
Abstract
In chronic kidney disease it is hypothesised that the association between loss of lean tissue mass (LLTM) and mortality is purely a function of multimorbidity. We conducted a systematic review in CKD patients to quantify the strength of association between LLTM and mortality or frailty surrogates, including hospitalisation and quality of life (QoL). Muscle mass was estimated using different whole-body bioimpedance methods (BI-MM). Searches of electronic databases identified 132 studies for inclusion (147542 dialysis patients; 15378 CKDG3−5 patients; 356 kidney transplant recipients [KTR], with 14429 deaths). From 67 studies reporting unadjusted analyses, 52 (78%) demonstrated associations between LLTM and mortality. In 80 studies reporting analyses adjusting for age, sex, and multimorbidity, 59 (74% overall: 74, 67 and 100% in dialysis, CKD, and KTR studies respectively) reported an association. Meta-analysis of dialysis studies reporting adjusted survival analyses found each degree decrease in phase angle or a lean tissue index < 10th percentile was associated with a 92 and 49% higher hazard of mortality respectively. In studies reporting hospitalisation and QoL measures, 63 and 76% reported associations with BI-MM respectively. In conclusion, having accounted for multimorbidity, LLTM remained associated with mortality and frailty surrogates in CKD, irrespective of the BI-MM method used.
Similar content being viewed by others

Introduction
Loss of lean tissue mass (LLTM) is common in many long-term conditions (LTCs)1. In chronic kidney disease (CKD), LLTM is postulated to reflect disease severity and is associated with fatigue, poor quality of life and frailty1. LLTM is part of the wider process of protein energy wasting (PEW) – the loss of protein and/or energy stores in CKD, which is associated with adverse outcomes, particularly as kidney function deteriorates. The pathogenesis of PEW is complex, with factors such as uraemic toxin accumulation, metabolic acidosis and breathlessness, collectively contributing to muscle deconditioning, and therefore, poorer mobility2. Additionally, CKD is characterised by multimorbidity and systemic inflammation, which both further accelerate LLTM3. However, it remains unclear whether LLTM is directly associated with adverse outcomes in CKD after controlling for the effects of multimorbidity, systemic inflammation and progressive kidney dysfunction, and whether similar associations exist in other conditions with comparable multimorbidity, such as heart failure (HF).
In CKD, LLTM commonly co-exists with tissue overhydration. Bioimpedance (BI) – a cheap, non-invasive technique which passes small alternating currents through the body, is widely used to quantify changes in body composition in CKD, by differentiating fat mass from fat free mass4. Single-frequency BI methods, such as phase angle (PA), derive from tissue resistance and reactance. Therefore, reduced PA, which is associated with increased mortality in CKD5, reflects increases in body hydration and LLTM. In contrast, multi-frequency BI methods, such as bio-impedance defined lean tissue mass (LTM), estimate body hydration and muscle mass separately, allowing for more direct assessments of the association between LLTM and adverse outcomes. Given the observed interrelationships between worsening kidney function, multimorbidity and tissue overhydration in CKD, it is crucial to determine whether the association between LLTM and adverse outcomes in CKD remains consistent as CKD progresses, particularly after adjusting for the effects of multimorbidity.
The aim of this systematic review and meta-analysis was to summarise the published evidence of the association between LLTM, using different BI methods to estimate muscle mass (BI-MM), and mortality (all-cause or cardiovascular), across different stages of CKD. By comparing analyses that did or did not adjust for comorbidities, we aimed to establish whether LLTM is associated with an increased mortality risk after controlling for multimorbidity. Where possible, we wished to quantitatively assess the strength of any associations by grouping together different BI-MM methods in meta-analyses. To further unpick the association between LLTM and mortality, we also included studies that reported frailty surrogates as secondary outcomes, including hospitalisation, and summarised these associations. Finally, we also included separate analyses for chronic heart failure - a comparator long-term condition associated with both muscle wasting and overhydration.
Results
Study population identified from systematic searches
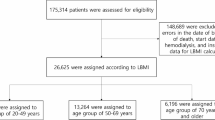
Systematic and grey literature searches yielded 12899 citations (Fig. 1), from which 7854 citations were identified following removal of duplicates. Following abstract and full paper review, 141 studies underwent data extraction: 9 in heart failure6,7,8,9,10,11,12,13,14 and 132 in kidney disease (Fig. 1). Of the kidney disease studies, 114 were in dialysis15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128, 13 were in CKD129,130,131,132,133,134,135,136,137,138,139,140,141, 2 were in KTR142,143 and 3 were in mixed kidney disease populations144,145,146. Two heart failure and 20 kidney studies were identified as describing 9 unique patient cohorts (Supplementary Table 1)8,9,19,20,27,28,31,36,38,39,62,63,70,84,94,95,103,104,122,123,124. There was considerable variation in the use of different BI measures across the studies, as summarised by (Table 1).

PRISMA flow diagram.
Methodological quality of studies
Methodological quality within the six QUIPS domains varied considerably (Supplementary Fig. 1). High risk of bias was identified in 19, 3, 6, 8, 32 and 38% of studies in the study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding and the statistical analysis domains respectively (Table 2). Sampling frame reporting, handling missing data, covariate handling (definitions, measurement and inclusion within analyses) and multiple aspects of the reporting of statistical analyses, were common methodological concerns identified across many studies.
Characteristics reported within unique cohorts identified from kidney disease and heart failure populations
Of 120 separate kidney cohorts, 78 were exclusively HD, 17 were exclusively PD, 7 were HD and PD, 13 were exclusively CKDG3A−5, 2 were exclusively KTR and 3 were in mixed kidney disease populations; containing collectively 147,542 dialysis (141930 HD and 5493 PD, with 2 studies not specifying the number of participants using each dialysis modality113,145, 15,378 CKDG3A−5 and 356 KTR participants (Table 2). Cohort size ranged from 18- 95,412 participants. Within cohorts, the reported mean or median age ranged between 38-76 years, the proportion of males ranged between 41-83% and the proportion of Caucasians ranged between 4-100%. The proportion of patients in kidney disease cohorts with different long-term conditions ranged between 5-69% for diabetes mellitus, 4–79% for cardiovascular disease and 47–98% for hypertension. A single cohort reported the proportion of patients with HIV/AIDS22, with 6 listing it as an exclusion criterion17,18,79,114,120,141. Where comorbidity scores were reported, 3 used Davies47,48,131, 19 used Charlson Comorbidity Index15,32,33,42,52,59,65,66,75,78,89,97,108,121,126,137,138,139,146 and 3 used other classifications27,44,57. Using reported mean or median values, BMI ranged between 21-32 kg/m2, serum albumin between 34- 47 g/L and high sensitivity C-reactive protein (CRP) between 0.82-122 mg/L (not counting 1 study reporting a mean CRP of 122120, the range was 0.82-22.80 mg/L). In cohorts containing dialysis patients, 20% reported residual kidney function, 55% dialysis dose (with a reported mean or median Kt/V ranging between 1.14-2.51), 2% previous transplant status and 19% dialysis access. Estimated glomerular filtration rate (eGFR) was reported as a mean or median for the whole cohort in 82% of non-dialysis CKD cohorts129,130,131,132,133,134,135,136,137,138,139,140,144,146 and 75% of KTR cohorts142,143,144; the weighted mean eGFR being 41.61 and 54.26 ml/min/1.73m2, respectively.
Within 8 heart failure cohorts there were 3716 participants with chronic heart failure (Table 2). Cohort size ranged between 41-2271. Within these cohorts, the reported mean or median age ranged between 63-72 years, the proportion of males ranged between 53-100% and the proportion of Caucasians ranged between 77-100%. The proportion of patients in heart failure cohorts with different long-term conditions ranged between 20-47% for diabetes mellitus and 27–67% for cardiovascular disease. Using reported mean or median values, BMI ranged between 27-29 kg/m2, serum albumin between 34-36 g/L, high sensitivity C-reactive protein between 3-7 mg/L and serum BNP between 370-3300pg/ml. Transthoracic echocardiogram data was reported in 88% of cohorts. Measures of kidney function were described in only 38% of heart failure cohorts; 6.7% of patients in Bieger et al. (2023)6 and 53.8% of patients in Orea-Tejeda et al. (2010)13 had an eGFR < 60 ml/min/1.73m2, with “extreme kidney failure” being treated as an exclusion criterion in Sobieszek et al. (2021)14.
