
Abstract
Dietary inflammatory index (DII) was demonstrated to be correlated to quality of life (QoL) in people with osteoarthritis (OA), but there is lack of an exploration of the relationship between the longitudinal trajectories of QoL and DII in OA people. This study aims to investigate the relationship between DII and longitudinal trajectories of QoL, and the moderating effect of physical activity on this relationship in OA people. Data from the Osteoarthritis Initiative database includes baseline measurements and follow-up data at 1, 2, 3, 4, 5, 6, and 8-year intervals for the 12-item Short-Form Health Outcome Survey questionnaire (physical and mental dimensions) and baseline sociodemographic characteristics utilized in this study. Dual Group-Based Trajectory Modeling analysis was employed to identify the profiles of physical and mental QoL trajectories. Multiple logistic regression analysis was used to determine the relationship between DII and QoL profiles. A structural equation model was conducted to assess the moderating effect of physical activity on the relationship between DII and QoL in OA people. A total of 1127 OA people were categorized into three profiles based on their physical and mental QoL: low physical-low mental QoL (14.5%), low physical-high mental QoL (27.1%), and high physical-high mental QoL (58.4%). People with higher DII were more likely to be in the low physical-low mental QoL profile (OR = 1.163, P = 0.014) and low physical-high mental QoL (OR = 1.131, P = 0.013) compared to the high physical-high mental QoL profile. Additionally, a higher level of physical activity could mitigate the relationship between a higher DII and lower QoL (β = 0.064, P = 0.029). A higher DII was associated with a greater likelihood of impaired QoL. Increasing physical activity levels can help mitigate the negative impact.
Similar content being viewed by others

Introduction
Osteoarthritis (OA) is a highly prevalent and disabling condition that affects over 7% of the global population, ranking as the 15th highest cause of years lived with disability worldwide1. The financial burden of OA on people and society is significant1, with main symptoms including joint pain, stiffness, activity limitations, and negative psychological effects such as depression and psychological distress, ultimately impacting people’ quality of life (QoL)1,2.
Low-grade inflammation, characterized by an increase in pro-inflammatory cytokines, can significantly impact people’ QoL3,4. Previous studies have suggested that adopting a healthy diet can lead to reduced inflammatory responses and serve as a cost-effective strategy to improve QoL5. To assess the inflammatory impact of diet, Shivappa et al. introduced the Dietary Inflammatory Index (DII)6. Higher DII scores have been associated with elevated levels of inflammatory cytokines such as interleukin-6, tumor necrosis factor, and high-sensitivity C-reactive protein7,8. A cross-sectional study by Toopchizadeh et al. involving 220 OA people revealed that higher DII scores were associated with poorer QoL9. While several studies10,11,12 have explored QoL trajectories in OA people, there is a research gap concerning the relationship between DII and the longitudinal trajectories of QoL. Furthermore, previous studies on QoL trajectories in OA people have predominantly focused on overall QoL without distinguishing between physical and mental QoL dimensions. Given that physical and mental QoL are distinct dimensions that may not exhibit consistent levels and trends, it is essential to delineate developmental pathways that capture the evolving tendencies of these two variables concurrently. By differentiating between physical and mental QoL, our understanding of the relationship between these dimensions can be enriched. Improving levels of physical activity is a recommended treatment for OA, as it has been proven to reduce pain, anxiety, and depression symptoms, and improve overall QoL13. One potential mechanism of action is the exercise-induced anti-inflammatory effects14.
Utilizing data from the Osteoarthritis Initiative (OAI) database, a prospective longitudinal cohort study, we conduct a Dual Group-Based Trajectory Modeling (DGBTM) analysis on the physical and mental QoL of OA people. This study aims to describe the characteristics of each physical and mental QoL profile, investigate the causal relationship between DII and QoL, and explore the moderating effect of physical activity on this relationship in OA people.
Methods
Study design
OAI15 is a multi-center, longitudinal, observational study sponsored by the National Institutes of Health. The data used in this study were obtained from the OAI database, including baseline measurements and follow-up data at 1-year, 2-year, 3-year, 4-year, 5-year, 6-year, and 8-year intervals for the 12-Item Short-Form Health Outcome Survey (SF-12) questionnaire. The analysis also included baseline data for the Physical Activity in the Elderly Scale (PASE) activity, the Block Brief 2000 Food Frequency Questionnaire (FFQ), the Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores, Kellgren and Lawrence (KL) grade, and sociodemographic characteristics. All publicly available data can be accessed through the OAI website (https://nda.nih.gov/oai/). The study was reported according to the STROBE guidelines.
