
Abstract
End-stage kidney disease (ESKD) is a growing health issue, especially among the very elderly. The optimal dialysis method for very elderly patients with ESKD remains uncertain, and there is a lack of evidence regarding the survival benefits of hemodialysis (HD) versus peritoneal dialysis (PD). This study is a multicenter cohort investigation that included 234 very elderly patients aged 75 years and older with ESKD who received HD or PD across six hospitals in China from January 2013 to December 2020. We employed Propensity Score Matching (PSM) to minimize the influence of confounding factors. Survival analyses were conducted using Kaplan-Meier curves, log-rank tests, and multivariable Cox proportional hazards regression models for the matched cohorts. In the multicenter cohort study with 234 very elderly ESKD patients, PSM was employed, with each group consisting of 56 participants, averaging 79.76 ± 4.15 years in age and having a male composition of 47.44%. Kaplan-Meier survival analysis indicated with no significant difference in survival rates (log-rank p = 0.123). Further analysis, excluding participants with less than 3 months of survival, also showed no significant differences. Cox regression with multiple variables indicated a HR of 0.73 (95% CI: 0.49, 1.10) for HD versus PD, with a p-value of 0.132. This investigation did not demonstrate a statistically significant difference in survival between PD and HD among very elderly patients with ESKD.
Similar content being viewed by others

Introduction
End-stage kidney disease (ESKD) represents a critical global health issue characterized by a markedly elevated mortality rate1,2. The incidence of ESKD among very elderly people (≥ 75 years old) is four times higher than that of the general adult population3. The latest United States Renal Data System (USRDS) report indicates that the prevalence of ESKD is highest among individuals aged 75 and older4. While kidney transplantation remains the ideal treatment for ESKD, dialysis is often favored for very elderly patients due to high comorbidity rates and limited donor availability5,6,7. The choice of dialysis treatment is crucial for very elderly patients who face challenges such as multiple comorbidities and high mortality rates8,9,10.
The selection of the optimal dialysis modality for elderly patients remains under discussion. Some studies have reported better survival with hemodialysis (HD)11,12,13, whereas others have favored peritoneal dialysis (PD)14. Although several analyses have found comparable outcomes between the two modalities15,16,17, the overall evidence remains inconclusive, particularly for patients aged 75 years and above. However, these studies often treat the elderly population as a homogeneous group, potentially overlooking the unique physiological characteristics of very elderly patients. Two studies focusing on patients older than 75 revealed comparable outlooks for both types of dialysis18,19. Previous studies have mainly focused on Caucasian populations, whose physical characteristics may limit the solute clearance efficiency of PD. The smaller body size of Asian populations could enhance PD effectiveness, indicating potential racial differences that affect the generalizability of findings. Additionally, Western countries typically administer hemodiafiltration (HDF) 1 to 3 times per week, China restricts it to just 1 to 2 sessions per month due to insurance policies. Consequently, the best dialysis modality for very elderly ESKD patients in Asia remains unclear. To resolve this issue, we conducted a comparison of survival rates between HD and PD among Asian very elderly ESKD patients aged 75 and over. Our aim is to provide a theoretical foundation for clinical decision-making.
Materials and methods
Patient selection
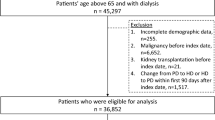
At 6 China hospitals, we performed a multicenter retrospective cohort study of very elderly (≥ 75 years) ESKD patients receiving dialysis. Between January1,2013, and December31,2020, we selected very elderly ESKD patients (aged ≥ 75 years) undergoing HD or PD from The Second Hospital of Jilin University, China-Japan Union Hospital of Jilin University, The First Hospital of Jilin University-the Eastern Division, Jilin First Automobile Work General Hospital, Jilin Central Hospital, and Inner Mongolia Xing’anmeng People’s Hospital. We excluded patients who were age less than 75 years, who were lost to follow-up (23%), or who had incomplete clinical information. The flow chart depicting the process for filtering groups is illustrated in Fig. 1. A regular follow-up was provided to all patients until death, a change in dialysis modality or 29 February 2024. Despite receiving guidance from experienced nephrologists, the ultimate decision regarding dialysis methods was left to the discretion of the patient. In this study, the Ethics Committee of the Second Hospital of Jilin University Hospital approved the study (No.2024317). This study is a retrospective investigation that does not involve the collection or use of patients’ private information. It has been reviewed and approved by the Ethics Committee, and the requirement for informed consent has been waived.

