
Abstract
Adolescent pregnancy is associated with elevated stress, anxiety, and depression, often exacerbated by limited social support. Despite the recognized risks faced by pregnant adolescents, there is a paucity of research evaluating the effectiveness of psychoeducational interventions specifically integrated into antenatal care for this population. Midwife-led care is widely recognized for its holistic and personalized approach, which is particularly valuable for adolescent mothers. Psychoeducational interventions, enhancements have shown promise in reducing psychological distress and improving well-being among pregnant adolescents. However, evidence remains limited, with few randomized controlled trials evaluating the impact of these interventions when delivered as part of routine childbirth preparation classes. This study aimed to assess the effect of a midwife-led psychoeducational life skills intervention, incorporated into routine childbirth preparation classes, on pregnancy-related anxiety, stress, depression, and perceived social support in pregnant adolescents. This randomized controlled trial involved 90 pregnant adolescents recruited from health centers, with 45 participants assigned to the intervention group and 45 to the control group. The intervention group received ten structured psychoeducational sessions focusing on life skills, delivered by a trained instructor alongside standard childbirth preparation classes. The control group received only routine prenatal education. The control group received routine care only. Outcome assessors were blinded to group allocation. Primary outcomes were pregnancy-related anxiety, perceived stress, and depression; the secondary outcome was perceived social support. Data were collected using validated self-report measures at three time points: baseline (pre-intervention), immediately post-intervention, and one month after the intervention. Statistical analyses were performed using SPSS version 22, including repeated-measures analysis of variance (ANOVA), independent t-tests, and chi-square tests. Ethical approval: IR.AJUMS.REC.1402.140. Trial registration: IRCT20190129042544N1 (26 June 2023). Compared with controls, the intervention group demonstrated significant reductions in anxiety (η² = 0.32, p < 0.001), perceived stress (η² = 0.29, p < 0.001), and depression (η² = 0.31, p < 0.001). Perceived social support increased within both groups, but between-group differences were not significant (p = 0.238). The group × time interaction was statistically significant for anxiety, stress, and depression, compared with the control group, and this effect was maintained at both the 1-month and 3-month follow-up assessments, indicating the sustained efficacy of the midwife-led psychoeducational life skills program. The integration of a psychoeducational life skills program into routine midwife-led antenatal education proved effective in improving the psychological well-being of pregnant adolescents, as evidenced by significant reductions in anxiety, stress, and depression. These findings support the inclusion of structured psychoeducational interventions in adolescent maternity care services to promote mental health during pregnancy. While both the intervention and control groups experienced increased perceived social support, the lack of a significant between-group difference suggests that additional or alternative strategies may be needed to further enhance social support outcomes in this population.
Trial registration: The study protocol was prospectively registered in the Iranian Registry for Randomized Controlled Trials on 26 June 2023 (registration number: IRCT20190129042544N1), and participant recruitment began on October 1, 2024.
Similar content being viewed by others

Introduction
Adolescent pregnancy, defined as pregnancy occurring between the ages of 10 and 191, presents significant health and social challenges worldwide2. Each year, approximately 15 million adolescents give birth, accounting for about 11% of all births globally1, This period is marked by rapid transitions to adulthood, motherhood, and often, marriage, which can be precipitated by unexpected pregnancy. The abrupt assumption of maternal identity during adolescence a critical developmental phase characterized by psychological, biological, and social changes can trigger psychological crises and heighten vulnerability to mood disorders3 Adolescent mothers report higher levels of depression, anxiety, and stress compared to older mothers3,4. Field et al. (2020) highlight the unique challenges faced by pregnant adolescents, including perinatal stress, low self-esteem, financial difficulties, inadequate social support, and societal stigma5.
Depression affects 4–8% of adolescents but rises to 16–44% during pregnancy, nearly double the prevalence among adult pregnant women and non-pregnant peers6. Psychological distress during pregnancy, including prenatal anxiety and stress, has been linked to adverse maternal and neonatal outcomes such as preterm birth, low birth weight, and infant developmental disorders7,8,9.
Anxiety affects approximately 15% of pregnant women in Iran, with prevalence increasing from 15.6% in early pregnancy to 20.6% in late pregnancy10,11,12. Pregnancy-related anxiety elevates stress hormones, impairs fetal brain development13, reduces uterine-placental blood flow, and increases the risk of fetal asphyxia, labor complications, postpartum mood disorders, and autoimmune issues13,14,15,16.
Several studies emphasize that inadequate psychosocial preparation for motherhood and poor social support significantly increase adolescents’ risk of stress and depression17,18. , Although midwives play a central role in providing comprehensive care during pregnancy, only a minority deliver high-quality psychosocial support19. Strengthening midwives’ clinical and emotional care competencies is thus essential to reducing maternal vulnerability and promoting mental health20,21. Midwife-led antenatal care offers a unique opportunity to address the psychosocial needs of adolescent mothers. Unlike traditional biomedical models, midwife-led care emphasizes holistic, continuous, and relationship-based support, which can foster trust and emotional well-being. Integrating psychoeducational interventions into this model can enhance adolescents’ coping mechanisms, strengthen emotional regulation, and promote adaptive responses to pregnancy-related stress. Community-based support resources are vital protective factors for fostering psychosocial resilience in adolescent mothers. The reciprocal relationship between support systems and positive maternal experiences is well-documented22. Comprehensive care that integrates medical, educational, and psychosocial components has been shown to improve maternal and child health outcomes. 23.
Given the limitations of medication use during pregnancy, researchers have increasingly focused on non-pharmacological interventions, such as education, cognitive-behavioral counseling, relaxation techniques, yoga, and massage. These low-cost, non-invasive alternatives offer fewer side effects and are widely accessible24,25,26. Life skills are defined as adaptive, positive behaviors that enable individuals to cope effectively with life’s demands27. These skills encompass psychological, social, and interpersonal abilities that enhance self-awareness, confidence, decision-making, stress reduction, communication, and problem-solving24,28.
Today, life skills are recognized as both a strategy for promoting mental health and a tool for preventing psychosocial harm, empowering youth and adolescents in their psychosocial and health development29. Despite strong evidence supporting life skills training as a mental health promotion strategy, research on its application among pregnant adolescents remains limited. In Iran, life skills education is not formally integrated into school or prenatal care curricula24. The World Health Organization and other international bodies advocate for life skills education as a means to equip future citizens with the tools to navigate complex social environments29.
While standard childbirth preparation classes are available in Iran, they are typically designed for adult women and may not address the distinct developmental and psychosocial needs of adolescents30,31. Psychosocial interventions that include life skills training have shown small to moderate positive effects on the mental health of pregnant adolescents and teen parents, though the evidence is of very low quality. There is an urgent need to design and test new psychosocial interventions for pregnant adolescents, particularly in low-income settings and for diverse demographic groups32. Existing studies have predominantly focused on adult or school-based populations, leaving critical gaps in understanding the applicability of psychoeducational interventions for pregnant adolescents. Moreover, cultural and developmental factors may influence intervention uptake and effectiveness, underscoring the need for contextually tailored models of care. Therefore, the present study aimed to evaluate the effectiveness of a midwife-led psychoeducational life skills program integrated into routine antenatal care on pregnancy-related stress, anxiety, depression, and perceived social support among pregnant adolescents.
