
Abstract
Antimicrobial resistance (AMR) is a global health challenge, with carbapenemase-producing organisms (CPOs) posing a significant concern in British Columbia, Canada. Traditional surveillance focuses on hospital-associated data, overlooking community-level trends. Monitoring carbapenemase genes in communities can provide early insights into resistance trends and support antimicrobial stewardship efforts. This study employs wastewater surveillance to track antimicrobial resistance genes (ARGs) at the community level. Four ARGs, blaNDM, blaKPC, blaOXA−48, and mcr-1, were detected and quantified in wastewater samples from five treatment plants across British Columbia. The results revealed year-round ARG presence in wastewater, with blaOXA−48 being the most prevalent, followed by blaNDM, blaKPC, and mcr-1. Seasonal fluctuations were observed, with most ARGs peaking in the winter and spring, a trend not reflected in clinical data. Notably, mcr-1 was detected in wastewater despite its limited clinical presence. These results highlight the value of integrating wastewater surveillance with traditional methods to enhance AMR monitoring.
Similar content being viewed by others

Introduction
Antimicrobial resistance (AMR) is an urgent public health issue. Currently, across the globe, 700,000 deaths are attributed to drug-resistant infections each year1. Among the most concerning AMR pathogens are carbapenemase-producing organisms (CPOs). CPOs refer to a group of bacteria that confer resistance to broad-spectrum carbapenem antimicrobials, due to the production of hydrolyzing enzymes called carbapenemases. Since carbapenems are considered last resort antibiotics, infections caused by CPOs are often complicated to treat, resulting in long hospital stays and poor outcomes2. Over the past two decades, the spread of CPOs has escalated into a global public health emergency, prompting the World Health Organization to declare CPOs one of the critical priority pathogens3. Importantly, even countries with historically low CPO prevalence, such as Canada, have observed a rise in colonization and infection rates4,5. Among the most prevalent and well-described carbapenemases on the rise both globally and in Canada are Klebsiella pneumoniae carbapenemase (KPC), New Delhi metallo-β-lactamase (NDM) and Oxacillinase 48 (OXA-48)4,6,7.
Currently, polymyxins, such as colistin, are increasingly being used to treat infections caused by CPOs8. Recently, however, concerns have emerged over the detection of the plasmid-borne mobilized colistin resistance (mcr-1) gene in China9, which has since been reported worldwide10. Of particular concern is the dissemination of mcr-1 to CPOs and other bacterial species, giving rise to multidrug-resistant “superbugs” that are potentially untreatable11,12. Alarmingly, several reports have surfaced describing the emergence of co-resistant isolates13,14,15,16,17,18, prompting the implementation of various surveillance strategies.
CPO surveillance programs play a pivotal role in the ongoing battle against antimicrobial resistance. Notably, in British Columbia (BC), Canada, in the wake of a hospital outbreak in 2014, the province launched a CPO surveillance program targeting acute care facilities19. This initiative was the result of a collaborative endeavor uniting frontline microbiology laboratories, the BC Centre for Disease Control Public Health Laboratory (BCCDC PHL), and the Provincial Infection Control Network of BC (PICNet). The program’s primary objective was to strengthen CPO prevention and control practices through the implementation of a comprehensive provincial surveillance protocol for collecting patient CPO data. Under the surveillance protocol, mandatory testing is routinely conducted for patients exhibiting potential risk factors contributing to CPO acquisition20. These risk factors include individuals who received healthcare outside Canada (i.e., overnight hospital stays and medical/surgical procedures), those who have traveled to an endemic region, and those who had close contact with either a CPO patient or their immediate surroundings20. Following routine screening from the frontline labs, positive samples are forwarded to the BCCDC PHL for further confirmation and CPO characterization. This involves molecular screening for various antibiotic resistance genes (ARGs) including blaNDM, blaKPC, blaOXA−48 and mcr-1.
While the collected data from frontline labs, BCCDC PHL and PICNet form the knowledge basis for BC’s provincial CPO surveillance program, relying predominantly on hospital-associated data may lead to sampling bias and underreporting of community-linked cases21,22. Unfortunately, however, the considerable expenses involved in conducting culture and molecular screening within the public domain have significantly limited our understanding of large-scale community-level epidemiology of these organisms. Despite these limitations, concerns have risen in recent years due to the establishment of CPOs within community settings, with some regions reporting endemic levels2,4,23.
The expansion of wastewater-based epidemiology has provided a unique opportunity to address gaps in community surveillance and broaden the understanding of AMR within local communities. While the concept is not new24, wastewater testing recently resurfaced as a timely, cost-effective, and scalable approach to community surveillance during the COVID-19 pandemic25,26,27. In the context of AMR, few wastewater studies exist28. Among these, most investigations have been conducted in Europe and Asia, with limited work emerging from North America29,30,31,32,33. Existing North American wastewater studies have primarily focused on related aspects of AMR—such as associations with antibiotic consumption34, detection of carbapenem resistance genes35,36 and resistome characterization37 —rather than on temporal dynamics for the use of community surveillance purposes. Nevertheless, wastewater surveillance (WWS) offers a powerful tool for tracking AMR and can provide a valuable complement to traditional clinical monitoring. By capturing the collective microbial signal from entire communities in wastewater, WWS can reveal the population-level prevalence of resistance genes, including those from asymptomatic individuals or groups underrepresented in clinical datasets38,39,40,41. WWS also enables detection of temporal patterns and seasonality in ARG loads, offering early warning of emerging resistance42,43. In addition, WWS can be applied to assess discharges and effluents from hospitals and wastewater treatment plants, providing insight into treatment efficacy, potential ARG release into the environment, and early detection of hospital-associated outbreaks44,45,46,47,48,49. Importantly, WWS supports the One Health framework by capturing ARGs that enter wastewater systems via human, animal, and environmental runoff28,33. However, it does not capture all ARGs present in the broader environment, including those in soil, surface water, wildlife, or livestock.
