
Abstract
Background
Postoperative Delirium (POD) is a relatively common acute neurocognitive complication in elderly patients with hip fractures. However, its incidence and independent risk factors remain incompletely defined. This analysis utilized prospectively collected data from 238 consecutive patients with hip fractures aged ≥ 60 years. Univariate analyses were first used to assess potential risk factors for POD. Variables showing significant associations underwent collinearity testing, and those with high variance inflation factors (VIF > 5.0) were excluded. To ensure model stability per the Events Per Variable (EPV) principle and to focus on clinically meaningful predictors, a final set of 7 variables was entered into a multivariate logistic regression model to identify independent predictors of POD. The analysis included 238 patients with an average age of 79.0 years, of whom 73.1% were women. The overall incidence of POD was 31.9%. Those who developed POD were significantly older (82.5 vs. 77.3 years) and a higher proportion were female (77.6% vs. 71.0%). Multivariate analysis identified four independent predictors of POD: frailty (OR = 2.62, 95% CI 1.22–5.62, P = 0.014), a preoperative waiting time exceeding 90 h (OR = 2.59, 95% CI 1.31–5.15, P = 0.007), postoperative infection (OR = 2.41, 95% CI 1.21–4.82, P = 0.013), and advanced age over 82 years (OR = 2.44, 95% CI 1.26–4.73, P = 0.008). Patients with POD experienced longer ICU stays (median 17.8 days vs. 0 days, P < 0.001) and longer total hospitalization (13 days vs. 10 days, P < 0.001). Frailty, prolonged preoperative waiting time, postoperative infection, and advanced age were identified as independent predictors of POD in older hip fracture patients. These findings may help improve understanding of delirium risk in this population and suggest areas for further investigation. Further studies are warranted to explore causal mechanisms and to evaluate whether perioperative interventions aimed at reducing waiting time, assessing frailty, or preventing infections might mitigate the risk of POD.
Similar content being viewed by others


Introduction
Hip fracture remains a major clinical challenge in the aging population, representing a leading cause of functional decline and increased long-term care dependency. Against this backdrop, POD has emerged as a frequent and serious neuropsychiatric complication in older hip fracture patients, with reported incidence rates ranging from 5 to 61%1,2,3, is recognized as a serious complication that independently predicts poor long-term functional outcomes4,5,6. Clinically, it is categorized into hyperactive, hypoactive, and mixed subtypes; however, it remains substantially underdiagnosed—only 20.9% of cases are systematically documented, and up to 75% are overlooked in emergency settings7, underscoring critical gaps in recognition and diagnosis.
The rising prevalence of hip fractures amid global aging further compounds this issue, particularly given the vulnerability of this patient cohort. These individuals often present with osteoporosis (prevalent in 69% of fragility fracture cohorts8, impaired ambulation, and complex multimorbidity profiles8,9, which may increase susceptibility to POD. This complication exerts considerable bidirectional strain on both the healthcare system and patient outcomes. Evidence indicates that POD is associated with a 36% prolongation of ICU stay and a 22% increase in total hospitalization duration10. Moreover, it extends rehabilitation time by 6.5 days, elevates the risk of pressure ulcer11,12 and surgical site infections (OR = 4.38)13, and is significantly associated with increased long-term mortality (OR = 2.11)14.
Previous systematic reviews and meta-analyses have consistently identified several core risk factors for POD in this population, such as advanced age, preoperative cognitive impairment, and specific comorbidities15,16. While acknowledging these foundations, such studies have concurrently highlighted knowledge gaps regarding additional modifiable factors like frailty and prolonged waiting time. Among these, frailty is of particular interest due to its multifaceted mechanistic links to POD. Frailty, defined by diminished physiological reserve and impaired stress response, predisposes patients to POD through interconnected mechanisms. Chronic inflammation, often termed “inflammatory aging,” marked by elevated pro-inflammatory cytokines such as interleukin-6 and tumor necrosis factor-α, disrupts the integrity of the blood-brain barrier17,18. This inflammatory burden is compounded by mitochondrial dysfunction19, which generates oxidative stress, triggers neuronal apoptosis, and impairs synaptic plasticity. Additionally, hypothalamic-pituitary-adrenal (HPA) axis dysregulation disrupts cortisol rhythm, contributing to cognitive fluctuations20. These insights highlight the potential of targeted frailty interventions as innovative strategies to mitigate the risk of POD21.
