non-response rate of 31%, a total of 637 participants were recruited. Of these, 562 completed the survey and were included in the final analysis.
Data collection
Data was collected from December 2024 to March 2025 using a structured, self-administered questionnaire developed following literature review18,22,26,27. The questionnaire was designed to capture demographic information, knowledge of BC screening and AI applications in BC screening, and attitudes toward AI-assisted modalities (Supplementary file 2). Knowledge of BC screening methods was assessed using a self-reported item in which participants were asked to rate their familiarity with these methods. Response options included: “I have no knowledge”, “I have little knowledge”, “I have intermediate knowledge”, and “I have very good knowledge”.
The instrument was developed in English and translated into Arabic using the WHO forward–backward translation protocol to ensure linguistic and cultural validity. The questionnaire underwent content validation by a panel of five subject-matter experts (oncology, public health, medical AI, survey design, and biostatistics) to evaluate clarity, relevance, and coverage. It was pre-tested among 58 Emirati women to assess comprehensibility and contextual appropriateness. Internal consistency reliability was assessed, yielding a Cronbach’s alpha of 0.82 for the attitude’s subscale and 0.79 for the perceptions subscale, indicating acceptable to good reliability. Feedback from expert reviewers and pilot respondents informed revisions prior to final administration.
The final questionnaire was distributed both electronically and in paper format. The survey was fully anonymous, with no personal identifiers collected. For the online version, duplicate entries were minimized by restricting submissions to one per device/browser and by monitoring IP addresses for irregularities. Participants were also given the option to indicate their interest in follow-up semi-structured interviews as part of a nested qualitative phase; contact details for those who volunteered were collected separately to preserve the anonymity of survey responses.
Ethical considerations
Ethical approval for this study was obtained from the United Arab Emirates University (UAEU) Social Sciences Research Ethics Committee (Ref: ERSC_2024_5561). All participants provided informed consent prior to participation. Participation was voluntary, and respondents were informed of their right to withdraw at any point without consequences. Anonymity and confidentiality were ensured throughout the study. All methods were performed in accordance with the relevant institutional guidelines and regulations and adhered to the principles of the Declaration of Helsinki.
Data analysis
All statistical analyses were performed using R version 4.4.1. Descriptive statistics were used to summarize categorical variables as frequencies and percentages. To identify factors associated with participants’ knowledge of AI applications in BC screening, binary logistic regression was conducted. A univariable model was first constructed; variables with a p-value ≤ 0.20 were subsequently included in the multivariable model to adjust for potential confounding. Statistical significance was set at p < 0.05.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Hamza, D. M. M. et al. A retrospective cohort study to evaluate disease burden, health care resource utilization, and costs in patients with breast cancer in Dubai, UAE. BMC Health Serv. Res 24, 810 (2024).
Giaquinto, A. N. et al. Breast cancer statistics 2024. CA Cancer J. Clin. 74, 477–495 (2024).
Farrell, K., Bennett, D. L. & Schwartz, T. L. Screening for breast cancer: what you need to know. Mo Med. 117, 133 (2020).
National Cancer Institute. Mammograms Fact sheet. https://www.cancer.gov/types/breast/mammograms-fact-sheet
So, V. H. T. et al. Uptake of breast and cervical cancer screening in four Gulf Cooperation Council countries. Eur. J. Cancer Prev. 28, 451–456 (2019).
Eurostat Statistics Explained. Cancer screening statistics. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Cancer_screening_statistics#Breast_cancer_screening
Pesapane, F. et al. Deep learning performance for detection and classification of microcalcifications on mammography. Eur Radiol. Exp 7, 69 (2023).
Pesapane, F. et al. Advances in breast cancer risk modeling: integrating clinics, imaging, pathology and artificial intelligence for personalized risk assessment. Future Oncol. 19, 2547–2564 (2023).
Al Muhaisen, S. et al. Artificial Intelligence-Powered Mammography: Navigating the Landscape of Deep Learning for Breast Cancer Detection. Cureus 16, e56945 (2024).
Rodriguez-Ruiz, A. et al. Stand-Alone artificial intelligence for breast cancer detection in mammography: comparison with 101 radiologists. J. Natl. Cancer Inst. 111, 916–922 (2019).
McKinney, S. M. et al. International evaluation of an AI system for breast cancer screening. Nature 577, 89–94 (2020).