In this study, we adapted an existing clinical assay to detect carbapenemase genes—blaNDM, blaKPC, blaOXA−48—and mcr-1, providing the first insight into baseline CPO and colistin-resistance levels in wastewater from urban centres in BC. By combining wastewater with clinical surveillance data from the same time and region, we obtain a more comprehensive view of CPO levels in both healthcare and community settings, enhancing our understanding of the prevalence of these resistance determinants.
Methods and materials
Sample collection and concentration
Between January and December 2022, 310 wastewater samples were collected on 62 dates from five treatment plants (Sites A-E) in British Columbia, Canada. The five wastewater treatment plants (WWTPs) collectively serve approximately 2.4 million people—about 42% of British Columbia’s population—across nine major cities in the Lower Mainland region.
These WWTPs primarily serve urban and/or suburban regions, characterized by high population density and diverse land uses. Several zones include critical public health infrastructure, such as clusters of hospitals, long-term care facilities, and areas with high travel activity due to their proximity to a major international airport and key transportation corridors.
In addition to residential sources (e.g., toilets, sinks, and showers), the wastewater entering these facilities includes inputs from commercial, institutional, and industrial operations, along with stormwater runoff and snowmelt. This complex mixture captures a broad spectrum of community-level activities, making these WWTPs particularly well-suited for public health surveillance.
For each wastewater sample, coarsely screened influent wastewater was collected over a 24-hour period using an auto-sampling device. One litre of the composite influent wastewater sample was then refrigerated and shipped to the BCCDC within 24 h of the end of collection. Upon receipt in the lab, the 1 L influent sample was homogenized by shaking and a 15 mL aliquot was centrifuged at 4200 × g for 20 min at 4 °C. The supernatant was transferred to an Amicon Ultra-15 Centrifugal Filter Unit (10 kDa cutoff; Millipore Sigma, UFC901096) and centrifuged at 4200 × g for 35 min to retain viral particles and large nucleic acid fragments while removing smaller impurities, resulting in a wastewater concentrate. A total of 200 µL of concentrate was frozen and stored at -20 °C prior to nucleic acid extraction.
DNA extraction
Nucleic acids from wastewater concentrates were extracted using the bioMerieux NucliSENS easyMAG by adding 200 µL of wastewater concentrate into 2 mL of bioMerieux NucliSENS easyMAG lysis buffer. Negative extraction controls were prepared similarly, using 200 µL of DEPC water instead of concentrate. Samples and controls were incubated in the lysis buffer for a minimum of ten minutes at room temperature. A 1:1 mixture of magnetic silica beads (Biomerieux) and DEPC water was prepared, and 100 µL of the mixture was added to each sample in lysis buffer. The samples and controls were mixed by pipetting and subsequently transferred to an easyMAG sample cartridge for extraction. Following extraction, the eluates were stored at 4 °C for up to 24 h or -80 °C for long-term storage.
Multiplex quantitative polymerase chain reaction (qPCR)
Eluates were tested for blaNDM, blaKPC, blaOXA−48, and mcr-1 using a multiplex qPCR assay. Each sample was tested by mixing 2 µL of eluate with 10 µL of 2 × Fast Advanced Mastermix (ThermoScientific), 7 µL ddH2O and 1 µL 20 × CPO primer/probe mix for blaOXA− 48, blaKPC and blaNDM as previously described50. In addition, mcr-1 primers and probes were incorporated into the 20 × CPO primer/probe mix, with primers at a final concentration of 200 nM and probes at 150 nM51. Negative (DEPC water) and positive controls (synthetic double stranded DNA for each target – Table S1) were used in each experiment. The PCR cycling conditions were as follows: 50 °C for 2 min, 95 °C for 20 s, then 45 cycles of 95 °C for 3 s, and 60 °C for 30 s. qPCR was run on an Applied Biosystems™ 7500 Fast Real-Time PCR system. Each wastewater sample was run in triplicate, and if two or more replicates had undetermined results, they were excluded from the analysis. Furthermore, external standard curves were established to measure the concentration of each target within wastewater as well as determine the lower limit of detection (LLoD). Using the synthetic dsDNA targets outlined in Table S1, six serial dilutions ranging from 1 × 105 copies/µl to 1 copy/µl were tested in 30 replicates. Following the MIQE guidelines, the LLoD was defined, based on the established standard curve, as the estimated concentration at which ≥ 95% of replicates were detected52.
Data analysis
To control for variation in overall wastewater input, wastewater data was normalized using the flow rate (in million litres/day) obtained from the treatment plant. AMR daily load (expressed as copies/day) was calculated by multiplying the target concentration (DNA copies/L) by the flow rate (L/day).
