
Abstract
Vaccination is a crucial public health intervention that reduces both morbidity and mortality globally. This study aims to assess and compare the vaccination coverage rates for routine childhood immunizations across different Lebanese governorates between 2011 and 2018. This is a retrospective secondary analysis. It incorporates vaccination data of 67,000 children (aged 0–18 years) documented by the “Health Society”, a prominent non-governmental organization, during its ‘Immunization’ project that aimed to improve childhood immunization in Lebanon. The project was carried out under three successive phases: Household Survey and Referral phase (2011–2014), Mobile Vaccination Clinics phase (2015), and Integrated Referral and Mobile Vaccination phase (2016–2018). Vaccination coverage rates for routine childhood immunizations were calculated for each governorate. Comparative analyses using SPSS V26 were performed to identify variations in vaccination rates across different governorates. Vaccination coverage rates demonstrated significant variability across Lebanese governorates and throughout the study period. In 2011, the average vaccination coverage was 51.2%. By 2018, coverage had dropped sharply to 13.1%. Mount Lebanon recorded the highest coverage during the study period, reaching 57%. In contrast, the South governorate showed a steady decline in coverage from 64.1% in 2011 to 10.5% in 2017. By the time coverage in the South reached 12.6% in the final year, the governorate had already experienced several years of very low coverage. These results highlight concerning trends in vaccination coverage, particularly in the South governorate, emphasizing the need for targeted interventions. This study highlights disparities in childhood vaccination coverage across Lebanese governorates. These findings underscore the need for targeted interventions and public health strategies that improve vaccination rates and ensure equitable access to immunization services.
Similar content being viewed by others


Introduction
Vaccination is one of the most effective ways to prevent diseases and save lives1. In Lebanon, a small country in the Middle East, childhood vaccines are provided by both public and private healthcare centers, including more than 700 primary health clinics2. Around 90% of Lebanese children receive their required vaccines3. However, since 2011, the large number of Syrian refugees in Lebanon has made vaccination programs more difficult—about half of Syrian children in Lebanon do not get al.l their needed vaccines4.
Additionally, the Lebanese Ministry of Public Health reported a 10% decline in coverage for key vaccines (OPV3, PENTA3, and MCV1) between 2012 and 2015 among the Lebanese population, including Syrian and Palestinian refugees5. During the same period, DPT3 coverage in Lebanon was approximately 90% according to world health organization (WHO) estimates report6. This has led to outbreaks of preventable diseases like measles, hepatitis A, and others7. To address this, Lebanon’s Expanded Program on Immunization (EPI) aims to increase vaccination coverage in all areas to over 95%, keep Lebanon free from polio, and Eliminate measles and rubella8.
There are several studies on vaccine delays and dropout rates in Lebanon. A 2016 survey highlighted substantial variability in vaccination coverage among children aged 12–59 months, with national coverage below the targeted 95%9. A 2018 study found that some parents’ lack of knowledge about vaccines and schedules led to delays in vaccination10. The same study showed that Lebanese children had higher vaccination rates and better on-time vaccination compared to Syrian children10. So far, no large nationwide study has examined children vaccination coverage across different regions in Lebanon.
Understanding the dynamics of vaccination coverage is paramount for public health planning and disease prevention, especially in a context as volatile as Lebanon. Therefore, this study aims to estimate the vaccination coverage and dropout rates for all vaccines mandated by the Ministry of Public Health in Lebanon among the Lebanese population (aged 0–18 years) across several Lebanese governorates, through secondary analysis on data collected between 2011 and 2018.
Methods
Study design and population
This study is a retrospective cross-sectional that examined epidemiological data over five years between January 2011 to September 2018 across four Lebanese governorates (Mont Lebanon, South Lebanon, Nabatieh, Baablbeck-Hemel).
