
Abstract
To determine the correlations between six serological inflammatory markers, namely the systemic immune-inflammation index (SII), systemic inflammatory response index (SIRI), aggregate index of systemic inflammation (AISI), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR), and various stages of type 2 diabetic retinopathy (T2DR). Additionally, the diagnostic value of these markers in T2DR was evaluated. Clinical data were collected from a total of 397 patients with type 2 diabetes who visited the ophthalmology department at Mian Yang Central Hospital and the Affiliated Hospital of Southwest Medical University from January 2023 to December 2023. Based on the results of fundus photography, patients were categorized into a non-diabetic retinopathy group (NDR, n = 121), a non-proliferative diabetic retinopathy group (NPDR, n = 77), and a proliferative diabetic retinopathy group (PDR, n = 199). General patient information and systemic inflammatory markers, including the SII, SIRI, AIRI, NLR, PLR, and MLR, were compared among the groups, and their correlations with T2DR were analyzed. The SII values were found to be significantly higher in the PDR group compared to the NPDR group, which in turn were higher than those in the NDR group (P < 0.05). Similarly, the AISI values were significantly elevated in the PDR group compared to both the NPDR and NDR groups (P < 0.05). The SIRI and MLR values were significantly higher in the PDR group than in the NDR group (P < 0.05). Furthermore, the NLR and PLR values were significantly higher in the NPDR and PDR groups compared to the NDR group (P < 0.05). The Mantel‒Haenszel chi-square test revealed a significant linear trend between the SII and PLR and the incidence of PDR (P < 0.001), with the incidence of PDR increasing as the quartile levels of the SII and PLR increased. Multivariate logistic regression analysis indicated that, compared with NDR, a higher SII was found to be an independent risk factor for NPDR (ORSII = 1.002, p = 0.001) and PDR (ORSII = 1.002, P < 0.001). The ROC curve analysis suggested that the combined assessment of the six inflammatory indices had the highest accuracy in the evaluation of DR, with an area under the curve (AUC) of 0.69, a sensitivity of 54%, and a specificity of 75%. The results of this study indicate that the SII is an independent risk factor for T2DR. A close correlation was observed between the SII and PLR and the occurrence and progression of T2DR. The high accuracy of the combined diagnosis of T2DR via various serological inflammatory markers underscores their potential as early biological indicators for the diagnosis of T2DR.
Similar content being viewed by others

Introduction
Diabetes, a group of metabolic disorders characterized by elevated blood glucose levels, has become a significant global health concern. According to research reports, the prevalence of diabetes among adults aged 20–79 years was 8.8% in 2015 and is projected to rise to 10.4% by 20401. Diabetes is associated with various complications, including cardiovascular diseases, kidney diseases, and retinopathy2. Type 2 diabetes mellitus (T2DM), a common form of diabetes in adults, is primarily associated with insulin resistance and a decline in pancreatic beta-cell function3. T2DR, one of the most common micro-vascular complications of T2DM, is a significant cause of blindness in adults. A systematic review of population studies indicated that the annual incidence rate of diabetic retinopathy (DR) ranges from 2.2 to 12.7%4. The scarcity of retinal specialists poses a challenge for the early screening of T2DR. Therefore, the discovery of new biomarkers is crucial for the early identification of high-risk patients and the prevention of disease progression.
The pathophysiological mechanism of T2DR is complex, and an increasing number of studies suggest that chronic low-grade inflammation plays a significant role in its development5. The inflammatory response, a defensive reaction of the body to injury or infection, involves a variety of cytokines, chemokines, leukocytes, and platelets6. While inflammatory responses are beneficial to the body’s repair and recovery to a certain extent, excessive or persistent inflammation can lead to tissue damage and organ dysfunction7. Patients with T2DM exhibit a state of chronic low-grade inflammation characterized by elevated levels of inflammatory factors in their blood8. This chronic inflammatory state leads to micro-vascular dysfunction, including damage to vascular endothelial cells, increased vascular permeability, increased blood flow resistance, and platelet aggregation9,10, thereby promoting the onset and progression of DR.