Therefore, this study aimed to address these specific gaps by identifying key risk factors using a substantial prospectively collected dataset, while also evaluating POD’s impact of POD on critical outcomes, including ICU stay, hospitalization duration, and postoperative complications. Our findings may inform targeted preventive strategies to improve care and reduce the associated healthcare burden.
Materials and methods
Study design
This was a prospective cohort study; all data collection for exposures and outcomes occurred after study initiation and followed patients forward in time.
This prospective cohort study was conducted at Beijing Tsinghua Chang Gung Hospital. It included patients aged ≥ 60 years with imaging-confirmed hip fractures requiring surgery. Patients were consecutively enrolled between January 2022 and November 2023. The study protocol was approved by the institutional ethics committee (No. 21277-0-01), and all methods were performed in accordance with the relevant guidelines and regulations. The trial was prospectively registered at ClinicalTrials.gov (NCT05246254). All participants provided witnessed written informed consent after trained researchers explained the study procedures. Data collection used standardized case report forms integrated with an electronic medical record system for real-time perioperative data verification.
Inclusion and exclusion criteria
This prospective cohort study enrolled 238 patients hospitalized for hip fractures between January 1, 2022, and November 30, 2023. The inclusion criteria were as follows: age ≥ 60 years, presence of hip fracture, signed informed consent form, American Society of Anesthesiologists (ASA) class I-IV, and surgery performed by a consistent anesthetic and surgical team. Exclusion criteria included: inability to provide informed consent; conservative treatment without surgery; duplicate fracture records (referring to instances where the same fracture episode was inadvertently entered into the screening log more than once); inability to complete cognitive function tests; delirium during initial assessment; diagnosed psychiatric or substance use disorders; and incomplete or missing follow-up data. All patients received standardized preoperative preparation, anesthesia, and postoperative management. The primary objective of this study was to evaluate the occurrence of POD.
Standardized anesthetic management protocol
A standardized anesthetic protocol was implemented for all patients. The operating room environment was maintained at 20–23 °C with 50–60% humidity. Active warming was achieved using forced-air blankets and fluid warmers to sustain normothermia (36.5–37.2 °C).
All patients received continuous monitoring including electrocardiography, non-invasive blood pressure, and pulse oximetry. For neuraxial anesthesia, combined spinal-epidural anesthesia was performed at L2-3/L3-4 interspaces using 0.75% isobaric ropivacaine (1.8–2.2 mL), followed by epidural catheter placement. Sedation was maintained with dexmedetomidine infusion (0.1–0.3 µg/kg/h) targeting Ramsay Sedation Scale scores of 2–3.
For patients requiring general anesthesia, induction included etomidate or propofol with sufentanil and rocuronium. Anesthesia was maintained with propofol or dexmedetomidine infusion combined with remifentanil and sevoflurane, targeting bispectral index values of 40–60. Invasive arterial monitoring was utilized for ASA class ≥ III patients or those with significant cardiopulmonary comorbidities. All patients received multimodal analgesia including ultrasound-guided continuous femoral nerve block.
Observation indicators
Preoperative variables included age, sex, BMI, smoking history, alcohol abuse, comorbidities (hypertension, heart disease, diabetes mellitus, kidney diseases, history of stroke), and Charlson Comorbidity Index (CCI), with patients categorized into low (≤ 2) and high (> 2) comorbidity burden groups. Nutritional status was assessed using the Mini Nutritional Assessment (MNA) scale, classifying participants as malnourished (< 17), at risk of malnutrition (17–23.5), or with a normal nutritional status (≥ 24). Frailty status, based on the Frailty Index (FI)22, divided participants into non-frail (FI < 0.25) and frail (FI ≥ 0.25) status. Other preoperative factors included medication history, fracture type and side, presence of multiple fractures, history of contralateral hip fracture, preoperative laboratory test results, Prognostic Nutrition Index (PNI), preoperative waiting time (from admission to surgery), and ASA classification. Operative variables comprised surgical method, anesthesia type, operation duration, and estimated blood loss. Postoperative variables covered complications (venous thromboembolism, urinary tract infections, pulmonary infections, myocardial infarction, stroke, gastrointestinal hemorrhage), hemoglobin level on postoperative day 1, ICU stay duration, and total hospital length of stay.