Procedures
This secondary analysis utilized data from the ‘Immunization’ project, a community-based initiative conducted by the “Health Society”, a major non-governmental organization in Lebanon, from 2011 to 2018. The project aimed to assess vaccination coverage among children aged 0–18 years in different Lebanese Governorates. The project evolved through three distinct phases (Fig. 1):
-
Phase 1 Household Survey and Referral (2011–2014):
A trained team of volunteers conducted door-to-door surveys in targeted residential areas to collect household demographics, presence of children, and vaccination status.Data collection was conducted through a house-to-house survey implemented in coordination with local mayors. All neighborhoods within each district were systematically visited, and every household encountered during fieldwork was approached for inclusion. As such, the survey covered the entire district without the use of sampling procedures. Vaccination status was determined through parental report and verification of vaccination cards, with coverage rates calculated based on well-documented vaccination records. Children with incomplete vaccinations or lacking vaccination cards were classified as ‘dropouts’ and referred to affiliated primary healthcare centers for free vaccination.
-
Phase 2 Mobile Vaccination Clinics (2015):
Following limited referral uptake in the initial phase, the project adapted its strategy by implementing mobile vaccination clinics. Children identified between 2011 and 2014 as unvaccinated were immediately referred to nearby primary healthcare centers offering free immunization, and families received repeated reminders to complete the vaccination schedule. In 2015, the strategy shifted to broaden the outreach to additional households. The children targeted during the 2015 phase were those who had not responded to earlier invitations to attend the health centers for vaccination. The mobile clinics were strategically located within communities to enhance accessibility and improve vaccination rates among the target population.
-
Phase 3 Integrated Referral and Mobile Vaccination (2016–2018)
Phase 3 implemented a combined approach integrating both referrals and mobile vaccination clinics to optimize vaccination rates. Following household surveys, families were provided with referrals to primary healthcare centers alongside schedules and locations for conveniently timed mobile vaccination clinics, operating during weekends and afternoons. At the mobile clinics, a pediatrician conducted pre-vaccination assessments, and vaccination cards were issued upon completion of immunization.
Fig. 1 Immunization Project Phases (2011–2018).

Variables
-
Vaccination Coverage Rate: (Number of vaccinated children / Number of surveyed children) x 100%11.
-
Vaccination Non-Coverage Rate: Vaccination non-coverage was defined as the absence of one or more age-appropriate routine vaccinations according to the Lebanese national immunization schedule at the time of data collection.
-
Catch-Up Vaccination Rate: (Number of children vaccinated after initially missing / Number of children who initially missed) x 100%12.
-
Overall Vaccination Coverage: recalculate the overall vaccination coverage rate after the catch-up campaign13.
Statistical analysis
Continuous variables were presented as mean ± standard deviation, median (range), while categorical variables were described as frequencies and percentages. Comparisons between groups were conducted using Pearson chi-square tests and Fisher’s exact test for categorical variables and Student’s t-tests and ANOVA for continuous variables.
All statistical tests conducted in the study were two-sided, with statistical significance defined as a p-value < 0.05. Data collection and analysis were performed using the Statistical Package for Social Sciences (SPSS) software, version 26.
Ethical aspects
This study is a secondary analysis of publicly available, aggregated, and anonymized national data, involving no human participants or identifiable private information. According to Lebanese national regulations, specifically the Ministry of Public Health Circular No. 117/2015/2016 (‘Regulating Scientific Health Research on Human Subjects in Lebanon’), formal Institutional Review Board (IRB) approval is mandated for research involving human subjects or identifiable data14. As this study did not fall under this mandate, the need for ethical approval was formally waived by the Research Ethics Committee of the Health Society on January 26, 2025 (Reference: 260125-26). The research protocol was conducted in accordance with relevant ethical guidelines outlined in the Declaration of Helsinki.
