
Abstract
Serum osmolality (SOSM) levels have been reported to be associated with the prognosis of critically ill patients. The purpose of this study was to analyze the impact of the trajectory of changes in SOSM on the 28-day mortality risk in patients with sepsis-associated delirium (SAD). Latent class trajectory modeling (LCTM) was employed in this retrospective cohort study of patients with SAD from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. SOSM trajectories were derived using LCTM based on three measurements obtained at two-day intervals during the first six days following ICU admission. The relationship between the SOSM and 28-day mortality risk was explored using restricted cubic spline (RCS), Cox regression models, and Kaplan–Meier curves. Subgroup analyses were conducted to examine the association and stability of SOSM trajectories with SAD patients’ outcome. Among the 3100 SAD patients included in the analysis, 488 (15.7%) died within 28 days. The median SOSM level was 294.8 (IQR 288.1–302.0) mmol/L. LCTM identified four distinct SOSM trajectories: normal-level-steady trend trajectory (Class 1), normal-level-increasing trend trajectory (Class 2), normal-level-decreasing and then increasing trend trajectory (Class 3), and normal-level-increasing and then decreasing trend trajectory (Class 4). Elevated baseline SOSM levels were independently associated with higher 28-day mortality (HR 1.02, 95% CI 1.01–1.03). RCS revealed a positive linear association between baseline SOSM levels and 28-day mortality risk (P overall < 0.001; P non-linearity = 0.87). Compared with Class 1, patients in Class 2 (HR 1.62, 95% CI 1.31–2.01), Class 3 (HR 1.71, 95% CI 1.19–2.47), and Class 4 (HR 1.99, 95% CI 1.39–2.84) exhibited significantly increased 28-day mortality risk. Subgroup analyses further demonstrated that the trajectory 2 was consistently associated with 28-day mortality in SAD patients aged over 60 years. SOSM was an independent risk factor for 28-day mortality in patients with SAD. Persistent elevation and fluctuation of SOSM trajectories after ICU admission were associated with increased 28-day mortality in patients with SAD.
Similar content being viewed by others


Introduction
Sepsis is a syndrome of multiple organ dysfunction arising from a dysregulated host response to infection1. Globally, it remains the leading cause of death in intensive care unit (ICU), with the ensuing organ failure accounting for its high mortality. Neurological manifestations of sepsis are collectively termed sepsis-associated encephalopathy (SAE), of which delirium is the predominant early feature2. Sepsis-associated delirium (SAD) is defined as an acute disturbance of mental status in the absence of central nervous system infection, characterized by impaired cognition, attentional deficits, and temporal fluctuation3. SAD is independently associated with increased short-term mortality, a heightened risk of long-term dementia and epilepsy, diminished quality of life, and a substantial global disease burden. Early and precise identification of risk factors for SAD progression, together with timely and effective interventions, is crucial for improving patient outcomes.
Serum osmolality (SOSM) reflects the balance between solutes and water in the circulation and serves as a key indicator of hydration status. Fluctuations in SOSM generate osmotic gradients that regulate transmembrane water flux, thereby exerting a critical influence on fluid homeostasis, cellular function, and electrolyte stability4,5,6. Perturbations in SOSM may arise from iatrogenic hypernatremia, impaired renal excretion, or disease-related metabolic alterations, disrupting the cellular microenvironment and physiological processes, and ultimately contributing to mortality in critically ill patients. Abnormal SOSM levels have been linked to adverse outcomes in heart failure, sepsis, traumatic intracerebral hemorrhage, and myocardial infarction7,8,9,10. Nonetheless, the association between SOSM and 28-day mortality risk in patients with SAD has not yet been elucidated.
Accordingly, this study utilized a large critical care database and applied latent class trajectory modeling (LCTM) to delineate longitudinal patterns of SOSM in patients with SAD11. By integrating cross-sectional and temporal data, it identified clinically meaningful SOSM trajectories. These insights may provide new avenues for the early evaluation and management of SAD, with the potential to improve patient prognosis and reduce healthcare burden.