Flowchart of participant inclusion. A total of 304 dialysis patients aged ≥ 75 years were initially enrolled. Seventy patients were excluded due to loss to follow-up (HD = 25, PD = 45), resulting in 234 participants included in the final analysis. After propensity score matching, 112 patients (HD = 56, PD = 56) were analyzed.
Data collection and definitions
We collected baseline data from patients, including age, gender, hypertension, diabetes, hemoglobin levels, serum albumin, creatinine, estimated glomerular filtration rate (eGFR), and chronic disease comorbidities. The primary outcome of this study is all-cause mortality. The follow-up period will conclude on February 29, 2024, upon the occurrence of death, kidney transplantation or a change in dialysis modality, whichever comes first. Survival status was ascertained through hospital electronic medical records, registry verification, and telephone follow‑up performed by experienced dialysis nurses.
Primary exposure
Based on the distinct dialysis modalities employed, we have categorized patients into two groups: HD and PD. For the HD group, patients underwent a rigorous dialysis regimen consisting of 2 to 4 sessions per week, each lasting for 3 to 4 h. Dialysis sessions utilized either semi-synthetic (cellulose diacetate) or synthetic (polysulfone) membranes, paired with a bicarbonate-based dialysate, to ensure optimal filtration and purification. Patients undergoing PD used a 2 L dialysis bag for 3 to 5 daily exchanges, employing PD fluids containing glucose at concentrations ranging from 1.5% to 4.25%, as well as icodextrin PD solutions and neutral PD solutions.
Statistical analyses
For continuous variables, the data are presented as mean (± SD) and median with interquartile range (IQR). Frequency (%) is the display value for categorical variables. Depending on the particular situation, the Student’s t-test, Mann-Whitney U test, or χ² test were used to evaluate differences among groups. Propensity Score Matching (PSM) is used to reduce selection bias and balance baseline characteristics. We utilized a 1:1 PSM method with a caliper value set at 0.2. The matching process accounted for the following covariates: sex, age, hypertension, diabetes, heart failure, Cerebrovascular disease, cancer, Chronic pulmonary disease, Chronic liver disease, Hemoglobin, albumin levels, and eGFR. Covariate balance between two groups was assessed using standardized mean differences (SMDs) (Table S1). An absolute SMD < 0.20 was considered indicative of adequate balance. The Love plot (Supplementary Figure S1) illustrates that all baseline covariates achieved acceptable balance after propensity‑score matching. There were no missing data in the matched cohort. We constructed Kaplan-Meier survival curves and analyzed survival differences by log-rank tests. Multivariate Cox proportional hazard regression model was used to calculate the risk ratio. Subgroup analyses were also performed to further evaluate the survival of HD and PD in different subgroups. A sensitivity analysis was additionally performed after excluding patients who survived less than 3 months to minimize the potential effect of non-disease-related early mortality. We considered statistically significant differences to be P < 0.05. In this study, the data were analyzed using R, version 4.2.0 (the R Foundation) and Empower Stats ((version 4.2).
Results
Baseline characteristics
Table 1 presents the baseline characteristics of all study participants. This study encompassed a total of 234 patients. Initially, before applying PSM, the cohort consisted of 101 patients in the PD group and 133 in the HD group. The PD group presented with lower hemoglobin levels and eGFR when compared with the HD group. Furthermore, the PD group exhibited a higher prevalence of co-existing hypertension, heart failure, and liver disease. Conversely, a comparatively larger proportion of patients in the HD group had tumors. After matched pairs of 56 patients in each group, there were no significant differences in covariates between the two groups.
Analysis of Kaplan-Meier survival curves
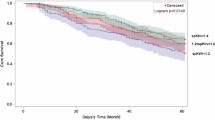
We employed Kaplan-Meier survival curves to assess and compare the survival probabilities of patients in the HD group and PD group (Fig. 2). The median survival time was 18.5 months for the HD group and 16 months for the PD group, with a total of 102 mortality events occurring during the follow-up period (Table S2). During the follow‑up period, seven patients (12.5%) transitioned from PD to HD due to inadequate dialysis adequacy or dialysis‑related complications. For the analysis, patients were classified according to their initial dialysis modality at the start of treatment (intention‑to‑treat principle). The results indicated no significant difference in survival rates between the two groups (log-rank p = 0.123). To enhance the reliability and accuracy of the results, we further excluded patients with a survival period of less than 3 months and found that there were no significant differences in survival rates after matching.