Assessing the associations between different BI-MM measures and mortality in CKD and HF
Dialysis dependent kidney disease
There were 11,963 deaths in 105 cohorts containing dialysis patients (Table 2) over a maximum follow up of 1–20 years (Table 3). Of the 58 studies reporting unadjusted survival analyses in dialysis-only cohorts, 2 had inconclusive results due to inconsistencies in reporting (Table 2)113,120. Of the remaining 56 studies, 43 (77%) reported associations between BI-MM loss and mortality. Of 72 studies reporting adjusted survival analyses in dialysis-only cohorts, 3 had inconclusive results due to inconsistent reporting107,113,120 and one reported cardiovascular events (Table 3)18. Of the remaining 68 studies, 50 (74%) showed associations between BI-MM loss and mortality: 79% in HD studies, 59% in PD studies and 40% in HD and PD studies, respectively. Assessing the impact of differences in follow-up duration, using the mean, median or maximum follow up reported for each study, BI-MM was associated with mortality in 75% of studies where follow up was < 2 years, 71% where follow up was ≥2 but < 4 years and 69% where follow up was ≥4 years. Associations between BI-MM and mortality remained despite adjusting for variables thought to be important in the causal pathway for mortality in CKD (Table 3). Age, sex and either diabetes or a comorbidity score were adjusted for in most analyses. Serum albumin, CRP or IL-6 were adjusted for in 66%, 34%, and 10% of analyses, respectively (see Table 3 for a summary of all variables adjusted for in analyses).
One study from the MONDO cohort demonstrated that LTI had different effects on survival across varying levels of inflammation and overhydration, suggesting the need to account for these factors separately when assessing associations between BI-MM loss and adverse outcomes in CKD38. Except for Qin et al. (2021), no study reporting two-compartment BI estimates, such as lean body mass and fat free mass, demonstrated associations with mortality. However, the estimate of effect from Qin et al. (2021) was likely imprecise, as suggested by the wide confidence intervals reported from the survival analysis (likely reflecting the small number of participants and multiple methodological concerns about the risk of bias identified from QUIPS assessments). Beberashvilli et al. (2014) demonstrated PA was no longer associated with mortality after adjusting for the Malnutrition Inflammation Atherosclerosis (MIA) score, which itself is strongly associated with LLTM. However, in this study, PA remained associated with hospitalisation and quality of life estimates.
CKDG3−5 (non dialysis)
There were 2432 deaths in 16 cohorts involving CKDG3−5 patients, with follow-up ranging between 1-10 years129,130,131,132,133,134,135,136,137,138,139,140,144. Seven of nine studies containing exclusively CKDG3−5 patients reporting unadjusted analyses demonstrated associations between BI-MM loss (4 out of 6 PA, 2 LTM and 1 skeletal muscle mass index) and mortality (Table 2), with two studies also showing associations with either cardiovascular events or progression to end stage kidney disease. Eleven studies containing CKDG3−5 patients reported adjusted analyses for mortality. One study could not be interpreted due to unclear reporting of the adjusted estimate of effect, and another was from a mixed kidney disease population, so did not report an association exclusively in CKDG3−5. Two studies used skeletal muscle mass index as part of the definition for sarcopaenia: Pereira et al. (2015) reported an association between sarcopaenia and mortality137, whereas Kruse et al. (2020) did not134. In the latter study, however, the number of deaths was not reported, and the nested CKD sample was small. In the remaining 7 studies reporting adjusted analyses, 5 reported associations between BI-MM loss and mortality (PA studies: 2 out of 3; FFM studies: 1 out of 2; LTM studies: 2 out of 2). Within 7 studies assessing associations between BI-MM and mortality using both adjusted and unadjusted analyses, there was complete agreement (Table 2). Age, sex and diabetes or a comorbidity score were adjusted for in most CKDG3−5 adjusted analyses (Table 3).
Kidney transplant recipients
There were 34 deaths reported in 3 cohorts involving KTR over a median follow up range of 2–8 years142,143,144. Three cohorts reported adjusted analyses containing KTR − 2 exclusively in KTR had associations between BI-MM loss and mortality, with Chan et al. (2019) additionally demonstrating an association with hospitalisation (Table 3). Furthermore, Kaya et al. (2019) reported comparable estimates of effect in both the unadjusted and adjusted survival analyses for mortality when PA < 5.85, although given the high risk of bias in the statistical methods domain of the QUIPS assessment, these results should be treated cautiously. The third adjusted analysis was in a mixed kidney disease cohort (HD, CKD and KTR; 25% of the deaths were in KTR)144, which demonstrated 1-degree lower PA was associated with higher mortality, albeit, this was likely an imprecise estimate due to the small number of deaths in this study.
Heart failure
There were 1161 deaths reported in 8 cohorts involving heart failure patients over a maximum follow up range of 2–5 years. Five out of six studies reporting unadjusted analyses demonstrated BI-MM loss was associated with higher risk of mortality (Table 2). Furthermore, when considering studies reporting adjusted analyses, four out of six studies reported BI-MM loss was associated with mortality (Table 3). When comparing the unadjusted and adjusted estimates of effect within the same studies, the association between BI-MM loss and adverse outcomes was consistent, suggesting this association was present despite adjusting for multimorbidity.
Quantifying the association between different BI-MM methods and mortality: sub-group meta-analyses in Dialysis dependent kidney disease cohorts
There were 20 dialysis studies reporting unadjusted analyses for all-cause mortality that were sufficiently comparable methodologically to proceed to random effects meta-analysis (Fig. 2). The pooled estimates of hazard ratios showed higher risk of mortality for a 1-degree decrease in PA (HR 1.66, 95% CI 1.13–2.45), a 1 kg/m2 decrease in LTI (HR 1.11, 95% CI 1.07–1.15) and a LTI < 10th percentile (HR 1.52, 95% CI 1.22–1.90). In contrast, no association was observed for a 1 kg/m2 decrease in skeletal muscle mass index (HR 1.22, 95% CI 0.90–1.63) and a 1 kg decrease in LTM (HR 1.03, 95%CI 1.00-1.06). In most unadjusted analyses, there were concerns regarding heterogeneity (I2 ranged between 0.05-92%).

Forest plot for all BI-MM measures used in unadjusted survival analyses in DD-KD. Abbreviations used in forest plots: BI_Time – timing of BI-MM measurement; FU – follow up (maximum follow up time used for classification); HD – haemodialysis; Inter-d – interdialytic timing of BI-MM measurement; KRT – kidney replacement therapy modality; n(patient) – number of patients in study; n(died) – number of patients who died; PD – peritoneal dialysis; PreHD – pre-dialysis timing of BI-MM measurement in haemodialysis patient; PostHD – post-dialysis timing of BI-MM measurement in haemodialysis patient; PD-full – BI-MM measurement in peritoneal dialysis patient with a full peritoneum; PD-empty – BI-MM measurement in peritoneal dialysis patient with an empty peritoneum. The QUIPS domains are abbreviated as follows: SP – study participation, SA – study attrition, PF – prognostic factor measurement, OM – outcome measurement, SC – study confounding and ST – statistical analyses and reporting.
There were 21 dialysis studies reporting adjusted analyses for all-cause mortality that were sufficiently comparable methodologically to proceed to random effects meta-analysis (Fig. 3). A 1 kg-decrease in LTM (HR 1.08, 95% CI 1.03–1.13) and a 1-unit increase in Impedance Ratio (HR 1.15, 95% CI 1.09–1.21) were both associated with higher risk of all-cause mortality.

Forest plot for all BI-MM measures used in adjusted survival analyses in DD-KD. Abbreviations used in forest plots: BI_Time – timing of BI-MM measurement; FU – follow up (maximum follow up time used for classification); HD – haemodialysis; Inter-d – interdialytic timing of BI-MM measurement; KRT – kidney replacement therapy modality; n(patient) – number of patients in study; n(died) – number of patients who died; PD – peritoneal dialysis; PreHD – pre-dialysis timing of BI-MM measurement in haemodialysis patient; PostHD – post-dialysis timing of BI-MM measurement in haemodialysis patient; PD-full – BI-MM measurement in peritoneal dialysis patient with a full peritoneum; PD-empty – BI-MM measurement in peritoneal dialysis patient with an empty peritoneum. The QUIPS domains are abbreviated as follows: SP – study participation, SA – study attrition, PF – prognostic factor measurement, OM – outcome measurement, SC – study confounding and ST – statistical analyses and reporting.