Specifically, the study tested the following hypotheses:
-
1.
Adolescents receiving the psychoeducational life skills intervention will demonstrate significantly lower levels of pregnancy-related anxiety, perceived stress, and depression than those receiving routine care.
-
2.
The intervention will lead to higher levels of perceived social support compared to standard antenatal education.
Methods
Trial design
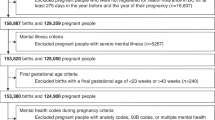
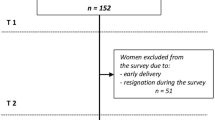
This study was a two-arm, parallel-group randomized controlled trial conducted from 2024 to 2025 to assess the effectiveness of a midwife-led psychoeducational life skills intervention on psychological outcomes in pregnant adolescents. The trial was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines. The completed CONSORT checklist is available as Supplementary File 1. Figure 1 presents the CONSORT flowchart of participant recruitment and retention.
This study received ethical approval from the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (approval code: IR.AJUMS.REC.1402.140). Additionally, the study protocol was prospectively registered in the Iranian Registry for Randomized Controlled Trials on 26 June 2023 (registration number: IRCT20190129042544N1), and participant recruitment began on October 1, 2024.
Result
Demographic characteristics

CONSORT flowchart of the study.
Participants
The study enrolled 90 pregnant adolescents aged 13–19 years who were referred to health centers affiliated with Ahvaz Jundishapur University of Medical Sciences in Ahvaz, Iran.
Inclusion Criteria:
-
Age between 13 and 19 years.
-
Gestational age between 11 and 15 weeks.
-
Low-risk singleton pregnancy.
-
Ability to read and speak Persian.
-
Willingness to participate and provide informed consent.
Exclusion Criteria:
-
High-risk pregnancy or detected fetal abnormalities.
-
History of major stressful events in the past three months.
-
Existing physical or mental illness.
-
Use of tobacco or alcohol.
Participants were recruited using a convenience sampling method following medical file screening, with eligibility confirmed via telephone or in-person consultation.
Setting
The study was conducted in two comprehensive health centers and their affiliated health bases in East and West Ahvaz, Iran. These facilities provide standard antenatal services and childbirth preparation classes under the supervision of the local university medical system.
Interventions
Intervention group
Participants in the intervention group received 10 structured psychoeducational sessions, each lasting 105 min, delivered in small groups of 5–7 participants by trained midwives. Two sessions were held before the 20th week of pregnancy, and the remaining eight sessions were aligned with the national routine prenatal care protocol, with an additional 15 min dedicated to reviewing and reinforcing a core life skill. This approach allowed participants to begin developing coping strategies earlier in pregnancy.
Each session integrated standard prenatal education per Iranian Ministry of Health guidelines with a core World Health Organization (WHO)-recommended life skill. Topics included stress management, emotional regulation, effective communication, problem-solving, and interpersonal relationship building. Applied exercises and group practice were used to reinforce these skills and enhance psychosocial competencies.
Session content includes
Session | Gestational age | Contents Life Skills Training Package, Based on Improving Perceived Psychosocial Support for Pregnant Adolescents, Specifically for Childbirth Class Instructors |
|---|---|---|
1 | 15–18 weeks | Group introduction and overview of the program: Establishing rapport and introducing participants. Basic emotional and interpersonal skills (self-awareness and communication): Understanding oneself and one’s abilities; developing emotional self-awareness as the foundation of all skills; recognizing and expressing emotions appropriately. Empathy: Understanding others’ emotions and preparing for social interaction. Effective communication: Learning how to express thoughts and feelings clearly and manage interpersonal conflict. Emotional regulation: Recognizing and controlling emotions as a prerequisite for more complex skills. These foundational skills are interrelated and strengthen adolescents’ emotional and social readiness |
2 | 18–20 weeks | Cognitive skills and coping strategies: Stress management: Using emotional skills to manage real-life stress. Problem-solving: Learning logical analysis and generating practical solutions for daily issues. Decision-making: Making informed decisions through evaluation of options and consequences. Critical and creative thinking: Applying previous skills to analyze, reason, and innovate. These advanced cognitive skills build upon the emotional foundation established in Session 1. |
3 | 20–22 weeks | Enhancing self-awareness and personal strengths: Participants explored their emotions, abilities, and personal needs through guided exercises. The aim was to strengthen emotional insight and self-knowledge as the basis for subsequent skills. |
4 | 23–25 weeks | Developing empathy: Participants learned to recognize and understand others’ feelings and needs through group discussions and exercises designed to improve social sensitivity and cooperation. |
5 | 26–28 weeks | Improving communication skills: This session focused on the principles of effective verbal and non-verbal communication, expressing thoughts and emotions appropriately, and developing constructive strategies for resolving conflicts. |
6 | 29–31 weeks | Emotional regulation and anger management: Group activities helped participants identify emotional triggers (especially anger) and practice relaxation and self-control techniques to reduce negative emotional reactions and enhance constructive responses in stressful situations. |
7 | 32–33 weeks | Stress management reinforcement: Participants were introduced to various coping techniques, relaxation exercises, and emotional regulation strategies aimed at managing psychological stress during pregnancy. |
8 | 34–35 weeks | Problem-solving skills: Training focused on identifying problems, evaluating alternative solutions, and selecting logical and practical strategies to address everyday challenges. |
9 | 36–37 weeks | Decision-making skills: Participants practiced making responsible and informed decisions by evaluating possible options and anticipating outcomes in different life situations. |
10 | 37–38 weeks | Critical and creative thinking: This final session focused on developing analytical thinking and generating creative solutions. Individual and group exercises were used to foster reasoning, innovation, and advanced problem-solving abilities. |
Instructional Methods:
-
Group discussions.
-
Role-playing.
-
Storytelling.
-
Guided question-and-answer.
-
Relaxation techniques.
-
Distribution of educational booklets and printed materials.
Midwives facilitating the sessions completed three structured training workshops led by the principal investigator, a Ph.D. candidate in midwifery with a master’s in counseling and certification in life skills education. The training covered psychosocial support, adolescent developmental psychology, and mental health in pregnancy. All workshops were supervised by a Ph.D.-level expert in counseling to ensure academic and clinical quality and fidelity to the intervention framework.
Control Group:
Participants in the control group attended standard prenatal education classes according to Iranian Ministry of Health guidelines. These included eight sessions (90 min each) between 20 and 37 weeks of gestation. Each session comprised:
-
30 min of theoretical education on pregnancy and childbirth.
-
45 min of physical activity (e.g., stretching, breathing, massage).
-
15 min of Q&A.
The sessions cover the following core topics:
-
1.
Physiological and emotional changes during pregnancy.
-
2.
Maternal nutrition, hygiene, and safe physical activity.
-
3.
Fetal growth and warning signs.
-
4.
Breathing, relaxation, and non-pharmacological pain relief techniques.
-
5.
Role of the spouse and family support.
-
6.
Stages of labor and delivery.
-
7.
Postpartum care, breastfeeding, and newborn care.
-
8.