In recent years, several new comprehensive inflammatory indices, such as the SII, SIRI, AIRI, NLR, PLR, and MLR, have been proposed. These indices utilize routine parameters from complete blood counts and integrate various leukocyte subgroups, providing a better reflection of the systemic inflammatory state in patients with T2DM11. Currently, various inflammation indices have been confirmed to be associated with the occurrence and prognosis of multiple diseases, including tumors, cardiovascular diseases, liver diseases, and kidney diseases12,13,14,15. However, the correlation between these systemic inflammatory indices and T2DR has not been fully elucidated. The present study aimed to explore the correlation between systemic inflammatory indices and T2DR and to evaluate their diagnostic value in T2DR.
Materials and methods
Experimental design
A retrospective case‒control study was conducted using clinical data collected from a total of 397 patients, including 187 males and 210 females, diagnosed with type 2 diabetes at the Affiliated Hospital of Southwest Medical University and Mianyang Central Hospital from January 2023 to December 2023. The inclusion criteria for individuals were as follows: (1) aged between 18 and 80 years, and (2) diagnosed with type 2 diabetes according to the World Health Organization’s 1999 diagnostic criteria for diabetes. The exclusion criteria were as follows: (1) presence of other ophthalmic diseases (such as glaucoma, macular degeneration, etc.); (2) presence of diseases that affect inflammatory markers (such as infections, tumors, autoimmune diseases, etc.); (3) presence of factors that affect the complete blood count (such as hematological diseases, transfusions, drugs, etc.). All patients underwent fundus examination and were subsequently classified into three groups according to the DR classification criteria established by the International Council of Ophthalmology in 2002: non-diabetic retinopathy (NDR), non-proliferative diabetic retinopathy (NPDR), and proliferative diabetic retinopathy (PDR). This study was conducted in compliance with the principles of the Declaration of Helsinki by the World Medical Association and was approved by the hospital’s ethics committee. Informed consent was obtained from all patients.
Data collection
Demographic data, including age, gender, height, and weight, were collected, and body mass index (BMI) was calculated by dividing weight by the square of height. Laboratory examinations included white blood cells (WBC), neutrophils (NE), lymphocytes (LYM), monocytes (Mo), platelets (PLT), glycated hemoglobin (HbA1c), aspartate aminotransferase (AST), alanine amino transferase (ALT), albumin (ALB), creatinine (Cr), uric acid (UA), urea, the glomerular filtration rate (eGFR), and total cholesterol (TC). The values of the inflammatory indices were calculated according to the following formulas:
Statistical analysis
Statistical analysis was conducted on the collected data using SPSS 26.0 software. Measurement data conforming to a normal distribution were expressed as the mean ± standard deviation, and comparisons between groups were performed using the two independent samples t-test. For measurement data not conforming to a normal distribution, the median (interquartile range) was employed, and comparisons among multiple groups were carried out using the Kruskal‒Wallis test, with post-hoc pairwise comparisons conducted via the Bonferroni test. Trend analysis was performed using the chi-square trend test through Mantel‒Haenszel analysis. The analysis of influencing factors was conducted using multivariate logistic regression. The diagnostic value of each inflammatory index for DR in T2DM patients was determined through receiver operating characteristic (ROC) curve analysis, which included the calculation of the AUC. For all analyses, P < 0.05 was considered statistically significant.
Results
Comparison of clinical data among groups with NDR, NPDR, and PDR
The Kruskal‒Wallis test and chi‒square test revealed no statistically significant differences (P > 0.05) in the comparisons of BMI, HbA1c, AST, ALT, eGFR, TC, MO, PLT, and WBC among the three groups of patients. The proportion of males, as well as the NLR and PLR, were found to be greater in the NPDR and PDR groups compared to the NDR group (P < 0.05). The age of the PDR group was observed to be younger than that of the NPDR group, which was in turn younger than that of the NDR group (P < 0.05). ALB levels were found to be lower in the PDR group compared to the NPDR and NDR groups (P < 0.05). The levels of Cr, UA, Urea, NE, and AISI were observed to be greater in the PDR group compared to the NPDR and NDR groups (P < 0.05). LYM levels were found to be lower in the NPDR and PDR groups compared to the NDR group (P < 0.05). The SII values were observed to be greater in the PDR group compared to the NPDR group, which were in turn greater than those in the NDR group (P < 0.05). The SIRI and MLR values were found to be greater in the PDR group compared to the NDR group (P < 0.05) (Table 1).
