
Abstract
Parents influence the physical activity (PA) of the childhood cancer survivors (CCS). This mixed-methods study, aiming to obtain an understanding of Chinese parents’ perceptions of PA in CCS and how the cancer experience changes their views, which may affect these children’s PA engagement. A mixed methods study was conducted at two hospitals in Hangzhou. A qualitative investigation using the thematic descriptive phenomenological approach analyzed data concerning the parents of 9-18-year-old childhood cancer survivors who had completed hospitalized treatment for at least three months. A cross-sectional investigation examined the association between parents’ attitudes and children’s PA levels using unconditioned binary logistic regression analysis. The qualitative investigation included 35 parents (74.3% female). More than half of the parents understood the benefits of regular PA. Most parents supported children’s participation in low-intensity PA, but opposed high-intensity activities. Many parents changed their parenting style after cancer diagnosis, which might affect the development and persistence of children’s PA. In the cross-sectional investigation, CCS were more likely to engage in low-level moderate-to-vigorous physical activity (MVPA) or less MVPA when receiving less paternal support (adjusted OR = 0.92, 95%CI:0.88–0.96) and maternal support (adjusted OR = 0.91, 95%CI:0.87–0.95). Insufficient paternal MVPA engagement (adjusted OR = 3.83, 95%CI: 2.57–5.70) and maternal MVPA engagement (adjusted OR = 5.65, 95%CI: 3.74–8.54) were associated with lower MVPA engagement in CCS. This study identified the understanding of parents of childhood cancer survivors concerning PA engagement and related life changes brought about by cancer experiences from the parental perspectives. These changes affect parental attitude towards children’s participation in PA, and parental attitude and behavior affect children’s participation in PA. Based on the above findings, some tentative practical implications for physical activity participation among childhood cancer survivors are drawn: (1) childhood cancer survivors should be encouraged to participate in more MVPA and consult a rehabilitation physician if necessary; (2) parents and children engage in exercise together is an important way to promote the levels of physical activity among childhood cancer survivors; (3) Chinese parents have insufficient awareness of the benefits of childhood cancer survivors participation in physical activity. We should strengthen health education for parents, promote parents to support childhood cancer survivors participate in physical activity.
Similar content being viewed by others


Introduction
Cancer and its treatment still cause serious harm to the health of childhood cancer survivors (CCS), and these treatment-related complications can last for a long time after the completion of treatment1. In addition to the side effects of the disease and treatment, lack of PA after the diagnosis of cancer will have a further adverse impact on health. For children who have completed treatment, regular PA (regular PA refers to at least 150 min of moderate-to-vigorous physical activity [MVPA] per week)2 is an effective way to enhance or maintain functional activities, physical performance, psychological well-being and health-related quality of life3,4,5, which can contribute to an overall decrease in chronic disease morbidity and mortality6. However, most CCS have difficulty participating in regular PA for various reasons7,8,9. To promote the long-term health of CCS, an array of studies focusing on the promotion of PA in CCS have been widely carried out in Western countries5. Studies exploring the influence of healthy children’s PA and exercise behaviour have confirmed that parental PA behaviour, knowledge beliefs, support and family sports environments are associated promoting children’s PA10,11. Considering that CCS are more dependent on parents during the process of cancer diagnosis and treatment, parents may have a greater impact on the PA of CCS than on healthy children and adolescents12. A recent study showed that parental support and family involvement are key factors in promoting PA among CCS13, while parental misunderstanding of PA is one of the major barriers affecting the PA levels of hospitalised children14. Norris et al.15 reported that mothers’ PA was significantly correlated with the PA of CCS, which is consistent with the finding that among family members, children prefer to choose their mother among family members as their exercise partner16. In addition to these common parental factors, parents can affect the PA by building a family PA environment13. However, the influence of parents and other family factors on children’s PA is multifaceted and multi-factorial, and the influence of Chinese parents on the PA of CCS has been rarely reported.