Final review and simulation of labor process.
These classes are considered a routine component of standard prenatal care in Iran, accessible to all pregnant women free of charge in public health centers.
Instructional materials included audiovisual aids, anatomical models, posters, and whiteboard demonstrations33.
Outcomes
Primary outcomes included changes in stress, anxiety, depression, and perceived social support, assessed using validated Persian versions of the following instruments:
-
Vaux Social Support Appraisal Scale (Cronbach’s α = 0.80)34.
-
Perceived Stress Scale (PSS-14) (Cronbach’s α = 0.84)35.
-
Edinburgh Postnatal Depression Scale (EPDS) (Cronbach’s α = 0.82)36.
-
Pregnancy-Related Anxiety Questionnaire (PRAQ) (Cronbach’s α = 0.70)37.
Questionnaires were administered at three time points: baseline (pre-intervention), immediately post-intervention, and four weeks after the final session. Demographic and obstetric history data were also collected.
Information collection
To assess psychological outcomes, the study utilized validated, self-administered Persian versions of standardized questionnaires. Each instrument was selected based on established reliability and validity within Iranian populations:
Pregnancy Anxiety Questionnaire (Van den berg, 1989):17-item scale measuring anxiety specific to pregnancy, with each item rated on a 7-point Likert scale. Total scores range from 17 to 119, with higher scores indicating greater anxiety. The Persian version was validated by Karamozyan et al. (2016), demonstrating content, face, and criterion validity. Internal consistency was acceptable, with a Cronbach’s alpha exceeding 0.7037.
Vaux Social Support Appraisal Scale (Wax et al., 1986): 23-item instrument evaluating perceived social support across three domains: family, friends, and significant others. Domain scores range from 0 to 23, with higher scores reflecting stronger perceived support. The Persian adaptation was validated by Rafi et al., who reported significant domain-specific correlations: friends (0.76), family (0.55), and significant others (0.74), all at p < 0.0001, confirming construct validity34.
Perceived Stress Scale (PSS-14): 14-item scale assessing perceived stress over the past month, with total scores ranging from 0 to 56. Higher scores indicate greater stress. Construct validity was supported by a correlation coefficient of 0.63 (p < 0.05)38. The Persian version demonstrated strong psychometric properties: Cronbach’s alpha of 0.84 in Asghari et al.’s study35., and content validity indices of 95% and 90% as reported by Dolatian et al. (2014)39.Original reliability values ranged from 0.84 to 0.86, with correlations between 0.52 and 0.76, unaffected by age or gender40. Bastani et al. reported a Cronbach’s alpha of 0.74 for the Persian version41,42.
Edinburgh Postnatal Depression Scale (EPDS) – Cox, 1987: 10-item scale measuring perinatal depression symptoms. Scores range from 0 to 30, with a cut-off of ≥ 12 indicating possible depression. Items 1, 2, and 4 are scored from 0 to 3; the remaining items are reverse scored (3 to 0). The Persian version demonstrated acceptable internal consistency, with a Cronbach’s alpha coefficient of 0.7043.
Sample size
Sample size was determined based on previous research on depression prevention programs for pregnant adolescents (“Effectiveness of an Early Depression Prevention Program on Coping Skills and Depression among Pregnant Adolescents: A Randomized Controlled Trial”)44 Using MedCalc software, with 90% power, 5% significance (α = 0.05), and the following parameters:
\(\begin{gathered} {\text{z}}\_({\text{1}} - {\text{a}}/{\text{2}})={\text{1}}.{\text{96}} \hfill \\ {\text{z}}\_({\text{1}} - {\text{b}})={\text{1}}.{\text{645}} \hfill \\ {\text{SD}}\_{\text{1}}={\text{9}}.{\text{14}} \hfill \\ {\text{SD}}\_{\text{2}}={\text{15}}.{\text{83}} \hfill \\ {\text{m}}\_{\text{1}}={\text{73}}.{\text{47}} \hfill \\ {\text{m}}\_{\text{2}}={\text{64}}.{\text{39}} \hfill \\ \end{gathered}\)
The formula used was:
The minimum required sample size was 76 participants (38 per group). To account for a 20% attrition rate, the final sample included 90 participants (45 per group).
Participant enrollment and intervention
Recruitment and consent
Following ethical approval and administrative authorization, eligible pregnant adolescents were recruited according to predefined inclusion criteria. Informed written consent was obtained from all participants prior to enrollment. Each participant received detailed information regarding the study’s purpose, procedures, and confidentiality measures, in accordance with ethical standards.
Sampling and randomization
Participants were enrolled by the principal investigator, who verified eligibility based on inclusion and exclusion criteria. Participants were recruited through convenience sampling from selected health centers affiliated with Ahvaz Jundishapur University of Medical Sciences. A total of 90 adolescents who met the eligibility requirements were included in the trial.
Randomization procedure
Group allocation was conducted using block randomization (block size = 6) to ensure balanced assignment to the intervention and control groups. The random allocation sequence was generated by an independent statistician using computer-based block randomization.
Group allocation
During enrollment, Group assignments were placed in sealed opaque envelopes and opened sequentially by a trained midwife not involved in data collection. This procedure preserved the integrity of the randomization process and ensured unbiased allocation.
Blinding
Blinding of participants and midwives was not feasible due to the nature of the intervention. However, Outcome assessors and data analysts were blinded to group allocation to minimize detection bias.
Data collection and management
Questionnaires were administered by the researcher at all three time points: baseline (pre-intervention), immediately post-intervention, and four weeks after the final session. Completed questionnaires were assigned unique codes and securely stored to ensure confidentiality. Data entry was performed by a research assistant who was blinded to group assignment, thereby minimizing the risk of bias.
Statistical methods
Data were analyzed using IBM SPSS Statistics version 22. Descriptive statistics were used to summarize baseline demographic and clinical characteristics. Chi-square tests were employed to assess group homogeneity for categorical variables, while independent t-tests were used for continuous variables. Repeated measures analysis of variance (ANOVA) was conducted to evaluate changes in psychological outcomes across the three assessment time points. Statistical significance was set at p < 0.05.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (approval code: IR.AJUMS.REC.1402.140). Written informed consent was obtained from all participants prior to enrollment. To ensure ethical treatment, control group participants received a summary booklet of the intervention content upon study completion. Additional individual counseling was made available upon request.
Results
Table 1 presents the demographic characteristics of the participants. No significant differences were observed between the intervention and control groups regarding qualitative or quantitative demographic variables. Chi-square and independent t-tests confirmed homogeneity across groups (all p-values > 0.05).
The majority of participants (over 96%) were homemakers. Approximately 85% reported that their pregnancy was planned, and about 70% rated their economic status as good or very good. Only 2% of participants had attained university-level education. The mean age was 16.73 ± 1.67 years in the control group and 16.69 ± 1.73 years in the intervention group (see Table 1).
Of the 90 adolescent participants initially recruited, all completed the intervention and follow-up periods. No attrition occurred in either the intervention or control group. Statistical analysis confirmed that the groups were homogeneous at baseline with respect to demographic and clinical characteristics (all p > 0.05).