Methods
Data source and study population
This study was a retrospective cohort study based on the large single-center database Medical Information Mart for Intensive Care IV (MIMIC-IV). The MIMIC-IV database collected information on patient demographics, laboratory measurements, vital signs, medication use, and mortality information. The author, Z.Y.H., gained access to the database by successfully completing the web-based training and examination provided by the National Institutes of Health (No. 67867250). The MIMIC-IV database had received ethical approval from the Institutional Review Boards of the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center. Informed consent may be waived for anonymized personal information12. As the present study did not involve the collection of additional data, no further ethical approval or informed consent was necessary.
SAD was defined as new-onset delirium after the diagnosis of sepsis. Sepsis was defined as a documented or suspected source of infection and a sequential organ failure assessment (SOFA) score ≥ 2 according to the Sepsis-3 criteria1. Delirium was defined as a response to verbal stimuli, eye opening, a positive Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)13. Previous reports indicated that the CAM-ICU shows a pooled sensitivity of 81% (95% CI 57–93%) and a pooled specificity of 98% (95% CI 86–100%) in delirium screening, highlighting its reliability for the precise diagnosis of delirium13. Exclusion criteria were as follows: missing survival information or laboratory measurements; intracranial infection or abscess; dementia; continuous renal replacement therapy (CRRT); end-stage renal disease; severe liver disease; malignant tumor; and the length of ICU stay was less than 3 h.
Data collection and endpoint
PostgreSQL and Navicat Premium (version 17.0.12) were used to retrieve anonymized patient hospitalizations. Confounding variables included the following: demographics data: age, gender, race; vital signs: mean arterial pressure (MAP), temperature, respiratory rate; laboratory measurements: sodium, glucose, blood urea nitrogen (BUN), white blood cell (WBC) count, hemoglobin concentration, platelet count, calcium, potassium, creatinine, lactate, activated partial thromboplastin time (APTT), prothrombin time(PT), international normalized ratio (INR), alanine aminotransferase (ALT), aspartate aminotransferase (AST), urine output, albumin, chloride, bicarbonate, arterial oxygen partial pressure (PO2), arterial carbon dioxide partial pressure (PCO2); comorbidities: congestive heart failure, cerebrovascular disease, chronic pulmonary disease, diabetes, AKI; medication use: furosemide use, vasopressor use, midazolam exposure; special scores: SOFA, Charlson comorbidity index (CCI), Glasgow coma scale (GCS), and acute physiology score III (APS III); treatment measures: mechanical ventilation. Variables with > 20% missing values were excluded, while those with < 20% missing values were imputed using the MICE package. The distribution of missing data is shown in Table S1. Comorbidities were identified using ICD-9/10 codes in the MIMIC-IV database.
The primary endpoint was 28-day mortality. The 28-day mortality was defined as the mortality that occurred within 28 days of ICU admission. Patients were followed from ICU admission until day 28 or death within 28 days. For patients with multiple hospitalizations, only data from the first ICU admission were analyzed.
Exposure
Sodium, glucose, and BUN levels measured on days 0–2, 2–4, and 4–6 days after ICU admission that were used to calculate SOSM levels. The SOSM levels were calculated using the following formula: sodium × 2 + (glucose/18) + (BUN/2.8)14. The normal reference range for SOSM levels was 280–310 mmol/L based on the reference values from the previous study 15. The current study divided SOSM levels on ICU admission into three groups: normal SOSM group Q1 (280–310 mmol/L), low SOSM group Q2 (< 280 mmol/L), and high SOSM group Q3 (> 310 mmol/L).
Statistical analysis
The Kolmogorov–Smirnov test was applied to assess the distribution of continuous variables. Owing to their non-normal distribution, continuous variables were presented as medians with interquartile ranges (IQRs) and were compared across groups using the Kruskal–Wallis test. Categorical variables were expressed as counts and percentages, and group differences were assessed using the chi-square test or Fisher’s exact test, as appropriate.
Latent class trajectory modeling (LCTM) was applied to identify SOSM trajectories within the first six days of ICU admission, using the LCMM package in R. An initial baseline model without covariates was fitted to establish the optimal model structure. LCTM partitions the study population into latent classes, each defined by similar temporal trajectories, while accounting for both inter- and intra-individual variability. Trajectory assignment was probabilistic and based on longitudinal data patterns. The optimal number of trajectory classes was determined using predefined criteria: minimization of the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC), entropy > 0.7, class proportions > 2%, and Average posterior probabilities (AvePP) > 70%16.