Setting
Data were collected from four clinical centers, including Baltimore, Maryland; Columbus, Ohio; Pittsburgh, Pennsylvania; and Pawtucket, Rhode Island.
Participants
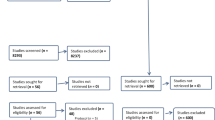
OAI enrolled 4796 participants with or at risk of knee OA to investigate the impact of knee OA over time to understand the prevention and treatment strategies better. This study focuses on people with radiographic OA (Kellgren and Lawrence grade ≥ 2)16 and symptomatic OA (The Western Ontario and McMaster Universities Arthritis Index pain score > 0)17. The cohort study initially enrolled 4796 participants and followed them for 10 years. To ensure complete data on the variables of interest, we ultimately included 1127 people with 8 years of follow-up data. Please refer to Fig. 1 for the selection process. Informed consent was obtained from all participants included in the study.

Flow diagram reflecting how 1127 participants were selected from the original participants. BMI, body mass index; OAI, Osteoarthritis Initiative; PASE, the Physical Activity in the Elderly Scale; ROA, radiographic osteoarthritis; SF-12, The 12-Item Short-Form Health Outcome Survey; SOA, symptomatic osteoarthritis; WOMAC, the Western Ontario and McMaster Universities Arthritis Index.
Variables and measurements
Outcome variable
SF-1218 was utilized to evaluate QoL as the primary outcome. This survey comprises 12 questions that are summarized into a physical composite scale and a mental composite scale. The final SF-12 scores range from 0 to 100, with higher scores indicating better health-related QoL.
Dependent variables
PASE19 was utilized to assess physical activity. It measures household, occupational, and leisure physical activities over a 7-day period and generates a single composite score ranging from 0 to 400. Higher scores indicate higher levels of physical activity.
FFQ20 was used to evaluate dietary intake. It assessed people’ typical food and beverage consumption over the past year, covering a total of seventy items. Consumption frequency was reported on a scale of nine levels, ranging from “never” to “every day”. Additionally, participants were queried about their dietary behaviors, including food preparation methods, fat intake, fiber intake, as well as about vitamin and mineral intakes.
DII6 is a tool designed to gauge the inflammatory potential of an individual’s overall diet and can be applied to various populations6,21. A higher DII score signifies a more pro-inflammatory diet characterized by increased consumption of saturated fats and refined carbohydrates, whereas a low score indicates an anti-inflammatory diet rich in antioxidants and fibers. In this study, the DII was calculated using the energy density approach, based on the energy-adjusted intake of 24 single food parameters out of the 45 possible parameters available from the FFQ. The DII was calculated per 4184 kJ (1000 kcal) of energy22. The 24 food parameters used for DII calculation in this study included vitamin B12, vitamin B6, β-carotene, carbohydrate, cholesterol, fat, fiber, folic acid, iron, magnesium, monounsaturated fat acids (MUFA), niacin, protein, polyunsaturated fatty acids (PUFA), riboflavin, saturated fat acids(SFA), selenium, thiamin, vitamin A, vitamin C, vitamin E, vitamin D, zinc, niacin, and caffeine. Higher DII indicates a higher intake of pro-inflammatory foods.
WOMAC23 was used to assess pain, stiffness, and physical functioning due to osteoarthritis. Responses for each subscale (pain, stiffness, and physical functioning) were rated on a 5-point Likert scale ranging from none (0 points) to extreme (4 points). The maximum possible score was 68, which was then normalized to 100 (range: 0-100). Higher scores reflect greater pain, stiffness, and physical functioning disability.
Charlson modified comorbidity score24 was used to assess validated general health measures of self-reported comorbidities. Medical conditions included in the Charlson comorbidity index were cerebrovascular disease, chronic obstructive pulmonary disease, gastro-intestinal ulcers, diabetes mellitus, asthma, heart failure, heart attack, percutaneous transluminal coronary angioplasty, coronary artery bypass, bone fractures, knee osteoarthritis, and cancer. Higher scores indicate increased severity of conditions.