Data between early and mid-October (epidemiological weeks 40–41) were omitted due to an insufficient volume of wastewater concentrates during this time. When aggregating daily load from all plants, a WWTP weighted sum method was applied to account for different populations served. For this method, a “WWTP weight” was first calculated for each individual site. The WWTP weight was derived by dividing the number of people served by an individual WWTP by the total number of people served by all WWTPs combined (Sites A-E). Subsequently, the daily load of each site was multiplied by its corresponding WWTP weight factor, before summing the daily weighted loads of all sites to obtain the aggregated load.
Data were analyzed and visualized using R and RStudio (version 4.1.2). Trend lines were generated using the Locally Estimated Scatterplot Smoothing (LOESS) method, which is a non-parametric regression technique to investigate longitudinal trends. This method was implemented using the stat_smooth() function from the ggplot R package (version 3.5.0).
Clinical surveillance
As previously described, under the province’s surveillance protocol, mandatory testing is routinely conducted for patients exhibiting potential risk factors contributing to CPO acquisition19. Initial testing is carried out in frontline labs, with positive samples subsequently forwarded to the BCCDC PHL for molecular confirmation. For this study, the BCCDC PHL provided clinical counts of PCR-positive samples for blaNDM, blaKPC, blaOXA−48 and mcr-1 from two health authorities (HA1 and HA2), corresponding to the wastewater catchment areas of Sites A-E. These data span the period from January to December 2022.
In addition, for this study, a specific case definition was used: individuals previously identified as colonized or infected with a CPO who undergo retesting on subsequent days and are found to still harbour the same gene, are considered distinct occurrences, thus classified as new cases. This approach was adopted to ensure the inclusion of retested patients who might exhibit heightened symptoms during flare-ups, potentially resulting in increased shedding in wastewater. Such cases might be missed by conventional provincial surveillance methods20, that typically count carriers once.
Statistical analysis
To assess seasonal variation in ARGs, samples were grouped by meteorological season based on collection date: Winter (December–February), Spring (March–May), Summer (June–August), and Fall (September–November). A non-parametric Kruskal–Wallis test was used to assess overall differences in ARGs, measured in copies per day, across seasons. Dunn’s post-hoc testing was then applied to identify which specific seasons differed significantly from one another. Statistical significance was denoted as follows: *p < 0.05; **p < 0.01; ***p < 0.001.
In addition, Kendall’s correlation and Kendall’s Tau statistic were used to assess the degree of correlation between total monthly ARG loads in wastewater and total monthly clinical case counts.
Results
Summary of wastewater trends
Prior to testing wastewater samples, a multiplex qPCR assay, which was first developed at the BCCDC PHL for clinical testing50, was adapted for use on wastewater samples. To ensure the assay’s suitability for environmental samples which may contain multiple ARGs, wastewater samples were spiked with all four targets and tested under both singleplex and tetraplex conditions. No discernible differences in cycle threshold (Ct) were noted between both singleplex and multiplex conditions, confirming all ARGs could be simultaneously detected in wastewater (data not shown). The lower limit of detection (LLoD) was interpolated using external standard curves and represented in Table S2.
Overall, blaNDM, blaKPC, blaOXA−48 and mcr-1 were detected in 82% of total samples (1013/1240). Of these, 37% (379/1013) of measurements fell below the established LLoD (Table S2) determined using MIQE guidelines, which are primarily designed for clinical assays requiring high diagnostic confidence and a 95% detection threshold52. Environmental matrices such as wastewater are complex, often contain PCR inhibitors, and frequently contain low-abundance targets; applying a conservative clinical-style LLoD would exclude many measurements that might provide meaningful information for surveillance and early-warning applications—a key advantage of wastewater monitoring. Accordingly, below-LLoD values were retained in the analysis, with emphasis on assessing overall temporal trends rather than interpreting absolute concentrations.
To understand the trend of ARG levels overall across all tested sites, daily loads were aggregated for all five WWTPs for each specific ARG using a weighted sum method. Generally, all four targets were detected consistently year-round (Fig. 1b-d). Among these, blaOXA−48 was detected at higher levels as compared to other targets, followed by blaNDM, blaKPC and mcr-1 (Fig. 1a).
Seasonal differences were examined by grouping population-weighted gene loads into meteorological seasons, with Kruskal–Wallis tests and Dunn’s post-hoc pairwise comparisons summarized in Table S3. Across the year, blaOXA−48 levels peaked in February and gradually declined through mid-September (Fig. 1b), with slightly higher loads in winter and spring compared to fall, though these differences were not statistically significant (all Dunn’s p > 0.5; Fig. 1f). In contrast, blaNDM levels displayed a pronounced increase over the winter and spring months, peaking in March (Fig. 1c), with post-hoc comparisons confirming significantly higher levels in winter and spring relative to fall (Dunn’s p < 0.05; Fig. 1g). blaKPC followed a different pattern, with levels peaking during the summer months (Fig. 1d/h), and was significantly elevated in both spring and summer relative to fall (Dunn’s p < 0.05; Fig. 1h). Finally, mcr-1 followed a similar trend to blaOXA−48 and blaNDM, with an early-year increase around February and a steady decline thereafter (Fig. 1e), but no significant seasonal differences were detected (all Dunn’s p > 0.05; Fig. 1i).