The univariate and multivariable Cox regression models were utilized to assess the association between SOSM levels (continuous and categorical) at ICU admission, SOSM trajectories within 6 days of ICU admission and the risk of 28-day mortality in patients with SAD. The hazard ratios (HRs) and 95% confidence intervals (95% CIs) were estimated. Confounding variables included variables selected based on P < 0.05 in univariate analysis, and clinically relevant and prognosis-associated variables were also enrolled in the multivariate model. Model 1: unadjusted; model 2: adjusted for age, gender, and race; model 3: adjusted for age, race, PCO2, PO2, respiratory rate, congestive heart failure, cerebrovascular disease, diabetes, CCI, vasopressor use, furosemide use, midazolam exposure, APS III, SOFA score, GCS, mechanical ventilation, AKI, urine output, INR, APTT, PT, chloride, bicarbonate, calcium, potassium, creatinine, hemoglobin, and lactate. The restricted cubic spline (RCS) curve was used to explore potential nonlinear associations between SOSM levels and the risk of 28-day mortality in patients with SAD. The Kaplan–Meier (K-M) curves were employed to assess the incidence rate of 28-day mortality among different trajectory classes of the SOSM, and their differences were assessed through the log-rank test. Multicollinearity was assessed using variance inflation factor (VIF), with values below 10 indicating the absence of substantial multicollinearity among the variables. All statistical analyses were performed using R software (version 4.4.3) and SPSS 26.0 (IBM SPSS Statistics, Armonk, NY, USA), and two-sided P < 0.05 was considered statistically significant.
Results
Baseline characteristics
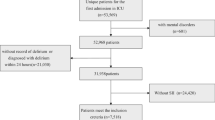
Figure 1 presented the flowchart of patient enrollment, through which 3,100 patients with SAD were included in the final cohort. Table 1 shows the characteristics of patients with SAD according to the 4 classes of SOSM trajectories. Age, race, SOFA score, PCO2, PO2, respiratory rate, congestive heart failure, diabetes, CCI, vasopressor use, furosemide use, APS III, GCS, mechanical ventilation, AKI, urine output, INR, PT, chloride, bicarbonate, calcium, potassium, creatinine, WBC, and lactate were significant differences in 4 trajectories (P < 0.05). Patients in trajectory 2 were distinguished by advanced age, greater comorbidity burden, including congestive heart failure and diabetes, higher CCI, and more frequent use of vasopressor and furosemide, as well as the highest rates of mechanical ventilation and AKI. Trajectory 3 was characterized by the lowest PO2 and urine output, together with the highest APS III. In contrast, Trajectory 4 exhibited the lowest PCO2 and the greatest prevalence of cerebrovascular disease.

Flow chart of patient’s enrollment.
The median age of the patients was 68.03 (55.59, 78.40) years, and the median SOFA score was 3 (2, 4). There were 1350 (43.5%) male patients, 1028 (33.2%) patients with congestive heart failure, 823 (26.5%) patients with cerebrovascular disease, 908 (29.3%) patients with chronic pulmonary disease, and 921 (29.7%) patients with diabetes. There were 2876 (92.8%) patients with AKI and 2966 (95.7%) patients with mechanical ventilation. The median follow-up time was 28.00 (28.00, 28.00) days, and 488 (15.74%) patients died during the follow-up period. The median SOSM was 294.8 (IQR 288.1–302.0) mmol/L.
Correlation of baseline SOSM levels with 28-day mortality risk
Table 2 shows the association between baseline SOSM levels and 28-day mortality risk. In univariate (HR = 1.02, 95% CI 1.02–1.02) and multivariate (HR = 1.02, 95% CI 1.01–1.03) Cox regression models, high SOSM levels were associated with an increased risk of 28-day mortality. In further analysis, the RCS demonstrated a significant linear and positive relationship between SOSM and 28-day mortality risk (P overall < 0.001, P non-linearity = 0.87) (Fig. 2). Categorizing the baseline SOSM levels, the high SOSM group Q3 was linked to the risk of 28-day mortality in SAD patients not only in univariate models (HR = 2.34, 95% CI 1.88–2.90) but also in multivariate models (HR = 1.50, 95% CI 1.14–1.96) when compared to the normal SOSM group Q1. Table S3 shows the baseline characteristics of the patients in the three SOSM groups. The Q3 group had older age, higher WBC, SOFA score, and CCI, lower PO2, and urine output (P < 0.05). Figure 3 shows the K-M curves according to the three SOSM groups, with a significantly increased 28-day mortality risk in the Q3 group (P < 0.001). Table S2 demonstrated that all continuous variables exhibited VIF values below 10, indicating the absence of multicollinearity.