Quartile ranges of the SII, SIRI, AISI, NLR, PLR, MLR, and trend tests for disease progression
Patients were classified into four groups (A-D) based on the quartile ranges of the SII, SIRI, AISI, NLR, PLR, and MLR to convert them into ordered multicategorical variables. The specific assignments were as follows: SII (“≦363.79” assigned as A, “365.25 ~ 491.25” assigned as B, “493.42 ~ 714.18” assigned as C, “≧726.05” assigned as D), SIRI (“≦0.67” assigned as A, “0.68 ~ 1.00” assigned as B, “1.01 ~ 1.47” assigned as C, “≧1.48” assigned as D), NLR (“≦1.86” assigned as A, “1.87 ~ 2.58” assigned as B, “2.59 ~ 3.47” assigned as C, “≧3.48” assigned as D), PLR (“≦96.48” assigned as A, “96.57 ~ 120.26” assigned as B, “120.42 ~ 154.85” assigned as C, “≧155.67” assigned as D), and MLR (“≦0.18” assigned as A, “0.19 ~ 0.24” assigned as B, “0.25 ~ 0.32” assigned as C, “≧0.33” assigned as D). After grouping, a significant linear trend was observed between the SII, the PLR, and the incidence of PDR (P < 0.001). The incidence of PDR increased as the quartile values of the SII and PLR increased. No significant trends were observed for the other indices (Tables 2 and 3).
Multivariate logistic regression analysis of clinical data for NDR, NPDR, and PDR
A multivariate logistic regression analysis was performed with the patient’s disease status as the dependent variable (NDR assigned a value of 1, NPDR as 2, PDR as 3) and incorporating indicators that differed between groups as independent variables. These indicators included age, ALB, Cr, UA, urea, NE, LYM, SII, SIRI, AISI, NLR, PLR, MLR, and sex (male assigned a value of 1, female assigned a value of 2). Compared with the NDR population, being younger and male were identified as independent risk factors for NPDR (ORage=0.961; ORgender=3.434) (P < 0.05). Being younger, having lower ALB levels, having higher NE levels, and having lower LYM levels were identified as independent risk factors for PDR (ORage=0.860; ORALB = 0.830; ORNE = 2.970; ORLYM = 0.233) (P < 0.05). Considering the issue of collinearity among various indicators, stepwise regression analysis was further applied to the SII, SIRI, AISI, NLR, PLR, and MLR. Compared with NDR, a higher SII was identified as an independent risk factor for NPDR (ORSII = 1.002, p = 0.001) and PDR (ORSII = 1.002, P < 0.001) (Tables 4 and 5).
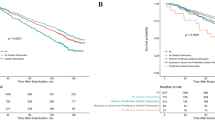
ROC curve analysis of the diagnostic value of various inflammatory indices for DR
ROC curve analysis revealed that the five inflammatory indices SII, SIRI, AISI, NLR, and PLR all demonstrated diagnostic value for diabetic retinopathy, with AUCs > 0.6 and P < 0.001. However, the combined assessment of the six inflammatory indices provided the highest accuracy for DR, with an AUC of 0.69, a sensitivity of 54%, and a specificity of 75% (Tables 6 and 7; Figs. 1 and 2).

ROC Curve Analysis of SII, SIRI, NLR, PLR, MLR, AISI.

ROC curves for each combination of indicators.
Discussion
An increasing number of studies have confirmed the crucial role of chronic low-grade inflammation in diabetic retinopathy16,17. Leukocyte extravasation, which includes neutrophils, lymphocytes, and monocytes, is currently considered the most significant characteristic of the inflammatory response. However, there is no consensus on the changes in the number of peripheral blood leukocytes and their subgroups in patients with DR. Some studies have indicated that there is no difference in the number of neutrophils and platelets in the early stages of DR, but a reduction in the number of monocytes has been observed18. Woo et al.19 proposed that patients with advanced DR exhibit increased neutrophil counts in the peripheral blood. Furthermore, patients with T2DR are believed to have significantly greater monocyte counts and significantly lower lymphocyte counts compared to patients with T2DM20. Our study revealed that the neutrophil count in the PDR group was greater than that in the NPDR and NDR groups. The lymphocyte counts in the NPDR and PDR groups were found to be lower than that in the NDR group, with no significant difference in monocyte count among the three groups. The discrepancies between our findings and those of previous studies may be attributed to differences in sample size; hence, our research focused on composite indices.