Pregnancy-related anxiety
Repeated measures analysis of variance (ANOVA) revealed a significant time × group interaction for pregnancy-related anxiety (P < 0.001). Over the course of the study, the intervention group demonstrated a significant reduction in anxiety scores (P < 0.001), whereas the control group experienced a significant increase (P < 0.001). Independent t-tests confirmed significant between-group differences at all three assessment points: before the intervention (P = 0.002), immediately after the intervention (P < 0.001), and one month post-intervention (P < 0.001). These results indicate a robust and sustained effect of the psychoeducational intervention in reducing pregnancy-related anxiety among adolescent participants. (See Table 2).

The mean scores of Pregnancy-Related Anxiety (Vandenberg Scale, 17–119) in the intervention and control groups across the three measurement times (1 Before the intervention, 2 Immediately after completing the intervention, 3 a month after completing the intervention).
Perceived stress
A significant interaction effect was observed for perceived stress scores (P < 0.001). Stress levels decreased significantly within the intervention group (P < 0.001), but increased in the control group over time (P < 0.001). Between-group differences were statistically significant at both the post-intervention and one-month follow-up assessments (P < 0.001). This pattern underscores the effectiveness of the psychoeducational sessions in stress management and highlights the intervention’s capacity to mitigate stress among pregnant adolescents. (See Table 2).

The mean scores of Perceived Stress Score (PSS-14, 0–56) in the intervention and control groups across the three measurement times (1 Before the intervention, 2 Immediately after completing the intervention, 3 a month after completing the intervention).
Depression
Depression scores exhibited a significant time × group interaction (P < 0.001). The intervention group showed a significant reduction in depressive symptoms over time (P = 0.001), while the control group displayed a significant increase (P < 0.001). Between-group differences were significant at both post-intervention time points (P < 0.001), demonstrating that the intervention had both preventive and therapeutic effects on depression. (See Table 2).

The mean scores of Pregnancy depression (EPDS; 0–30) in the intervention and control groups across the three measurement times (1 Before the intervention, 2 Immediately after completing the intervention, 3 a month after completing the intervention).
Perceived social support
A significant within-group increase in perceived social support was observed for both the intervention and control groups (P < 0.001). However, the time × group interaction was not statistically significant (P = 0.238), and no significant between-group differences were found at any time point (P > 0.05). Although the intervention group consistently reported slightly higher mean scores, this suggests that the psychoeducational program had an additive, but not decisive, effect on social support. This outcome may reflect the influence of external support sources, such as family and peers, which are particularly salient for adolescents. (See Table 2).

The mean scores of perceived social support (SSA: 23–92) in the intervention and control groups across the three measurement times (1 Before the intervention, 2 Immediately after completing the intervention, 3 a month after completing the intervention).
As shown in Figs. 2, 3 and 4, and 5, mean scores of perceived social support in the intervention group increased over time, while mean scores of perceived stress, anxiety, and depression decreased over time. The results demonstrate large effects for anxiety (d = 1.14, η²=0.25), stress (d = 2.71, η²=0.45), and depression (d = 1.33, η²=0.30), and a small effect for social support (d = 0.32, η²=0.02), indicating substantial clinical significance of the intervention beyond statistical significance.(Table 3) Overall, the findings highlight the intervention’s significant role in improving mental health outcomes, specifically, reducing pregnancy-related anxiety, stress, and depression among pregnant adolescents. The results support the potential scalability of psychoeducational life skills programs within adolescent antenatal care settings.
Discussion
In this randomized controlled trial, we explored whether embedding a psychoeducational life skills module into routine midwife-led childbirth preparation classes could reduce psychological distress and improve social support among pregnant adolescents. The findings demonstrated statistically and clinically significant reductions in anxiety, stress, and depressive symptoms within the intervention group. Although perceived social support improved over time in both groups, the lack of significant between-group differences suggests that routine antenatal classes may already provide some degree of psychosocial benefit. These results have important implications for adolescent-focused prenatal care. Adolescents are particularly vulnerable to psychological distress during pregnancy due to their ongoing cognitive, emotional, and social development, compounded by stigma, social isolation, and limited access to mental health resources32,45,46.
The present study adds to a growing body of evidence demonstrating that structured psychoeducational interventions, particularly those that emphasize life skills such as emotional regulation, stress management, communication, and problem-solving, can serve as protective factors against the mental health challenges of pregnancy46,47,48.
A key finding was the significant reduction in pregnancy-related anxiety in the intervention group, contrasted by an increase in the control group. This supports existing literature indicating that psychoeducation equips adolescents with coping strategies, enhances their sense of control, and mitigates fear of childbirth46,48. Similar anxiety reductions have been reported across varied cultural settings, suggesting that such interventions are broadly applicable48,49, For example, McMullen and McMullen (2018) found that 24 sessions of teacher-led life skills training significantly reduced anxiety and depression in adolescents over a year50. while Mohammadi and Poursaberi (2018) observed similar outcomes among Iranian adolescent cancer patients following 13 sessions of psychologist-led training51.
Our findings on perceived stress also align with existing evidence showing that adolescent mothers often experience elevated stress levels, which can contribute to adverse outcomes like preterm birth and low birth weight32,45 The life skills intervention likely acted as a protective factor by fostering emotional resilience and promoting adaptive coping mechanisms, mirroring the impact of cognitive-behavioral and skills-based programs in pregnant populations47,48. Roy et al. (2016), for example, demonstrated significant stress reduction in adolescent boys following a brief, seven-day intervention52. These outcomes are particularly relevant given the public health priority of reducing stress-related perinatal complications.
Depressive symptoms significantly declined in the intervention group while increasing in the control group, reinforcing the value of timely psychosocial interventions during pregnancy. Given the limitations of pharmacologic treatments due to safety concerns, psychoeducational strategies offer a safe, scalable, and effective alternative for adolescents47,53. Moreover, the group-based format may have reduced feelings of isolation and fostered peer connection, both of which are critical in addressing adolescent perinatal depression46,47,53.
Marjan Mohammadzadeh and colleagues found a decrease in depression scores in their intervention group54. In contrast, Islami et al. (2016) conducted their study among high school students aged 15–18, reported no significant reduction in depression despite reduced anxiety and stress from life skills training. However, the current study identified a significant decrease in depressive symptoms among pregnant adolescents, likely due to the specific needs and challenges faced by this population. This discrepancy may be attributed to differences in the target population, the psychological vulnerability associated with adolescent pregnancy, or the structure and delivery of the intervention in the current study. These findings suggest that life skills training may be particularly effective in addressing depression when tailored to the unique needs and contextual challenges of pregnant adolescents55. Discrepancies between our findings and studies reporting limited effects particularly in children or non-pregnant adolescents may be attributed to key differences. Pregnancy entails profound biological, emotional, and social shifts that may both increase vulnerability and enhance responsiveness to psychosocial support. Additionally, developmental maturity, gender-related coping styles, and the sociocultural context of intervention delivery can significantly influence outcomes. Unlike school-based programs, our intervention was embedded in a culturally specific prenatal care environment, where adolescents may be more motivated to adopt behavioral changes. These considerations underscore the importance of tailoring interventions to the developmental stage, gender, and cultural context of the target population56.