Results
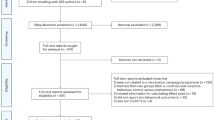
Over a seven-year period, a total of 67,776 children were assessed to identify vaccination dropout. Figure 1 illustrates the trends in vaccination coverage rates between 2011 and 2018. The data show a substantial improvement in vaccination uptake in the early part of the period. Specifically, vaccination coverage increased markedly from 26% in 2011 to over 59% in 2016. However, this progress was not sustained, as coverage declined again to 43% by 2018. A Kruskal–Wallis test confirmed that these temporal differences in vaccination coverage were statistically significant (p < 0.0001), indicating meaningful variation in coverage across the study years (Fig. 2).

Evolution of vaccination coverage rate (2011–2018); p-value of Kruskal Wallis test were presented.
Between 2011 and 2013, Nabatieh exhibited the highest rate (48.8%), followed by North (43.0%) and South (35.9%). A notable shift occurred in 2014, with Mount Lebanon displaying the highest non-coverage (80.4%), followed by South (60.8%), Nabatieh (42.3%), and Baalbek-Hermel (41.5%). This pattern persisted in 2016, where Baalbek-Hermel recorded the highest rate (95.6%), followed by South (90.1%), North (87.6%), and Nabatieh (83.1%). In 2017, Baalbek-Hermel remained high (92.0%), with South (89.5%) and Nabatieh (84.6%) following. Finally, in 2018, Mount Lebanon showed the highest non-coverage (87.4%), closely followed by Baalbek-Hermel (85.4%) (Fig. 3).

Geographic distribution of non-coverage vaccination rate by governorate. This file is licensed under the Creative Commons Attribution 4.0 International license15.
Figure 4 presents a comparison of vaccination coverage rates across four governorates (Mont Lebanon, Nabatieh, Baalbeck-Hermel, and South) at different time points: “Before Vaccination” (referring to a baseline period, specifically 2011–2014) and “After Vaccination” (following the implementation of an Integrated Referral and Mobile Vaccination initiative for the years 2016, 2017, and 2018). In 2016, coverage increased substantially in all governorates following the intervention, rising from 12.6% to 46.4% in Mount Lebanon, from 9.8% to 58.1% in Nabatieh, from 4.4% to 63.9% in Baalbeck-Hermel, and from 16.9% to 64.4% in the South. A similar pattern was observed in 2017, with notable increases in Baalbeck-Hermel (8.0% to 63.4%) and moderate improvements in Nabatieh (15.4% to 34.2%) and the South (10.5% to 40.0%). In 2018, vaccination coverage again improved following the intervention, increasing from 12.6% to 42.3% in Mount Lebanon and from 14.6% to 46.4% in Baalbeck-Hermel (Fig. 4).

Vaccination coverage trends by governorate: before and after integrated referral and mobile vaccination
Discussion
Vaccination non-coverage rates (2011–2018) revealed not only broad disparities across the four Lebanese governorates but also important variations within them. For example, in Nabatieh governorate, certain areas such as Maroun Ras showed notably higher coverage compared to other nearby villages and towns, suggesting localized differences in health service accessibility, community engagement, and population mobility. These intra-governorate contrasts indicate that challenges in vaccine uptake are not uniformly distributed, even within the same region. In addition to geographic remoteness from primary health care centers, local socioeconomic factors, population displacement patterns, and the varying presence of community-based organizations may have contributed to these micro-level disparities4.
The data collection period (2011–2018) coincided with the height of the Syrian refugee crisis in Lebanon. Between 2011 and 2015, Lebanon hosted a total of 1,166,488 registered Syrian refugees, according to the United Nations High commissioner for Refugees (UNHCR)7. Notably, children benefiting from the ‘Immunization’ project were not limited to Lebanese nationals; Syrian children, including refugees, were also included. That is important because certain regions like Baalbeck-Hermel that experienced the highest influx of Syrian refugees, concurrently, demonstrated the highest peak in non-coverage rates, reaching 95.6% by 2016. A household survey (2015) found that only 46.5% of Syrian refugees living outside of camps in Lebanon were able to produce their children’s vaccination cards16. Moreover, when relying on routine non-campaign se12rvices, only 12.5% of Syrian children had completed their immunization schedule16. These findings reflect major challenges in obtaining routine vaccinations among Syrian refugees in Lebanon and underscore the importance of carrying vaccination campaigns. Also, despite the many campaigns carried by MOPH, vaccination coverage rates remained alarmingly low.