A 1-degree decrease in PA (HR 1.92, 95%CI 1.49–2.48) was associated with higher risk of all-cause mortality (Fig. 3). This association held in leave one out meta-analysis (Fig. 4B) and when assessed graphically, using a funnel plot, studies were distributed reasonably symmetrically (Fig. 4A), suggesting publication bias was not a major concern. The proportion of variance in the observed effects when removing the effects of sampling error (I2) was 49% and the between study variance of the underlying distribution of true effect size (\(\:{\tau\:}^{2}\)) was 0.05, suggesting there were some potential concerns about heterogeneity. One study was located on the boundary of the 95% confidence interval of the funnel plot, suggesting either small sampling variation, or potentially biased estimates25: from QUIPS assessments, this study was at high risk of statistical bias. Having excluded two studies at high risk of statistical bias using the QUIPS assessment, the sensitivity pooled estimate was similar in magnitude (HR 1.78, 95%CI 1.33–2.38), but concerns about heterogeneity remained (I2 = 55% and \(\:{\tau\:}^{2}\)=0.05). Using this pooled sensitivity analysis, the 95% hazard ratio prediction interval for future survival studies using a 1-degree decrease in PA was 0.57–5.54. In the 4 studies included in the sensitivity analysis, all adjusted for age, sex and diabetes mellitus / comorbidity score. However, crucially, none of these studies adjusted for albumin (Table 3).

Leave one out meta-analysis and funnel plots for pooled estimates using LTI < 10th percentile and a 1-degree decrease in PA.
Two separate meta-analyses were conducted in studies using LTI < 10th percentile to account for different models reported by Kim et al. (2021)58. Both analyses demonstrated associations with all-cause mortality (Fig. 3), with the Kim et al. 2021a model (HR 1.49, 95%CI 1.32–1.68) being selected for subsequent sensitivity analyses (Table 3 for details). Although Marcelli et al. (2015) contributed 44% towards the final pooled estimate70, leave one out meta-analysis did not alter the overall association (Fig. 4D). The funnel plot (Fig. 4C) demonstrated that five smaller studies were distributed asymmetrically58,60,66,111,115. Although this distribution may reflect small study effects, including potentially publication bias, given their small impact on the overall weighting of the pooled estimate of effect, their influence was likely to be minimal. The proportion of variance in the observed effects when removing the effects of sampling error (I2) was 26% and the between study variance in the underlying distribution of the true effect size (\(\:{\tau\:}^{2}\)) was 0.01. Collectively, this suggested low between study heterogeneity. Sensitivity analyses that excluded studies at high risk of statistical or confounding bias (using QUIPS assessments) found the pooled estimate remained robust (HR 1.52, 95%CI 1.42–1.63), with minimal concerns about heterogeneity (I2 = 0% and\(\:{\:\tau\:}^{2}\)<0.01), suggesting the observed between study variance in the original pooled analysis was likely explained by confounding bias or methodological errors. Using the sensitivity pooled analysis, the 95% prediction interval for the hazard ratio for future survival studies using LTI < 10th percentile was 1.37–1.70. In this pooled sensitivity analysis, 80% of studies adjusted for diabetes mellitus, age and sex, with 60% adjusting for albumin, giving greater confidence that the pooled estimates of effect for a LTI < 10th percentile were adjusted for key variables thought to be associated with mortality.
Associations between BI-MM loss and secondary outcomes in CKD and HF
Of the 36 CKD studies that reported secondary outcomes (see Table 2 for further details), 63% of studies reporting on hospitalisation, 76% of studies reporting on health-related quality of life measures, 71% of studies reporting on cognitive function and 60% of studies reporting on frailty, demonstrated associations with BI-MM. Three dialysis studies showed BI-MM loss was associated with hospitalisation in adjusted analyses, with Beberashvilli et al. (2014) additionally demonstrating an association with health-related quality of life, again in an adjusted analysis. Two HF studies reported on secondary outcomes (Table 2): one showed lower PA was associated with hospitalisation and one showed FFM was not associated with HRQoL measures.
Discussion
This systematic review is the first to collate comprehensive evidence using different BI-MM methods that LLTM is associated with mortality across all stages of CKD, including in kidney transplant recipients. This association remains after adjusting for potential confounders (Table 3), such as age, biological sex, multimorbidity, inflammation, serum albumin and dialysis specific factors (such as dialysis dose and residual kidney function), suggesting LLTM is important in explaining mortality in CKD. The observed associations were consistent across different BI-MM methodologies and different sub-group meta-analyses: LTI below the 10th percentile was associated with a 49% higher risk of mortality and for every degree decrease in phase angle the mortality risk rose by 92%. Furthermore, just over 70% of kidney disease studies reporting on secondary outcomes, such as hospitalisation, quality of life, cognitive function and frailty, reported associations with BI-MM. The findings of this review are summarised graphically in (Fig. 5).

Graphical representation of the results of the systematic review. A graphical display demonstrating factors hypothesised to be important in explaining the association between LLTM and mortality in CKD, including how overhydration, although inter-related with LLTM, may explain mortality through different biological processes. Boxes highlighted with * is a primary outcome for the review and ** as a secondary outcome. AA – adjusted analysis; CKD – chronic kidney disease; CRP – C reactive protein; CVD – cardiovascular disease; DM – diabetes mellitus; HRQoL – health related quality of life measures, such as SF-36 / SF-12 and KDOQL; HTN – hypertension; IL-6 – interleukin-6; MMSE – mini mental state examination; PTH – parathyroidism; RKF – residual kidney function.
A crucial study identified in this review was Dekker et al. (2018), which reported the associations between LLTM and mortality in dialysis patients for varying levels of overhydration and systemic inflammation38. This showed haemodialysis patients with systemic inflammation and overhydration had the strongest association between LTI and mortality, whereas those without systemic inflammation and overhydration had no association. They concluded that LLTM and overhydration are linked, and that these two processes could synergistically worsen prognosis in dialysis patients38. This review, which found an association between reduced PA and mortality in dialysis patients, supports this conclusion, as PA is derived from the vector that links LLTM and tissue hydration. However, our review further quantifies the LLTM-overhydration-survival relationship and found that this varies across different grades of CKD. First, we found that BI-MM loss was associated with adverse outcomes across the whole range of kidney function – including patients with kidney transplants, where the weighted mean eGFR was just over 50 ml/min/1.73m2. Second, despite adjustment for variables known to be directly associated with overhydration – including hypoalbuminaemia, residual kidney function (in dialysis studies) and bio-impedance defined overhydration (BI-OH), which were adjusted for in 68%, 10% and 27% of these studies (Table 3), LLTM continued to be associated with mortality in 71%, 67% and 60% respectively. Therefore, although overhydration and LLTM are inextricably linked, as suggested in extreme starvation where extracellular fluid volume does not proportionally decrease with falling muscle mass147, our findings suggest LLTM is associated with mortality in CKD through potentially distinct biological processes, and not directly through overhydration (Fig. 5).
LLTM has been shown to drive the metabolic phenotype of insulin resistance, along with acting as an early marker of reduced physiological reserve148. LLTM may contribute to adverse outcomes by increasing the risk of developing frailty, where multisystem dysregulation leads to lower physiological reserve and increased vulnerability to stressors. However, the timeframe over which LLTM is associated with adverse outcomes across different stages of CKD may differ. In our study, LLTM was associated with adverse outcomes, over shorter follow up times, in dialysis studies – especially within the MONDO cohort31,34,38,39,70. In contrast, LLTM was generally associated with adverse outcomes, in studies with longer periods of follow up, in both CKDG3−5 and kidney transplant studies, and the reported associations were weaker than in the dialysis studies. These findings support the hypothesis that there is progressive skeletal muscle dysfunction with worsening kidney disease, suggesting the need to intervene during the earlier stages of CKD, if LLTM is to become a therapeutic target to improve outcomes. Furthermore, in dialysis patients, where muscle loss is most severe, there is likely to be a limited therapeutic window where the effects of LLTM could be mitigated. This hypothesis, based on the “catabolic crisis model”, suggests drivers of catabolism (such as kidney disease) slow down recovery to baseline muscle function following periods of immobility / acute illness148. It may be that kidney failure, through uraemia, metabolic acidosis and secondary hyperparathyroidism, acts as catabolic driver, with severe kidney disease more rapidly exhausting the metabolic reserve of skeletal muscle1,148. This is further exacerbated by kidney failure affecting pro-anabolic hormones (Fig. 5), which act to maintain skeletal muscle health90,149.
These hypotheses are further supported by another finding from our systematic review– that losses in muscle function do not completely nullify the association between LLTM and adverse outcomes. Sarcopaenia, defined as LLTM and loss of muscle function (commonly measured using either hand grip strength [HGS] or gait speed), is commonly observed in ageing, and is crucial in the development of frailty150. Of 10 kidney disease studies adjusting for physical strength (either directly by including hand grip strength as a variable in adjusted analyses, or by using LLTM as part of the sarcopaenia definition), half reported preserved associations between LLTM and adverse outcomes. Furthermore, of the four studies expressing LLTM as sarcopaenia (including HGS in the definition), two demonstrated associations with adverse outcomes. Overall, adjustment for muscle strength / function did not completely mitigate the relationship between LLTM and adverse outcomes in CKD, suggesting losses in skeletal muscle, and not just losses of muscle function, may explain the emergence of frailty phenotypes in CKD148.