The six indices explored in this study are novel serological inflammatory markers calculated by integrating multiple routine blood parameters, which reflects the combined effect of platelets, neutrophils, lymphocytes, and monocytes on inflammation. Our analysis revealed significant differences among the NDR, NPDR, and PDR patient groups for the aforementioned six indices. Both the SII and PLR were found to be significantly correlated with the occurrence and progression of T2DR, which is consistent with the conclusions of Gao et al.21 The SII serves as a comprehensive indicator reflecting the status of inflammation and immunity. These results suggest the significant role of systemic inflammation in the pathogenesis of T2DR. Furthermore, an increase in the SII is associated with a clear linear trend in the incidence of PDR. This indicates that the SII may serve as a potent biomarker for predicting the occurrence and progression of T2DR. Multivariate logistic regression analysis further confirmed the status of the SII as an independent risk factor for both NPDR and PDR. This finding emphasizes the importance of monitoring changes in the SII in clinical practice, as it could aid in the early identification of patients at high risk for T2DR.
The increase in the PLR also exhibits a linear trend with the incidence of PDR, potentially reflecting the role of platelets in the pathophysiology of diabetic retinal diseases. Studies have indicated that antiplatelet therapy exerts a significant protective effect on the development of NPDR in patients with T2DM22. Platelets not only participate in blood coagulation but also perform functions, such as immune regulation, inflammation mediation, and vascular repair23. During inflammatory responses, platelets interact with neutrophils and are capable of releasing a variety of inflammatory factors24. These factors increase vascular permeability, promote leukocyte adhesion and migration, stimulate endothelial cell proliferation, and induce angiogenesis25, potentially exacerbating the development of DR.
Only the SII was statistically significant in the multivariate logistic regression analysis. However, this is considered to be due to the high collinearity among the indices, arising from the repeated use of data such as neutrophils and lymphocytes in their calculation. However, in the ROC curve analysis, the combined assessment of the six inflammatory indices demonstrated the highest accuracy for evaluating DR, with an AUC of 0.69, a sensitivity of 54%, and a specificity of 75%. These results indicate that single indices have limitations in diagnosing T2DR. By integrating multiple inflammatory indices, the diagnostic accuracy can be significantly improved. This finding provides a new direction for future research, namely, to further explore and optimize the combined assessment model of multiple indices, thereby increasing the diagnostic efficiency of T2DR.
Current research indicates that systemic inflammatory markers, such as the SII, play a significant role in the prognosis of diseases, such as cancer, infectious diseases, cardiovascular diseases, and stroke26,27. However, limited research has been conducted on their prognostic value in patients with DR. Researchers have found that the NLR and SII are significantly elevated in patients with diabetic macular edema (DME) complicated by serous macular detachment (SMD), especially in late-stage cases. This suggests that the increase in systemic inflammatory mediators may be related to the high incidence of SMD28. Si et al. found through a retrospective analysis that elevated levels of NLR, MLR, and systemic inflammation response index (SIRI) are associated with all-cause mortality and diabetes-cardiovascular mortality in DR patients, suggesting that they may serve as independent prognostic predictors for DR29. Other studies have suggested that the SII has significant predictive ability for microvascular and macrovascular complications, mortality, and their combined parameters in the early stages. However, its long-term predictive value is limited30. In summary, incorporating systemic inflammatory markers in clinical practice can enhance the accuracy of prognosis prediction for DR patients, aiding in early diagnosis and timely treatment. This approach can improve patients’ quality of life and reduce healthcare costs. Therefore, it is necessary to further explore the impact of systemic inflammatory markers on the prognosis of DR patients.
Despite the valuable insights provided by this study, several limitations exist. First, this was a retrospective case‒control study. Some parameters and information, such as the duration of diabetes and fasting blood glucose levels, were incomplete when patient data were collected. Second, the study included patients from only three groups, namely, the no diabetic retinopathy (NDR), NPDR, and PDR groups, without a comparison with healthy individuals. Furthermore, no follow-up observations were conducted to examine the relationships between various indicators and the prognosis of DR. Lastly, the study did not explore the specific mechanisms by which changes in each indicator contribute to the occurrence and progression of DR.
Conclusion
The present study highlights the significant roles of the SII and PLR in the occurrence and progression of T2DR. Moreover, the study demonstrates the potential of combining multiple indices to improve the diagnostic accuracy of T2DR. These findings provide novel perspectives and tools for future research and clinical practice.