KL16 grade was assessed through auxiliary radiography studies. The images were centrally graded by two expert readers who were blinded to each other’s readings and to clinical data from the individuals.
Sociodemographic characteristics included age, gender, employment status, frequency of knee bending activities, family income, level of education, race, body mass index (BMI), varus or valgus alignment, smoking and drinking habits, and history of surgery or arthroscopy.
Statistical methods
Group-Based Trajectory Modeling (GBTM) utilizes multivariate longitudinal data to track outcomes and assess population heterogeneity, allowing for precise individual classifications into various groups using finite mixture modeling25,26. DGBTM is an extension of GBTM that determines the co-occurring trajectories of two variables26. DGBTM will be used to examine how physical and mental QoL trajectories evolve simultaneously over time, providing insights into the QoL of OA people.
SAS 9.4 and STATA 17 were used for conducting DGBTM analysis, which aimed to identify developmental trajectories for physical and mental QoL in OA people. The optimal number of trajectories was determined based on the fit indices, including Akaike information criterion (AIC), Bayesian information criterion (BIC), entropy, Lo-Mendell-Rubin (LMR) test, and the parametric bootstrap likelihood-ratio test (BLRT), as well as the interpretability of the model. The selected number of classes/trajectories was determined by considering the rate of decrease in the information criterion, higher entropy indicating better classification, and significant LMR test or BLRT likelihood-ratio test indicating a better fit compared to the previous number of classes, along with interpretability of the trajectories.
Statistical analysis was conducted using SPSS 25.0. The Kolmogorov-Smirnov test was employed to assess the normality of continuous variables. Variables that conformed to a normal distribution were described using the mean (standard deviation, SD), while non-normally distributed variables were described using the [interquartile range (IQR)]. Categorical data were presented as numbers and percentages. The Mann-Whitney test was used for comparing two independent non-normally distributed continuous variables, while the Kruskal-Wallis test was used for multiple independent non-normally distributed continuous variables. Chi-square test was used for analyzing categorical data. Spearman analysis was used to examine the correlation between continuous variables. Multiple logistic regression analysis was performed to identify independent factors influencing QoL profiles. A two-tailed P-value < 0.05 was considered statistically significant.
AMOS 26.0.0 was utilized to examine the moderating effect of physical activity on the relationship between DII and QoL score. Bootstrapping was used to evaluate the significance of the moderating effect. A total of 2000 bootstrap resamples were conducted with 95% confidence intervals (CIs) to analyze both direct and indirect effects. The fit of the hypothesized model to the data was assessed by calculating absolute and incremental fit indices.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by Institutional Review Board (IRB) for the University of California, San Francisco (UCSF) and its affiliates (approval number: FWA00000068). The IRB approval was also obtained from all the four clinical sites located at Brown University in Rhode Island, Ohio State University in Columbus, Ohio, University of Maryland/Johns Hopkins University joint center in Baltimore, Maryland, and at the University of Pittsburgh in Pennsylvania.
Results
Sociodemographic characteristics of people with osteoarthritis
A total of 1127 OA people aged from 45 to 79 years were included in this study, with 57.2% (645/1127) of the people being female. The DII of the people varied from − 4.58 to 3.44. Please refer to Table 1 for more details.
Profiles of quality of life in people with osteoarthritis
Based on the results of analyzing the physical and mental QoL of OA people using DGBTM (refer to Supplementary Tables 1–3), it was determined that the optimal number of individual profiles was considered three. Subsequently, the people were categorized into three distinct groups: G1 (low physical-low mental QoL), comprising 14.5% (164/1127) of the total people, G2 (low physical-high mental QoL), encompassing 27.1% (304/1127) of the people, and G3 (high physical-high mental QoL), representing 58.4% (659/1127) of the people cohort (refer to Fig. 2).

Longitudinal trajectories of physical and mental QoL in people with OA. Abbreviations: OA, osteoarthritis; QoL, quality of life. Depictions – G1 refers to low physical-low mental QoL profile; G2 refers to low physical-high mental QoL profile; G3 refers to high physical-high mental QoL; the horizontal coordinate indicates the number of years of follow-up from the baseline; the vertical coordinate indicates physical or mental QoL scores.