There are tremendous differences between the cultural backgrounds of China and Western countries, with potentially differing influences affecting Chinese parents and families on shaping children’s PA behaviour. Therefore, Chinese parents’ attitudes and viewpoint towards the PA of CCS need to be explored. The purpose of the current study was to gain a comprehensive understanding of Chinese parents’ perceptions of PA in CCS, how children’s cancer experiences changed their views and parental factors associated with PA in CCS.
Materials and methods
This study combined qualitative and quantitative methods to comprehensively explore the influence of parental factors on the PA of CCS. An exploratory qualitative investigation was conducted to explore the perspectives of both children and their parents regarding CCS’ participation in PA, and analyze the impact of childhood cancer on parental viewpoints. As the results of the children’s interviews have been previously published17, we only present and analyse the results of parent interviews in this investigation. This study employed a descriptive phenomenological approach to depict the experiences and attitudes of parents of CCS towards PA. Parents were interviewed face-to-face to collect information. The confirmatory cross-sectional survey mainly focused on verifying the influence of parental attitude, parental behaviour and family social status on the PA of CCS. Findings from both the qualitative and quantitative elements are drawn together in the discussion.
This study was approved by the Ethics Committee of XX University School of Public Health (******) and the Ethics Committee of the Children’s Hospital of XX University School of Medicine (*******).
Qualitative methods
Participants
Purposive sampling was used to recruit participants with different types of cancers and diverse sociodemographic backgrounds. Parents of CCS who were attending medical follow-ups in four pediatric oncology outpatient departments from two hospitals in XX (Children’s Hospital of XX University & YY Third Hospital) and who met the inclusion criteria were invited to participate in the study. The study design inclusion criteria were as follows: (1) parents of CCS aged between 9 and 18 years who had been diagnosed with pediatric cancer without physical disabilities; (2) their children had completed at least 3 months of hospitalized treatment prior to joining the study; (3) they were the primary caregiver of their child, either father or mother; and (4) they could read and understand Chinese.
The study was conducted until data saturation was reached in each interview set, which was defined as the absence of new themes in the last three interviews18.
Data collection
This qualitative study was conducted between September and December 2020. Before attending the interview, the participants were asked to sign an informed consent form and complete a questionnaire related to their demographic characteristics. The questionnaire included questions on their relationships with the child, gender, age, education level, marital status, employment status, annual household income and attitudes towards the child’s participation in PA. When primary information collection was completed, the face-to-face interview process began and lasted approximately 30 min under two research assistants who worked on interviewing and audio recording. The interview context applied family system theory that involved using open and neutral questions under five sections: (1) recognition of the need for regular PA; (2) perceived benefits and risks of PA; (3) attitudes towards participation in PA by CCS; (4) parents’ own participation in PA; and (5) changes in parenting styles (Supplementary File 1). The interview outline followed that used in similar studies13,14,19. Relevant experts (two in clinical pediatric oncology, two in public health and one pediatric nurse) confirmed the interview outline, and experienced interview personnel confirmed the wording of the questions.
Data analysis
We analysed the transcripts using thematic framework analysis20 and inductively identified and structured the emergent themes. A group consensus process was also implemented. First, after reading the transcribed text repeatedly, three research assistants built a codebook through group discussions. Second, two of them coded the transcripts independently and reached a consensus using NVivo (version 12.0), a qualitative data management and analysis software program. Finally, the coded and classified data were combined and collated, followed by a descriptive analysis.
Quantitative methods
Participants
In this cross-sectional investigation, we collected information concerning the CCS and their parents. Since children younger than 10 years of age may have difficulty accurately estimating the time and intensity of their PA participation, we only included children aged 10–18 years old, as suggested by the developers of the scale used in this study (Godin Leisure Time Exercise Questionnaire, GLTEQ). The other inclusion criteria were identical to those used in the qualitative study.
Data collection
From July 2021 to June 2022, eligible patients were first screened through the hospital’s electronic medical record system to form a patient information list, and parents of CCS were contacted individually by phone. If they agreed to complete the questionnaire, a URL was sent to their mobile phone via text messages or WeChat messages. The questionnaire includes the parent response part and the child response part. We collected information on socio-demographic, disease, parental and family characteristics, parents’ attitudes towards their children’s participation in PA, and PA behaviors. The CCS reported their participation in PA.