Outcome measures
The Confusion Assessment Method (CAM)23,24, the internationally validated gold-standard instrument for delirium detection, was systematically implemented with its four diagnostic pillars: (1) acute onset/fluctuating course, (2) inattention, (3) disorganized thinking, and (4) altered consciousness. Demonstrating exceptional psychometric properties (sensitivity: 95–100%; specificity: 90–95%), this protocol enabled standardized identification of both hyperactive and hypoactive delirium subtypes. Certified delirium assessments were conducted by a trained research team, which included clinical research nurses performing twice-daily evaluations under the supervision of a consultant geriatrician specialized in cognitive disorders. This multi-rater, instrument-based approach was implemented to ensure consistent and objective diagnosis. Assessments were carried out at critical postoperative intervals (POD 1, 2, 3, 5, 7) using time-series CAM evaluations to capture dynamic symptom trajectories. The rigorous assessment framework incorporated serial neurological examinations to differentiate transient cognitive changes from true delirium episodes.
Outcome indicators
The primary outcome was the occurrence of POD, which was diagnosed using the Confusion Assessment Method (CAM). Secondary outcomes included the hospital length of stay and the ICU length of stay (defined as the duration from ICU admission to transfer to a general ward). Outcome assessors received standardized training in delirium evaluation protocols prior to data collection.
Sample size estimation
The required sample size was estimated a priori based on data from our previous cohort study25. In that study, the incidence of POD was 42.3% (30/71) in frail patients versus 7.8% (6/77) in non-frail patients following hip fracture surgery. Utilizing the established proportions (p1 = 0.423, p0 = 0.078), a two-sided alpha of 0.05, and 90% power (β = 0.1), the minimum sample size necessary to detect this difference was calculated to be 118 participants (59 per group) employing the standard formula for comparing two proportions. The final cohort of 238 patients therefore provided sufficient statistical power (> 99%) for the primary analysis.
Statistical analysis
The analytical cohort was stratified based on the occurrence of POD within 7 postoperative days. The normality of continuous variables was assessed using the Kolmogorov-Smirnov test. Data that is normally distributed (for example, metabolic and nutritional parameters) is presented as mean (SD); data that is not normally distributed (for example, surgical parameters and length of stay) is expressed as the median and interquartile range (IQR). Categorical variables are summarized as frequencies and percentages. Intergroup comparisons employed Student’s t-test or the Mann-Whitney U test for continuous variables, and the Chi-square or Fisher’s exact test for categorical variables, as appropriate.
Univariate logistic regression was performed to identify variables associated with POD. All variables with a significance level of p < 0.05 in univariate analysis were assessed for multicollinearity using VIF diagnostics. Variables with a VIF > 5 were excluded from subsequent multivariate analysis.
The observed 76 POD events were used to assess the stability of the multivariable model, with the EPV principle guiding the inclusion of approximately 7 predictors. In order to adhere to this principle and focus on core pathophysiological pathways, urinary tract and pulmonary infections were combined into a composite “postoperative infection” variable. The final multivariable logistic regression model was adjusted for the following covariates: age > 82 years, frailty status, preoperative waiting time > 90 h, postoperative infection, nutritional status (MNA scale), CCI score, and ASA physical status classification.
Adjusted odds ratios with 95% confidence intervals were computed, and all statistical analyses were performed using SPSS (version 27.0; IBM Corp., Armonk, NY, USA). A two-sided p value < 0.05 was considered statistically significant.
Results
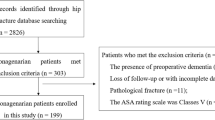
In the period spanning from January 2021 to November 2023, a total of 286 patients were systematically evaluated for their suitability for inclusion. Of these, 238 satisfied the stipulated inclusion criteria and were consequently enrolled in the present cohort (see Fig. 1 for details). The collection of all prespecified outcome data was conducted prospectively, with complete follow-up and no missing data.

Depicts the flowchart of patient enrollment, with POD denoting postoperative delirium.
Characteristics of the study population
The study cohort comprised 238 older hip fracture patients with mean age 79.0(SD 8.7) years (females: 73.1%, n = 174). POD occurred in 76 cases (31.9%). Comparative analysis revealed significant intergroup disparities in demographic and clinical profiles: POD patients demonstrated significantly higher prevalence of advanced age (> 82 years: 63.2% vs. 34.0%, p < 0.001), preoperative frailty (76.3% vs. 34.6%, OR = 6.10, 95% CI 3.28–11.34), and malnutrition (22.4% vs. 4.3%, p < 0.001). Nutritional biomarkers showed marked deterioration in POD group - total albumin (66.8 [SD 5.5] vs. 69.3 [SD 5.4] g/L, p < 0.001) and PNI (37.2 [SD 4.0] vs. 39.5 [SD 4.0], p < 0.001). The mean preoperative waiting time was 65.5 h. Delays beyond 48 h were primarily due to medical optimization of comorbidities and operational constraints, reflecting real-world clinical practice at our center during the study period. Comparative analysis of anesthetic modalities revealed a predominance of combined spinal anesthesia over general anesthesia in both POD and non-POD cohorts (67.1% vs. 32.9% and 72.2% vs. 27.8%, respectively), though these proportional differences lacked statistical significance (p > 0.05). Similarly, no significant intergroup disparities emerged in operative strategy selection, with comparable utilization rates of arthroplasty versus internal fixation (46.6% vs. 53.4%, p = 0.337) across study populations, as detailed in Table 1. These findings suggest that neither anesthetic modality nor surgical approach independently contributed to delirium risk stratification in this cohort.