Univariate factors influencing quality of life profiles in people with osteoarthritis
The analysis of the relationship between sociodemographic characteristics and QoL profiles in OA people indicated significant associations with various factors. These included age (p < 0.001), gender (X2 = 20.842, p < 0.001), employment (X2 = 22.838, p < 0.001), family income (X2 = 81.344, p < 0.001), Charlson modified comorbidity score (p < 0.001), education degree (X2 = 47.671, p < 0.001), BMI (X2 = 42.063, p < 0.001), PASE activity (p < 0.001), KL grade (p < 0.001), WOMAC physical functioning (p < 0.001), WOMAC pain (p < 0.001), WOMAC stiffness (p < 0.001), smoking habit (X2 = 17.765, p = 0.007), drinking habit (X2 = 18.866, p = 0.016), and DII score (p = 0.020). These factors exhibited statistically significant differences across the various QoL profiles in people with OA.
Older individuals were more likely to be in the low physical-high mental QoL profile. Males were more likely to be in the high physical-high mental QoL profile. Those who worked for pay were more likely to be in the high physical-high mental QoL profile. Individuals with a family income greater than $50k were more likely to be in the high physical-high mental QoL profile. Additionally, people with a lower Charlson modified comorbidity score were more likely to be in the high physical-high mental QoL profile. Obese individuals were more likely to be in the low physical-low mental or low physical-high mental QoL profiles. Higher levels of physical activity, as measured by the PASE, were associated with a greater likelihood of being in the high physical-high mental QoL profile. Conversely, individuals with a higher KL grade were more likely to be in the low physical-high mental QoL profile. Those with lower WOMAC scores for physical functioning, pain, or stiffness were more likely to be in the high physical-high mental QoL profile. Current smokers were more likely to be in the low physical-low mental QoL profile, while individuals consuming eight or more alcoholic drinks per week were more likely to be in the low physical-low mental or low physical-high mental QoL profiles. Finally, individuals with a lower DII score were more likely to be in the high physical-high mental QoL profile, and those with an educational degree of less than college were more likely to be in the low physical-low mental QoL profile. Please refer to Table 2 for more detailed information.
Independent factors influencing quality of life profiles in people with osteoarthritis
Age, WOMAC pain, Charlson modified comorbidity score, WOMAC physical functioning, WOMAC stiffness, DII, PASE activity, and KL grade were continuous variables, while other variables were assigned as shown in Supplementary Table 4.
The multiple logistic regression analysis indicated an excellent model fit (refer to Table 3). In comparison to the high physical-high mental QoL profile, people with higher Charlson modified comorbidity score (OR = 1.375, p = 0.004), elevated WOMAC physical functioning score (OR = 1.090, p < 0.001), increased DII score (OR = 1.163, p = 0.014), family income < $25k (OR = 2.956, p = 0.005) or between $25k ~ $50k (OR = 2.134, p = 0.023), and current smoking habit (OR = 2.215, p = 0.039) were more likely to be in the low physical-low mental QoL profile. Conversely, people of male gender (OR = 0.556, p = 0.011) were less likely to be in the low physical-low mental QoL profile.
People with older age (OR = 1.032, p = 0.005), higher Charlson modified comorbidity score (OR = 1.216, p = 0.043), higher WOMAC physical functioning score (OR = 1.080, p < 0.001), elevated DII (OR = 1.131, p = 0.013), higher KL grade (OR = 1.360, p = 0.006), drinking habit of 8 + drinks per week (OR = 1.803, p = 0.005) or 4–7 drinks per week (OR = 1.829, p = 0.028), and obesity in terms of BMI (OR = 1.939, p = 0.009) were more likely to be in the low physical-high mental QoL profile. For a comprehensive overview, please refer to Table 3.
Structural equation model of dietary inflammatory index, physical activity, and quality of life in people with osteoarthritis
In developing a structural equation model (R2 = 0.28, F = 10.74, p < 0.001), DII was utilized as the independent variable, the total QoL score as the dependent variable, and the PASE activity score as the moderating variable. The model, shown in Supplementary Fig. 1, demonstrated that DII had a negative impact on the QoL score (β = -0.117, p < 0.001). Furthermore, physical activity played a significant moderating role in the relationship between DII and QoL (β = 0.064, p = 0.029).