Measurements
Background characteristics
The parental questionnaire sought details concerning the parental age, education level, marital status, employment status, household income, attitudes towards their children’s participation in sports, and disease.
PA behavior: In this study, we used the GLTEQ21 to assess the current MVPA behaviour of children and their parents. The GLTEQ consists of three questions that assess the duration and frequency of mild, moderate, and vigorous PA during a week22. In this study, we utilized the duration of participation in moderate and vigorous PA to assess the level of MVPA among participant. When the Leisure Score Index (LSI) score is 24 or above, the participant is deemed physically active22. The GLTEQ has demonstrated reliability and concurrent validity for measuring PA in children and adults23.
Parental support: The Activity Support Scale (ACTS), developed by Davison, was used to assess parents’ attitudes towards CCS participation activities24. The ACTS comprises two independent sections, the father section and the mother section, each with 9 items. A four-point Likert scale ranging from “strongly disagree” to “strongly agree,” scored 1 to 4 respectively, is used. Higher scores indicate greater parental support. The Cronbach’s α coefficients of the overall scale is above 0.8, demonstrating good construct validity and internal consistency. The scale can effectively reflect parents’ support for PA engagement among children and adolescents25.
Data analysis
Multivariable regression analysis was used to examine the relationships among parental attitude, paternal MVPA, maternal MVPA and MVPA engagement of CCS.
Results
Qualitative results
Parents’ characteristic
Because of a low willingness to attend and schedule conflicts, five parents failed to attend the interview; finally, the study involved 35 participants, with a response rate of 87.50%, among whom mothers predominated (n = 26; 74.29%). As shown in Table 1, the parents’ ages (mean = 40.51, standard deviation [SD] = 5.48) ranged from 32 to 52 years. Except for 10 parents (28.57%) who had received college or higher education, most parents were poorly educated. Eight (22.86%), 11 (31.43%) and six (17.14%) parents had graduated from primary school, middle school and high school education, respectively. Almost all the parents (n = 34, 97.14%) were married, except for one who was divorced. More than half of the parents (n = 23, 65.71%) had full-time jobs, four (11.43%) had part-time jobs and seven (20.00%) took care of their families as housewives. Regarding annual family income, more than half of the households (n = 22, 62.86%) earned about between 3400 and 8,000 dollars (24,000–56,000 yuan) each year, nine families (25.71%) earned less than 3,400 dollars and four families (11.43%) earned more than 8,000 dollars.
Qualitative data themes
The qualitative data were divided into the following themes: Theme (1) Recognition of PA, Theme (2) Attitude towards children’s participation in PA, Theme (3) PA behaviour and Theme (4) The impact of the cancer experience on their lives.
Theme 1. Recognition of PA
Sub-theme 1.1: limited understanding of regular PA
More than 50% of the parents had a basic understanding of regular PA and could roughly describe the frequency or type of regular exercise in combination with their own or their children’s situations, but their understanding was still not comprehensive.
“I think it should be two or three times a week. Usually brisk walking generally, there seems to be no other sports in the countryside.” (CBF).
Some parents also reported that they never paid attention to regular PA. Therefore, they knew little about regular PA and could not correctly guide their children on how to engage in it.
“I still don’t quite understand it, I don’t know much about this thing. Because I don’t understand it and I have no idea of putting it into practice. We can’t keep up with others’ ideas, and I don’t understand what it means. We don’t know how to exercise. We can only do what we usually do. ” (FYT).
Sub-theme 1.2:benefits of PA
Most parents were aware that long-term inactivity was harmful to health, while appropriate exercise could promote physical recovery, enhance resistance, strengthen health, control weight and be conducive to children’s growth and development. Outdoor activities also helped in terms of breathing fresh air. Indeed, some parents had created opportunities for their children to go out and exercise, hoping that they would engage in more activities and reduce their sitting time.
“It’s better for the body and meridians. I think exercise is still necessary. If you don’t do exercise and lie there, it must be get worse and worse. Just like us in confinement, lying down all the time can can make one sick. I think it’s good to have activities even if we only walk a bit.” (XHB).