CPO clinical surveillance
In combination with the wastewater data, positive clinical case counts for patients in HA1 and HA2 tested between January and December 2022 were obtained. Across this period, 314 positive cases were identified, each instance corresponding to a distinct ARG detected within a patient isolate. An overview of the case data is presented in Fig. 2. Notably, blaNDM emerged as the dominant ARG, accounting for 55.7% of all cases (175/314), followed by blaKPC (71/314; 22.6%), blaOXA−48 (67/314; 21.3%), and mcr-1 (1/314; 0.3%) (Fig. 2a). As a result of the relatively small number of cases when stratified by gene type, case counts for all tested ARGs were aggregated by month and shown in Fig. 2b. Interestingly, there was an uptick of AMR cases in October that was not reflected in the wastewater data. When further examining the relationship between total monthly clinical case counts and total monthly ARG wastewater load, no correlation was found (Kendall’s tau value = 0.0923) (Figure S1).

Wastewater ARG trends during 2022. (a) Proportion of ARGs detected in wastewater, combined across all five WWTPs. The annual total concentration of each target gene was summed across treatment plants and expressed as a percentage. (b–e) Longitudinal trends in wastewater for (b) blaOXA−48, (c) blaNDM, (d) blaKPC and (e) mcr-1 throughout 2022 in BC. LOESS regression lines (blue) and 95% confidence intervals (grey) are shown. Background shading indicates seasons: blue (Winter), green (Spring), yellow (Summer), and orange (Fall). (f–i) Seasonal variation in ARG levels for (f) blaOXA−48, (g) blaNDM, (h) blaKPC and (i) mcr-1. Seasonal differences were assessed using the Kruskal-Wallis test with Dunn’s post-hoc pairwise comparisons. Significance is denoted as follows: * p < 0.05; ** p < 0.01; *** p < 0.001. Error bars represent the standard error of the mean (SEM).

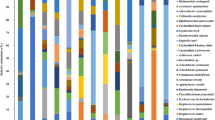
Summary of clinical data obtained from patients in Health authority 1 and 2 (HA1 and HA2) in 2022. (a) Percentage of cases by ARG (b) Total monthly case counts stratified by ARG. Background shading indicates seasons: blue (Winter), green (Spring), yellow (Summer), and orange (Fall). (c) Percentage of cases by organism (d) ARG association with organism.
Across the study period, more than half of the recovered isolates were E. coli (166/314, 52.9%), followed by Klebsiella spp. (78/314, 24.8%) and Citrobacter spp. (44/314, 14.0%) (Fig. 2c). Furthermore, the distribution of carbapenemase enzymes varied with bacterial species. Specifically, blaNDM was most often associated with E. coli while blaKPC was most commonly detected in Klebsiella and Citrobacter spp. isolates (Fig. 2d).
Of particular concern are isolates that harbour multiple carbapenemase genes, as they pose significant challenges in clinical management and may act as a reservoir of carbapenemase genes for other bacterial pathogens53. In this study, co-carriage—defined as the detection of more than one ARG within the same sample—was relatively uncommon, occurring in a small subset of patients (n = 41) (Table S4). In individuals with multiple ARGs identified, typically blaNDM and blaOXA−48 were more commonly detected together (Table S4). Interestingly, the single occurrence of mcr-1 that was identified in E. coli, was also associated with blaNDM co-carriage (Table S4). Lastly, it was of interest to determine whether samples collected reflected infection or colonization cases. Notably, the majority of cases (65%; 203/314) were collected as a screening isolate (rectal swabs or stool samples collected in the absence of clinical symptoms) while 34% (108/314) of cases were collected as clinical isolates (collected from wound, blood, urine, surgical sites) (Figure S2a). Given that screening cases are normally collected as rectal swabs or stool samples, we sought to identify if there was a stronger correlation between these monthly case counts and wastewater. Correlational analysis by Kendall’s Tau did not reveal a stronger correlation (Figure S2b).
Discussion
Wastewater surveillance can capture the community-level abundance of ARGs, provide insight into asymptomatic caseloads and help inform public health interventions and policies54. Importantly, as isolates with different carbapenemases display different resistances, measuring CPO abundance in a community can help monitor the temporal and spatial changes in the quantity of targeted resistance genes, and capture emerging regional trends before they can be detected at the local healthcare facility level. This study employed a multiplex molecular assay to simultaneously detect the presence of three distinct CPO targets and mcr-1 in wastewater between January and December 2022 across the Lower Mainland, a region comprising British Columbia’s most densely populated municipalities. An additional objective of this study was to compare the wastewater data with clinical data collected during the same time period and geographic region.
Overall, when aggregating data from five WWTPs, the tested ARGs were consistently detected year-round in BC wastewater. A significant finding from this study revealed that levels of blaOXA−48, blaNDM and mcr-1 exhibited similar seasonal trends, peaking during the winter and spring months and gradually decreasing by the summer. On the other hand, less prevalent blaKPC levels peaked in the summer and gradually decreased by the fall. Interestingly, previous clinical studies have reported higher AMR in the winter and spring months, often attributed to increased antibiotic prescription rates and consumption48,55,56,57,58. Similarly, in biosolids, a higher degree of horizontal gene transfer of antibiotic resistance genes was reported during the winter months59. This phenomenon was attributed to the cold stress response which increases the competence and transformation capability of bacterial cells59. Furthermore, similar to our study, earlier wastewater studies in Germany reported higher levels of beta-lactamases and mcr genes in the winter months32. Collectively, these observations highlight the influence of seasonal factors on ARG dissemination both within communities and wastewater systems.