Data availability
Data can be provided by the corresponding author upon reasonable request.
References
Ogurtsova, K. et al. IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 128, 40–50 (2017).
Demir, S., Nawroth, P. P., Herzig, S. & Ekim Üstünel, B. Emerging targets in type 2 diabetes and Diabetic complications. Adv. Sci. (Weinh). 8 (18), e2100275 (2021).
ElSayed, N. A. et al. 2. Classification and diagnosis of diabetes: standards of Care in Diabetes-2023. Diabetes Care. 46 (Suppl 1), S19–S40 (2023).
Sabanayagam, C. et al. Incidence and progression of diabetic retinopathy: a systematic review. Lancet Diabetes Endocrinol. 7 (2), 140–149 (2019).
Tang, L., Xu, G. T. & Zhang, J. F. Inflammation in diabetic retinopathy: possible roles in pathogenesis and potential implications for therapy. Neural Regen Res. 18 (5), 976–982 (2023).
Bhat, A. A. et al. Cytokine- and chemokine-induced inflammatory colorectal tumor microenvironment: emerging avenue for targeted therapy. Cancer Commun. (Lond). 42 (8), 689–715 (2022).
Yue, T. et al. The role of inflammation in immune system of diabetic retinopathy: molecular mechanisms, pathogenetic role and therapeutic implications. Front. Immunol. 13, 1055087 (2022).
Kaštelan, S., Orešković, I., Bišćan, F., Kaštelan, H. & Gverović Antunica, A. Inflammatory and angiogenic biomarkers in diabetic retinopathy. Biochem. Med. (Zagreb). 30 (3), 030502 (2020).
Spencer, B. G., Estevez, J. J., Liu, E., Craig, J. E. & Finnie, J. W. Pericytes, inflammation, and diabetic retinopathy. Inflammopharmacology 28 (3), 697–709 (2020).
Tang, L. et al. Melatonin maintains inner blood–retinal barrier by regulating Microglia via Inhibition of PI3K/Akt/Stat3/NF-κB signaling pathways in Experimental Diabetic Retinopathy. Front. Immunol. 13, 831660 (2022).
Dascalu, A. M. et al. The value of White Cell inflammatory biomarkers as potential predictors for Diabetic Retinopathy in type 2 diabetes Mellitus (T2DM). Biomedicines 11 (8), 2106 (2023).
Choucair, K. et al. Characterization of Age-Associated, Neutrophil-to-lymphocyte ratio (NLR) and systemic Immune-Inflammatory Index (SII) as biomarkers of inflammation in geriatric patients with Cancer treated with Immune Checkpoint inhibitors: impact on efficacy and survival. Cancers (Basel). 15 (20), 5052 (2023).
Gu, L. et al. Systemic inflammatory response index (SIRI) is associated with all-cause mortality and cardiovascular mortality in population with chronic kidney disease: evidence from NHANES (2001–2018). Front. Immunol. 15, 1338025 (2024).
Tuzimek, A., Dziedzic, E. A., Beck, J. & Kochman, W. Correlations between Acute Coronary Syndrome and Novel inflammatory markers (systemic Immune-inflammation index, systemic inflammation response index, and Aggregate Index of systemic inflammation) in patients with and without diabetes or Prediabetes. J. Inflamm. Res. 17, 2623–2632 (2024).
Mandaliya, H., Jones, M., Oldmeadow, C. & Nordman, I. I. Prognostic biomarkers in stage IV non-small cell lung cancer (NSCLC): neutrophil to lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR) and advanced lung cancer inflammation index (ALI). Transl Lung Cancer Res. 8 (6), 886–894 (2019).
Youngblood, H., Robinson, R., Sharma, A. & Sharma, S. Proteomic biomarkers of retinal inflammation in diabetic retinopathy. Int. J. Mol. Sci. 20 (19), 4755 (2019). PMID: 31557880; PMCID: PMC6801709.
Portillo, J. C. et al. Disruption of retinal inflammation and the development of diabetic retinopathy in mice by a CD40-derived peptide or mutation of CD40 in müller cells. Diabetologia 65 (12), 2157–2171 (2022). PMID: 35920844; PMCID: PMC9630214.
Wan, H. et al. The unique association between the level of peripheral blood monocytes and the prevalence of diabetic retinopathy: a cross-sectional study. J. Transl Med. 18, 248 (2020).