Our review highlights the urgent need for recommendations regarding which BI-MM measures to use in CKD and heart failure studies. The use of single frequency bioimpedance measurements, such as phase angle, influenced by both muscle mass and body hydration, does not allow for dissection of relative overhydration from fat free mass. Therefore, single frequency methods cannot accurately quantify the differential associations between LLTM and overhydration on adverse outcomes in CKD and in heart failure151. In contrast, BI methods based on 3 compartmental modelling, such as the Fresenius BCM device, overcome this challenge4 by estimating LTM separately from overhydration. Given the consistent associations across different stages of CKD between LTI (LTM indexed for height squared) and mortality, using unadjusted and adjusted analyses, and given that published reference ranges in men and women for LTI are now available4, we recommend the use of 3-compartment bioimpedance methods in future studies. This recommendation was similarly proposed by Mayne et al. (2023) for studies assessing BI-OH in similar populations152.
This review has several strengths. Firstly, this is the first review to comprehensively describe the associations between LLTM and adverse outcomes across all CKD stages and heart failure using different BI-MM measures. Secondly, our findings are in line with the results of a previous systematic review and meta-analysis which assessed the association between BI-OH and mortality in dialysis patients, with similar pooled estimates of effect being observed for a 1-degree decrease in phase angle5. However, given our review employed a more exhaustive search strategy, additional studies were identified and added to the pooled estimate of effect for PA. Thirdly, from citation screening to data extraction, we used two independent study reviewers, minimising the risk of individual rater biases affecting the results from the review. Fourthly, we followed recommendations to use a-priori defined operationalisation criteria when using the QUIPS tool for bias assessment153, minimising the risk that we would systematically bias our own assessment of bias within included studies.
However, given the observational nature of studies included in this review, there were several limitations. Firstly, all described associations cannot be interpreted as causal associations. Secondly, methodological reporting varied considerably across studies, with over a third being rated as high risk of bias from confounding and errors in statistical reporting. Therefore, despite efforts to mitigate the effect of bias on our meta-analysis estimates, the results should still be interpreted with caution. Thirdly, there was widespread variation in how LLTM was defined, particularly when BI-MM was reported in survival analysis as a categorical variable, with wide variation in the cut offs used, which precluded more extensive meta-analysis. As such, future research using BI-MM should use standardised cut offs where possible, or report BI-MM as a continuous variable, when conducting survival analyses – which would yield more meaningful inter-study comparisons, and allow for more extensive meta-analyses to be conducted. Fourthly, there was considerable variation in variable inclusion across adjusted analyses, with only consistent adjustment for age, sex and diabetes / comorbidity score. As such, the possibility of residual confounding affecting the described associations, due to differential adjustment for comorbidities across studies, remains. Finally, our study was limited by our inability to adjust for the effect that LLTM has on the measurement of kidney function itself. Serum creatinine is derived from skeletal muscle, and therefore, losses of muscle mass could impact estimated GFR when used to categorise CKD. Our understanding of the associations between LLTM and mortality across different CKD stages, particularly in those with extreme LLTM, therefore may be subject to misclassification bias.
Although this review clearly establishes that LLTM is associated with mortality across all stages of CKD and in heart failure, there is no clear consensus on how BI-MM should be used in clinical practice. Given the association between LLTM and frailty (Fig. 5), and given frailty prevalence ranges between 21 and 82% in dialysis populations worldwide154, BI-MM could provide a non-invasive, easy to apply longitudinal assessment for changes in muscle mass in CKD, allowing identification of those most at risk of frailty. Although the bioimpedance spectroscopy to maintain renal output (BISTRO) trial failed to demonstrate any benefit from using bio-impedance defined overhydration to determine dry weight in dialysis patients, the role of BI-MM in identifying patients or targeted nutritional interventions has not yet been tested155. This represents a potentially novel application, since increased protein intake is recognised to reduce mortality in older adults with CKD, despite traditional concerns about accelerated disease progression. Therefore, BI-MM may help identify CKD patients at risk of frailty and potentially facilitate timely interventions, such as dietetic assessment, referral for Kidney BEAM engagement, which has been shown to reduce symptoms of fatigue in dialysis patients156, or exercise training, which has been shown to improve physical function in dialysis patients157. Furthermore, given the associations between LLTM and mortality in kidney transplant recipients, the use of BI-MM in wait-listed patients, to identify those at greatest benefit of pre-habilitation prior to transplantation, could be another important application of this technology158.
Methods
Study registration and resign
The systematic review was prospectively registered with the International Prospective Register for Systematic Reviews (PROSPERO 2021 CRD42021240688), with the design guided by the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA)159.
Search criteria
The study population was adults (≥ 18 years) with either CKD grade 3–5 (CKDG3−5), kidney transplant recipients (KTR), dialysis dependent kidney disease (DD-KD) or chronic stable heart failure who had at least one measurement of whole-body BI-MM. The primary outcome was all-cause mortality. Secondary outcomes included cardiovascular mortality, hospitalisation, falls, quality of life measures and cognitive function.
Search strategy
A comprehensive electronic systematic search of MEDLINE, EMBASE, PsychINFO, Web of Science Core Collection, AMED, CINAHL and the Cochrane Register for Controlled Trials (CENTRAL) was originally conducted from inception until the 20th June 2023. A full updated search was conducted from the 1st January 2023 to the 20th -23rd October 2025 to identify additional citations prior to publication. The updated search included a six month overlap with the original search to allow for maximal capture of newly published studies, as well as to compensate for indexing delays in electronic databases. The search strategy used a combination of medical subject headings (MeSH) and free text search terms chosen a-priori for electronic database searches. Searches of grey literature sources, including pre-print databases (bioRxiV and medRxiV), electronic thesis repositories (EThOS) and trial registries (International Standard Randomised Controlled Trial Number and the WHO International Clinical Trials Registry Platforms), used a simpler combination of free text terms, as more complex searches using Boolean operators are not possible on these platforms. Additionally, the International Journal of Body Composition Research (IJBCR) was searched manually as this is not electronically indexed. All citations from electronic and manual searches were stored in EndNote20. The full search strategies employed for all major electronic databases are provided in Supplementary Tables 2–8.
Study selection and data extraction
Duplicate screening was conducted using both semi-automatic (in EndNote20) and manual processes (Fig. 1). For the updated search, an additional duplicate removal step was performed to exclude citations already identified in the original search. Following duplicate removal, citations were transferred from EndNote20 to Rayyan to assist with screening160. Abstracts were reviewed by two independent researchers (MT all citations, with EE, AUH, RS, MS, CS, JP, BA, AMP, NW, OI or JS as the second reviewer). Studies were excluded if they reported data from acute kidney injury patients, recently hospitalised cohorts (including decompensated heart failure) or if they reported intrathoracic / segmental bioimpedance data. Citations fulfilling the inclusion criteria following abstract review then had full manuscript review by the same reviewing team, with citations being excluded if any violation of the specified exclusion criteria was found or if an English language full paper manuscript could not be sourced electronically or through external health library searches161. Individual papers were then extracted (MT all full papers, with EE, AUH, RS, MS, CS, BA, OI, JS, AMP or NW as second reviewer) using a standardised piloted template (on Microsoft Excel), based on the principles outlined by Riley et al. 2019 (CHARMS-PF162, which included assessments for the risk of bias (ROB). No a-priori assumptions were made about data quality during data extraction. If disagreements between two reviewers could not be resolved following discussion, then adjudication was sought by a third reviewer (SJD).
Risk of bias (ROB) assessment
The Quality in Prognostic Studies (QUIPS)153 tool, a validated assessment method used in a previous meta-analysis of bioimpedance defined overhydration, was employed to assess for ROB5. QUIPS uses six separate domains (participation, attrition, prognostic factor measurement, outcome measurement, confounding and statistical analyses), with each domain containing a series of signalling items that assist the reviewer in determining the ROB for each domain. Full details of how the QUIPS tool was operationalised in this review can be found in Supplementary Table 9.
Narrative review method
Study characteristics, demographics, whole body BI-MM methods, outcomes and methods for reporting estimates of effect were systematically described separately for both the kidney disease and heart failure studies. BI measurement method was characterised by the timing of the BI measurement, the device used (along with the frequency used to determine the reading) and the method itself: single-frequency methods including phase angle (PA), fat free mass (FFM) or bioimpedance vector analysis (BIVA), with multi-frequency methods including impedance ratio (IR), lean tissue / body mass estimation (LTM / LBM, expressed as absolute values or indexed to the square of the height) and body cell mass estimation (BCM, expressed as absolute values or indexed to the square of the height), as previously reported5,163. Estimates of effect, when reported using both unadjusted and adjusted analyses, were compared to assess the consistency of these estimates when adjusting for the effect of multimorbidity.