Since the inception of the mandatory provincial CPO surveillance program to BC acute care facilities in 2014, CPO cases have steadily increased from 2014 to 2018, with blaNDM being the predominant carbapenemase-encoding gene detected in each year of testing2,19. This trend continued to be seen for the duration of our study period. Co-resistance was found in a small subset of patients and most commonly linked to acquisition of both blaNDM and blaOXA−48 genes. Certainly, co-resistance with this combination of carbapenemases is not uncommon and has been documented across numerous studies53,60,61,62, with cases expanding globally53. When examining trends between clinical and wastewater datasets, it was interesting to see differences in the observed ARG abundance profiles. Notably, blaOXA−48 dominated in wastewater samples, followed by blaNDM, blaKPC and mcr-1. Interestingly, OXA-48 has been shown to be abundant outside hospital settings, expanding into reservoirs within environmental, agricultural and veterinary sectors63. Likewise, in previous wastewater studies, OXA-like enzymes have shown to be the most frequently recovered beta lactamases32. In the clinical context, the widespread increase in prevalence and dissemination of OXA-48 producing isolates has been described numerous times64,65. Notably, OXA-48 enzymes possess limited hydrolytic activity towards carbapenems compared to other CPOs and can therefore be more difficult to detect when not co-expressed with other resistance mechanisms65,66. Because of this, OXA-48 has been coined a “silent spreader” and can be more difficult to detect and potentially underreported by clinical testing6,65.
When comparing seasonality between wastewater and clinical datasets, there was no correlation. However, this divergence was not entirely unexpected. Firstly, wastewater samples are a blend of human, animal and environmental contributions representing the cumulative presence of a target that is detectable over time. In contrast, clinical specimens represent singular, isolated events and data is susceptible to biases stemming from sampling methodologies dictated by surveillance protocols28. For example, the predominance of blaNDM in clinical samples may be influenced by sampling methods that favour patients with recent hospital exposures or travel to regions where NDM is endemic23. Furthermore, wastewater is a complex matrix containing a mixture of extracellular, intracellular, and fragmented DNA from a broad range of organisms—both viable and non-viable, and not necessarily of human origin. In contrast, clinical ARG detection is typically performed on cultured isolates from individual patients, usually representing one or a few viable, clinically relevant organisms. Lastly, clinical datasets primarily highlight severe clinical outcomes or cases meeting specific surveillance criteria. In contrast, wastewater data offers insights at the community level, capturing a broader spectrum of the population, including both asymptomatic and symptomatic carriers shedding into the wastewater systems.
While wastewater data can provide community-level surveillance, it is important to acknowledge the limitations within wastewater testing. Firstly, our analysis focused on the wastewater liquid fraction, potentially overlooking the presence of AMR targets in the solid or sludge fractions. Indeed studies have reported different proportions of carbapenemase genes in different partitions of wastewater32, and as such, exploring various components could provide a more comprehensive understanding of ARG prevalence in wastewater. ARGs can originate from multiple sources, including humans, animals, and the environment, and are often transferred between species via mobile genetic elements. Wastewater testing therefore captures contributions from these sources while also reflecting potential amplification within biofilms in the wastewater system itself57,67. The extent to which genes spread through horizontal gene transfer in wastewater however is largely unknown57. Lastly, molecular detection of AMR targets in wastewater cannot be linked to viable bacterial load or the number of infected individuals. This underscores the importance for wastewater surveillance being accompanied by other comprehensive monitoring systems (i.e., hospitalization and mortality data), to effectively report on human AMR activity. Likewise, the relatively limited sample size of clinical data in this study demonstrates the utility of wastewater data in identifying trends that might escape detection through conventional clinical testing. For example, while there was a scant number of mcr-1 positive clinical cases (n = 1), this resistance gene was detected year-round in wastewater.
To complement wastewater-based findings, future studies should prioritize culturing from wastewater samples to determine whether detected ARGs originate from viable, potentially transmissible organisms. Plasmid analysis should also be undertaken to better understand the mechanisms and origins of ARG transmission. Sequencing can help characterize which plasmid types are carrying ARGs, which genes propagate most frequently together, and which are more persistent in wastewater systems. Furthermore, understanding the extent to which ARGs propagate and amplify within wastewater, can help distinguish AMR contributions originating from the wastewater environment itself and those arising from human shedding.
Historically, CPO-related infections have been linked with exposures in healthcare facilities and travel to endemic regions. Few studies have provided epidemiological insights on CPO levels in the community, especially in Canada. Our study revealed a consistent presence of ARGs in wastewater samples, suggesting significant colonization and/or transmission in communities not captured by current clinical surveillance programs deployed in the province.
Data availability
Wastewater datasets generated and analyzed in this study are available from the corresponding author upon reasonable request. Aggregated, anonymized clinical data are likewise available upon reasonable request.