Lång, K. et al. Artificial intelligence-supported screen reading versus standard double reading in the mammography screening with artificial intelligence trial (MASAI): a clinical safety analysis of a randomised, controlled, non-inferiority, single-blinded, screening accuracy study. Lancet Oncol. 24, 936–944 (2023).
Rutherford, F. N. Y. U. and NYU Abu Dhabi develop new AI tool for breast cancer detection | Healthcare IT News. (2023). https://www.healthcareitnews.com/news/emea/nyu-and-nyu-abu-dhabi-develop-new-ai-tool-breast-cancer-detection
Pesapane, F. & Cassano, E. Enhancing breast imaging practices: addressing false-positive findings, personalization, and equitable access. Radiology 309, e232189 (2023).
Ongena, Y. P., Yakar, D., Haan, M. & Kwee, T. C. Artificial intelligence in screening mammography: A population survey of women’s preferences. J. Am. Coll. Radiol. 18, 79–86 (2021).
Pesapane, F. et al. Women’s perceptions and attitudes to the use of AI in breast cancer screening: a survey in a cancer referral centre. Br J. Radiol 96, 20220569 (2023).
Pesapane, F. et al. Patients’ perceptions and attitudes to the use of artificial intelligence in breast cancer diagnosis: A narrative review. Life 2024. 14, 454 (2024).
Adams, S. J., Tang, R. & Babyn, P. Patient perspectives and priorities regarding artificial intelligence in radiology: opportunities for Patient-Centered radiology. J. Am. Coll. Radiol. 17, 1034–1036 (2020).
Bersu Ozcan, B., Dogan, B. E., Xi, Y. & Knippa, E. E. Patient perception of artificial intelligence use in interpretation of screening mammograms: A survey study. Radiol Imaging Cancer 7, e240290 (2025).
Carter, S. M., Popic, D., Marinovich, M. L., Carolan, L. & Houssami, N. Women’s views on using artificial intelligence in breast cancer screening: A review and qualitative study to guide breast screening services. Breast 77, 103783 (2024).
Gatting, L. et al. Acceptability of artificial intelligence in breast screening: focus groups with the screening-eligible population in England. BMJ Public. Heal. 2, e000892 (2024).
El-Sayed, M. Z. et al. Patient perspectives on AI in radiology: insights from the united Arab Emirates. Clin. Imaging. 125, 110543 (2025).
Bunnell, A. & Rowe, S. The Effect of AI-Enhanced Breast Imaging on the Caring Radiologist-Patient Relationship. Pacific Symp. Biocomput. 472–483 (2023). https://doi.org/10.1142/9789811270611_0043
Pearce, A. et al. Implementing artificial intelligence in breast cancer screening: women’s preferences. Cancer 131, e35859 (2025).
Eysenbach, G. Improving the quality of web surveys: the checklist for reporting results of internet E-Surveys (CHERRIES). J. Med. Internet Res. 6 (3), e34 (2004). https//www.jmir.org/2004/3/e34 6, e132 (2004).
Elbarazi, I. et al. Knowledge, attitudes and practices of women in the UAE towards breast and cervical cancer prevention: A cross-sectional study. Cancer Control 30, 10732748231211459 (2023).
Pesapane, F. et al. Women’s perceptions and attitudes to the use of AI in breast cancer screening: a survey in a cancer referral centre. Br. J. Radiol. 96, 20220569 (2022).
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
ATR conceptualized and led the study. RA, AA, HA, HAAl, MA, and SA contributed to protocol writing, preparing data collection sheet, participant recruitment, and critically reviewed the manuscript. ASA conducted the data analysis. YAME drafted the initial manuscript, contributed to data visualization and validation, and critically revised the manuscript for important intellectual content. All authors contributed to the writing, review and editing of the manuscript, read and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was reviewed and approved by the Social Sciences Research Ethics Committee at United Arab Emirates University (Ref: ERSC_2024_5561). Informed consent was obtained from all participants prior to data collection. Participation was voluntary, and respondents were assured of their right to withdraw at any time without consequence. All data were collected anonymously and handled in accordance with ethical research standards.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Elhadi, Y.A.M., Abdullahi, A.S., Shamsi, A.A. et al. Women’s perspectives on integrating artificial intelligence in breast cancer screening services in Abu Dhabi, united Arab Emirates. Sci Rep 16, 1209 (2026). https://doi.org/10.1038/s41598-025-30880-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30880-y