Woo, S. J., Ahn, S. J., Ahn, J., Park, K. H. & Lee, K. Elevated systemic neutrophil count in diabetic retinopathy and diabetes: a hospital-based cross-sectional study of 30, 793 Korean subjects. Invest. Ophthalmol. Vis. Sci. 52 (10), 7697–7703 (2011).
Huang, Q. et al. Clinical and predictive significance of plasma fibrinogen concentrations combined Monocyte-lymphocyte ratio in patients with Diabetic Retinopathy. Int. J. Med. Sci. 18 (6), 1390–1398 (2021).
Gao, Y. et al. Systemic immune-inflammation index, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio in patients with type 2 diabetes at different stages of diabetic retinopathy. Int. J. Ophthalmol. 17 (5), 877–882 (2024).
Eng, C. J., Hsieh, Y. T., Lin, C. L. & Wang, I. J. Effect of anticoagulant/antiplatelet therapy on the development and progression of diabetic retinopathy. BMC Ophthalmol. 22 (1), 127 (2022).
Franco, A. T., Corken, A. & Ware, J. Platelets at the interface of thrombosis, inflammation, and cancer. Blood 126 (5), 582–588 (2015).
Ramirez, G. A., Manfredi, A. A. & Maugeri, N. Misunderstandings between platelets and neutrophils build in chronic inflammation. Front. Immunol. 10, 2491 (2019).
Thomas, M. R. & Storey, R. F. The role of platelets in inflammation. Thromb. Haemost. 114 (3), 449–458 (2015).
Zhang, Y., Xing, Z., Zhou, K. & Jiang, S. The predictive role of systemic inflammation response index (SIRI) in the prognosis of stroke patients. Clin. Interv Aging. 16, 1997–2007 (2021).
Dziedzic, E. A. et al. Investigation of the associations of Novel inflammatory biomarkers-systemic Inflammatory Index (SII) and systemic inflammatory response index (SIRI)-With the severity of coronary artery Disease and Acute Coronary Syndrome occurrence. Int. J. Mol. Sci. 23 (17), 9553 (2022).
Özata Gündoğdu, K., Doğan, E., Çelik, E. & Alagöz, G. Serum inflammatory marker levels in serous macular detachment secondary to diabetic macular edema. Eur. J. Ophthalmol. 32 (6), 3637–3643 (2022).
Si, Y., Chen, Q., Xiong, X. & Zheng, M. The association of inflammatory biomarkers with clinical outcomes in diabetic retinopathy participants: data from NHANES 2009–2018. Diabetol. Metab. Syndr. 16 (1), 181 (2024).
Tabakoglu, N. T. & Celik, M. Investigation of the systemic Immune inflammation (SII) Index as an Indicator of Morbidity and Mortality in type 2 Diabetic Retinopathy patients in a 4-Year Follow-Up period. Med. (Kaunas). 60 (6), 855 (2024).
Funding
This research was partly supported by a statutory grant to the Sichuan Medical Association (Grant Number: Q15036).
Author information
Authors and Affiliations
Contributions
Conceptualization, Hongbin Lv and Yan Dai; methodology, Rongjin Deng, Suhui Zhu; statistical analysis, Rongjin Deng; data curation, Bin Fan; writing—original draft preparation, Rongjin Deng; writing—review and editing, Xiaohu Chen and Yan Dai; funding acquisition, Yan Dai. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of the Affiliated Hospital of Southwest Medical University (ethics batch number: KY2024269).
Informed consent
Informed consent was obtained from all subjects involved in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Deng, R., Zhu, S., Fan, B. et al. Exploring the correlations between six serological inflammatory markers and different stages of type 2 diabetic retinopathy. Sci Rep 15, 1567 (2025). https://doi.org/10.1038/s41598-025-85164-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-85164-2
Keywords
This article is cited by
-
The relationship between pan-immune inflammation value and different stages of diabetic retinopathy in patients with type 2 diabetes mellitus: a prospective cross-sectional study
BMC Endocrine Disorders (2025)
-
The association of peripheral blood inflammatory markers with the distribution patterns of IgE in children with allergen sensitization
BMC Immunology (2025)
-
Correlation Between NLR to Albumin Ratio and 90-day Prognosis After Treatment for Acute Ischemic Stroke
Journal of Cardiovascular Translational Research (2025)