References
World Health Organization. New Report Calls for Urgent Action to Avert Antimicrobial Resistance Crisis [Internet]. https://www.who.int/news/item/29-04-2019-new-report-calls-for-urgent-action-to-avert-antimicrobial-resistance-crisis. Accessed 24 Aug 2023.
Sekirov, I. et al. Epidemiologic and genotypic review of carbapenemase-producing organisms in British Columbia, Canada, between 2008 and 2014. J. Clin. Microbiol. 54 (2), 317–327 (2016).
World Health Organization. WHO bacterial priority pathogens list, 2024: Bacterial pathogens of public health importance to guide research, development and strategies to prevent and control antimicrobial resistance [Internet]. (2024). https://www.who.int/publications/i/item/9789240093461. Accessed 21 Sep 2024.
Government of Canada. Canadian Antimicrobial Resistance Surveillance System (CARSS) Report 2022 [Internet]. https://www.canada.ca/en/public-health/services/publications/drugs-health-products/canadian-antimicrobial-resistance-surveillance-system-report-2022.html. Accessed 18 Aug 2023.
Government of Canada. Canadian Antimicrobial Resistance Surveillance System Report 2021 [Internet]. https://www.canada.ca/en/public-health/services/publications/drugs-health-products/canadian-antimicrobial-resistance-surveillance-system-report-2021.html. Accessed 18 Aug 2023.
Nordmann, P., Naas, T. & Poirel, L. Global spread of carbapenemase-producing Enterobacteriaceae. Emerg. Infect. Dis. 17 (10), 1791–1798 (2011).
Mataseje, L. F. et al. Results from the Canadian nosocomial infection surveillance program on carbapenemase-producing Enterobacteriaceae, 2010 to 2014. Antimicrob. Agents Chemother. 60 (11), 6787–6794 (2016).
Kaye, K. S., Pogue, J. M., Tran, T. B., Nation, R. L. & Li, J. Agents of last resort: Polymyxin resistance. Infect. Dis. Clin. North. Am. 30 (2), 391–414 (2016).
Liu, Y. Y. et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: A microbiological and molecular biological study. Lancet Infect. Dis. 16 (2), 161–168 (2016).
Schwarz, S. & Johnson, A. P. Transferable resistance to colistin: A new but old threat. J. Antimicrob. Chemother. 71 (8), 2066–2070 (2016).
Mediavilla, J. R. et al. Colistin- and carbapenem-resistant Escherichia coli harboring mcr-1 and blaNDM-5, causing a complicated urinary tract infection in a patient from the United States. mBio 7 (4), e01191–e01116 (2016).
Tang, B. et al. Emergence of co-existence of mcr-1 and blaNDM-5 in Escherichia fergusonii. Int. J. Antimicrob. Agents. 61 (3), 106742 (2023).
Huang, H. et al. Colistin-resistance gene mcr in clinical carbapenem-resistant Enterobacteriaceae strains in China, 2014–2019. Emerg. Microbes Infect. 9 (1), 237–245 (2020).
Rhodes, H., Loveland, C., Van Houten, C., Hull, N. & Harrist, A. Notes from the field: Carbapenem-resistant Klebsiella pneumoniae with mcr-1 gene identified in a hospitalized patient — Wyoming, January 2019. MMWR Morb Mortal. Wkly. Rep. 69 (6), 171–172 (2020).
Du, H., Chen, L., Tang, Y. W. & Kreiswirth, B. N. Emergence of the mcr-1 colistin resistance gene in carbapenem-resistant Enterobacteriaceae. Lancet Infect. Dis. 16 (3), 287–288 (2016).
Muktan, B. et al. Plasmid mediated colistin resistant mcr-1 and co-existence of OXA-48 among Escherichia coli from clinical and poultry isolates: first report from Nepal. Gut Pathog. 12, 44 (2020).
Yao, X., Doi, Y., Zeng, L., Lv, L. & Liu, J. H. Carbapenem-resistant and colistin-resistant Escherichia coli co-producing NDM-9 and MCR-1. Lancet Infect. Dis. 16 (3), 288–289 (2016).
Tacão, M. et al. mcr-1 and blaKPC-3 in Escherichia coli sequence type 744 after meropenem and colistin Therapy, Portugal - 23, number 8—August 2017 - Emerging infectious diseases journal - CDC. Emerg. Infect. Dis. 23 (8), 1419–1421 (2017).
Provincial Infection Control Network of BC (PICNet). Carbapenemase-Producing Organisms (CPOs) | PICNet [Internet]. https://picnet.ca/surveillance/cpo/. Accessed 18 Aug 2023.
Provincial Infection Control Network of BC (PICNet). PICNet Surveillance Protocol [Internet]. https://picnet.ca/surveillance/surveillance-protocols/. Accessed 22 Aug 2023.
Mao, K. et al. The potential of wastewater-based epidemiology as surveillance and early warning of infectious disease outbreaks. Curr. Opin. Environ. Sci. Health. 17, 1–7 (2020).
Sims, N. & Kasprzyk-Hordern, B. Future perspectives of wastewater-based epidemiology: Monitoring infectious disease spread and resistance to the community level. Environ. Int. 139, 105689 (2020).