Through simple slope analysis, it was observed that for people with lower PASE activity levels (Mean − 1 SD), DII had a significant negative impact on QoL (β = -1.210, p < 0.001). Similarly, for people with median PASE activity levels (M), DII also had a significant impact on QoL (β = -0.775, P < 0.001). However, for people with higher PASE activity levels (Mean + 1 SD), DII did not exhibit a significant impact on QoL (β = -0.340, p = 0.219), as illustrated in Fig. 3. Further a more comprehensive understanding of the structural equation model, additional information can be found in Supplementary Tables 5 and 6.

The simple slope analysis shows that PASE activity moderated the relation between DII and QoL. Abbreviations: DII, dietary inflammatory index; OA, osteoarthritis; PASE, the Physical Activity in the Elderly Scale; QoL, quality of life.
Discussion
This study identified three profiles representing the longitudinal trajectories of physical and mental QoL in OA people: low physical-low mental QoL, low physical-high mental QoL, and high physical-high mental QoL, accounting for 14.5%, 27.1%, and 58.4% of the people, respectively. People with higher DII were more likely to be in the low physical-low mental QoL profile and low physical-high mental QoL compared to the high physical-high mental QoL profile. Furthermore, the DII exhibited a negative correlation with overall QoL (both physical and mental). Moreover, an increase in physical activity was found to potentially mitigate the adverse effects of high DII on overall QoL (both physical and mental).
This study found that DII was an independent factor affecting QoL profiles and directly negatively impacting QoL scores in OA people. Previous studies also found that various individual groups such as hemodialysis people, women with obesity or overweight, and healthy people etc. with a higher DII were more likely to experience poorer physical and mental QoL4. A higher DII score indicates a higher consumption of pro-inflammatory foods, leading to increased production of inflammatory substances7,8. Additionally, higher DII scores have been associated with a higher incidence of frailty27, depressive symptoms27, and greater pain28 in OA people. Furthermore, higher DII values have been linked to a higher prevalence of knee osteoarthritis29,30. These may ultimately reduce the QoL of OA people. A previous cross-sectional survey9 found that a higher DII in the diets was associated with higher odds of severe pain and lower QoL in people with knee OA. Our longitudinal study further confirms the relationship between DII and QoL, providing new insights in this research field.
Numerous studies have emphasized the intricate relationship between diet and physical activity and their impact on human health31. This study further supports this conclusion by suggesting that increased physical activity can counteract the negative effects of pro-inflammatory diets on QoL. Physical activity is related to the regulation of the innate immune system and the treatment of OA32. Regular physical activity may increase serotonin synthesis, improve noradrenergic neurotransmission, trigger the release of endorphins, and reduce long-term sympathetic nervous system activity, thereby reducing systemic inflammation in the people33. Additionally, physical activity can prevent inflammation of chondrocytes and cartilage matrix by reducing IL-6 and TNF-α, as well as other inflammatory markers related to OA, thereby delaying the degeneration of articular cartilage and improving joint function34. It may also increase the level of protective inflammation markers in the body to inhibit the progression of OA35,36. Therefore, it is recommended to promote anti-inflammatory diets and encourage appropriate levels of physical activity for OA people. Further research should be conducted to explore the mechanism of the interaction between physical activity and DII in OA people.
This study identified a discrepancy between physical QoL and mental QoL in certain people, where some exhibited poor physical QoL alongside good mental QoL. Interestingly, no profile was observed with good physical QoL and poor mental QoL, suggesting that mental well-being may be more easily influenced by various factors compared to physical well-being. A positive mental state can benefit disease progression and overall health status in people. Therefore, distinguishing the characteristics of people in the group with both poor physical and mental QoL form those with poor physical QoL and good mental QoL is crucial. This differentiation can offer valuable insights for healthcare providers to enhance the mental well-being of OA people and serve as a foundation for future research on mental interventions for this population.