Patients with POD exhibited a statistically significant elevation in complication rates compared to the control cohort (47.4% vs. 20.4% for urinary tract infections, p < 0.001; 18.4% vs. 4.3% for pulmonary infections, p < 0.001), with infectious complications emerging as the most prominent manifestations. The delirium cohort demonstrated substantially prolonged critical care utilization (median ICU duration: 17.8 days vs. 0 days, p < 0.001) and increased total hospitalization requirements (median hospital stay: 13.0 days vs. 10.0 days, p < 0.001), reflecting greater healthcare resource consumption.
Univariate analysis (Table 2) identified multiple significant predictors of POD, including advanced age (> 82 years; OR = 3.34), prolonged preoperative waiting time (> 90 h; OR = 3.57), frailty (OR = 6.10), comorbidities (hypertension, respiratory diseases, stroke history), malnutrition (OR = 12.68), and infectious complications (urinary tract infections: OR = 3.52; pulmonary infections: OR = 5.00). Notably, nutritional indices (MNA scale), ASA classification and CCI demonstrated statistical significance in univariate models (all p < 0.05) but were excluded from the multivariate model. This exclusion likely reflects either collinearity with retained variables (e.g., frailty and age) or their potential role as secondary outcomes rather than independent etiological factors. Multivariable logistic regression analysis (see Table 3) identified four independent predictors of POD: frailty (OR = 2.62, P = 0.014), preoperative waiting time > 90 h (OR = 2.59, P = 0.007), postoperative infection (OR = 2.41, P = 0.013), and age > 82 years (OR = 2.44, P = 0.008). Collectively, these findings suggest that frailty, protracted preoperative waiting time, and postoperative infection are the primary factors associated with POD in this cohort. This provides an evidence-based foundation for refining perioperative assessment and guiding future interventional research.
Discussion
This study identifies frailty, a preoperative waiting time exceeding 90 h, and postoperative infection as independent and significant risk factors for POD in older hip fracture patients, even after adjustment for advanced age (> 82 years). Our findings regarding the association between frailty and delirium are consistent with previous observations across surgical cohorts3,25,26, and the adverse impact of delayed surgery has likewise been reported in earlier work27,28. The present analysis adds specificity by demonstrating that frailty remains an independent predictor even after adjustment for age and surgical timing, by identifying a data-driven threshold of 90 h for prolonged waiting time, and by confirming postoperative infection as an additional independent factor. The establishment of this threshold may facilitate the elucidation of the inconsistencies observed in previous studies that evaluated the clinical relevance of waiting time28,29. The correlation with postoperative infection underscores the potential contribution of inflammatory processes to the risk of delirium. Taken together, these findings offer clinically relevant information for risk stratification and perioperative decision-making, while acknowledging that the observational design precludes conclusions about causality or the effectiveness of specific interventions.
Our study demonstrates that preoperative frailty is a significant and independent predictor of POD in older patients with hip fractures (OR = 2.65), a finding that is consistent with and adds supportive evidence to the existing body of research25,30,31. The association between frailty and adverse postoperative outcomes, including delirium, has been repeatedly demonstrated in diverse surgical and hospitalized older populations. For instance, Leung et al. identified frailty as an independent risk factor for POD in non-cardiac surgery patients26, while a meta-analysis of 15 cohorts (n = 3,250) reported a frailty prevalence of 27.1% and a POD incidence of 15.8%, demonstrating an elevated risk associated with frailty (pooled OR = 3.23)32. The findings of this study are further supported by cohort-specific evidence from geriatric trauma patients studied by Esmaeeli et al.33 (n = 556, OR = 1.33) and from the total hip arthroplasty cohort reported by Chen et al.34 (n = 383, OR = 3.31), both of which also identified frailty as an independent predictor. By providing data from a well-characterized older hip fracture cohort, the results of this study add to and extend the accumulating evidence on the central role of frailty in delirium vulnerability.