The restricted cubic spline (RCS) curve for the potential linear associations between SOSM levels and the risk of 28-day mortality in patients with SAD.

Kaplan–Meier curves for SAD patients with different SOSM groups. Q1: SOSM 280–310 mmol/L, Q2: SOSM < 280 mmol/L, Q3: SOSM > 310 mmol/L.
Correlation of SOSM trajectories with 28-day mortality risk
Based on these metrics and class distribution (Supplementary Table S4), four distinct SOSM trajectory classes were identified, with each class achieving an AvePP exceeding 70% (Supplementary Table S5). There were 2218 (71.55%) patients in the normal-level-steady trend trajectory (Class 1), 577 (18.61%) patients in the normal-level-increasing trend trajectory (Class 2), 141 (4.55%) patients in the normal-level-decreasing and then increasing trend trajectory (Class 3), and 164 (5.29%) patients in the normal-level-increasing and then decreasing trend trajectory (Class 4). Figure 4 shows the detailed 4 classes of trajectories of the SOSM.

SOSM classes (trajectories) within 6days (144 h) of ICU admission in patients with SAD. Class 1 exhibited normal-level-steady trend trajectory. Class 2 exhibited normal-level-increasing trend trajectory. Class 3 exhibited normal-level-decreasing and then increasing trend trajectory. Class 4 exhibited normal-level-increasing and then decreasing trend trajectory.
Compared with trajectory 1, trajectory 2 (HR = 1.62, 95% CI 1.31–2.01), trajectory 3 (HR = 1.71, 95% CI 1.18–2.46), and trajectory 4 (HR = 1.99, 95% CI 1.39–2.85) were associated with an increased risk of 28-day mortality (Table 2). Figure 5 shows the K-M curves according to SOSM trajectories, with a significant difference in 28-day mortality risk between the SOSM trajectory classes compared with Class 1 (P < 0.001). The 28-day mortality rates of SOSM trajectory 1, 2, 3, and 4 were 264 (11.90%), 146 (25.30%), 40 (28.37%), and 38 (23.17%), respectively.

Kaplan–Meier curves for SAD with different SOSM classes (trajectories). Class 1 exhibited normal-level-steady trend trajectory. Class 2 exhibited normal-level-increasing trend trajectory. Class 3 exhibited normal-level-decreasing and then increasing trend trajectory. Class 4 exhibited normal-level-increasing and then decreasing trend trajectory.
Subgroup analysis and interaction
To evaluate the association and robustness of SOSM trajectories with 28-day mortality, subgroup analyses were stratified by age, gender, race, congestive heart failure, cerebrovascular disease, chronic pulmonary disease, diabetes, the use of furosemide, and vasopressor use. The forest plots (Fig. 6 and Fig. S1) demonstrated that SOSM trajectory 2 was associated with elevated 28-day mortality risk in patients with SAD aged > 60 years and comorbid congestive heart failure, cerebrovascular disease, chronic pulmonary disease, or diabetes. SOSM trajectory 3 was linked to increased mortality risk in patients > 60 years with concomitant congestive heart failure and diabetes, but without cerebrovascular disease or chronic pulmonary disease. SOSM trajectory 4 conferred a heightened risk of 28-day mortality in patients > 60 years with congestive heart failure and cerebrovascular disease, but without chronic pulmonary disease or diabetes. No significant interactions were observed between SOSM trajectories and the examined subgroups.

Subgroup analysis for associations between SOSM trajectories and the risk of 28-day mortality according to age, gender, race, congestive heart failure, and cerebrovascular disease.