The study findings indicated that older age, higher KL grade, increased alcohol consumption, and obesity were associated with the low physical-high mental QoL profile, rather than the low physical-low mental QoL profile. Solmi et al.37 also found that mental health-related QoL was higher in older people, consistent with previous findings in the general population38. This may be because elderly people possess better mental toughness, ability to handle pressure, and tolerance due to their rich life experience. Furthermore, while alcohol consumption can adversely affect physical health, such as harming the liver, kidneys, and causing serious coronary effects, etc39, it can also provide a sense of pleasure40, thereby impacting physical QoL more. Additionally, it is important to note that many studies have highlighted the dependency effects of alcohol and the depressive psychological effects of drinking39. Therefore, healthcare providers should recommend that people with OA decrease their alcohol consumption. Obesity has been shown to be associated with reduced health-related QoL, with a stronger impact on physical QoL than mental QoL41, similar to the findings of this study. The KL grade, reflecting worse physical condition, may not directly impact the mental QoL of OA people. The relationship and mechanism between these characteristics and the mental health of OA people can be further explored.
Limitations and implications of the study
The limitations of this study include that the data were generated from the OAI database, some people with missing data were excluded from the analysis, which may introduce potential bias to the results. Additionally, the number of individuals from the Asian race was significantly smaller compared to those from the White and African American races, which may introduce bias in the statistical analysis results. Therefore, we did not compare the differences in DII scores between Asian individuals and those from the White and African American races. This disparity may also affect the representativeness of the results, and caution should be exercised when interpreting the relationship between race and QoL profiles.
This study is the first study to explore the relationship between DII and the dual longitudinal trajectories of physical and mental QoL in OA people, providing novel insight into the nutritional research on OA people. Healthcare providers should pay close attention to the inflammatory nature of the diets of people with OA and recommend that they consume more anti-inflammatory foods while appropriately increasing their activity levels to enhance both their physical and mental QoL. Furthermore, researchers can conduct similar studies focusing on Asian populations and develop more clinical trials to further explore and confirm the causal relationship and mechanisms between the DII and QoL in people with OA.
Conclusion
This study analyzes the physical and mental QoL trajectories of OA people over an 8-year period using longitudinal data from the OAI database, a prospective cohort study. The QoL of OA people can be categorized into three profiles: low physical-low mental QoL, low physical-high mental QoL, and high physical-high mental QoL. Individuals with a higher DII were significantly correlated with lower QoL, while a higher level of physical activity could mitigate this relationship. OA people with severe physical symptoms, poor social and financial status, unhealthy habits such as smoking and drinking, intrinsic properties such as female gender, and older age, as well as consumption of pro-inflammatory diets, require more attention to their QoL. Further clinical trials are necessary to evaluate the effectiveness of anti-inflammatory diets in improving QoL in OA people.
Data availability
Data were obtained from the OAI clinical dataset. These data are available for public access (https://nda.nih.gov/oai/), and permission was obtained by the team from the NIMH Data Archive (NDA) to access the data. The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request and with the permission of the NDA.
Abbreviations
- DII:
-
Dietary Inflammatory Index
- QoL:
-
Quality of Life
- OA:
-
Osteoarthritis
- GBTM:
-
Group-Based Trajectory Modeling
- DGBTM:
-
Dual Group-Based Trajectory Modeling
- OAI:
-
Osteoarthritis Initiative
- SF-12:
-
The 12-Item Short-Form Health Outcome Survey
- PASE:
-
The Physical Activity in the Elderly Scale
- FFQ:
-
The Block Brief 2000 Food Frequency Questionnaire
- WOMAC:
-
The Western Ontario and McMaster Universities Arthritis Index
- KL:
-
Kellgren and Lawrence
- BMI:
-
Body Mass Index
- AIC:
-
Akaike Information Criterion
- BIC:
-
Bayesian Information Criterion
- LMR:
-
Lo-Mendell-Rubin
- BLRT:
-
Bootstrap Likelihood-Ratio Test
- SD:
-
Standard Deviation
- IQR:
-
Interquartile Range
- KOOS QoL:
-
The Quality of Life Subscale of the Knee Injury and Osteoarthritis Outcome Score
References
Leifer, V. P., Katz, J. N. & Losina, E. The burden of OA-health services and economics. Osteoarthr. Cartil. 30, 10–16 (2022).
Bartholdy, C. et al. Association between Weight loss and spontaneous changes in physical inactivity in Overweight/Obese individuals with knee osteoarthritis: an eight-week prospective cohort study. Arthritis Care Res. (Hoboken). 72, 397–404 (2020).