In addition to physical health, a few parents realized that outdoor activities could bring psychological and emotional changes to children, such as creating a good mood.
“If you go outside more, you will be more cheerful.” (CBF).
“Participating in sports is good for children’s psychological state.” (SHXY).
Sub-theme 1.3: hazards of PA
Many parents also recognized potential adverse physical consequences of exercise for their children such as injury or overexertion, which might aggravate their illness. In particular, when a child was still in the early stage of finishing hospitalized treatment, their body was also involved with auxiliary treatment equipment (e.g., infusion ports, peripherally inserted central catheters and joint prosthess). If they exercise improperly, children are more likely to experience serious consequences. Consequently, the parents often instructed their children to avoid high-intensity activities and limit the types of activities in which they could participate.
“I told her just not to do intensive activities. I didn’t let her exercise for a period of time after the operation. I’m afraid the wound would open. Even now I think it’s still necessary to control the amount of exercise.” (ZXY).
Theme 2: attitude towards children’s participation in PA
Most parents were supportive of their children’s participation in light activities (such as walking), while they were relatively resistant to children’s participation in high-intensity activities such as competitions or school physical education. Some parents asked their children to reduce their engagement in physical education, or communicate with the teacher directly to obtain the teacher’s understanding and support, and did not allow children to join high-intensity activities. Particularly when more vigorous exercise had been involved prior to a child’s illness, the parents would be more cautious.
“I don’t support it. I’ve asked him to drop out of physical education during school. I think he can take a walk in a flat place in the morning, noon and evening. That’s all.” (QXN).
“Physical exercise, if it is light, we will be supportive of her participation. We dare not allow her to do strenuous exercise, because before she got sick, she often had to jump up because of strenuous exercise and badminton learning. " (FXY).
Some children had completed the treatment not long beforehand. The implantation of treatment equipment such as infusion ports, ventricular shunt tubes and artificial joints increases the risk of injury for children participating in activities. Parents had a more negative attitude towards their children’s participation in PA in such cases, hoping that their children would rest more and engage in fewer activities.
“Before, we often climbed mountains, but then he fell ill, I think he should have more rest… Now he has an infusion port installed in his body, and I dare not let him do strenuous activities. If the infusion port can be removed next year, he can do proper activities.” (WHL).
Theme 3: PA behaviour
Sub-theme 3.1: parents’ own PA behaviour
Among the parents interviewed, only a very small number performed regular PA, while most parents rarely or did not participate in PA. Almost all the parents who did not participate in PA stated that they had no time to participate in PA because of their busy work hours. Some parents reported that after their children fell ill, their family’s economic burden increased, and they felt under greater psychological pressure and were in no mood to think about their own exercise. Some parents said that they were very tired at work or did manual work; therefore, they did not need extra exercise.
“I don’t have time to attend at all. Because right now, to be honest, my family financial pressure is quite heavy. I have to spend a long time at work (mom cries). Basically, I go to work every day, and sometimes I can’t go home until eight or nine o’clock or one or two o’clock at night.” (ZYJ).
“I have no time. Because I work all day long, I have enough exercise, I am tired enough at work, I don’t need exercise anymore.” (HRY).
The parents’ comments indicated that having a child with cancer had increased the financial burden on the family and the burden of parental care and had indirectly influenced the behaviour of parents to some extent and changed their lifestyle.
Sub-theme 3.2: parents’ efforts to encourage children’s PA behaviour
Most parents will actively urge their children to perform PA in their daily lives and provided practical help for their children to participate in PA. When there was time, parents chose to accompany their children in performing activities.
“Sometimes, for example, in the evening, I would take him out for a walk after he finished his homework.” (FHR).
Some parents also supported children’s participation in PA, but due to a lack of knowledge and skills concerning effective PA, they were more concerned about their children’s participation in PA and indifferent towards PA, and did not actively urge their children to participate in PA.
“Because of this concern (physical injury caused by sports), we didn’t urge him… on weekends, he often watches TV, if he doesn’t want to walk, we let him go.” (ZCY).
Supportive attitudes and sports knowledge/ skills were prerequisites for parents in terms of encouraging their children to engage in PA. Parents with supportive attitudes were psychologically better prepared to encourage their children to carry out PA, while having correct PA knowledge and skills was the triggering condition.