Discussion
The present study investigated the association between baseline SOSM levels at ICU admission, SOSM trajectories over the first six days of ICU stay, and survival outcomes in patients with SAD. After adjustment for pertinent confounders, elevated SOSM levels at admission were independently linked to an increased risk of 28-day mortality. Especially when SOSM levels exceeded 310 mmol/L, the 28-day mortality risk in SAD patients increased by 1.5-fold (HR 1.50, 95% CI 1.14–1.96; P = 0.003). Moreover, longitudinal trajectory analysis demonstrated that, in contrast to patients with normal and stable trend trajectories, those with normal-level-increasing trend trajectory, normal-level-decreasing and then increasing trend trajectory, and normal-level-increasing and then decreasing trend trajectory were at a higher risk of 28-day mortality. Subgroup analyses confirmed the robustness of these findings across diverse patient strata.
SOSM represents the solute concentration per unit mass of serum water and is chiefly governed by circulating sodium, glucose, and BUN levels. SOSM underlies a range of essential physiological processes, including the regulation of intra- and extracellular water balance, the preservation of erythrocyte morphology and membrane integrity, and the maintenance of normal organ function17,18. Previous studies had established that aberrant SOSM was associated with an elevated risk of mortality across diverse patient populations, including those with cardiovascular disease, critical illness, and septic shock. Perturbations in SOSM exhibited a non-linear correlation with both all-cause and cardiovascular mortality, with the lowest risk observed at approximately 278 mmol/L19. Elevated SOSM has further been implicated in increased mortality related to disorders of the cardiovascular, neurological, vascular, and gastrointestinal systems20. In septic shock, dysregulated SOSM is strongly associated with 28-day mortality, with survival markedly higher among patients maintaining normal osmolality compared with those in the hypo- or hyperosmolar ranges21. Our findings align with these prior observations: elevated SOSM was independently associated with greater 28-day mortality in patients with SAD, with a near-linear relationship evident between rising osmolality and short-term mortality risk. Recently, the prognostic significance of SOSM in encephalopathy has also garnered increasing attention. In a cohort of 141 patients with traumatic brain injury, Ziaei et al. reported that non-survivors exhibited significantly higher SOSM levels than survivors, with an optimal cutoff of 298.90 mmol/L22. Similarly, Fang et al. identified a U-shaped association between SOSM and the risk of SAD, whereby patients in both hypo- and hyperosmolar groups demonstrated higher rates of delirium compared with those within the intermediate range (286–301 mmol/L)23. Collectively, our study adds new evidence supporting the clinical utility of SOSM as a prognostic biomarker in encephalopathy. Notably, SOSM represents a composite index determined by sodium, glucose, and BUN levels. Accordingly, perturbations in these biochemical parameters directly precipitate abnormalities in osmolality. Prior work had demonstrated that derangements in sodium, glucose, and BUN levels during sepsis are each independently associated with mortality risk24,25,26,27. Thus, as an integrative measure, SOSM may serve as a sensitive marker reflecting concurrent shifts in multiple metabolic substrates. A more comprehensive elucidation of the mechanistic pathways underlying these alterations could offer enhanced clinical insight.
In addition to examining the association between baseline SOSM levels and 28-day mortality in patients SAD, we further employed longitudinal analyses to further investigate the impact of SOSM trajectories on the 28-day mortality risk. Based on the SOSM change trajectories after admission to the ICU, patients were stratified into four trajectory groups. Only trajectory 1 exhibited a stable course within the normal range, whereas trajectories 2–4 began within the reference range but diverged subsequently. Importantly, If only the single time point of admission to the ICU was considered, the normal starting points of the 4 types of trajectories did not increase the short-term mortality risk of SAD patients. However, the SOSM after admission to the ICU showed different trajectory change patterns. The results of longitudinal trajectory analysis indicated that compared with the normal and stable trajectory 1, the fluctuation of SOSM trajectory after admission to the ICU was associated with the 28-day mortality of SAD patients. Moreover, trajectory 4 had returned to the normal SOSM range within the observed period, but still remained associated with an increased short-term mortality risk of SAD patients. It is speculated that the progression and death risk of SAD and related encephalopathy are sensitive to the changes of SOSM and have relatively irreversible manifestations. It is necessary to monitor the trajectory of SOSM in patients with SAD within the first 6 days of ICU admission, which may provide a basis for judging the short-term mortality risk of SAD patients. Clinicians should take active intervention measures when SOSM exceeds the risk threshold or when SOSM fluctuates. These interventions may include closer monitoring and timely medication or symptomatic treatment to reduce the risk of death and improve the prognosis of patients with SAD.