Pengpid, S. & Peltzer, K. The impact of Chronic diseases on the quality of life of primary care patients in Cambodia, Myanmar and Vietnam. Iran. J. Public. Health. 47, 1308–1316 (2018).
Golmohammadi, M. et al. Is there any association between dietary inflammatory index and quality of life? A systematic review. Front. Nutr. 9, 1067468 (2022).
Saghafi-Asl, M. et al. The association of dietary patterns with dietary inflammatory index, systemic inflammation, and insulin resistance, in apparently healthy individuals with obesity. Sci. Rep. 11, 7515 (2021).
Shivappa, N., Steck, S. E., Hurley, T. G., Hussey, J. R. & Hébert, J. R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public. Health Nutr. 17, 1689–1696 (2014).
Tabung, F. K. et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 25, 398–405 (2015).
Na, W., Kim, M. & Sohn, C. Dietary inflammatory index and its relationship with high-sensitivity C-reactive protein in Korean: data from the health examinee cohort. J. Clin. Biochem. Nutr. 62, 83–88 (2018).
Toopchizadeh, V., Dolatkhah, N., Aghamohammadi, D., Rasouli, M. & Hashemian, M. Dietary inflammatory index is associated with pain intensity and some components of quality of life in patients with knee osteoarthritis. BMC Res. Notes. 13, 448 (2020).
Costa, D. et al. Trajectories of physical function and quality of life in people with osteoarthritis: results from a 10-year population-based cohort. BMC Public. Health. 23, 1407 (2023).
Törmälehto, S. et al. Eight-year trajectories of changes in health-related quality of life in knee osteoarthritis: data from the Osteoarthritis Initiative (OAI). PLoS One. 14, e0219902 (2019).
Han, A. & Gellhorn, A. C. Trajectories of Quality of Life and Associated Risk factors in patients with knee osteoarthritis: findings from the Osteoarthritis Initiative. Am. J. Phys. Med. Rehabil. 97, 620–627 (2018).
Goh, S-L. et al. Relative efficacy of different exercises for Pain, function, performance and quality of life in knee and hip osteoarthritis: systematic review and network Meta-analysis. Sports Med. 49, 743–761 (2019).
Skou, S. T., Pedersen, B. K., Abbott, J. H., Patterson, B. & Barton, C. Physical activity and Exercise Therapy Benefit more than just symptoms and impairments in people with hip and knee osteoarthritis. J. Orthop. Sports Phys. Ther. 48, 439–447 (2018).
Eckstein, F., Kwoh, C. K. & Link, T. M. Imaging research results from the osteoarthritis initiative (OAI): a review and lessons learned 10 years after start of enrolment. Ann. Rheum. Dis. 73, 1289–1300 (2014).
Kellgren, J. H. & Lawrence, J. S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 16, 494–502 (1957).
Collins, J. E., Katz, J. N., Dervan, E. E. & Losina, E. Trajectories and risk profiles of pain in persons with radiographic, symptomatic knee osteoarthritis: data from the osteoarthritis initiative. Osteoarthr. Cartil. 22, 622–630 (2014).
Ware, J., Kosinski, M. & Keller, S. D. A 12-Item short-form Health Survey: construction of scales and preliminary tests of reliability and validity. Med. Care. 34, 220–233 (1996).
Washburn, R. A., McAuley, E., Katula, J., Mihalko, S. L. & Boileau, R. A. The physical activity scale for the elderly (PASE): evidence for validity. J. Clin. Epidemiol. 52, 643–651 (1999).
Block, G., Hartman, A. M. & Naughton, D. A reduced dietary questionnaire: development and validation. Epidemiology 1, 58–64 (1990).
Hébert, J. R., Shivappa, N., Wirth, M. D., Hussey, J. R. & Hurley, T. G. Perspective: the Dietary Inflammatory Index (DII)-Lessons learned, improvements made, and future directions. Adv. Nutr. 10, 185–195 (2019).
Willett, W. C., Howe, G. R. & Kushi, L. H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. ;65: (1997).
Bellamy, N., Buchanan, W. W., Goldsmith, C. H., Campbell, J. & Stitt, L. W. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 15, 1833–1840 (1988).
Katz, J. N., Chang, L. C., Sangha, O., Fossel, A. H. & Bates, D. W. Can comorbidity be measured by questionnaire rather than medical record review? Med. Care. 34, 73–84 (1996).