Kaplan-Meier survival curves comparing the survival outcomes of PD and HD treatment. (A) K-M survival curves for the matched cohort, p = 0.123. (B) K-M survival curves for the matched cohort excluding patients with a survival time of less than 3 months, p = 0.080.
Relationship between different dialysis methods and survival of very elderly patients
Table 2 displays the relationship between the choice of dialysis methods and survival outcomes in elderly patients with ESKD. We conducted a multicollinearity assessment of the covariates and found that all covariates had a VIF of less than 5 (Table S3). The mortality rate in the PD group was 0.588 per patient-year, while the mortality rate in the HD group was 0.396 per patient-year. Compared to the PD group, the HR for the HD group was 0.73 (0.49, 1.10). After adjusting for confounding factors, the results remained consistent. Although the point estimate favored HD, the wide confidence interval suggests that the study may have been insufficiently powered to detect a clinically meaningful difference between the two modalities. Furthermore, we performed a sensitivity analysis by excluding patients with a survival period of less than 3 months and found no statistically significant differences in survival rates between the two dialysis methods (Table 3).
Subgroup analyses
We conducted subgroup analyses and interaction tests to evaluate the impact of dialysis modality on survival across different populations (Table 4). In subgroups stratified by heart failure, cerebrovascular disease, sex, and diabetes, we did not observe any significant interactions (p for interaction > 0.1). These findings suggest that PD and HD yield consistent survival outcomes across all examined subgroups, with no significant differences identified. However, some subgroups included relatively small numbers of patients, which may limit the statistical power. Therefore, these results should be interpreted with caution.
Discussion
In this multicenter cohort study, we conducted PSM on patients aged 75 years and older undergoing dialysis for ESKD. We performed multivariable Cox regression analysis on the matched cohort. Our findings indicated that there was no significant difference in the risk of mortality between elderly patients receiving HD and those receiving PD. Kaplan-Meier survival curve analysis indicated that there were no statistically significant differences in survival outcomes between the two dialysis modalities. Furthermore, no significant interactions were observed across various subgroups. To enhance the robustness of our results, we excluded patients with a survival duration of less than three months, and the findings remained stable. However, the confidence intervals in this study were relatively wide, possibly due to the sample size after matching. After adjustment for confounding factors, no statistically significant difference in survival was observed between HD and PD, and the results should be interpreted with caution.
The choice of dialysis strategies for elderly patients with ESKD remains a significant controversy within the current literature. A recent meta‑analysis by Cheng et al.13, which included more than 770,000 elderly dialysis patients, provided the most comprehensive pooled evidence to date comparing PD and HD in older populations. The study showed a modestly higher all‑cause mortality risk for PD (pooled HR = 1.17, 95% CI 1.10–1.25), particularly among patients with diabetes or multiple comorbidities. However, Cheng et al. emphasized substantial heterogeneity and recommended individualized treatment decisions. In our study focusing on very elderly patients aged ≥ 75 years, no significant survival difference between PD and HD was observed, suggesting that when patient selection and management are optimized, survival outcomes may become comparable in this age group. Research conducted by Yu-Kai Peng et al.20. found no substantial difference in all-cause mortality risk when comparing PD to HD among patients aged 65 and older. In contrast, studies by Seung Seok Han et al.11. indicated that older patients receiving PD have a significantly higher mortality risk compared to those on HD. Notably, previous research has often treated the older population as a homogeneous group, overlooking the unique physiological characteristics of the subgroup aged 75 and above. Our study specifically targets this older demographic, revealing that the survival rates between PD and HD do not show statistical significance, thus providing new evidence in this ongoing debate. It is essential to highlight that regional study findings exhibit considerable discrepancies. For instance, a study by Celine Foote et al.18. involving 1,781 patients aged 75 years and older in Australia and New Zealand reported a 26% increase in mortality risk for patients on PD. Similarly, research from France supports the notion that elderly patients on PD face higher mortality risks19. It is important to note that most previous studies were conducted in predominantly Caucasian populations, which may limit the generalizability of their findings to Asian patients21. Moreover, differences in body composition and dialysis practice patterns—such as the frequency of HDF—could partly explain the variability in reported outcomes between regions22,23,24. This study, conducted within the Chinese population, is the first systematic evaluation of survival differences between PD and HD in elderly ESKD patients (≥ 75 years) in a real-world medical setting. It provides evidence-based insights for the selection of dialysis modalities among older populations in Asia and addresses the potential confounding effects of healthcare policy differences on research findings.