Although the mechanisms linking SOSM to mortality in patients with SAD remain incompletely understood, recent evidence offers important insights. Abnormal osmolality has been closely associated with organ dysfunction, particularly acute kidney injury and impaired pulmonary function. The kidney, highly vulnerable to osmotic stress, plays a central role in maintaining osmotic balance. Experimental studies have shown that hyperosmolality injures renal tubular epithelial cells by inducing oxidative stress and cytoskeletal disruption, thereby contributing to kidney injury28. Similarly, hyperosmotic states elevate intracellular Ca2⁺ and reactive oxygen species (ROS), which in turn trigger endoplasmic reticulum stress and cardiomyocyte apoptosis29,30. Such damage to vital organs may accelerate the development of multiple organ dysfunction syndrome (MODS) and heighten mortality in SAD. Beyond peripheral organ injury, several mechanisms directly implicate abnormal SOSM in SAD pathogenesis. The release of inflammatory cytokines, disruption of the blood–brain barrier, ischemic insults, neurotransmitter dysregulation, and mitochondrial dysfunction have all been linked to delirium31. Elevated SOSM has been shown to impair blood–brain barrier integrity32, while simultaneously modulating neutrophil activity and amplifying the release of pro-inflammatory mediators, including leukotrienes, TNF-α, and IL-633,34. These cytokines, once permitted entry into the central nervous system through a compromised barrier, may further drive the onset and progression of SAD. In addition, serum hypertonicity promotes osmotic shifts that dehydrate cells and cause cellular atrophy35. These morphological alterations, which compromise mitochondria, nuclei, and energy metabolism, ultimately predispose cells to irreversible injury and death36.
This study demonstrates that SOSM trajectories are strongly associated with 28-day mortality, providing a novel basis for risk stratification and early prognostication in patients with SAD. Dynamic monitoring of SOSM and identification of high-risk trajectories may offer opportunities to optimize clinical management and improve outcomes. Nevertheless, several limitations warrant consideration. First, the retrospective design precludes causal inference. Although subgroup analyses and multivariable adjustments were employed to enhance robustness, residual confounding from unmeasured variables cannot be excluded. Second, most patients in this cohort experienced mechanical ventilation and AKI. To avoid potential model overfitting, we did not conduct separate subgroup analyses for these populations. Third, as a single-center study based on the MIMIC-IV database, the cohort was predominantly White and derived exclusively from ICU patients, which may limit the generalizability of our findings to other populations and healthcare settings. Prospective multicenter validation is therefore required. Finally, given the clinical nature of this study, mechanistic insights remain speculative, and further basic and translational research will be essential to elucidate the underlying pathways.
Conclusion
SOSM was an independent risk factor for 28-day mortality in patients with SAD. Persistent elevation and fluctuation of SOSM trajectories after ICU admission were associated with increased 28-day mortality in patients with SAD.
Data availability
The datasets generated and/or analyzed during the current study are available in the MIMIC-IV database, https://mimic.mit.edu/docs/iv/. Upon reasonable request, the corresponding author can provide all detailed information on statistical analysis code and structured data.
Abbreviations
- ICU:
-
Intensive care unit
- SAE:
-
Sepsis-associated encephalopathy
- SAD:
-
Sepsis-associated delirium
- SOSM:
-
Serum osmolality
- LCTM:
-
Latent Class Trajectory Modeling
- MIMIC-IV:
-
Medical Information Mart for Intensive Care IV
- SOFA:
-
Sequential Organ Failure Assessment
- CAM-ICU:
-
Confusion Assessment Method for the Intensive Care Unit
- MAP:
-
Mean arterial pressure
- BUN:
-
Blood urea nitrogen
- WBC:
-
White blood cell
- APTT:
-
Activated partial thromboplastin time
- PT:
-
Prothrombin time
- INR:
-
International normalized ratio
- ALT:
-
Aminotransferase
- AST:
-
Aspartate aminotransferase
- PO2 :
-
Arterial oxygen partial pressure
- PCO2:
-
Arterial carbon dioxide partial pressure
- CCI:
-
Charlson comorbidity index
- GCS:
-
Glasgow Coma Scale
- APS III:
-
Acute physiology score III
- IQR:
-
Interquartile range
- CRRT:
-
Continuous renal replacement therapy
- AIC:
-
Akaike Information Criterion
- BIC:
-
Bayesian Information Criterion
- AvePP:
-
Average posterior probability
- HR:
-
Hazard ratio
- 95% CI:
-
95% Confidence interval
- RCS:
-
Restricted cubic spline
- VIF:
-
Variance Inflation Factor
- AKI:
-
Acute kidney injury
- MODS:
-
Multiple organ dysfunction syndrome
References
Singer, M. et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315(8), 801–810 (2016).