Statistical analysis and meta-analysis
Where studies had sufficient homogeneity within study reporting, including in the reported BI-MM methods, they were considered suitable for quantitative pooling. Where more than one study reported on outcomes from the same patient cohort with the same BI-MM measure, careful consideration was given to the survival analysis method, the number of events reported and the duration of the follow up period when choosing to include the study in the meta-analysis (Supplementary Table 1). Separate analyses were performed for studies reporting unadjusted and adjusted analyses, and additionally, where time-varying analyses were identified, these were analysed separately from non-time varying analyses. For studies reporting PA as a continuous variable, the effect of PA was expressed for a 1-degree decrease in PA. Random effects meta-analysis using the restricted maximum likelihood (REML) estimation, along with the calculation of two separate statistics used to assess heterogeneity within meta-analyses (I2 and Tau2), were performed using STATA SE 16.2. Funnel plots were used to assess symmetry of distribution around the pooled estimate of effect to potentially identify publication bias. Leave one out meta-analysis was used to assess the robustness of pooled estimates when removing individual studies. Confidence and prediction intervals are reported, allowing for more informative inferences to be made from the meta-analysis164. Prediction intervals are a useful measure of uncertainty for meta-analyses that capture the likely effect size of a new (similar) study based on the included studies. In comparison, confidence intervals reflect the uncertainty around the point estimate, but provide an incomplete summary of the underlying heterogeneity in the meta-analysis164.
Data availability
The datasets generated for this study are available from the corresponding author on reasonable request.
References
Hanna, R. M. et al. A practical approach to Nutrition, Protein-Energy Wasting, Sarcopenia, and cachexia in patients with chronic kidney disease. Blood Purif. 49 (1–2), 202–211 (2020).
Carrero, J. J. et al. Global prevalence of Protein-Energy wasting in kidney disease: A Meta-analysis of contemporary observational studies from the international society of renal nutrition and metabolism. J. Ren. Nutr. 28 (6), 380–392 (2018).
Hawthorne, G. et al. Multimorbidity prevalence and patterns in chronic kidney disease: findings from an observational multicentre UK cohort study. Int. Urol. Nephrol. 55 (8), 2047–2057 (2023).
Broers, N. J. H. et al. Three compartment bioimpedance spectroscopy in the nutritional assessment and the outcome of patients with advanced or end stage kidney disease: what have we learned so far? Hemodial. Int. Int. Symp. Home Hemodial. 24 (2), 148–161 (2020).
Tabinor, M. et al. Bioimpedance-defined overhydration predicts survival in end stage kidney failure (ESKF): systematic review and subgroup meta-analysis. Sci. Rep., 8. (2018).
Bieger, P. et al. Association of phase angle values and sarcopenia in older patients with heart failure. Nutr. Clin. Pract. 38 (3), 672–685 (2023).
Castillo-Martinez, L. et al. Cachexia assessed by bioimpedance vector analysis as a prognostic indicator in chronic stable heart failure patients. Nutrition 28 (9), 886–891 (2012).
Colin-Ramirez, E. et al. Bioelectrical impedance phase angle as a prognostic marker in chronic heart failure. Nutrition 28 (9), 901–905 (2012).
Colin-Ramirez, E. et al. Malnutrition syndrome, but not body mass index, is associated to worse prognosis in heart failure patients. Clin. Nutr. 30 (6), 753–758 (2011).
Doesch, C. et al. Bioimpedance analysis parameters and epicardial adipose tissue assessed by cardiac magnetic resonance imaging in patients with heart failure. Obesity 18 (12), 2326–2332 (2010).
dos Santos, J. J. A. Quality of life and clinical indicators in heart failure: a multivariate analysis. Arq. Bras. Cardiol. 93 (2), 149–156 (2009).
Futter, J. E., Cleland, J. G. F. & Clark, A. L. Body mass indices and outcome in patients with chronic heart failure. Eur. J. Heart Fail. 13 (2), 207–213 (2011).
Orea-Tejeda, A. et al. Prognostic value of cardiac troponin T elevation is independent of renal function and clinical findings in heart failure patients. Cardiol. J. 17 (1), 42–48 (2010).
Sobieszek, G. et al. Soluble ST2 proteins in male cachectic patients with chronic heart failure. Nutr. Metab. Cardiovasc. Dis. 31 (3), 886–893 (2021).
Abad, S. et al. The phase angle of the electrical impedance is a predictor of long-term survival in Dialysis patients. Nefrologia 31 (6), 670–676 (2011).
Abdulan, I. M. et al. The predictive value of malnutrition for functional and cognitive status in elderly Hemodialysis patients. Int. Urol. Nephrol. 51 (1), 155–162 (2019).
Antunes, A. A. et al. Influence of protein intake and muscle mass on survival in chronic Dialysis patients. Ren. Fail. 32 (9), 1055–1059 (2010).
Antunes, A. D. et al. Associations between bioelectrical impedance parameters and cardiovascular events in chronic Dialysis patients. Int. Urol. Nephrol. 45 (5), 1397–1403 (2013).
Avram, M. M. et al. Extracellular mass/body cell mass ratio is an independent predictor of survival in peritoneal Dialysis patients. Kidney Int. 78 (SUPPL. 117), S37–S40 (2010).
Avram, M. M. et al. Malnutrition and inflammation as predictors of mortality in peritoneal Dialysis patients. Kidney Int. 70 (SUPPL. 104), S4–S7 (2006).
Bae, E. et al. Impact of phase angle and sarcopenia estimated by bioimpedance analysis on clinical prognosis in patients undergoing hemodialysis: A retrospective study. Medicine 101 (25), e29375 (2022).
Barra, A. B. L. et al. Characteristics and predictors of mortality on haemodialysis in brazil: a cohort of 5,081 incident patients. BMC Nephrol. 23 (1), 77 (2022).
Basile, C. et al. Comparison of alternative methods for scaling Dialysis dose. Nephrol. Dialysis Transplantation. 25 (4), 1232–1239 (2010).
Beberashvili, I. et al. Longitudinal changes in bioimpedance phase angle reflect inverse changes in serum IL-6 levels in maintenance Hemodialysis patients. Nutr. (Burbank Los Angeles Cty. Calif). 30 (3), 297–304 (2014).
Beberashvili, I. et al. Objective score of nutrition on Dialysis (OSND) as an alternative for the malnutrition-inflammation score in assessment of nutritional risk of haemodialysis patients. Nephrol. Dialysis Transplantation. 25 (8), 2662–2671 (2010).
Beberashvili, I. et al. IL-6 levels, nutritional status, and mortality in prevalent Hemodialysis patients. Clin. J. Am. Soc. Nephrol. 6 (9), 2253–2263 (2011).
Beberashvili, I. et al. Interaction between acyl-ghrelin and BMI predicts clinical outcomes in Hemodialysis patients. BMC Nephrol. 18, 1–10 (2017).
Beberashvilil, I. et al. Bioimpedance phase angle predicts muscle function, quality of life and clinical outcome in maintenance hemodialysis patients. Eur. J. Clin. Nutr. 68, 683–689 (2014).
Brito, C. P. et al. Relationship of phase angle and peak torque of knee extensors with the performance in six-minute step test in haemodialysis patients. BMC Nephrol. 22 (1), 56 (2021).
Caetano, C. et al. Body composition and mortality predictors in Hemodialysis patients. J. Ren. Nutr. 26 (2), 81–86 (2016).
Canaud, B. et al. Clinical and predictive value of simplified creatinine index used as muscle mass surrogate in end-stage kidney disease haemodialysis patients-results from the international monitoring Dialysis outcome initiative. Nephrol. Dialysis Transplantation. 35 (12), 2161–2171 (2021).
Castellano, S. et al. Appropriate assessment of body composition to identify haemodialysis patients at risk. Nefrologia 36 (3), 268–274 (2016).
Chan, G. C. K. et al. Adipose and serum zinc alpha-2-glycoprotein (ZAG) expressions predict longitudinal change of adiposity, wasting and predict survival in Dialysis patients. Sci. Rep. 12 (1), 9087 (2022).
Chaudhuri, S. et al. Predicting mortality risk in dialysis: assessment of risk factors using traditional and advanced modeling techniques within the monitoring Dialysis outcomes initiative. Hemodial. Int. 27 (1), 62–73 (2023).
Cheng, L. et al. The predictive value of bioimpedance-derived fluid parameters for cardiovascular events in patients undergoing Hemodialysis. Ren. Fail. 44 (1), 1192–1200 (2022).