Kohler, P. P. et al. Emergence of carbapenemase-producing Enterobacteriaceae, South-Central Ontario, Canada. Emerg. Infect. Dis. 24 (9), 1674–1682 (2018).
Paul, J. R., Trask, J. D. & Gard, S. II. Poliomyelitic virus in urban sewage. J. Exp. Med. 71 (6), 765–777 (1940).
Centers for Disease Control and Prevention. Wastewater Surveillance: Progress in the United States [Internet]. https://www.cdc.gov/nwss/progress.html. Accessed 7 Sep 2023.
BC Centre for Disease Control. Wastewater Surveillance [Internet]. http://www.bccdc.ca/our-services/programs/wastewater-surveillance. Accessed 7 Sep 2023.
O’Keeffe, J. Wastewater-based epidemiology: Current uses and future opportunities as a public health surveillance tool. Environ. Health Rev. 64 (3), 44–52 (2021).
Fouz, N. et al. The contribution of wastewater to the transmission of antimicrobial resistance in the environment: Implications of mass gathering settings. Trop. Med. Infect. Dis. 5 (1), 33 (2020).
Knight, M. E. et al. National-scale antimicrobial resistance surveillance in wastewater: A comparative analysis of HT qPCR and metagenomic approaches. Water Res. 262, 121989 (2024).
Al-Mustapha, A. I. et al. Wastewater based genomic surveillance key to population level monitoring of AmpC/ESBL producing Escherichia coli. Sci. Rep. 15 (1), 7400 (2025).
Teban-Man, A. et al. Municipal wastewaters carry important carbapenemase genes independent of hospital input and can mirror clinical resistance patterns. Microbiol. Spectr. 10(2), e02711–e02721 .
Schages, L., Wichern, F., Kalscheuer, R. & Bockmühl, D. Winter is coming - Impact of temperature on the variation of beta-lactamase and mcr genes in a wastewater treatment plant. Sci. Total Environ. 712, 136499 (2020).
Punch, R. et al. The surveillance of antimicrobial resistance in wastewater from a one health perspective: A global scoping and temporal review (2014–2024). One Health. 21, 101139 (2025).
Leal, H. F. et al. Influence of antimicrobial consumption (AMC) on the detection of antimicrobial resistance genes (ARGs) in urban wastewater. Int. J. Hyg. Environ. Health. 268, 114621 (2025).
Cooper, A. et al. Detection of carbapenem-resistance genes in bacteria isolated from wastewater in Ontario. FACETS 6 (1), 569–591 (2021).
Hoelle, J. et al. Survey of US wastewater for carbapenem-resistant Enterobacteriaceae. J. Water Health. 17 (2), 219–226 (2019).
Lee, J. et al. Longitudinal monitoring of sewershed resistomes in socioeconomically diverse urban neighborhoods. Commun. Med. (Lond). 5 (1), 7 (2025).
Sims, N. et al. Antimicrobials and antimicrobial resistance genes in a one-year city metabolism longitudinal study using wastewater-based epidemiology. Environ. Pollut. 333, 122020 (2023).
Prieto Riquelme, M. V. et al. Demonstrating a comprehensive wastewater-based surveillance approach that differentiates globally sourced resistomes. Environ. Sci. Technol. 56 (21), 14982–14993 (2022).
Chau, K. K. et al. Systematic review of wastewater surveillance of antimicrobial resistance in human populations. Environ. Int. 162, 107171 (2022).
Conforti, S., Holschneider, A., Sylvestre, É. & Julian, T. R. Monitoring ESBL-Escherichia coli in Swiss wastewater between November 2021 and November 2022: Insights into population carriage. mSphere 9 (5), e0076023 (2024).
Lambrou, A. S. Early detection and surveillance of the SARS-CoV-2 variant BA.2.86 — Worldwide, July–October 2023. MMWR Morb Mortal. Wkly. Rep. 72 (43), 1162–1167 (2023).
Flach, C. F., Hutinel, M., Razavi, M., Åhrén, C. & Larsson, D. G. J. Monitoring of hospital sewage shows both promise and limitations as an early-warning system for carbapenemase-producing enterobacterales in a low-prevalence setting. Water Res. 200, 117261 (2021).
Silvester, R. et al. Metagenomics unveils the role of hospitals and wastewater treatment plants on the environmental burden of antibiotic resistance genes and opportunistic pathogens. Sci. Total Environ. 961, 178403 (2025).
Jakobsen, L. et al. Characterisation, dissemination and persistence of gentamicin resistant Escherichia coli from a Danish university hospital to the waste water environment. Environ. Int. 34 (1), 108–115 (2008).
Guo, X. et al. Metagenomic analysis of antibiotic resistance genes in untreated wastewater from three different hospitals. Front. Microbiol. 12, 709051 (2021).
Freeman, C. N. et al. Antimicrobial resistance gene surveillance in the receiving waters of an upgraded wastewater treatment plant. FACETS 3 (1), 128–138 (2018).
Mosaka, T. B. M., Unuofin, J. O., Daramola, M. O., Tizaoui, C. & Iwarere, S. A. Inactivation of antibiotic-resistant bacteria and antibiotic-resistance genes in wastewater streams: Current challenges and future perspectives. Front. Microbiol. 13, 1100102 (2023).