The high overall non-coverage rate in Lebanon may be further attributed to poor parental health literacy. A study assessing 3,500 parents in Lebanon found that higher levels of education and good parent-physician communication were associated with better vaccination practices10. Another study conducted in Lebanon showed that parents erroneously assuming their children’s vaccination status aligned with their vaccination schedule was inversely related to timely administration of vaccines17. Other factors were found to contribute to this negative association including poor maternal knowledge on immunization schedules and relying on schools and nurseries to make decisions on children’s vaccination17. A systematic review found that negative attitudes towards vaccination and incorrect beliefs on the reliability of vaccines were associated with decreased herd immunity and increased vaccine hesitancy18. These factors show the importance of educating parents on maintaining timely vaccination and good parent-physician communication, especially in developing countries such as Lebanon.
A secondary analysis done in India showed that dropout rates were higher among children of younger mothers (aged 15–19 years)19. Additionally, rural areas experienced higher drop-out rates compared to urban. Other factors were shown to contribute to higher non-coverage rate such as wealth, birth order, religion, antenatal visits, and public/private health facilities19. Lebanon is another developing country, and such factors may have played a role in the disparities recorded between different Lebanese districts.
A nationwide survey conducted by Mansour et al. in 2016, amidst the Syrian refugee crisis, assessed the immunization coverage for children aged 12–59 months. Researchers in this study found that the overall vaccination coverage rate was below 95% for any recommended last dose7. Moreover, a discrepancy was found between different Lebanese districts. For instance, Aley district (Mount Lebanon) exhibited the highest polio third dose coverage among Lebanese children at 95.5%, compared to only 61.3% coverage rate in Becharre district (North governorate)7. Furthermore, Syrian children exhibited higher dropout rates compared to Lebanese children. Dropout rates ranged between 10.2% and 23.4% among Syrian children, compared to 6.7% and 18.9% among Lebanese children7.
This is the first large-scale, multi-governorate study to assess childhood vaccination status in Lebanon. A total of 63,912 child were included across four Lebanese governorates. Only high-quality data were utilized, since only vaccination cards were approved to determine children’s vaccination status. Additionally, the study assessed vaccination status of children from ages 0 to 18 years. This broad age range means that coverage rates measured included all routine vaccinations provided in Lebanon.
Limitations to this study are primarily related to the study design. The study has a retrospective cross-sectional design. This prevents tracking changes in vaccination status for individuals over time. Moreover, it relies on secondary data, hence there is limited control over the nature and scope of information available. The absence of nationality data is particularly important, as it restricts our ability to examine associations related to refugee status or migrant populations, which may have influenced vaccination patterns in certain regions. Major gaps include lack of information on the nature of vaccines taken as well as children’s nationalities. This study did not collect detailed age-stratified vaccination data, which prevented us from conducting age-specific analyses. This limits the ability to compare vaccination gaps across specific age groups. In addition, the secondary data used did not contain sufficient variables that allow comprehensive analysis of the factors contributing to the high non-coverage rate. Furthermore, analysis was conducted in only four regions (Mount Lebanon, South Lebanon, Nabatieh, Baalbeck-Hermel), which limits the generalizability of findings to all of Lebanon.
Implications for Public Health
This study’s findings carry significant implications for public health in Lebanon, particularly highlighting the need for targeted interventions to address the concerning decline in childhood vaccination coverage.
First, community outreach programs should be adapted to local contexts to improve vaccine awareness, rebuild trust in healthcare institutions, and ensure the dissemination of accurate information. Outreach intensity and messaging should reflect local determinants of hesitancy, especially in regions reporting higher non-coverage.