Chertow, G. M. et al. Phase angle predicts survival in Hemodialysis patients. J. Ren. Nutr. 7 (4), 204–207 (1997).
De Oliveira, C. M. C. et al. Adductor pollicis muscle thickness: A promising anthropometric parameter for patients with chronic renal failure. J. Ren. Nutr. 22 (3), 307–316 (2012).
Dekker, M. J. E. et al. Interactions between Malnutrition, Inflammation, and fluid overload and their associations with survival in prevalent Hemodialysis patients. J. Ren. Nutrition: Official J. Council Ren. Nutr. Natl. Kidney Foundation. 28 (6), 435–444 (2018).
Dekker, M. J. E. et al. Unraveling the relationship between mortality, hyponatremia, inflammation and malnutrition in Hemodialysis patients: results from the international MONDO initiative. Eur. J. Clin. Nutr. 70 (7), 779–784 (2016).
Delgado, C. et al. Longitudinal assessment of body composition and its association with survival among participants of the ACTIVE/ADIPOSE study. J. Ren. Nutrition: Official J. Council Ren. Nutr. Natl. Kidney Foundation. 32 (4), 396–404 (2022).
Demirci, C. et al. Impedance ratio: a novel marker and a powerful predictor of mortality in Hemodialysis patients. Int. Urol. Nephrol. 48 (7), 1155–1162 (2016).
Di Iorio, B. et al. Charlson comorbidity index is a predictor of outcomes in incident Hemodialysis patients and correlates with phase angle and hospitalization. Int. J. Artif. Organs. 27 (4), 330–336 (2004).
Dong, J. et al. Correlations of lean body mass with nutritional indicators and mortality in patients on peritoneal Dialysis. Kidney Int. 73 (3), 334–340 (2008).
Elder, M. et al. Chronic kidney disease-related sarcopenia as a prognostic indicator in elderly haemodialysis patients. BMC Nephrol. 24 (1). (2023).
Fein, PA. et al. Usefulness of bioelectrical impedance analysis in monitoring nutrition status and survival of peritoneal Dialysis patients. Adv. Perit. Dial. 18, p195–199 (2002). Conference on Peritoneal Dialysis.
Fiedler, R. et al. Clinical nutrition scores are superior for the prognosis of haemodialysis patients compared to lab markers and bioelectrical impedance. Nephrol. Dialysis Transplantation. 24 (12), 3812–3817 (2009).
Filipcic, T. et al. Physical activity and quality of life in Hemodialysis patients and healthy controls: a cross-sectional study. Int. J. Environ. Res. Public Health 18 (4). (2021).
Gadaen, R. J. R. et al. The effects of chronic Dialysis on physical Status, quality of Life, and arterial stiffness: A longitudinal study in prevalent Dialysis patients. Nephron 145 (1), 44–54 (2021).
Garagarza, C. et al. Hypophosphatemia: nutritional status, body composition, and mortality in Hemodialysis patients. Int. Urol. Nephrol. 49 (7), 1243–1250 (2017).
Gracia-Iguacel, C. et al. Low intracellular water, overhydration, and mortality in hemodialysis patients. J. Clin. Med. 9 (11). (2020).
Hoppe, K. et al. Dialysis vintage stratified comparison of body composition, hydration and nutritional state in peritoneal Dialysis and Hemodialysis patients. Archives Med. Sci. 14 (4), 807–817 (2018).
Huang, R. et al. Lower phase angle measured by bioelectrical impedance analysis is a marker for increased mortality in incident continuous ambulatory peritoneal Dialysis patients. J. Ren. Nutr. 30 (2), 119–125 (2020).
Hur, E. et al. New method to predict survival in Hemodialysis patients using the impedance ratio. Turkish J. Nephrol. 28 (1), 24–29 (2019).
Ikizler, T. A. et al. Association of morbidity with markers of nutrition and inflammation in chronic Hemodialysis patients: a prospective study. Kidney Int. 55 (5), 1945–1951 (1999).
Kang, S. H., Do, J. Y. & Kim, J. C. Impedance-derived phase angle is associated with muscle mass, strength, quality of life, and clinical outcomes in maintenance Hemodialysis patients. PLoS One. 17 (1 January), e0261070 (2022).
Kaysen, G. A. et al. Baseline physical performance, health, and functioning of participants in the frequent Hemodialysis network (FHN) trial. Am. J. Kidney Dis. 57 (1), 101–112 (2011).
Keane, D. et al. Changes in body composition in the two years after initiation of haemodialysis: A retrospective cohort study. Nutrients 8 (11). (2016).
Kim, C. et al. Longitudinal changes in body composition are associated with all-cause mortality in patients on peritoneal Dialysis. Clin. Nutr. 40 (1), 120–126 (2021).
Kim, J. K. et al. Prevalence of and factors associated with sarcopenia in elderly patients with end-stage renal disease. Clin. Nutr. 33 (1), 64–68 (2014).
Kim, J. K. et al. Impact of sarcopenia on long-term mortality and cardiovascular events in patients undergoing Hemodialysis. Korean J. Intern. Med. 34 (3), 599–607 (2019).
Kittiskulnam, P. et al. Sarcopenia and its individual criteria are associated, in part, with mortality among patients on Hemodialysis. Kidney Int. 92 (1), 238–247 (2017).
Kittiskulnam, P. et al. Protein-Energy wasting and mortality risk prediction among peritoneal Dialysis patients. J. Ren. Nutr. 31 (6), 679–686 (2021).
Kittiskulnam, P. et al. Association analysis of body composition with survival among prevalent peritoneal Dialysis patients. Int. Urol. Nephrol. 54 (2), 437–446 (2022).
Koh, K. H. et al. Normalized bioimpedance indices are better predictors of outcome in peritoneal Dialysis patients. Perit. Dial. Int. 31 (5), 574–582 (2011).
Lee, H. S. et al. Fat-to-Lean mass ratio can predict cardiac events and All-Cause mortality in patients undergoing Hemodialysis. Ann. Nutr. Metab. 73 (3), 241–249 (2018).
Li, F. et al. Established risk prediction models for the incidence of a low lean tissue index in patients with peritoneal dialysis. Ren. Fail. 44 (1), 1417–1425 (2022).
Lim, Y. et al. Association between ultrafiltration rate and clinical outcome is modified by muscle mass in Hemodialysis patients. Nephron 144 (9), 447–452 (2020).
Lin, Y. L. et al. Impact of sarcopenia and its diagnostic criteria on hospitalization and mortality in chronic Hemodialysis patients: A 3-year longitudinal study. J. Formos. Med. Assoc. 119 (7), 1219–1229 (2020).
Maggiore, Q. et al. Nutritional and prognostic correlates of bioimpedance indexes in Hemodialysis patients. Kidney Int. 50 (6), 2103–2108 (1996).
Marcelli, D. et al. Body composition and survival in Dialysis patients: results from an international cohort study. Clin. J. Am. Soc. Nephrol. 10 (7), 1192–1200 (2015).
Mizuiri, S. et al. Relationship of serum magnesium level with body composition and survival in Hemodialysis patients. Hemodial. Int. 24 (1), 99–107 (2020).
Mok, N. M. Y. et al. Relationship between sodium removal, hydration and outcomes in peritoneal Dialysis patients. Nephrology 26 (8), 676–683 (2021).
Mushnick, R. et al. Relationship of bioelectrical impedance parameters to nutrition and survival in peritoneal Dialysis patients. Kidney Int. 64, S53–S56 (2003).
Muzasti, R. A. & Lubis, H. R. Association of phase angle on bioelectrical impedance analysis and dialysis frequency with survival of chronic hemodialysis patients. In 1st Int Conf On Trop Med & Infect Dis Fac Of Med Univ Sumatera Utara In Conjunction With The 23rd Natl Congress Of The Indonesian Soc Of Trop & Infect Dis Consultant And The 18th Annual Meeting Of Internal Med Dept Fac Of Med Univ Sumatera Utara. (2018).
Nagy, E. et al. Impact of malnutrition on health-related quality of life in patients on maintenance Hemodialysis. Therapeut. Apheres. Dial. 25 (4), 467–474 (2021).
Ng, H. M. et al. Is malnutrition a determining factor of health-related quality of life in Hemodialysis patients? A cross-sectional design examining relationships with a comprehensive assessment of nutritional status. Qual. Life Res. Int. J. Qual. Life Aspects Treat. Care Rehabilit. 31 (5), 1441–1459 (2022).
Noori, N. et al. Frailty and the quality of life in Hemodialysis patients: the importance of waist circumference. J. Ren. Nutr. 28 (2), 101–109 (2018).