Theme 4: the impact of the cancer experience on their lives
Sub-theme 4.1 changes in values
The experiences of children suffering from cancer have had a significant impact on their families. Before being diagnosed with cancer, most parents attached great importance to their children’s academic performance and hoped that their children would achieve academic success. When cancer was confirmed, most parents lowered their expectations of their children’s academic performance and paid more attention to their children’s physical health and life needs.
“I used to have very high expectation for her. I wanted her to study hard and have a better future. But now, I only wish her to be healthy, to be able to stand up and walk, to move, I don’t care anything else.” (LXY).
“In the past, we paid more attention to his study. We were very strict with him. But now we pay more attention to his life. The focus has changed. " (MZY).
Some parents believed that their child had already experienced overwhelming pain during the illness so they did not want their child to study hard but rather to keep a healthy body as a new goal. These parents were also more meticulous in terms of spending time with their children and cherishing their time with their children, sometimes to the point of reducing work hours.
“I definitely care more about her than before she was sick. No matter what, I will do anything for her as long as I can. Sometimes, I’d rather shut the door (the parent has a barbershop) for half a day. I’d take her out for a walk, just to get some air and get some exercise.” (CRR).
Sub-theme 4.2 change of parenting style
The majority of parents reported that their attitudes towards their child had improved compared to the days before their child became sick. Previously, the parents had usually been more demanding, controlling and autocratic, often shouting at their children when disciplining them; however, after the disease was confirmed, they felt that they needed to be more patient and reasonable with their children, and to be more accepting of their difficult situation as a family. The parents now tended to no longer force their children to do things, cared more about their children’s feelings and respected their wishes.
“My attitude has changed a lot. I used to be very grumpy. I would scold him if he didn’t obey me. Now I think, it is a hard-won fate that he came to my life. Because of that, I will endure it when sometimes he is not very obedient. Now, although he is disobedient sometimes, I can bear it and just use my loud voice occasionally. " (THW).
Several parents have gone to the the extreme of doting on their child, hoping to emotionally compensate for the damage caused by the illness .
“Now I spoil and indulge him, unlike before. Since he got sick, he had a bad temper, and we can’t deal with him. We stayed in the hospital to accompany him in the first half of the year. Everything was done according to his wishes during that time and I am still tolerant of him in life and study.” (ZJL).
Cross-sectional results
Participants’ characteristics
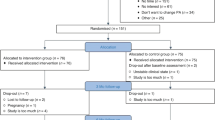
In the cross-sectional investigation survey, 993 CCS were screened. After telephone contact, 186 CCS lost to follow-up and death were excluded, and 807 CCS were approached, of whom 503 completed and returned questionnaires (response rate, 62.33%). Over half of the participants were male (n = 270, 53.68%). Their ages ranged from 10 to 18 years (mean = 13.23, SD = 2.46). Among the CCS, the most common diagnosis was leukaemia. More specific information is provided in Table 2.
In seven of the children surveyed, the guardians were not their parents. As Table 3 shows, 472 fathers and 481 mothers participated in the survey. More than half of the parents (fathers: 67.79%, mothers: 60.71%) had secondary education. Only a few fathers (n = 19, 4.03%) were unemployed, whereas more mothers (n = 99, 20.58%) were unemployed. In terms of MVPA participation, more than half of both fathers (61.44%) and mothers (52.81%) actively participated. The family information is shown in Table 4. Most of the parents were married or living together. Regarding the economic impact of cancer on the families, most families of CCS had been moderately to severely affected.
Parental support and parental PA behaviour in relation to the PA behaviour of the CCS
Parental attitudes and behaviour were closely associated with the PA behaviour of CCS. Parental support encouraged the CCS to participate in higher-level MVPA. The more supportive the father (adjusted OR = 0.94, 95%CI: 0.90–0.98, p = 0.003) and/or the mother (adjusted OR = 0.93, 95%CI: 0.89–0.97, p<0.001 ), the higher the child’s MVPA levels. High parental levels of MVPA behaviour also promoted the PA behaviour of CCS. When the father (adjusted OR = 4.45, 95%CI: 2.83–6.99, p<0.001) and/or the mother (adjusted OR = 6.26, 95%CI: 3.94–9.96, p<0.001) engaged in more MVPA, it was more likely for the CCS to participate in higher-level MVPA. More specific information is shown in Table 5.