The observed increase in perceived social support in both the intervention and control groups is likely attributable to the social dynamics naturally created within standard antenatal preparation classes. These sessions, led by midwives, often promote interaction, shared experiences, and a supportive environment among pregnant women, which can enhance social connectedness and empathy even without additional psychoeducational components.
Regarding social support, although both groups demonstrated significant within-group improvements, the absence of a significant between-group difference may reflect the characteristics of the measurement tool used. The Social Support Appraisals Scale (SSA; Vaux et al., 1986) primarily measures general perceived social support, which tends to remain relatively stable over short periods and may be less sensitive to detecting subtle, intervention-specific changes. Furthermore, participants in both groups attended routine prenatal classes and interacted with midwives and peers, experiences that likely fostered mutual understanding and social connection regardless of intervention exposure. While the SSA demonstrated high internal consistency in this study (Cronbach’s α = 0.89), its limited responsiveness to short-term psychosocial changes should be acknowledged. Future studies may benefit from employing multidimensional or context-specific measures to better capture dynamic aspects of perceived social support during pregnancy. It is also important to acknowledge that the Vaux Social Support Appraisal Scale (SSA), while psychometrically sound, may have limited sensitivity for detecting short-term or intervention-specific changes in perceived support among adolescents. The SSA primarily captures global appraisals of support, which tend to remain relatively stable over time and may not fully reflect dynamic, functional, or context-dependent aspects of social support during pregnancy. Given that adolescents’ support networks are strongly shaped by family structures, peer interactions, and sociocultural norms, future research would benefit from employing more multidimensional or domain-specific instruments—such as the Multidimensional Scale of Perceived Social Support (MSPSS) or the Social Support Behaviors Scale—to better differentiate emotional, instrumental, and informational support. Utilizing such measures, potentially combined with longer postpartum follow-up, may enhance the detection of subtle changes influenced by psychoeducational interventions.
Previous literature on social support interventions emphasizes that peer interaction, particularly in group-based antenatal settings, can help normalize the pregnancy experience, reduce feelings of isolation, and foster a sense of belonging and mutual understanding among expectant mothers57,58,59.
The sociocultural context in which this study was conducted played a major role in shaping both engagement and outcomes. In Iran’s southern provinces, family-centered living arrangements, collectivist cultural norms, and religious beliefs emphasize social cohesion and shared caregiving responsibilities. Such cultural features likely facilitated adolescents’ acceptance of the intervention, as group-based and discussion-oriented sessions harmonized with community traditions of mutual learning and collective coping31,60 Furthermore, midwives occupy a respected position in Iranian society as trusted health educators and moral authorities, which likely enhanced participants’ comfort and trust in the intervention process. This finding is consistent with earlier research highlighting that culturally congruent care provided by midwives promotes better communication, compliance, and emotional safety among young mothers20,61.
However, the same sociocultural strengths may also explain the absence of significant between-group differences in perceived social support. In collectivist communities, adolescents often benefit from strong extended-family networks and neighborhood-based support systems, which may buffer psychological distress independent of formal interventions17,62.
In this context, the findings of the present study suggest that while routine prenatal care provides a valuable foundation of social support, the midwife-led psychoeducational life skills program offers added value by strengthening internal coping resources such as emotional regulation, problem-solving, and stress management, thereby producing greater improvements in overall psychological well-being. The improvement in perceived social support observed in both groups may reflect the inherently supportive nature of standard prenatal care. In the Iranian antenatal system, midwife-led childbirth classes often provide a semi-structured group environment that fosters communication, empathy, and shared experiences among expectant mothers63,64,65. These interactions, along with the emotional attention given by midwives, may themselves act as a form of psychosocial intervention, enhancing perceived support and reducing isolation. This interpretation aligns with previous studies demonstrating that routine group-based care can promote social connectedness and normalize the experiences of pregnancy60,66. Nonetheless, the life skills program appears to offer additional benefits in helping adolescents manage internal psychological states, particularly anxiety and stress, by strengthening emotional regulation and coping capacities beyond what standard care alone provides.
Nevertheless, the within-group improvements in the intervention arm indicate that life skills training may enhance adolescents’ ability to identify, seek out, and engage with support networks. These findings are consistent with prior research showing that childbirth preparation programs can improve social connectedness, resilience, and emotional well-being67. Peer support, in particular, has been shown to reduce distress through shared experiences, emotional validation, and practical assistance68,69. Likewise, a narrative review on social support interventions emphasized the importance of peer support in normalizing experiences, providing coping strategies, and fostering a sense of community among participants46. It is also important to note that adolescents often draw support from informal sources such as family, partners, or community networks—factors not assessed in this study. For instance, research in Turkey highlighted the central role of family in supporting pregnant adolescents, with perceived support influenced by cultural attitudes toward early pregnancy62. In traditional or religious societies where early childbearing is socially accepted, adolescents may benefit from robust familial and community-based support systems3.
Even in the absence of a statistically significant between-group difference, the intervention group’s gains suggest that life skills education may strengthen adolescents’ social awareness and relational competencies. Previous studies have shown that such programs enhance interpersonal and emotional skills, enabling adolescents to build meaningful relationships, seek help effectively, and improve their self-concept70,71 For example, Akbarzadeh et al. (2020) found that antenatal education emphasizing emotional and communication skills improved maternal mental health outcomes72 while Mohammadpour et al. (2020) demonstrated reductions in anxiety and enhanced perceived support in pregnant adolescents following structured education73.
Taken together, these findings highlight the importance of embedding life skills training and mental health literacy into adolescent antenatal care. Developmentally appropriate, culturally sensitive interventions are critical to promoting mental well-being in this vulnerable population, particularly in settings where family and societal structures exert a strong influence on maternal experiences and outcomes74.
Despite these promising results, the study has several limitations. First, although participants were recruited using a convenience sampling method, potential selection bias was minimized through random allocation, concealed assignment, and comparable baseline characteristics between groups. Nonetheless, the use of convenience sampling may limit generalizability, and this limitation has been acknowledged accordingly. The participants were drawn from a culturally specific, predominantly collectivist community in southern Iran, where strong family networks, early marriage norms, and the central role of midwives may influence both perceived social support and responsiveness to psychoeducational interventions. These cultural and demographic characteristics may not reflect adolescent populations in other regions or health systems. Future studies should replicate this model in more diverse sociocultural contexts and with probability-based sampling to strengthen external validity. Second, another potential limitation of this study is the possibility of information transfer between participants or facilitators in the intervention and control groups, which could lead to contamination bias. To minimize this risk, the intervention sessions were conducted by midwives who received standardized training and followed a unified session checklist to ensure consistent delivery. Separate timing and locations were arranged for the two groups, confidentiality was emphasized, and random monitoring of control sessions confirmed adherence to routine prenatal protocols. Although complete elimination of contamination is not possible in educational interventions, these measures considerably reduced its likelihood, and the results should therefore be interpreted with appropriate caution. Third, no postpartum follow-up was conducted to determine the sustainability of the intervention’s benefits. Future studies should incorporate longitudinal follow-up, including postpartum assessments, to determine the durability of the intervention’s effects and to better understand how maternal psychological outcomes evolve after childbirth. Fourth, another limitation is that the study did not formally assess the influence of family or partner support, despite their well-documented role in shaping adolescents’ psychological well-being and engagement with prenatal care. Because these relational factors may interact with or amplify the effects of psychoeducational interventions, future studies should incorporate validated measures of family- and partner-based support to more comprehensively capture the contextual determinants of adolescent maternal mental health. Finally, another important limitation relates to the inability to blind participants and facilitators, which is inherent to psychoeducational interventions. This may introduce expectancy effects or response bias, particularly for self-reported measures such as anxiety, stress, and depression. Although we attempted to mitigate this risk by using blinded outcome assessors, standardized questionnaire procedures, and validated instruments, the potential influence of subjective awareness of group assignment cannot be fully excluded.