Nowicka, M. et al. Association of physical Performance, muscle strength and body composition with Self-Assessed quality of life in hemodialyzed patients: A Cross-Sectional study. J. Clin. Med. 11 (9), 2283 (2022).
Nugroho, P. et al. Correlation of body composition and quality of life in maintenance Hemodialysis patients. Nephro-Urol. Monthly 14 (4), e129587 (2022).
Oliveira, C. M. C. et al. Depression in Dialysis patients and its association with nutritional markers and quality of life. J. Nephrol. 25 (6), 954–961 (2012).
Oliveira, T. et al. Low body cell mass index in Hemodialysis patients: association with clinical parameters and survival. Hemodial. Int. 24 (2), 228–236 (2020).
Parthasarathy, R., Oei, E. & Fan, S. L. Clinical value of body composition monitor to evaluate lean and fat tissue mass in peritoneal Dialysis. Eur. J. Clin. Nutr. 73 (11), 1520–1528 (2019).
Paudel, K. et al. Can bioimpedance measurements of lean and fat tissue mass replace subjective global assessments in peritoneal Dialysis patients? J. Ren. Nutr. 25 (6), 480–487 (2015).
Pillon, L. et al. Vector length as a proxy for the adequacy of ultrafiltration in Hemodialysis. Kidney Int. 66 (3), 1266–1271 (2004).
Pupim, L. B. et al. Uremic malnutrition is a predictor of death independent of inflammatory status. Kidney Int. 66 (5), 2054–2060 (2004).
Qin, Z. et al. Serum leptin concentration can predict cardiovascular outcomes and all-cause death in maintenance Hemodialysis patients. Clin. Chim. Acta. 520, 87–94 (2021).
Ren, H. et al. Sarcopenia in patients undergoing maintenance hemodialysis: incidence rate, risk factors and its effect on survival risk. Ren. Fail. 38 (3), 364–371 (2016).
Rosenberger, J. et al. Malnutrition in haemodialysis patients assessed by body composition monitor. Nephrol. Dialysis Transplant. 29 (SUPPL. 3), iii289 (2014).
Ruperto, M. & Barril, G. The extracellular mass to body cell mass ratio as a predictor of mortality risk in Hemodialysis patients. Nutrients 14 (8). (2022).
Rymarz, A. et al. Low lean tissue mass can be a predictor of one-year survival in Hemodialysis patients. Ren. Fail. 40 (1), 231–237 (2018).
Saitoh, M. et al. Bioelectrical impedance analysis-derived phase angle as a determinant of protein-energy wasting and frailty in maintenance Hemodialysis patients: retrospective cohort study. BMC Nephrol. 21 (1), 438 (2020).
Schwermer, K. et al. N-terminal pro-B-type natriuretic peptide as a marker of hypervolemia and predictor of increased mortality in patients on Hemodialysis. Pol. Arch. Med. Wewn. 125 (7–8), 560–569 (2015).
Segall, L. et al. Nutritional status evaluation and survival in haemodialysis patients in one centre from Romania. Nephrol. Dialysis Transplantation. 24 (8), 2536–2540 (2009).
Segall, L. et al. Protein-energy wasting, as well as overweight and obesity, is a long-term risk factor for mortality in chronic Hemodialysis patients. Int. Urol. Nephrol. 46 (3), 615–621 (2014).
Shin, J. H. et al. Predicting clinical outcomes using phase angle as assessed by bioelectrical impedance analysis in maintenance Hemodialysis patients. Nutrition 41, 7–13 (2017).
Song, Y. R. et al. Serum levels of protein carbonyl, a marker of oxidative stress, are associated with overhydration, sarcopenia and mortality in Hemodialysis patients. BMC Nephrol. 21 (1), 281 (2020).
Souweine, J. S. et al. Dynapaenia and sarcopaenia in chronic haemodialysis patients: do muscle weakness and atrophy similarly influence poor outcome? Nephrol. Dialysis Transplantation. 36 (10), 1908–1918 (2021).
Szuck, P. et al. Association between nutritional indicators and risk of hospitalization among Hemodialysis patients. Revista De Nutricao-Brazilian J. Nutr. 29 (3), 317–327 (2016).
Tabibi, H. et al. Associations of body Composition, muscle Function, and physical activity with mortality in peritoneal Dialysis patients. Iran. J. Kidney Dis. 14 (3), 224–230 (2020).
Valente, A. et al. Evaluating haemodialysis patient’s nutritional status: body mass index or body cell mass index? Nephrology 24 (9), 967–974 (2019).
Verger, C. et al. Association of prescription with body composition and patient outcomes in incident peritoneal dialysis patients. Front. Med., 8. (2021).
Wang, K. et al. Body composition changes following Dialysis initiation and cardiovascular and mortality outcomes in CRIC (Chronic renal insufficiency Cohort): A bioimpedance analysis substudy. Kidney Med. 3 (3), 327–334e1 (2021).
Wu, H. C. et al. The association between serum testosterone and mortality among elderly men on Hemodialysis. J. Clin. Lab. Anal. 32 (5), 1–1 (2018).
Wu, H. C. et al. Association between obesity with low muscle mass and Dialysis mortality. Intern. Med. J. 47 (11), 1282–1291 (2017).
Xiong, Y. et al. Visceral fat area is a better predictor than coronary artery calcification score for cardiovascular outcomes and All-Cause death in patients on Hemodialysis. J. Ren. Nutr. pp. 306–312. (2021).
Yajima, T. et al. The associations of fat tissue and muscle mass indices with all-cause mortality in patients undergoing Hemodialysis. PLoS One 14 (2). (2019).
Yaprak, B., Arslan, N. & Alatas, H. Multiple factors influencing mortality in Hemodialysis patients. Eur. Rev. Med. Pharmacol. Sci. 23 (5), 1095–1103 (2023).
Yavuz, Y. C. et al. SARC-F is a weaker predictor compared to muscle strength and a stronger predictor compared to muscle mass for mortality and hospitalization in Hemodialysis patients. Turkish J. Nephrol. 31 (4), 314–320 (2022).
Zavacka, M. et al. Vascular access as a survival factor for the Hemodialysis population: a retrospective study. Int. Angiol. 39 (6), 525–531 (2020).
Zha, Y. et al. Muscle strength performed better than muscle mass in identifying cognitive impairment risk in maintenance Hemodialysis patients. Eat. Weight Disord. Stud. Anorexia Bulimia Obes. 27 (7), 2533–2540 (2022).
Zhang, H. F. et al. Evaluation of body composition monitoring for assessment of nutritional status in Hemodialysis patients. Ren. Fail. 41 (1), 377–383 (2019).
Delgado, C., Doyle, J. W. & Johansen, K. L. Association of frailty with body composition among patients on Hemodialysis. J. Ren. Nutr. 23 (5), 356–362 (2013).
Akin, S. et al. Cut-Off values for sarcopenia and mortality risk in older Dialysis patients. J. Clin. Pract. Res. 47 (3), 272 (2025).
Borges, S. et al. Performance of SARC-F and SARC-CalF scores to predict risk of mortality in Hemodialysis patients: a cohort study. Sci. Rep. 14 (1), 23262 (2024).
Cheng, L. et al. Association of changes in body composition with all-cause mortality in patients undergoing hemodialysis: A prospective cohort study. Nutrition 128, 112566 (2024).
Chiu, L. T. et al. Association of serum fibroblast growth factor 21 levels with skeletal muscle mass and mortality in chronic Hemodialysis patients. J. Formos. Med. Assoc. 121 (12), 2481–2489 (2022).
Gan, W. Y. et al. Association between serum uric acid and all-cause and cardiovascular-related mortality in Hemodialysis patients. Front. Nutr., 11. (2024).
Li, J. H. et al. Association between disability in activities of daily living and phase angle in Hemodialysis patients. BMC Nephrol. 24 (1). (2023).
Park, K. et al. Impact of handgrip strength on survival in Hemodialysis patients. Diagnostics 15 (1), 75 (2025).
Saez, A. L. et al. Influence of albumin and phase angle on the survival of patients with chronic kidney disease on hemodialysis: a prospective study. J. Brasileiro De Nefrol. 47 (4), e20240207 (2025).
Than, W. H. et al. Plasma Vaspin levels and clinical outcome in incident peritoneal Dialysis patients. BMC Nephrol. 24 (1), 206 (2023).
Tian, M. et al. Low lean tissue index and muscle strength combined with high fat tissue index are associated with cardiovascular Disease-Related hospitalisation in patients on haemodialysis. Cardiorenal Med. 13 (1), 363–371 (2023).
Tian, M. et al. Lean-to-fat tissue ratio as a risk factor for cognitive impairment in patients undergoing maintenance Hemodialysis. J. Psychosom. Res. 174, 111464 (2023).