The present analysis contributes to a more refined understanding of POD risk in hip fracture patients. Our findings show that frailty remains a robust and independent predictor even after comprehensive adjustment for factors such as advanced age and prolonged preoperative waiting time. This observation supports the view of frailty as a distinct state of physiological vulnerability, characterized by dysregulated inflammatory and stress-response pathways that may underlie key pathogenic mechanisms17,18,19,20. The integration of a standardized frailty assessment within the preoperative evaluation process has the potential to facilitate the early identification of high-risk patients who could benefit from targeted perioperative strategies, including geriatric co-management or prehabilitation. It is evident from the aforementioned findings that assessments and interventions targeting the physiological pathways central to frailty are of paramount importance when seeking to enhance perioperative care21.
The multivariate analysis indicates that advanced age (> 82 years) remains an independent predictor of POD (OR = 2.44). This observation supports the view that the influence of age persists even after adjusting for clinically relevant factors such as frailty and preoperative waiting time. The study emphasizes the significance of age as a reflection of cumulative biological susceptibility. The association aligns well with the existing literature describing the relationship between older age and delirium, a link often attributed to age-related reductions in physiological reserve, compromised neurovascular function, and a greater comorbidity burden35,36,37.
The critical refinement offered by our study lies in the identification of a specific threshold (> 82 years) within a hip fracture cohort and its demonstration as an independent factor after adjustment for other modifiable factors. This indicates that in the very old, biological aging processes may create a substrate of heightened neuroinflammatory susceptibility and reduced physiological resilience17,19,38,39. Consequently, advanced age may serve as a crucial, independent risk indicator, warranting particular attention in the perioperative risk stratification of geriatric hip fracture patients.
Similarly, prolonged preoperative waiting time (> 90 h) was identified as a potent and modifiable risk factor for POD (adjusted OR = 2.59). As is well-established, there is a detrimental association between surgical delay and postoperative complications27,28,29. However, the present analysis offers greater precision and refinement to this understanding. The present study proposes a high-risk threshold of 90 h, independent of frailty and chronological age, thereby providing healthcare systems with a pragmatic, evidence-based operational target. This delineated threshold also offers a plausible explanation for the variability reported in previous studies40,41,42, suggesting that the escalation in delirium risk may occur predominantly beyond this critical temporal tipping point. These findings emphasize the necessity of implementing expedited surgical pathways with a view to mitigating preventable risk in this vulnerable population.
The findings of this study demonstrate that the risk associated with waiting is not merely a function of elapsed time, but rather appears to escalate once a biological tipping point is exceeded, potentially through compounded pain, stress, inflammation, and metabolic derangement43,44,45. Consequently, in conjunction with system-level endeavours to minimise delays, proactive prehabilitation strategies that mitigate these physiological stressors may hold particular significance for patients who encounter unavoidable waiting periods prior to surgery44,45.
Furthermore, this prospective study confirms postoperative infection as an independent risk factor for POD in older hip fracture patients. This finding aligns with previous research46, and the prospective design offers a clearer temporal sequence between postoperative infection and subsequent delirium compared with retrospective analyses. In these vulnerable patients, infection may function as a systemic stressor rather than a localized event, potentially contributing to neuropsychiatric manifestations through inflammatory mediator cascades and metabolic disturbances. While acknowledging the multifactorial origins of delirium, the prospectively validated independent association with infection underscores its clinical significance. Incorporating rigorous infection-control measures—such as vigilant monitoring for early signs, strict adherence to aseptic technique, and minimizing invasive device use—into broader delirium-prevention protocols may help reduce the risk of POD and support better long-term outcomes for patients47.
In contrast, neither the type of anaesthesia nor the surgical procedure showed a significant association with the incidence of postoperative delirium (POD), which is consistent with recent meta-analyses16. This suggests that these perioperative management choices are not the main determinants of delirium risk in this population. Instead, our findings reinforce the idea that intrinsic patient vulnerability, as measured here by frailty, plays a more pivotal role. This highlights the importance of prioritizing comprehensive geriatric assessment over procedure-centric approaches.
The present study demonstrates that POD is associated with important clinical sequelae, including a markedly higher incidence of myocardial infarction (5.3% vs. 0.6%) and a prolonged ICU length of stay, consistent with previous reports of increased resource utilization48,49. The potential for a pathophysiological relationship between delirium and cardiac events may be attributable to shared mechanisms, such as systemic inflammation19. The higher incidence of POD in our cohort compared with that reported by Hernandez et al. in a general surgical population (31.9% vs. 16.4%)50, highlights the substantial baseline vulnerability characteristic of geriatric patients with hip fractures. It is important to note that our model identified frailty, rather than the more conventional ASA classification, as a primary predictor. This finding suggests that conventional perioperative risk tools may inadequately capture the dimension of physiological reserve that is most relevant for older adults. The observed discrepancy from prior findings16 may be attributed to the distinctively high vulnerability inherent to the hip fracture population, which is not fully captured by conventional perioperative risk assessments.