The lack of a significant difference in survival between HD and PD among very elderly patients with ESKD may be attributed to the interaction of multiple underlying mechanisms. The continuous, slow ultrafiltration characteristic of PD significantly reduces the risk of hemodynamic fluctuations, which is particularly important for the cardiovascular fragile elderly population25. Although the intermittent nature of HD allows for efficient solute removal and control of volume overload, it can provoke hemodynamic instability events such as dialysis-induced hypotension26,27. While elderly patients on PD face a higher risk of peritonitis, studies indicate that their technical survival rates are not significantly different from those of younger patients28. Modern PD techniques, utilizing biocompatible dialysis solutions and nutritional interventions, have considerably improved nutritional indicators such as serum albumin, effectively narrowing the traditional survival gap compared to HD29. Crucially, PD is more conducive to preserving residual renal function (RRF), an advantage that can offset some of the benefits of HD’s solute clearance efficiency30,31. Furthermore, RRF has been established as an independent predictor of reduced mortality risk, serving as a key mediator for the convergence of survival outcomes between these two modalities32. In addition, the home-based treatment model of PD enhances the autonomy of elderly patients and reduces the burden associated with medical transportation33,34. This social and psychological benefit may indirectly contribute to the similarity in survival outcomes through improved treatment adherence.
The strengths of this study lie in its status as the first multicenter cohort study spanning 11 years to investigate the outcomes of HD versus PD in patients aged 75 and older with ESKD. By employing PSM, we minimized the impact of confounding factors. This research contributes to the existing literature by providing valuable insights for the selection of dialysis modalities in elderly ESKD patients.
Our study has several limitations. As it was a retrospective study, we were unable to adjust for all confounding factors, and selection bias was unavoidable. In particular, because of the advanced age of the participants, some potentially important factors such as frailty status, cognitive function, nutritional parameters, residual renal function, and social or family support were not captured, which might have influenced both the choice of dialysis modality and survival outcomes. In addition, although a sensitivity analysis excluding early deaths was conducted to minimize the potential for immortal time bias, this bias cannot be entirely ruled out. Furthermore, the multivariate Cox regression model did not incorporate several dialysis‑related and prognostic variables (BMI, blood pressure, ultrafiltration volume, dialysis adequacy [Kt/V], and markers of mineral and bone metabolism such as calcium, phosphate, and parathyroid hormone), which may have affected the precision of the estimated associations. Finally, the study population is exclusively drawn from the Northeast region of China, necessitating larger, multicenter prospective cohort studies to validate the generalizability of the findings.
Conclusion
Our study demonstrated no statistically significant difference in survival between PD and HD in very elderly patients with ESKD. Personalized dialysis decisions, based on patients’ clinical characteristics and preferences, are essential for optimizing care in this population. Future research should focus on prospective studies to enhance treatment strategies.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- eGFR:
-
Estimated glomerular filtration rate
- ESKD:
-
End-stage kidney disease
- HD:
-
Hemodialysis
- HDF:
-
Hemodiafiltration
- HR:
-
Hazard ratio
- PD:
-
Peritoneal dialysis
- PSM:
-
Propensity score matching
- SMDs:
-
Standardized mean differences
- USRDS:
-
United States renal data system
References
Nordheim, E. & Geir Jenssen, T. Chronic kidney disease in patients with diabetes mellitus. Endocr. Connections. 10, R151–R159. https://doi.org/10.1530/ec-21-0097 (2021).
Li, H. L., Tai, P. H., Hwang, Y. T., Lin, S. W. & Lan, L. C. Causes of hospitalization among End-Stage kidney disease cohort before and after Hemodialysis. Int. J. Environ. Res. Public Health. 19 https://doi.org/10.3390/ijerph191610253 (2022).
Gupta, R., Woo, K. & Yi, J. A. Epidemiology of end-stage kidney disease. Semin. Vasc. Surg. 34, 71–78. https://doi.org/10.1053/j.semvascsurg.2021.02.010 (2021).
United States Renal Data System. USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States (National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2024).