Hong, Y. et al. Sepsis-associated encephalopathy: From pathophysiology to clinical management. Int Immunopharmacol. 124(Pt A), 110800 (2023).
Fang, Y. et al. Association of triglyceride-glucose index and delirium in patients with sepsis: A retrospective study. Lipids Health Dis. 23(1), 227 (2024).
Büyükkaragöz, B. & Bakkaloğlu, S. A. Serum osmolality and hyperosmolar states. Pediatr. Nephrol. 38, 1013–1025 (2023).
Verbalis, J. G. Disorders of body water homeostasis. Best Pract. Res. Clin. Endocrinol. Metab. 17(4), 471–503 (2003).
Palmer, L. G. & Schnermann, J. Integrated control of Na transport along the nephron. Clin. J. Am. Soc. Nephrol. 10(4), 676–687 (2015).
Zou, Q. et al. Association between serum osmolality and 28-day all-cause mortality in patients with heart failure and reduced ejection fraction: A retrospective cohort study from the MIMIC-IV database. Front. Endocrinol. (Lausanne). 15, 1397329 (2024).
Liang, M. et al. The U-shaped association between serum osmolality and 28-day mortality in patients with sepsis: A retrospective cohort study. Infection 52(5), 1931–1939 (2024).
Chen, X. H. et al. The U-shaped relationship between serum osmolality and in-hospital mortality in patients with traumatic brain injury: A retrospective study based on the MIMIC-IV database. Eur. J. Med. Res. 30(1), 126 (2025).
Gui, L. et al. The J-shaped relationship between serum osmolality and all-cause mortality in critically ill patients with myocardial infarction: A retrospective cohort study. Front. Endocrinol. (Lausanne). 16, 1542403 (2025).
Nguena Nguefack, H. L. et al. Trajectory modelling techniques useful to epidemiological research: A comparative narrative review of approaches. Clin. Epidemiol. 12, 1205–1222 (2020).
Johnson, A. E. W. et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci. Data. 10(1), 1 (2023).
Shi, Q., Warren, L., Saposnik, G. & Macdermid, J. C. Confusion assessment method: A systematic review and meta-analysis of diagnostic accuracy. Neuropsychiatr. Dis. Treat. 9, 1359–1370 (2013).
Kanbay, M. et al. Serum osmolarity as a potential predictor for contrast-induced nephropathy following elective coronary angiography. Int. Urol. Nephrol. 52(3), 541–547 (2020).
Danziger, J. & Zeidel, M. L. Osmotic homeostasis. Clin. J. Am. Soc. Nephrol. 10(5), 852–862 (2015).
Vrieze, S. I. Model selection and psychological theory: A discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychol. Methods 17(2), 228 (2012).
Guzik, M. et al. Serum osmolarity and vasopressin concentration in acute heart failure-influence on clinical course and outcome. Biomedicines. 10(8), 2034 (2022).
Argyropoulos, C. et al. Hypertonicity: Pathophysiologic concept and experimental studies. Cureus. 8(5), e596 (2016).
Wang, S. et al. Association of serum osmolality with all-cause and cardiovascular mortality in US adults: A prospective cohort study. Nutr. Metab. Cardiovasc. Dis. 33(4), 844–852 (2023).
Shen, Y. et al. Association between serum osmolarity and mortality in patients who are critically ill: A retrospective cohort study. BMJ Open 7(5), e015729 (2017).
Heng, G. et al. Increased ICU mortality in septic shock patients with hypo- or hyper- serum osmolarity: A retrospective study. Front. Med. (Lausanne). 10, 1083769 (2023).