This study has several limitations. The single-center design and the absence of inflammatory biomarker assessment (e.g., IL-6, CRP) may limit the generalizability of our findings. While clinically representative, the inclusion of patients with preexisting dementia in our frailty assessment may introduce selection bias. Furthermore, the exclusion of patients unable to consent or complete baseline tests may limit the applicability of our findings to the most vulnerable patients. Our focus on new-onset delirium precluded analysis of preoperative delirium as a risk factor. Additionally, the dichotomization of continuous variables (age and preoperative waiting time) may introduce bias and result in a loss of statistical information, although it was performed to identify clinically actionable thresholds. Most importantly, the observational nature of this study, while identifying significant associations, cannot establish causality between identified risk factors and POD due to potential residual confounding. Finally, this study focused on in-hospital outcomes; long-term survival was not assessed.
Consequently, future research should prioritize multicentre studies to validate the identified risk model. This would address the above-noted limitations and confirm the robustness of our core findings. Of particular significance is the potentially modifiable nature of the key predictors identified in this study: frailty and prolonged preoperative waiting time. These observations provide a strong rationale for interventional research. Randomized controlled trials evaluating targeted prehabilitation programs to mitigate frailty, alongside clinical pathway interventions aimed at reducing time-to-surgery towards or below the observed 90-hour threshold, are promising next steps in determining whether modifying these factors can causally reduce POD, and in supporting their translation into effective clinical practice.
Conclusion
This study identifies frailty, prolonged preoperative waiting time (> 90 h), and postoperative infection as important and potentially modifiable predictors of POD in older hip fracture patients, while advanced age (> 82 years) as a non-modifiable risk indicator. These findings highlight the potential value of incorporating routine frailty assessment, streamlined surgical pathways, and strengthened infection control into perioperative management strategies aimed at reducing delirium risk. By quantifying the associated healthcare burden, including prolonged ICU stays, the results also underscore the potential economic implications of targeted preventive approaches. Further randomized controlled trials are recommended to validate this multi-component intervention strategy.
Data availability
The corresponding author can provide the raw data from this study upon reasonable request.
References
Robertson, B. D. & Robertson, T. J. Postoperative delirium after hip fracture. J. Bone Joint Surg. Am. 88, 2060–2068 (2006).
Chen, Y. R., Chen, Y. L., Chen, W. Y., Lin, Y. C. & Jane, S. W. [Evidence-Based nursing care of older adult patient with postoperative delirium and hip Fracture]. Hu Li Za Zhi. 68, 90–96 (2021).
Mosk, C. A. et al. Dementia and delirium, the outcomes in elderly hip fracture patients. Clin. Interv Aging. 12, 421–430 (2017).
Swarbrick, C. J. & Partridge, J. S. L. Evidence-based strategies to reduce the incidence of postoperative delirium: A narrative review. Anaesthesia 77 (Suppl 1), 92–101 (2022).
Flikweert, E. R. et al. Complications after hip fracture surgery: are they preventable? Eur. J. Trauma. Emerg. Surg. 44, 573–580 (2018).
Pollmann, C. T. et al. Orthogeriatric co-management reduces incidence of delirium in hip fracture patients. Osteoporos. Int. 32, 2225–2233 (2021).
Mailhot, T. et al. Prise En charge du délirium Chez les personnes âgées à l’urgence. Soins D’urgence. 1, 43–51 (2023).
Viveros-García, J. C. et al. Fragile hip fracture in mexico: where are we today? where do we want to go? Acta Ortop. Mex. 32, 334–341 (2018).
Rincón Gómez, M. et al. Hip fracture co-management in the elderly in a tertiary referral hospital: A cohorts study. Rev. Clin. Esp. (Barc). 220, 1–7 (2020).
Kirfel, A. et al. Postoperative delirium is an independent factor influencing the length of stay of elderly patients in the intensive care unit and in hospital. J. Anesth. 36, 341–348 (2022).
Berian, J. R. et al. Optimizing surgical quality datasets to care for older adults: lessons from the American college of surgeons NSQIP geriatric surgery pilot. J. Am. Coll. Surg. 225, 702–712e701 (2017).