Brown, E. A. & Johansson, L. Epidemiology and management of end-stage renal disease in the elderly. Nat. Rev. Nephrol. 7, 591–598. https://doi.org/10.1038/nrneph.2011.113 (2011).
Isaacs, A., Burns, A. & Davenport, A. Is Dialysis a viable option for the older patient? Outcomes for patients starting Dialysis aged 80 years or older. Blood Purif. 33, 257–262. https://doi.org/10.1159/000337100 (2012).
Mikolasevic Ivana, I., Bubic, I., Sladoje-Martinovic, B., Racki, S. & Orlic, L. Survival of chronic Hemodialysis patients over 80 years of age. Clin. Interv. Aging. https://doi.org/10.2147/cia.S58976 (2014).
Byrne, C. & Cohen, V. P. Effect of age and diagnosis on survival of older patients beginning chronic Dialysis. JAMA 271, 34–36 (1994).
Canaud, B. et al. Clinical practices and outcomes in elderly Hemodialysis patients. Clin. J. Am. Soc. Nephrol. 6, 1651–1662. https://doi.org/10.2215/cjn.03530410 (2011).
Noppakun, K. et al. Survival rates in comprehensive Conservative care compared to Dialysis therapy in elderly end-stage kidney disease patients: a propensity score analysis. Ren. Fail. 46, 2396448. https://doi.org/10.1080/0886022X.2024.2396448 (2024).
Han, S. S. et al. Dialysis modality and mortality in the elderly: A Meta-Analysis. Clin. J. Am. Soc. Nephrol. 10, 983–993. https://doi.org/10.2215/CJN.05160514 (2015).
Chang, J. H. et al. Hemodialysis leads to better survival in patients with diabetes or high comorbidity, compared to peritoneal Dialysis. Tohoku J. Exp. Med. 229, 271–277. https://doi.org/10.1620/tjem.229.271 (2013).
Cheng, L., Hu, N., Song, D. & Chen, Y. Mortality of peritoneal Dialysis versus Hemodialysis in older adults: an updated systematic review and Meta-Analysis. Gerontology 70, 461–478. https://doi.org/10.1159/000536648 (2024).
Lukowsky, L. R. et al. Comparing mortality of peritoneal and Hemodialysis patients in the first 2 years of Dialysis therapy: a marginal structural model analysis. Clin. J. Am. Soc. Nephrol. 8, 619–628. https://doi.org/10.2215/CJN.04810512 (2013).
Wong, B. et al. Comparison of patient survival between Hemodialysis and peritoneal Dialysis among patients eligible for both modalities. Am. J. Kidney Dis. 71, 344–351. https://doi.org/10.1053/j.ajkd.2017.08.028 (2018).
Liem, Y. S., Wong, J. B., Hunink, M. G. M., de Charro, F. T. & Winkelmayer, W. C. Comparison of Hemodialysis and peritoneal Dialysis survival in the Netherlands. Kidney Int. 71, 153–158. https://doi.org/10.1038/sj.ki.5002014 (2007).
Yao, X. et al. Impact of initial Dialysis modality on the survival of patients with ESRD in Eastern china: a propensity-matched study. BMC Nephrol. 21, 310. https://doi.org/10.1186/s12882-020-01909-3 (2020).
Foote, C. et al. Survival of elderly Dialysis patients is predicted by both patient and practice characteristics. Nephrol. Dial Transpl. 27, 3581–3587. https://doi.org/10.1093/ndt/gfs096 (2012).
Couchoud, C. et al. Associations between comorbidities, treatment choice and outcome in the elderly with end-stage renal disease. Nephrol. Dial Transpl. 22, 3246–3254. https://doi.org/10.1093/ndt/gfm400 (2007).
Peng, Y. K. et al. Clinical outcomes between elderly ESKD patients under peritoneal Dialysis and hemodialysis: a National cohort study. Sci. Rep. 13, 16199. https://doi.org/10.1038/s41598-023-43476-1 (2023).
Obi, Y. et al. Impact of obesity on modality Longevity, residual kidney Function, Peritonitis, and survival among incident peritoneal Dialysis patients. Am. J. Kidney Dis. 71, 802–813. https://doi.org/10.1053/j.ajkd.2017.09.010 (2018).