Discussion
According to family system theory, the characteristics of parents are important factors affecting children’s behavioural development26. To explore the parental and family factors affecting children’s PA, we first evaluated parental recognition of PA. In this study, more than half of the parents had a certain understanding of the need for regular PA, while some paid less attention to PA as they knew little about it. To some extent, this result reflects that Chinese parents of CCS are generally less aware of PA, which is related to the fact that most people in China are not concerned about exercise27. In some theoretical models of health behaviour (i.e. the knowledge–attitude–practice model), the score for behavioural knowledge is closely associated with the occurrence of behaviour28. If parents have little knowledge of PA, they cannot guide their children to perform PA correctly. However, Xu examined the relationship between parents’ health, sports knowledge and children’s sports participation, and found that the conversion rate from knowledge to behaviour was not high29 and the impact of knowledge on behaviour was limited. The pathway from knowledge to behaviour may be mediated by other cognitive factors such as the benefits and risks of PA. It is widely recognized that PA can enhance health and promote the growth and development of children, including CCS30. The parents were also aware that improper exercise could cause physical harm to their children. In fact, many children do not fully recover in the early stages after hospitalization, and some of them still retain treatment equipment (e.g., port-catheter systems and joint prostheses). Moreover, many parents lack the knowledge and skills to conduct activities safely and effectively in a cancer setting, and their ability to increase the PA of CCS is limited13.
Many studies on children without cancer have shown that parental support is positively correlated with children’s participation in and maintenance of PA31,32. The same correlation holds true for MVPA participation among CCS33. In this study, we found that parental support was closely related to the participation of CCS in MVPA. However, not all parents supported the participation of CCS in sports. Given the coexistence of beneficial and harmful physical activities for CCS, parents’ attitudes towards their children’s participation in MVPA were mixed and contradictory. On the one hand, they hoped that their children could participate in more activities to promote physical health; on the other hand, they worried that sports injuries might happen and inhibit rehabilitation. In line with a previous study13,14, this attitude suggests that parents would tend to support CCS to participate in low-intensity PA, but oppose high-intensity activities that they believe are risky for CCS. Cheung et al. found that more than half of parents misunderstood CCS participation in PA, which was thought to lead to or even aggravate fatigue13. Such parental concerns are reasonable because they lack the guidance of professional rehabilitation personnel. It is necessary to educate parents about PA knowledge and techniques during follow-ups to improve their understanding of PA.
Parental behaviour is another important factor affecting children’s behaviour development in the family, which not only plays a role in behaviour demonstration for children but also shapes children’s behaviour by affecting the family environment12. Our study also showed that parental PA behaviour was a direct predictor of the PA levels of CCS. Regrettably, most parents of the CCS rarely participated in the exercises, which is consistent with the results of a previous study34 that surveyed the parents of CCS from more than 10 medical centers. These parents reported that all their health-related behaviour, especially in terms of unhealthy diet and nutritional intake, less PA and less time spent on recreational activities, had deteriorated significantly. The fundamental cause of this was that parents had to undertake more care-giving responsibilities and had many disease-related stressors. In this study, the parents also reported many reasons for their low PA levels, such as busy work (no time), economic burden, psychological pressure and bad mood. Further economic reasons for low PA were also found in the sociodemographic data reported by the parents (such as family income and children’s medical insurance). The annual household income reported by the parents indicated that most families were at a lower–middle socioeconomic level. Moreover, the children had only basic medical insurance, except for one who had commercial insurance. In China, if someone has cancer and relies only on basic medical insurance, the family is likely to face major economic pressure35. As in other developing countries, some families have to exhaust their savings in such situations and may even be in debt36. The relevance of parent-child behavioral interaction once again underscores the need to incorporate parents into PA interventions for CCS.