Kazaure, H. S., Johnson, K. S., Rosenthal, R. & Lagoo-Deenadayalan, S. Priority areas for outcomes improvement among older adults undergoing inpatient general surgery inclusive of geriatric-pertinent complications. World J. Surg. 48, 2646–2657 (2024).
Körber, M. I. et al. Periinterventional inflammation and blood transfusions predict postprocedural delirium after percutaneous repair of mitral and tricuspid valves. Clin. Res. Cardiol. 110, 1921–1929 (2021).
Prasitlumkum, N. et al. Delirium is associated with higher mortality in transcatheter aortic valve replacement: Systemic review and meta-analysis. Cardiovasc. Interv Ther. 35, 168–176 (2020).
Yang, Y. et al. Risk factors for postoperative delirium following hip fracture repair in elderly patients: A systematic review and meta-analysis. Aging Clin. Exp. Res. 29, 115–126 (2017).
Qi, Y. M. et al. Risk factors for postoperative delirium in geriatric patients with hip fracture: A systematic review and meta-analysis. Front. Aging Neurosci. 14, 960364 (2022).
Healy, D. et al. Susceptibility to acute cognitive dysfunction in aged mice is underpinned by reduced white matter integrity and microgliosis. Commun. Biol. 7, 105 (2024).
Quinlan, N. et al. Vulnerability: the crossroads of frailty and delirium. J. Am. Geriatr. Soc. 59 (Suppl 2), S262–268 (2011).
Jia, M. et al. Liraglutide ameliorates delirium-like behaviors of aged mice undergoing cardiac surgery by mitigating microglia activation via promoting mitophagy. Psychopharmacol. (Berl). 241, 687–698 (2024).
Olsson, T. Activity in the hypothalamic-pituitary-adrenal axis and delirium. Dement. Geriatr. Cogn. Disord. 10, 345–349 (1999).
Guncay, T. et al., Nicotinamide prevents the plasticity impairments and the cognitive dysfunction caused by bone fracture in older mice. J. Gerontol. Biol. Sci. Med. Sci. (2025).
Song, X., Mitnitski, A. & Rockwood, K. Prevalence and 10-year outcomes of frailty in older adults in relation to deficit accumulation. J. Am. Geriatr. Soc. 58, 681–687 (2010).
Spies, M., Frey, R., Friedrich, M-E., Kasper, S. & Baldinger-Melich, P. Delir – ein evidenzbasierter Überblick. Wiener Klinische Wochenschrift Educ. 14, 1–17 (2019).
Becker, C. & Bühl, K. Delir in der alterstraumatologie. Op-Journal 30, 40–45 (2014).
Feng, C. et al. Association of preoperative frailty with the risk of postoperative delirium in older patients undergoing hip fracture surgery: A prospective cohort study. Aging Clin. Exp. Res. 36, 16 (2024).
Leung, J. M., Tsai, T. L. & Sands, L. P. Brief report: preoperative frailty in older surgical patients is associated with early postoperative delirium. Anesth. Analg. 112, 1199–1201 (2011).
Zhou, B., Wang, A. & Cao, H. Risk prediction models for postoperative delirium in elderly patients with fragility hip fracture: A systematic review and critical appraisal. Int. J. Orthop. Trauma. Nurs. 52, 101077 (2024).
Wan, W., Li, L., Zou, Z. & Chen, W. Study on the predictive model of delirium risk after surgery for elderly hip fractures based on meta-analysis. Eur. Geriatr. Med. 16, 245–270 (2025).
Lee, H. B. et al. Predisposing factors for postoperative delirium after hip fracture repair in individuals with and without dementia. J. Am. Geriatr. Soc. 59, 2306–2313 (2011).
Dong, X. et al. Association of frailty with adverse outcomes in surgically treated geriatric patients with hip fracture: A meta-analysis and trial sequential analysis. PLoS One. 19, e0305706 (2024).
Zhao, H., Wei, P. & Feng, Y. Association between frailty and clinical outcomes and quality of life in older adults following hip fracture surgery: A retrospective cohort study. Anesth. Analg. 134, 1035–1042 (2022).
Fu, D., Tan, X., Zhang, M., Chen, L. & Yang, J. Association between frailty and postoperative delirium: a meta-analysis of cohort study. Aging Clin. Exp. Res. 34, 25–37 (2022).
Esmaeeli, S. et al. Association of preoperative frailty with postoperative delirium in elderly orthopedic trauma patients. Aging Clin. Exp. Res. 34, 625–631 (2022).