Canaud, B., Köhler, K., Sichart, J. M. & Möller, S. Global prevalent use, trends and practices in haemodiafiltration. Nephrol. Dial Transpl. 35, 398–407. https://doi.org/10.1093/ndt/gfz005 (2020).
Tang, S. C. W. et al. Dialysis care and Dialysis funding in Asia. Am. J. Kidney Dis. 75, 772–781. https://doi.org/10.1053/j.ajkd.2019.08.005 (2020).
Kusirisin, P. & Srisawat, N. Hemodiafiltration in developing countries. Semin. Dial. 35, 449–456. https://doi.org/10.1111/sdi.13077 (2022).
Sarnak, M. et al. (ed, J.) Cardiovascular effects of home Dialysis therapies: A scientific statement from the American heart association. Circulation 146 https://doi.org/10.1161/cir.0000000000001088 (2022).
Canaud, B., Chazot, C., Koomans, J. & Collins, A. Fluid and hemodynamic management in Hemodialysis patients: challenges and opportunities. Brazilian J. Nephrol. 41, 550–559. https://doi.org/10.1590/2175-8239-jbn-2019-0135 (2019).
Satish, A. et al. Dialysis in the elderly: A practical guide for the clinician. Int. J. Nephrol. 2025 (9538115). https://doi.org/10.1155/ijne/9538115 (2025).
Çankaya, E. & Altunok, M. Comparison of young and old patients on peritoneal dialysis: A retrospective observational study. Semin. Dial. 37, 153–160. https://doi.org/10.1111/sdi.13180 (2023).
Hao, N. et al. Time-varying serum albumin levels and all-cause mortality in prevalent peritoneal Dialysis patients: a 5-year observational study. BMC Nephrol. 20 https://doi.org/10.1186/s12882-019-1433-8 (2019).
Liu, X. & Dai, C. Advances in Understanding and management of residual renal function in patients with chronic kidney disease. Kidney Dis. (Basel). 2, 187–196. https://doi.org/10.1159/000449029 (2017).
Hu, Y. H., Liu, Y. L., Meng, L. F., Zhang, Y. X. & Cui, W. P. Selection of Dialysis methods for end-stage kidney disease patients with diabetes. World J. Diabetes. 15, 1862–1873. https://doi.org/10.4239/wjd.v15.i9.1862 (2024).
Liao, C. T. et al. Rate of decline of residual renal function is associated with all-cause mortality and technique failure in patients on long-term peritoneal Dialysis. Nephrol. Dialysis Transplantation. 24, 2909–2914. https://doi.org/10.1093/ndt/gfp056 (2009).
Chuasuwan, A., Pooripussarakul, S., Thakkinstian, A., Ingsathit, A. & Pattanaprateep, O. Comparisons of quality of life between patients underwent peritoneal Dialysis and hemodialysis: a systematic review and meta-analysis. Health Qual. Life Outcomes. 18 https://doi.org/10.1186/s12955-020-01449-2 (2020).
Wong, B. et al. Selection of peritoneal dialysis among older eligible patients with end-stage renal disease. Nephrol. Dial Transpl. 32, 384–392. https://doi.org/10.1093/ndt/gfw367 (2017).
Funding
This study received support from the Jilin Province Medical and Health Talent Special Project (No. 2024WSZX-B01).
Author information
Authors and Affiliations
Contributions
Yaohua Hu: Writing – original draft, Software; Xueyan Zhu: Resources; Yingying Liu: Resources; Liming Yang: Resources; Zhanshan Sun: Resources; Xiaoxuan Zhang: Resources; Jian Li: Writing – review & editing; Xinyang Li: Writing – review & editing.Xinyu Gao: Writing – review & editing; Mengyuan Yu: Supervision; Wenpeng Cui: Writing – review & editing, Methodology.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
In this study, the Ethics Committee of the Second Hospital of Jilin University Hospital approved the study (No.2024317). This study is a retrospective investigation that does not involve the collection or use of patients’ private information. It has been reviewed and approved by the Ethics Committee (No. 2024317), and the requirement for informed consent has been waived. The research strictly adheres to ethical guidelines, ensuring full compliance with relevant laws and regulations. Our study complied with the Declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hu, Y., Zhu, X., Liu, Y. et al. Choosing dialysis modality in patients aged 75 and above with end-stage kidney disease: a multicenter cohort study. Sci Rep 16, 2174 (2026). https://doi.org/10.1038/s41598-025-31857-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-31857-7