Ziaei, M. et al. The level of serum osmolarity at admission in prognosis of nosocomial mortality in patients with severe brain trauma. Adv. Biomed. Res. 12, 40 (2023).
Fang, Y., Xie, H., Dou, A., Cui, Y. & Xie, K. The U-shaped relationship between serum osmolality and the risk of sepsis-associated delirium development: A retrospective study. BMC Neurol. 25(1), 246 (2025).
Li, Y., Li, W. & Xu, B. Between blood glucose and mortality in critically ill patients: Retrospective analysis of the MIMIC-IV database. J. Diabetes Investig. 15(7), 931–938 (2024).
O’Sullivan, M. & McCarthy, K. F. Sodium: Sign, signifier, or signified, of sepsis?. Eur. J. Intern. Med. 83, 10–11 (2021).
Sordi, R., Fernandes, D., Heckert, B. T. & Assreuy, J. Early potassium channel blockade improves sepsis-induced organ damage and cardiovascular dysfunction. Br. J. Pharmacol. 163(6), 1289–1301 (2011).
Harazim, M., Tan, K., Nalos, M. & Matejovic, M. Blood urea nitrogen—Independent marker of mortality in sepsis. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 167(1), 24–29 (2023).
Shi, J. et al. Renal tubular epithelial cells injury induced by mannitol and its potential mechanism. Ren. Fail. 40(1), 85–91 (2018).
Burgos, J. I. et al. Hyperosmotic stress promotes endoplasmic reticulum stress-dependent apoptosis in adult rat cardiac myocytes. Apoptosis 24(9–10), 785–797 (2019).
Ricardo, R. A., Bassani, R. A. & Bassani, J. W. Osmolality- and Na+-dependent effects of hyperosmotic NaCl solution on contractile activity and Ca2+ cycling in rat ventricular myocytes. Pflugers Arch. 455(4), 617–626 (2008).
Hu, W. et al. Exploring and validating the mechanism of ulinastatin in the treatment of sepsis-associated encephalopathy based on transcriptome sequencing. J. Inflamm. Res. 17, 8753–8773 (2024).
Huang, K. et al. Imaging effects of hyperosmolality on individual tricellular junctions. Chem. Sci. 11(5), 1307–1315 (2019).
Burks, S. R. et al. Blood-brain barrier opening by intracarotid artery hyperosmolar mannitol induces sterile inflammatory and innate immune responses. Proc. Natl. Acad. Sci. USA 118(18), e2021915118 (2021).
Schwartz, L. et al. Is inflammation a consequence of extracellular hyperosmolarity?. J. Inflamm. (Lond.). 6, 21 (2009).
Burg, M. B., Ferraris, J. D. & Dmitrieva, N. I. Cellular response to hyperosmotic stresses. Physiol. Rev. 87(4), 1441–1474 (2007).
Dmitrieva, N. I., Boehm, M., Yancey, P. H. & Enhörning, S. Long-term health outcomes associated with hydration status. Nat. Rev. Nephrol. 20(5), 275–294 (2024).
Funding
This work was supported by the National Nature Science Foundation of China Grants (82260371), Yunnan health training project of high level talents (L-2024008), and Yunnan Revitalization Talent Support Program.
Author information
Authors and Affiliations
Contributions
Youhui Zhao was instrumental in collecting and analyzing data, as well as drafting the manuscript. Hong Zhu were pivotal in data extraction and played a significant role in the study’s design. Jun Ding, Jin Chen, Weiyan Gong, and Shujuan Mi revised the manuscript for intellectual content. Kun Yang who oversaw the entire project, contributed by reviewing and designing the study, in addition to providing supervision. Youhui Zhao and Hong Zhu contributed equally to this work. All authors actively participated in the development of the article and gave their approval for the final version to be submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study used public de-identification databases, so there is no need to obtain the informed consent and approval of the Institutional Review Board. After completing the Collaborative Institutional Training Initiative programme, we got permission to access the database.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhao, Y., Zhu, H., Ding, J. et al. Trajectory of serum osmolality changes and 28-day mortality risk in patients with sepsis-associated delirium based on the MIMIC-IV database. Sci Rep 16, 2261 (2026). https://doi.org/10.1038/s41598-025-32057-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-32057-z