Nonetheless, this study offers meaningful implications for clinical practice. Embedding life skills education into routine prenatal care presents a feasible, cost-effective, and scalable approach to improving adolescent maternal mental health. Its delivery by midwives within existing health infrastructure further supports its real-world applicability, especially in low-resource environments. As adolescent pregnancy continues to pose public health challenges, particularly in low- and middle-income countries such interventions may play a key role in closing service gaps and supporting psychological resilience in this at-risk population.
Future studies need to extend evaluation into the postpartum period to assess the durability of outcomes related to maternal mental health, parenting, and infant development. Studies incorporating family and partner perspectives would also help elucidate the broader social dynamics influencing intervention impact. Finally, there is a pressing need to design and test culturally tailored programs across diverse contexts, ensuring their relevance, acceptability, and effectiveness for adolescent mothers worldwide. These findings directly support the policy recommendation outlined in the Declarations, underscoring the feasibility of integrating midwife-led psychoeducational life skills programs into standard antenatal care to enhance adolescent maternal mental health.
Conclusion
This randomized controlled trial offers robust evidence that integrating a psychoeducational life skills program into routine midwife-led antenatal care can significantly enhance the psychological well-being of pregnant adolescents. The intervention resulted in substantial reductions in pregnancy-related anxiety, perceived stress, and depressive symptoms, underscoring its effectiveness as a targeted psychosocial strategy during this critical developmental period.
Although both the intervention and control groups demonstrated improvements in perceived social support over time, the between-group difference was not statistically significant. This finding may reflect the baseline support already provided through standard childbirth preparation classes. Nevertheless, the overall trend suggests that structured life skills education, when embedded within routine care, can contribute to strengthening adolescents’ support networks and fostering a sense of community.
Given its accessibility, feasibility, and compatibility with existing maternal health services, integrating life skills education into antenatal programs represents a scalable model for addressing the mental health needs of pregnant adolescents, an often underserved and vulnerable population. This approach not only equips young mothers with essential coping and problem-solving skills but also promotes emotional resilience and healthier maternal-child outcomes.
Further research should investigate the long-term effects of such interventions on postpartum mental health and parenting, explore the potential benefits of involving partners and family members, and evaluate the adaptability of the program across diverse cultural and socioeconomic contexts. Expanding this approach could play a critical role in reducing the global burden of perinatal mental health disorders and fostering more supportive environments for adolescent mothers.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to confidentiality and privacy concerns of adolescent participants, but are available from the corresponding author on reasonable request.
Abbreviations
- WHO:
-
World Health Organization
- EDS:
-
Edinburgh Depression Scale
- PSS:
-
Perceived Stress Questionnaire
- SPSS:
-
Statistical Package for the Social Sciences
- ANOVA:
-
Analysis of Variance
- CONSORT:
-
Consolidated Standards of Reporting Trials
References
Teekhasaenee, T. & Kaewkiattikun, K. Birth preparedness and complication readiness practices among pregnant adolescents in Bangkok. Thail. Adolesc. Health Med. Ther. 11, 1 (2020).
Adolescent pregnancy 31 January. 2020 [Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy
Mohammadi, N., Montazeri, S., Ardabili, H. E. & Gharacheh, M. Iranian pregnant teenage women tell the story of fast development: A phenomenological study. Women Birth. 29 (4), 303–309 (2016).
Laurenzi, C. A. et al. Psychosocial interventions targeting mental health in pregnant adolescents and adolescent parents: a systematic review. Reproductive Health. 17 (1), 1–15 (2020).
Ernestina Coast, M. M. M., Roberte Isimbi, E., Ngabonzima, P., Pereznieto, S. & Buzby Rebecca Dutton & Sarah Baird ‘If she’s Pregnant, then that means that her Dreams fade away’: exploring experiences of adolescent pregnancy and motherhood in Rwanda. Eur. J. Dev. Res. 33, pages1274–pages1302 (2021).
Fleming, N. et al. Adolescent pregnancy guidelines. J. Obstet. Gynecol. Can. 37 (8), 740–756 (2015).
Davis, E. P. et al. Prenatal maternal anxiety and depression predict negative behavioral reactivity in infancy. Infancy 6 (3), 319–331 (2004).
Dunkel Schetter, C. Psychological science on pregnancy: stress processes, biopsychosocial models, and emerging research issues. Ann. Rev. Psychol. 62 (1), 531–558 (2011).
Lobel, M. et al. Pregnancy-specific stress, prenatal health behaviors, and birth outcomes. Health Psychol. 27 (5), 604 (2008).
Mehraban, Z., Alizadeh, L. & Narimani, M. Maternal prenatal pregnancy-related anxiety and spontaneous preterm birth in ardebil health centers in 2011. Stud. Med. Sci. 23 (6), 670–675 (2013).
Weissman, M. M. & Olfson, M. Depression in women: implications for health care research. Science 269 (5225), 799–801 (1995).
Kang, Y. et al. Prevalence and risk factors of maternal anxiety in late pregnancy in China. Int. J. Environ. Res. Public Health. 13 (5), 468 (2016).
Rahimi, F. A. M., Rosta, F., Majd, H. A. & Valiani, M. Effect of relaxation training on pregnancy anxiety in high risk women. Saf. Promotion Injury Prev. 2 (3), 180–188 (2014).
Torabi, M., Salavati, M. & Sarabi, A. G. Effect of foot reflexology massage and Benson relaxation techniques on anxiety and physiological indexes of patients undergoing coronary heart angiography. Avicenna J. Nurs. Midwifery Care. 20 (1), 63–73 (2012).
Alio, A. P., Mbah, A. K., Grunsten, R. A. & Salihu, H. M. Teenage pregnancy and the influence of paternal involvement on fetal outcomes. J. Pediatr. Adolesc. Gynecol. 24 (6), 404–409 (2011).
Weiss, J. A. Who will listen? Rural teen pregnancy reflections. J. Nurse Practitioners. 8 (10), 804–809 (2012).
Wainaina, C. W. et al. Psychosocial challenges and individual strategies for coping with mental stress among pregnant and postpartum adolescents in Nairobi informal settlements: a qualitative investigation. BMC Pregnancy Childbirth. 21 (1), 1–11 (2021).
Naghizadeh, S. Comparison of pregnancy self-care, perceived social support and perceived stress in low-risk and high-risk groups. J. Health Care. 21 (1), 16–25 (2019).