Childhood cancer is a devastating diagnosis for children and their parents and severely disrupts the lifestyle of the family unit, having a profound impact on parents, parent–child relationships and the whole family environment37. Many parents revalued what was important to them and created a new ranking of important things in life. Most Chinese parents have high academic expectations and strict requirements for their children, hoping that their children advance professionally, gain a decent and well-paid job through study and live a financially secure life38, which they believe represents a successful life. In such a cultural background that tends to define success in a single and one-sided way, Chinese parents are inclined to mainly focus their concerns on their children’s academic performance, and children give up rest and exercise time for learning; however, the diagnosis of cancer pushes parents to realize that they may lose their children. Parents in such cases have to ask their children to strictly abide by the treatment plan, reduce their expectations for children’s academic performance, and no longer demand that their children single-mindedly pursue greater knowledge and stay up late in pursuit of academic performance; this result is similar to findings concerning the parents of CCS in Hong Kong39, whereas parents’ obsession with academic performance is rarely found in studies in Western countries. After their child’s cancer diagnosis, concern for the future makes parents sense that the most important thing in life is to cherish the present moment40, make full use of their time with their children and enjoy their time together. These positive changes in values tend to encourage parents to become more inclusive of their children and respect their children’s wishes more when they meet behavioral requirements.
Childhood cancer experiences also influenced parenting styles. Parenting style refers to a combination of parenting concepts, parenting behaviour and emotional expression for children, which reflect the basic strategies used by parents in the process of parenting41. In traditional Chinese culture, authoritarian parenting has always been highly respected, which involves severe punishment and restrictive parenting42. Authoritarian parents often oblige their children to obey instructions without explaining or responding to them, or paying attention to their children’s feelings. Corporal punishment and shouting are the usual forms of discipline used by parents with authoritarian values. With the occurrence and treatment of cancer, parents witness the illness and treatment devastating the child’s body. These painful experiences can inspire parents to love and protect their child more comprehensively43. Many parents had begun to rethink their behaviour and how they treated their children. They did not want to add any physical or psychological pain to their children; therefore, the parents were willing to express their feelings and show more emotional warmth and understanding of their children. Consequently, they tended to be more willing to consider their children’s wishes in terms of behavioral requirements and adopt a tolerant approach in terms of diet and exercise12. However, if the degree of parenting style change is not well controlled, it may become counterproductive such that parents show more love for the CCS, favoring them over their brothers and sisters and spoiling them44. An overly lax parenting style is not conducive to the cultivation of healthy behaviour in children.
Our study had some limitations. First, the single-setting recruitment may have limited the generalisability of our findings. Second, we recruited parents of CCS aged between 9 and 18 years old, and parents of children under this age range were not eligible for our study. Therefore, the results do not apply to the parents of the youngest CCS. Third, although we sought to recruit parents of children with different cancers, patients were difficult to find because of the relatively limited differing types of tumors.
Conclusion
This mixed-methods study provides insights into the perspectives on PA among Chinese parents of CCS, which enriches the current literature in relation to findings from different cultural backgrounds. Our findings indicated that Chinese parents’ safety concerns about PA participation for CCS led them to support their engagement in light activities. Parental support promoted the participation of CCS in MVPA, and parental PA behaviour was closely associated with CCS engagement. Chinese parents need to increase their efforts to shape their family PA environment. A permissive parenting style formed after a child’s illness was not found to be conducive to the development of children’s PA.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
References
Landier, W. et al. Surveillance for late effects in childhood cancer survivors. J. Clin. Oncol. 36(21), 2216–2222. https://doi.org/10.1200/jco.2017.77.0180 (2018).
Chung, O. K., Li, H. C., Chiu, S. Y., Ho, K. Y. & Lopez, V. The impact of cancer and its treatment on physical activity levels and behavior in Hong Kong Chinese childhood cancer survivors. Cancer Nurs. 37(3), E43–51. https://doi.org/10.1097/NCC.0b013e3182980255 (2014).
Wurz, A., McLaughlin, E., Lategan, C., Ellis, K. & Culos-Reed, S. N. Synthesizing the literature on physical activity among children and adolescents affected by cancer: evidence for the international Pediatric Oncology Exercise guidelines (iPOEG). Transl. Behav. Med. 11(3), 699–708. https://doi.org/10.1093/tbm/ibaa136 (2021).