Second, the Ministry of Public Health should prioritize mobile health clinics in underserved and geographically isolated governorates. These units can reduce physical and financial access barriers and play a critical role in areas where fixed PHCCs are sparse or overstretched.
Third, implementing a national digital immunization registry with automated reminders would facilitate timely vaccination nationwide while enabling subnational monitoring. Such systems are essential for PHC teams to detect and investigate high-dropout clusters at the district or municipality level.
Moreover, refugees and socioeconomically vulnerable groups, who are unevenly distributed across governorates, require targeted support to ensure equitable access to routine immunization services. Tailoring service delivery to these populations is critical for preventing localized immunity gaps that can trigger outbreaks.
Finally, further research should explore region-specific barriers to vaccination such as supply chain issues, workforce constraints, community mistrust, or transportation difficulties to guide evidence-based interventions by governmental and non-governmental stakeholders.
Conclusions
This retrospective analysis of vaccination data across Lebanese governorates from 2011 to 2018 reveals significant disparities and an overall trend of declining vaccination coverage and increasing non-coverage. While Mount Lebanon consistently exhibited the highest coverage, the South governorate experienced a particularly sharp and sustained decline. The substantial shift toward non-coverage across Lebanon by 2018 suggests challenges in maintaining routine childhood immunization. These findings indicate the need for targeted, governorate-specific interventions to address factors that may be contributing to declining vaccination rates—particularly in vulnerable regions such as the South—in order to safeguard public health and reduce the risk of outbreaks of vaccine-preventable diseases.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ANOVA:
-
One-way analysis of variance
- BMI:
-
Body Mass Index
- CI:
-
Confidence Interval
- MoPH:
-
Ministry of Public Health
- PHCC:
-
Primary health care centers
- SD:
-
Standard Deviation
- WHO:
-
World Health Organization
- UNICEF:
-
United Nations Children’s Fund
References
Nandi, A. & Shet, A. Why vaccines matter: understanding the broader health, economic, and child development benefits of routine vaccination. Hum Vaccin Immunother [Internet]. [cited 2025 Jul 2];16(8):1900–4. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7482790/
moph [Internet]. [cited 2025 Jul 2]. Available from: http://www.moph.gov.lb
Osseiran, A. et al. Using behavioral insights to increase the demand for childhood vaccination in low resource settings: Evidence from a randomized controlled trial in Lebanon. SAGE Open Med [Internet]. Oct 6 [cited 2025 Jul 2];11:20503121231199857. (2023). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10559695/
Kmeid, M., Azouri, H., Aaraj, R., Bechara, E. & Antonios, D. Vaccine coverage for Lebanese citizens and Syrian refugees in Lebanon. Int. Health. 11 (6), 568–579 (2019).
Alawieh, A. et al. Assessing the impact of the Lebanese National polio immunization campaign using a population-based computational model. BMC Public. Health. 17 (1), 902 (2017).
Immunization Lebanon country profile [Internet]. [cited 2025 Jul 3]. (2024). Available from: https://www.who.int/publications/m/item/immunization-2024-lebanon-country-profile
Mansour, Z. et al. Estimating population immunity to poliovirus in lebanon: results from a Seroprevalence survey, 2016. Vaccine 38 (31), 4846–4852 (2020).
Hammoud, S., Onchonga, D., Amer, F. & Kocsis, B. The burden of communicable diseases in lebanon: trends in the past decade. Disaster Med. Public. Health Prep. 16 (5), 1725–1727 (2022).