Farokhi, F. Quality assessment of midwives performance in prenatal cares in urban health centers in Mashhad, Iran. Payesh (Health Monitor). 7 (3), 0 (2008).
Razavinia, F. et al. The effect of a midwifery continuity of care program on clinical competence of midwifery students and delivery outcomes: a mixed-methods protocol. BMC Med. Educ. 24 (1), 338 (2024).
Mann, J. R., Mannan, J., Quiñones, L. A., Palmer, A. A. & Torres, M. Religion, spirituality, social support, and perceived stress in pregnant and postpartum Hispanic women. J. Obstetric Gynecologic Neonatal Nurs. 39 (6), 645–657 (2010).
Brand, G., Morrison, P. & Down, B. How do health professionals support pregnant and young mothers in the community? A selective review of the research literature. Women Birth. 27 (3), 174–178 (2014).
Govender, D., Taylor, M. & Naidoo, S. Adolescent pregnancy and parenting: perceptions of healthcare providers. J. Multidisciplinary Healthc. 13, 1607 (2020).
Hassanpour, F., Javadnoori, M., Maraghi, E. & Zargar Shirazi, F. Effect of life skills training by a midwife on pregnancy anxiety: A randomized controlled trial. Avicenna J. Nurs. Midwifery Care. 32 (4), 288–298 (2024).
Ghazaie, M., Davoodi, I., Neysi, A., Honarmand, M. M. & Nejad, S. B. The effectiveness of cognitive-behavioral therapy on fear of childbirth, fear of pain, self-efficacy of childbirth and tendency to caesarean in nulliparous women. (2016).
Najafi, F., Abouzari-Gazafroodi, K., Jafarzadeh-Kenarsari, F., Rahnama, P. & Gholami Chaboki, B. Relationship between attendance at childbirth Preparation classes and fear of childbirth and type of delivery. Hayat 21 (4), 30–40 (2016).
Madhukaillya, M. Smriti. Design Intervention To Teach Life Skills: Understanding Life Skills and Designing a Pedagogy To Teach Stress Management p. 15–22 (Springer, 2022).
Sherif, Y. et al. Effectiveness of life skills intervention on Depression, anxiety and stress among children and adolescents: A systematic review. Malaysian J. Med. Sciences: MJMS. 30 (3), 42–59 (2023).
LIFE SKILLS EDUCATION - World Health Organization. [ (1996). Available from: https://iris.who.int/bitstream/handle/10665/338491/MNH-PSF-96.2.Rev.1-eng.pdf
Montgomery, K. S. Planned adolescent pregnancy: themes related to the pregnancy. J. Perinat. Educ. 13 (4), 27 (2004).
Dehghan-Nayeri, N. & Tajvidi, M. Experiences of pregnancy among Iranian adolescents: A qualitative study. Iran. J. Nurs. Midwifery Res. 19 (7 Suppl 1), S7–s12 (2014).
Laurenzi, C. A. et al. Psychosocial interventions targeting mental health in pregnant adolescents and adolescent parents: a systematic review. Reproductive Health. 17 (1), 65 (2020).
Mousavi, S. R. & Amiri Farahani, L. Effectiveness of virtual and In-person methods of education on pregnant women’s satisfaction with childbirth Preparation classes: A pilot study. J. Client-Centered Nurs. Care. 8 (4), 253–264 (2022).
1, M. M. & 2, V. A. 3 The relationship between depression during pregnancy with social support and some demographic variables in pregnant women. IJOGI 18 (142), 12–20 (2015).
Asghari, F., Sadeghi, A., Aslani, K., Saadat, S. & Khodayari, H. The survey of relationship between perceived stress coping strategies and suicide ideation among students at university of Guilan, Iran. Int. J. Educ. Res. 1 (11), 111–118 (2013).
Azevedo FBd, Wang, Y-P., Goulart, A. C., Lotufo, P. A. & Benseñor, I. M. Application of the spielberger’s state-trait anger expression inventory in clinical patients. Arq. Neuropsiquiatr. 68, 231–234 (2010).
Askarizadeh, G., Karamoozian, M. & Darekordi, A. Validation of Iranian version of pregnancy related anxiety questionnaire. Int. J. Prev. Med. 8 (1), 17 (2017).
Behroozi, N., Shahani Yeylaq, M. & Pourseyed, S. M. Relationship between perfectionism, perceived stress and social support with academic burnout. (2013).
Dolatian, M. & Alavi Majd, H. Comparison of pregnancy self-care, perceived social support and perceived stress of women with gestational diabetes and healthy pregnant women. Iran. J. Endocrinol. Metabolism. 16 (3), 156–164 (2014).
Cohen, S., Kamarck, T. & Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. :385–396. (1983).
Bastani, F., Rahmatnejad, L., Jahdi, F. & Haghani, H. Breastfeeding self efficacy and perceived stress in primiparous mothers. Iran. J. Nurs. 21 (54), 9–24 (2008).
Jafarnejad, F., Azmoudeh, E., Mazloum, S. R. & Reyhani, T. The effect of self-efficacy training package on maternal self-confidence of primiparous women in infant care. Iran. J. Obstet. Gynecol. Infertility. 17 (104), 18–28 (2014).
Wisner, K. L., Parry, B. L. & Piontek, C. M. Clinical practice. Postpartum depression. N. Engl. J. Med. 347 (3), 194–199 (2002).
Boobpamala, S., Kongvattananon, P. & Griffin, M. T. Q. Effectiveness of an early depression prevention program on coping skills and depression among pregnant adolescents: A randomized controlled trial. Pac. Rim Int. J. Nurs. Res. 26 (2), 296–312 (2022).
Lesinskienė, S., Andruškevič, J. & Butvilaitė, A. Adolescent pregnancies and perinatal mental Health-Needs and complex support options: A literature review. J. Clin. Med. ;14(7). (2025).
Ediz, Ç. & Kavak Budak, F. Effects of psychosocial support-based psychoeducation for Turkish pregnant adolescents on anxiety, depression and perceived social support: a randomized controlled study. Rural Remote Health. 23 (3), 7553 (2023).
Mhango, W., Crowter, L., Michelson, D. & Gaysina, D. Psychoeducation as an active ingredient for interventions for perinatal depression and anxiety in youth: a mixed-method systematic literature review and lived experience synthesis. BJPsych open. 10 (1), e10 (2023).
Akgün, M., Boz, İ. & Özer, Z. The effect of psychoeducation on fear of childbirth and birth type: systematic review and meta-analysis. J. Psychosom. Obstet. Gynaecol. 41 (4), 253–265 (2020).
Motrico, E. et al. Effectiveness of interventions to prevent perinatal depression: an umbrella review of systematic reviews and meta-analysis. Gen. Hosp. Psychiatry. 82, 47–61 (2023).
McMullen, J. D. & McMullen, N. Evaluation of a teacher-led, life-skills intervention for secondary school students in Uganda. Social science & medicine 2018;217:10 – 7. (1982).
Mohammadi, M. M. & Poursaberi, R. The effects of Stress-coping strategies and life skills trainings on the mental health and academic progress of adolescent cancer patients: A Quasi-experimental study. Nurs. Midwifery Stud. 7 (1), 12–17 (2018).