Tian, M. et al. Low intracellular water and incident cognitive impairment in chronic Hemodialysis patients. Int. J. Geriatr. Psychiatry. 38 (10), 1–8 (2023).
Wang, L. et al. Association between cognitive function and skeletal muscle in patients undergoing maintenance Hemodialysis. Front. Endocrinol. 15, 1324867 (2024).
Xu, L. X. et al. Early change in lean tissue mass after peritoneal dialysis: prevalence, risk factors, and clinical implications. BMC Nephrol. 26 (1). (2025).
Xu, Y. et al. The ability of phase angle and body composition to predict risk of death in maintenance Hemodialysis patients. Int. Urol. Nephrol. 56 (2), 731–737 (2024).
Yang, Y. et al. Bioelectrical impedance phase angle combined with physical function predicts pre-frailty in maintenance Hemodialysis patients: a prospective study. BMC Nephrol. 25 (1), 1–9 (2024).
Bansal, N. et al. Bioelectrical impedance analysis measures and clinical outcomes in CKD. Am. J. Kidney Dis. 72 (5), 662–672 (2018).
Barril, G. et al. Nutritional predictors of mortality after 10 years of Follow-Up in patients with chronic kidney disease at a multidisciplinary unit of advanced chronic kidney disease. Nutrients 14 (18), 3848 (2022).
Caravaca, F. et al. Hydration status assessment by multi-frequency bioimpedance in patients with advanced chronic kidney disease. Nefrologia 31 (5), 537–544 (2011).
D’Alessandro, C. et al. Nutritional aspects in diabetic CKD patients on tertiary care. Medicina (Kaunas, Lithuania), 55 (8). (2019).
Harhay, M. N. et al. Obesity weight loss phenotypes in CKD: Findings from the chronic renal insufficiency cohort study (Kidney International Reports, 2023).
Kruse, N. T. et al. Association of skeletal muscle mass, kidney disease and mortality in older men and women: the cardiovascular health study. Aging 12 (21), 21023–21036 (2020).
Lin, T. Y. et al. Body composition is associated with clinical outcomes in patients with non-dialysis-dependent chronic kidney disease. Kidney Int. 93 (3), 733–740 (2018).
Miranda Alatriste, P. V. et al. Hydration status according to impedance vectors and its association with clinical and biochemical outcomes and mortality in patients with chronic kidney disease. Estado de hidratacion Por vectores de impedancia y Su asociacion Con desenlaces clinicos, bioquimicos y Mortalidad En Pacientes Con Enfermedad renal cronica 39 (5), 1037–1046. (2022).
Pereira, R. A. et al. Sarcopenia in chronic kidney disease on Conservative therapy: prevalence and association with mortality. Nephrol. Dialysis Transplant. 30 (10), 1718–1725 (2015).
Shin, J. et al. Phase angle as a marker for muscle health and quality of life in patients with chronic kidney disease. Clin. Nutr. 41 (8), 1651–1659 (2022).
Vega, A. et al. Low lean tissue mass is an independent risk factor for mortality in patients with stages 4 and 5 non-dialysis chronic kidney disease. Clin. Kidney J. 10 (2), 170–175 (2017).
Wilson, F. P. et al. Urinary creatinine Excretion, bioelectrical impedance Analysis, and clinical outcomes in patients with CKD: the Cric study. Clin. J. Am. Soc. Nephrol. 9 (12), 2095–2103 (2014).
Tseng, P. W., Lin, T. Y. & Hung, S. C. Association of frailty with nutritional status in patients with chronic kidney disease. J. Ren. Nutr. 34 (2), 133–140 (2024).
Chan, W. et al. The associations of muscle Strength, muscle Mass, and adiposity with clinical outcomes and quality of life in prevalent kidney transplant recipients. J. Ren. Nutrition: Official J. Council Ren. Nutr. Natl. Kidney Foundat. 29 (6), 536–547 (2019).
Kaya, E. et al. Association of nutritional assessment by phase angle with mortality in kidney transplant patients in an 8-year follow-up. Progress Transplantation (Aliso Viejo Calif). 29 (4), 321–326 (2019).
Dahl, H. et al. The association of sarcopenia and central obesity with mortality risk in patients with chronic kidney Disease - a 2-Year observational study. Curr. Developments Nutr. 7 (1), 100014 (2023).
Lai, S. et al. Sarcopenia and cardiovascular risk indices in patients with chronic kidney disease on conservative and replacement therapy. Nutrition 62, 108–114 (2019).
Yongsiri, S. et al. The association between bioimpedance analysis and quality of life in pre-dialysis stage 5 chronic kidney disease, Hemodialysis and peritoneal dialysis patients. J. Med. Assoc. Thai. 97 (3), 293–299 (2014).
Barac-Nieto, M. et al. Body composition in chronic undernutrition. Am. J. Clin. Nutr. 31 (1), 23–40 (1978).
Bowden Davies, K. A. et al. Reduced physical activity in young and older adults: metabolic and musculoskeletal implications. Therapeut. Adv. Endocrinol. Metab.. 10, 2042018819888824 (2019).
Romejko, K. et al. Testosterone deficiency as one of the major endocrine disorders in chronic kidney disease. Nutrients 14 (16). (2022).
Cruz-Jentoft, A. J. et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 48 (1), 16–31 (2019).
Chamney, P. W. et al. A whole-body model to distinguish excess fluid from the hydration of major body tissues2. Am. J. Clin. Nutr. 85 (1), 80–89 (2007).
Mayne, K. J. et al. Bioimpedance indices of fluid overload and cardiorenal outcomes in heart failure and chronic kidney disease: a systematic review. J. Card. Fail. 28 (11), 1628–1641 (2022).
Hayden, J. A., Côté, P. & Bombardier, C. Evaluation of the quality of prognosis studies in systematic reviews. Ann. Intern. Med. 144 (6), 427–437 (2006).
Chan, G. C. et al. Frailty in patients on dialysis. Kidney Int. 106 (1), 35–49 (2024).
Davies, S. J. et al. Bio-impedance Spectroscopy Added To a Fluid Management Protocol Does not Improve Preservation of Residual Kidney Function in Incident Hemodialysis Patients in a Randomized Controlled Trial (Kidney international, 2023).
Greenwood, S. A. et al. Evaluating the effect of a digital health intervention to enhance physical activity in people with chronic kidney disease (Kidney BEAM): a multicentre, randomised controlled trial in the UK. Lancet Digit. Health. 6 (1), e23–e32 (2024).
Bernier-Jean, A. et al. Exercise training for adults undergoing maintenance dialysis. Cochrane Database Syst. Rev., (1). (2022).
Quint, E. E. et al. Prehabilitation in adult solid organ transplant candidates. Curr. Transplantation Rep. 10 (2), 70–82 (2023).
Moher, D. et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6 (7), e1000097 (2009).
Ouzzani, M. H., Fedorowicz, H. & Elmagarmid, Z. A., Rayyan — a web and mobile app for systematic reviews. Syst. Rev. 5 (210). (2016).
Nussbaumer-Streit, B. et al. Excluding non-English publications from evidence-syntheses did not change conclusions: a meta-epidemiological study. J. Clin. Epidemiol. 118, 42–54 (2020).
Riley, R. D. et al. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ 364, k4597 (2019).
Tabinor, M. & Davies, S. J. The use of bioimpedance spectroscopy to guide fluid management in patients receiving Dialysis. Curr. Opin. Nephrol. Hypertens. 27 (6), 406–412 (2018).
IntHout, J. et al. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open. 6 (7), e010247 (2016).
Funding
This research was made possible, in part, through funding from the North Staffordshire Medical Institute.
Author information
Authors and Affiliations
Contributions
MT, SJD, IST, CJF and JB were all involved with the inception of the study. MT, EE, CS, NW, AUH, RS, MS, AMP, JP, BA, OI and JS were all involved in citation review and data extraction (as described in methods). MT compiled the final narrative review, meta-analysis and wrote up the manuscript. MT, SJD, IST, OI and CJF were all involved in editing the manuscript prior to submission. All authors reviewed the manuscript prior to submission.
Corresponding author
Ethics declarations
Competing interests
MT has received honoraria from Bayer and Vantive. SJD has received honoraria from Baxter HealthCare and Fresenius Medical Care, and is on the steering group for the Behring CSL300_2301 POSIBIL₆ESKD trial. All other authors have nothing to declare.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tabinor, M., Elphick, E., Stephens, C. et al. Lean tissue mass is associated with adverse outcomes across different stages of chronic kidney disease: a systematic review and meta-analysis. Sci Rep 16, 4011 (2026). https://doi.org/10.1038/s41598-025-34111-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-34111-2