Chen, Y. & Qin, J. Modified frailty index independently predicts postoperative delirium and delayed neurocognitive recovery after elective total joint arthroplasty. J. Arthroplasty. 36, 449–453 (2021).
Proulx, E., Piva, M., Tian, M. K., Bailey, C. D. & Lambe, E. K. Nicotinic acetylcholine receptors in attention circuitry: The role of layer VI neurons of prefrontal cortex. Cell. Mol. Life Sci. 71, 1225–1244 (2014).
Wang, P. et al. Neurovascular and immune mechanisms that regulate postoperative delirium superimposed on dementia. Alzheimers Dement. 16, 734–749 (2020).
Zhu, D. et al. Comorbidity in lung cancer patients and its association with hospital readmission and fatality in China. BMC Cancer. 21, 557 (2021).
Marzola, P., Melzer, T., Pavesi, E., Gil-Mohapel, J. & Brocardo, P. S. Exploring the role of neuroplasticity in development, aging, and neurodegeneration. Brain Sci., 13 (2023).
Francavilla, F. et al., Inflammaging and Immunosenescence in the Post-COVID Era: Small molecules, big challenges. ChemMedChem. e202400672. (2024).
Lee, K. H., Ha, Y. C., Lee, Y. K., Kang, H. & Koo, K. H. Frequency, risk factors, and prognosis of prolonged delirium in elderly patients after hip fracture surgery. Clin. Orthop. Relat. Res. 469, 2612–2620 (2011).
Levinoff, E. et al. Precipitants of delirium in older inpatients admitted in surgery for Post-Fall hip fracture: An observational study. J. Frailty Aging. 7, 34–39 (2018).
Juliebø, V. et al. Risk factors for preoperative and postoperative delirium in elderly patients with hip fracture. J. Am. Geriatr. Soc. 57, 1354–1361 (2009).
Hasanzadeh-Kiabi, F. & Negahdari, B. Applications of drug anesthesia in control chronic pain. J. Invest. Surg. 32, 232–237 (2019).
Tong, R. L. et al. Stress circuitry: Mechanisms behind nervous and immune system communication that influence behavior. Front. Psychiatry. 14, 1240783 (2023).
Kiecolt-Glaser, J. K., Page, G. G., Marucha, P. T., MacCallum, R. C. & Glaser, R. Psychological influences on surgical recovery. Perspectives from psychoneuroimmunology. Am. Psychol. 53, 1209–1218 (1998).
de Haan, E., van Rijckevorsel, V., Bod, P., Roukema, G. R. & de Jong, L. Delirium after surgery for proximal femoral fractures in the frail elderly patient: risk factors and clinical outcomes. Clin. Interv Aging. 18, 193–203 (2023).
Guo, Y. et al. Prevalence and risk factors of postoperative delirium in elderly hip fracture patients. J. Int. Med. Res. 44, 317–327 (2016).
Wu, F. et al. Systemic immune responses after ischemic stroke: from the center to the periphery. Front. Immunol. 13, 911661 (2022).
Lu, S. et al. Risk factors for postoperative delirium in patients with Stanford type A aortic dissection: A systematic review and meta-analysis. J. Cardiothorac. Surg. 19, 16 (2024).
Hernandez, B. A. et al. Post-anaesthesia care unit delirium: incidence, risk factors and associated adverse outcomes. Br. J. Anaesth. 119, 288–290 (2017).
Acknowledgements
We thank all the patients who participated in this study.
Funding
This research was financially supported by the Beijing Municipal Administration of Hospitals Incubating Program [Approval No. PX2022037].
Author information
Authors and Affiliations
Contributions
Yuzhi Wei, Haotian Wu and Huan Zhang conceptualized and designed the study, coordinated and supervised data collection, drafted the initial manuscript, and approved the final manuscript as submitted. Chunyu Feng, Ziheng Qi and Yujie Wang carried out the initial analyses, reviewed and revised the manuscript, and approved the final manuscript as submitted. Haotian Wu, Yuzhi Wei, and Huan Zhang designed the data collection, critically reviewed the manuscript, and approved the final manuscript as submitted. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by the Institutional Review Board of Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University (Approval No. 21277-0-01). The protocol was prospectively registered at ClinicalTrials.gov (NCT05246254).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wei, Y., Wu, H., Feng, C. et al. Frailty and prolonged preoperative waiting time as independent predictors of postoperative delirium in older hip fracture patients. Sci Rep 16, 3019 (2026). https://doi.org/10.1038/s41598-025-32904-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-32904-z