Roy, K. K. V., Kamath, A., Hegde, A., Alex, J. & Ashok, L. Effectiveness of life skill training program on stress among adolescents at a school setting. J. Indian Association Child. Adolesc. Mental Health Oct. 1 (4), 309–322 (2016).
Kachingwe, M., Chikowe, I., van der Haar, L. & Dzabala, N. Assessing the impact of an intervention project by the young women’s Christian association of Malawi on psychosocial Well-Being of adolescent mothers and their children in Malawi. Front. Public. Health. 9, 585517 (2021).
Mohammadzadeh, M., Awang, H., Ismail, S. & Kadir Shahar, H. Improving emotional health and self-esteem of Malaysian adolescents living in orphanages through life skills education program: A multi-centre randomized control trial. PloS One. 14 (12), e0226333 (2019).
Eslami, A. A., Rabiei, L., Afzali, S. M., Hamidizadeh, S. & Masoudi, R. The effectiveness of assertiveness training on the levels of Stress, Anxiety, and depression of high school students. Iran. Red Crescent Med. J. 18 (1), e21096 (2016).
Lee, M-J. et al. Effectiveness of a school-based life skills program on emotional regulation and depression among elementary school students: A randomized study. Child Youth Serv. Rev. 118, 105464 (2020).
Dennis, C. L., Ross, L. E. & Grigoriadis, S. Psychosocial and psychological interventions for treating antenatal depression. Cochrane Database Syst. Rev. (3):Cd006309. (2007).
Brixval, C. S., Axelsen, S. F., Andersen, S. K., Due, P. & Koushede, V. The effect of antenatal education in small classes on obstetric and psychosocial outcomes – a systematic review. Syst. Reviews. 5 (1), 1–12 (2016).
Leahy-Warren, P., McCarthy, G. & Corcoran, P. First-time mothers: social support, maternal parental self-efficacy and postnatal depression. J. Clin. Nurs. 21 (3–4), 388–397 (2012).
Mohammadi, N., Montazeri, S., Alaghband rad, J., Ardabili, H. E. & Gharacheh, M. Iranian pregnant teenage women tell the story of fast development: A phenomenological study. Women Birth. 29 (4), 303–309 (2016).
Brand, G., Morrison, P. & Down, B. How do health professionals support pregnant and young mothers in the community? A selective review of the research literature. Women Birth: J. Australian Coll. Midwives. 27 (3), 174–178 (2014).
Yurdakul, M. Perceived social support in pregnant adolescents in Mersin area in Turkey. Pakistan J. Med. Sci. 34 (1), 115–120 (2018).
Baheiraei, A., Mirghafourvand, M., Mohammadi, E., Charandabi, S. M. & Nedjat, S. Social support for women of reproductive age and its predictors: a population-based study. BMC Womens Health. 12, 30 (2012).
Maharlouei, N. The importance of social support during pregnancy. Women’s Health Bull. 3 (1), 1 (2016).
Renbarger, K. M., Place, J. M. & Schreiner, M. The influence of four constructs of social support on pregnancy experiences in group prenatal care. Women’s Health Rep. 2 (1), 154–162 (2021).
Azmoude, E., Jaafarnejad, F. & Mazloum, S. Effect of self-efficacy-based training on maternal sense of competency of primiparous women in the infants care. Evid. Based Care. 4 (3), 7–14 (2014).
Hajihatamloo, H., Ebrahimi, M., Alinejad, V. & Bayrami, R. Anxiety, self-compassion, perceived social support and resilience in two groups of primiparous pregnant women fully and not attending childbirth Preparation classes. BMC Psychol. 13 (1), 467 (2025).
Hölzle, L. et al. Identifying and synthesizing components of perinatal mental health peer support - a systematic review. Front. Psychiatry. 15, 1389545 (2024).
Norazman, C. W. & Lee, L. K. The Influence of Social Support in the Prevention and Treatment of Postpartum Depression: an intervention-based Narrative Review Vol. 20, 17455057241275587 (Women’s health, 2024).
Aromatario, O. et al. Improving personal, social, and life skills in adolescents: a scoping review of key components in interventions. J. Public Health (2024).
Kauts, D. S. & Saini, J. Life skill based education: A systematic narrative review. MIER J. Educational Stud. Trends Practices :407–422. (2022).
Asadzadeh, L., Jafari, E., Kharaghani, R. & Taremian, F. Effectiveness of midwife-led brief counseling intervention on post-traumatic stress disorder, depression, and anxiety symptoms of women experiencing a traumatic childbirth: a randomized controlled trial. BMC Pregnancy Childbirth. 20 (1), 142 (2020).
Ertekin Pinar, S., Daglar, G. & Duran Aksoy, O. The effect of stress management training on perceived stress, anxiety and hopelessness levels of women with high-risk pregnancy. J. Obstet. Gynaecology: J. Inst. Obstet. Gynecol. 42 (1), 17–22 (2022).
Health, L. L. U. B. Pregnant teens deserve optimal care: Why comprehensive, developmentally appropriate prenatal care is essential. (2025) [updated January 14, 2025]. Available from: https://behavioralhealth.llu.edu/blog/pregnant-teens-deserve-optimal-care-why-comprehensive-developmentally-appropriate-prenatal-care-essential
Acknowledgements
The study is part of the results of the PhD dissertation of the first author in midwifery (research project number: 330101729). The authors would like to thank all the participants in this study and Ahvaz Jundishapur University of Medical Sciences in Iran. We would like to thank Mr. Navid Jahanshahi, PhD Candidate at the Faculty of Letters, University of Lisbon, and member of the Lisbon Baby Lab, for his assistance in editing the English language of this manuscript.
Funding
This study was financially supported by the Office of Research and Technology at Ahvaz Jundishapur University of Medical Sciences, under Grant Number 330101729.
Author information
Authors and Affiliations
Contributions
S.Y. contributed to project development, data collection, data analysis and interpretation, manuscript drafting, and final approval. S.M. and N.J. contributed to project development and approved the final version. S.Gh. was responsible for data analysis and interpretation. All training sessions during the intervention were supervised by A.A. All authors contributed to the manuscript revisions and approved the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1402.140). Written informed consent was obtained from all participants. All procedures were conducted in accordance with the Declaration of Helsinki. The study protocol was also registered in the Iranian Registry of Randomized Controlled Trials on 2023-06-26 (IRCT20190129042544N1). Prior to participation, permission was obtained from all participants. A comprehensive consent form was prepared, which included a clear and concise explanation of the research objectives and procedures. Participants were required to read, complete, and sign the form. Additionally, permission was obtained for recording interviews, and measures were implemented to ensure the confidentiality and anonymity of all participants throughout the study.
Policy recommendations
The findings of this study can support healthcare providers and policymakers in designing and implementing effective interventions to reduce complications associated with adolescent pregnancy.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yousefi, S., Montazeri, S., Javadifar, N. et al. Midwife-led psychoeducational life skills training reduces anxiety, stress, and depression in pregnant adolescents: a randomized trial. Sci Rep 15, 45081 (2025). https://doi.org/10.1038/s41598-025-32021-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-32021-x