Mansour, Z. et al. Vaccination coverage in Lebanon following the Syrian crisis: results from the district-based immunization coverage evaluation survey 2016. BMC Public Health [Internet]. 2019 Jan 14 [cited 2023 Nov 22];19(1):58. Available from: https://doi.org/10.1186/s12889-019-6418-9
Matta, P., El Mouallem, R., Akel, M., Hallit, S. & Fadous Khalife, M. C. Parents’ knowledge, attitude and practice towards children’s vaccination in Lebanon: role of the parent-physician communication. BMC Public Health [Internet]. Sep 22 [cited 2025 Jul 2];20:1439. (2020). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7510257/
Seither, R. Coverage with Selected Vaccines and Exemption Rates Among Children in Kindergarten — United States, 2023–24 School Year. MMWR Morb Mortal Wkly Rep [Internet]. 2024 [cited 2025 Apr 8];73. Available from: https://www.cdc.gov/mmwr/volumes/73/wr/mm7341a3.htm
Manandhar, P. et al. Use of catch-up vaccinations in the second year of life (2YL) platform to close immunity gaps: A secondary DHS analysis in Pakistan, Philippines, and South Africa. Vaccine [Internet]. 2023 Jan 4 [cited 2025 Apr 8];41(1):61–7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9662756/
Mancarella, M. et al. Catch-up vaccination campaign in children between 6 and 8 years old during COVID-19 pandemic: The experience in a COVID hub in Milan, Italy. Vaccine [Internet]. 2022 Jun 9 [cited 2025 Apr 8];40(26):3664–9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9098956/
Clinical Trials [Internet]. [cited 2025 Dec 23]. Available from: http://www.moph.gov.lb/en/DynamicPages/view/4760/clinical-trial-regulations
JRC & English ECHO Lebanon BaseMap A4 Portrait [Internet]. [cited 2025 Dec 23]. (2013). Available from: https://commons.wikimedia.org/wiki/File:Lebanon_Base_Map.png
Roberton, T., Weiss, W., Jordan Health Access Study Team, Lebanon Health Access Study Team & Doocy, S. Challenges in estimating vaccine coverage in refugee and displaced populations: results from household surveys in Jordan and Lebanon. Vaccines (Basel). 5 (3), 22 (2017).
Mansour, Z. et al. Factors affecting age-appropriate timeliness of vaccination coverage among children in Lebanon. Gates Open. Res. 2, 71 (2018).
Yörük, S. & Güler, D. Factors associated with pediatric vaccine hesitancy of parents: a cross-sectional study in Turkey. Hum. Vaccin Immunother. 17 (11), 4505–4511 (2021).
Dhalaria, P. et al. Exploring the pattern of immunization dropout among children in india: A District-Level comparative analysis. Vaccines (Basel). 11 (4), 836 (2023).
Acknowledgements
Authors express their sincere gratitude to all volunteers who helped in data collection in several Lebanese regions.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization L.H, K.B, S.M, AND A.H ; methodology L.H, software R.E.H; validation S.M, A.H, AND R.E.H; formal analysis investigation S.M, A.H, AND R.E.H; resources L.H, K.B, S.M, AND A.H; data curation R.E.H writing—original draft preparation Z.H, H.F, A.B.B, M.C, AND Z.K; writing—review and editing Z.H, H.F, A.B.B, M.C, Z.K, AND R.B; visualization R.B, L.H, K.B, S.M, AND A.H; supervision R.E.H project administration L.H, K.B, S.M, AND A.H. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study is a secondary analysis of publicly available, aggregated, and anonymized national data, involving no human participants or identifiable private information. According to Lebanese national regulations, specifically the Ministry of Public Health Circular No. 117/2015/2016 (‘Regulating Scientific Health Research on Human Subjects in Lebanon’), formal Institutional Review Board (IRB) approval is mandated for research involving human subjects or identifiable data. As this study did not fall under this mandate, the need for ethical approval was formally waived by the Research Ethics Committee of the Health Society on January 26, 2025 (Reference: 260125-26). The research protocol was conducted in accordance with relevant ethical guidelines outlined in the Declaration of Helsinki.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hazime, Z., Ftouni, H., Bazzal, A.A. et al. Evolution of vaccination coverage among children in Lebanon (2011–2018): a comparative epidemiological analysis. Sci Rep 16, 4216 (2026). https://doi.org/10.1038/s41598-025-34322-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-34322-7

{kind=link}