Cai, M. et al. Occurrence and temporal variation of antibiotics and antibiotic resistance genes in hospital inpatient department wastewater: impacts of daily schedule of inpatients and wastewater treatment process. Chemosphere 292, 133405 (2022).
Lee, T. D. et al. Rapid detection of KPC, NDM, and OXA-48-like carbapenemases by real-time PCR from rectal swab surveillance samples. J. Clin. Microbiol. 53 (8), 2731–2733 (2015).
Payne, M. et al. mcr-1–positive colistin-resistant Escherichia coli in traveler returning to Canada from China. Emerg. Infect. Dis. 22 (9), 1673–1675 (2016).
Bustin, S. A. et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 55 (4), 611–622 (2009).
Guo, H. et al. Global emergence of carbapenem-resistant Klebsiella pneumoniae co-carrying multiple carbapenemases. Comput. Struct. Biotechnol. J. 21, 3557–3563 (2023).
Diamond, M. B. et al. Wastewater surveillance of pathogens can inform public health responses. Nat. Med. 28 (10), 1992–1995 (2022).
Goossens, H., Ferech, M., Vander Stichele, R., Elseviers, M. & ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 365 (9459), 579–587 (2005).
Martinez, E. P. et al. Seasonality of antimicrobial resistance rates in respiratory bacteria: A systematic review and meta-analysis. PLoS One. 14 (8), e0221133 (2019).
Tiwari, A. et al. Wastewater surveillance detected carbapenemase enzymes in clinically relevant Gram-Negative bacteria in Helsinki, Finland; 2011–2012. Front. Microbiol. 13, 887888 (2022).
Suda, K. J., Hicks, L. A., Roberts, R. M., Hunkler, R. J. & Taylor, T. H. Trends and seasonal variation in outpatient antibiotic prescription rates in the United States, 2006 to 2010. Antimicrob. Agents Chemother. 58 (5), 2763–2766 (2014).
Miller, J., Novak, J., Knocke, W. & Pruden, A. Elevation of antibiotic resistance genes at cold temperatures: Implications for winter storage of sludge and biosolids. Lett. Appl. Microbiol. 59(6), 587–593 (2014).
Lorenzin, G. et al. Detection of NDM-1/5 and OXA-48 co-producing extensively drug-resistant hypervirulent Klebsiella pneumoniae in Northern Italy. J. Glob Antimicrob. Resist. 28, 146–150 (2022).
Ahmed El-Domany, R., El-Banna, T., Sonbol, F. & Abu-Sayedahmed, S. H. Co-existence of NDM-1 and OXA-48 genes in carbapenem resistant Klebsiella pneumoniae clinical isolates in Kafrelsheikh, Egypt. Afr. Health Sci. 21 (2), 489–496 (2021).
Verma, A. et al. Outcomes in oxacillinases β-lactamases (OXA-48) and New Delhi metallo-β-lactamase (NDM-1)-producing, carbapenem-resistant Klebsiella pneumoniae isolates obtained from bloodstream infections. Cureus 14 (7), e27197 (2022).
Mairi, A., Pantel, A., Sotto, A., Lavigne, J. P. & Touati, A. OXA-48-like carbapenemases producing Enterobacteriaceae in different niches. Eur. J. Clin. Microbiol. Infect. Dis. 37 (4), 587–604 (2018).
Poirel, L., Héritier, C., Tolün, V. & Nordmann, P. Emergence of oxacillinase-mediated resistance to imipenem in Klebsiella pneumoniae. Antimicrob. Agents Chemother. 48 (1), 15–22 (2004).
Poirel, L., Potron, A. & Nordmann, P. OXA-48-like carbapenemases: The phantom menace. J. Antimicrob. Chemother. 67 (7), 1597–1606 (2012).
Dabos, L. et al. To be or not to be an OXA-48 carbapenemase. Microorganisms 10 (2), 258 (2022).
Singh, S., Singh, S. K., Chowdhury, I. & Singh, R. Understanding the mechanism of bacterial biofilms resistance to antimicrobial agents. Open. Microbiol. J. 11, 53–62 (2017).
Acknowledgements
We would like to thank the Metro Vancouver Laboratory team for collecting wastewater samples used in this study. We would also like to acknowledge all regional health authorities for obtaining the specimens and participating in the provincial CPO surveillance program. Moreover, we would like to thank the Bacteriology and Mycology Laboratories at the BCCDC Public Health Laboratories for conducting confirmatory qPCR testing for CPOs and generously sharing the positive case count data.
Funding
All work was conducted with support from British Columbia provincial funding allocated to the BCCDC Public Health Laboratory.
Author information
Authors and Affiliations
Contributions
SCM wrote the main manuscript text, prepared figures, and conducted both clinical and wastewater data analysis. SMW performed wastewater experiments. JK assisted with the design and analysis of wastewater experiments. SR contributed to the analysis of clinical data. FB facilitated the acquisition of wastewater samples used in the study. BH assisted with wastewater experimental work. NP and LH reviewed the manuscript and provided feedback and insight on the wastewater and clinical analyses. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mansour, S.C., Woo, S.M., Kopetzky, J. et al. Enhancing surveillance of antimicrobial resistant organisms in British Columbia through community-level wastewater testing. Sci Rep 16, 2835 (2026). https://doi.org/10.1038/s41598-025-32629-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-32629-z