Nagin, D. Analyzing Developmental trajectories: a Semiparametric, Group-Based Approach. Psychol. Methods. 4, 139–157 (1999).
Zang, E. & Max, J. T. Bayesian estimation and model selection in group-based trajectory models. Psychol. Methods. 27, 347–372 (2022).
Shivappa, N. et al. The relationship between the dietary inflammatory index (DII®) and incident depressive symptoms: a longitudinal cohort study. J. Affect. Disord. 235, 39–44 (2018).
Ma, C. et al. Dietary inflammatory index and magnetic resonance imaging-detected knee Structural Change and Pain: a 10.7-Year follow-up study. Arthritis Care Res. (Hoboken) ; (2024).
Veronese, N. et al. The relationship between the dietary inflammatory index and prevalence of radiographic symptomatic osteoarthritis: data from the Osteoarthritis Initiative. Eur. J. Nutr. 58, 253–260 (2019).
Liu, Q. et al. Inflammatory potential of diet and risk of incident knee osteoarthritis: a prospective cohort study. Arthritis Res. Ther. 22, 209 (2020).
Koehler, K., Drenowatz, C. & Editorial Understanding the Interaction between Physical Activity and Diet for the Promotion of Health and Fitness. Front. Nutr. 8, 835535 (2021).
Skou, S. T., Bricca, A. & Roos, E. M. The impact of physical activity level on the short- and long-term pain relief from supervised exercise therapy and education: a study of 12,796 Danish patients with knee osteoarthritis. Osteoarthr. Cartil. 26, 1474–1478 (2018).
Draganidis, D. et al. Disparate habitual physical activity and Dietary Intake profiles of Elderly men with Low and elevated systemic inflammation. Nutrients ;10: (2018).
Puts, S. et al. Exercise-induced effects on inflammatory markers and brain-derived neurotrophic factor in patients with knee osteoarthritis. A systematic review with meta-analysis. Exerc. Immunol. Rev. 29, 22–53 (2023).
Joseph, K. L., Dagfinrud, H., Christie, A., Hagen, K. B. & Tveter, A. T. Criterion validity of the International Physical Activity Questionnaire-Short Form (IPAQ-SF) for use in clinical practice in patients with osteoarthritis. BMC Musculoskelet. Disord. 22, 232 (2021).
Liao, C-D. et al. Effects of protein-Rich Nutritional Composition supplementation on Sarcopenia Indices and Physical Activity during Resistance Exercise training in older women with knee osteoarthritis. Nutrients ;13: (2021).
Solmi, M. et al. Network analysis of the relationship between depressive symptoms, demographics, nutrition, quality of life and medical condition factors in the Osteoarthritis Initiative database cohort of elderly north-american adults with or at risk for osteoarthritis. Epidemiol. Psychiatr Sci. 29, e14 (2019).
Bell, A. Life-course and cohort trajectories of mental health in the UK, 1991–2008–a multilevel age-period-cohort analysis. Soc. Sci. Med. 120, 21–30 (2014).
MacKillop, J. et al. Hazardous drinking and alcohol use disorders. Nat. Rev. Dis. Primers. 8, 80 (2022).
Anderson, P. The impact of alcoholic beverages on Human Health. Nutrients ;13: (2021).
Wiczinski, E., Döring, A., John, J. & von Lengerke, T. Obesity and health-related quality of life: does social support moderate existing associations? Br. J. Health Psychol. 14, 717–734 (2009).
Acknowledgements
CZ, ZH, CH, and LB designed research; CZ and ZH conducted research; CZ analyzed data; and CZ, ZH, JJ, SC, CH, and LB wrote the paper. LB had primary responsibility for final content. All authors read and approved the final manuscript.
Funding
The study was supported by the National Natural Science Foundation of China (grant numbers 82102661) and Peking University Third Hospital Key Project (BYSYRCYJ2024003). Data from the OAI have been used for this study.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, Z., Zhang, H., Jin, J. et al. A longitudinal study of dietary inflammatory index and quality of life in people with osteoarthritis: data from the Osteoarthritis Initiative database. Sci Rep 15, 6024 (2025). https://doi.org/10.1038/s41598-025-86431-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-86431-y