Wurz, A. et al. The international pediatric oncology exercise guidelines (iPOEG). Transl. Behav. Med. 11(10), 1915–1922. https://doi.org/10.1093/tbm/ibab028 (2021).
Morales, J. S. et al. Exercise and Childhood Cancer-A historical review. Cancers (Basel). 14(1). https://doi.org/10.3390/cancers14010082 (2021).
Scott, J. M. et al. Association of exercise with mortality in adult survivors of childhood cancer. JAMA Oncol. 4(10), 1352–1358. https://doi.org/10.1001/jamaoncol.2018.2254 (2018).
Ha, L. et al. Accuracy of perceived physical activity and fitness levels among childhood cancer survivors. Pediatr. Blood Cancer. 68(9), e29134. https://doi.org/10.1002/pbc.29134 (2021).
Yeo, Y. et al. Self-reported physical activity behaviors of childhood cancer survivors: comparison to a general adolescent population in Korea. Support Care Cancer 31(3), 164. https://doi.org/10.1007/s00520-023-07612-x (2023).
Li, W. H. C., Cheung, A. T., Ho, L. K. & Chung, J. O. K. Promoting physical activity among Childhood Cancer survivors: the Way Forward. Cancer Nurs. 46(1), 86–87. https://doi.org/10.1097/ncc.0000000000001182 (2023).
Rhodes, R. E. et al. Development of a consensus statement on the role of the family in the physical activity, sedentary, and sleep behaviours of children and youth. Int. J. Behav. Nutr. Phys. Act. 17(1), 74. https://doi.org/10.1186/s12966-020-00973-0 (2020).
Wilk, P., Clark, A. F., Maltby, A., Tucker, P. & Gilliland, J. A. Exploring the effect of parental influence on children’s physical activity: the mediating role of children’s perceptions of parental support. Prev. Med. 106, 79–85. https://doi.org/10.1016/j.ypmed.2017.10.018 (2018).
Santa Maria, D. et al. Exploring parental factors related to weight management in survivors of childhood central nervous system tumors. J. Pediatr. Oncol. Nurs. 31(2), 84–94. https://doi.org/10.1177/1043454213518112 (2014).
Cheung, A. T., Li, W. H. C., Ho, L. L. K., Chan, G. C. F. & Chung, J. O. K. Parental perspectives on promoting physical activity for their children surviving cancer: a qualitative study. Patient Educ. Couns. 104(7), 1719–1725. https://doi.org/10.1016/j.pec.2020.11.009 (2021).
Wright, M. Physical activity participation and preferences: Developmental and Oncology-related transitions in adolescents treated for Cancer. Physiother Can. 67(3), 292–299. https://doi.org/10.3138/ptc.2014-25LHC (2015).
Norris, J. M., Moules, N. J., Pelletier, G. & Culos-Reed, S. N. Families of young pediatric cancer survivors: a cross-sectional survey examining physical activity behavior and health-related quality of life. J. Pediatr. Oncol. Nurs. 27(4), 196–208. https://doi.org/10.1177/1043454209358411 (2010).
Badr, H., Paxton, R. J., Ater, J. L., Urbauer, D. & Demark-Wahnefried, W. Health behaviors and weight status of childhood cancer survivors and their parents: similarities and opportunities for joint interventions. J. Am. Diet. Assoc. 111(12), 1917–1923. https://doi.org/10.1016/j.jada.2011.09.004 (2011).
Xu, F. et al. Associated factors on physical activity among childhood cancer survivors in Mainland China: a qualitative exploration applied health belief model. Support Care Cancer. 30(11), 9221–9232. https://doi.org/10.1007/s00520-022-07324-8 (2022).
Francis, J. J. et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol. Health. 25(10), 1229–1245. https://doi.org/10.1080/08870440903194015 (2010).
Grimshaw, S. L., Taylor, N. F., Mechinaud, F., Conyers, R. & Shields, N. Physical activity for children undergoing acute cancer treatment: a qualitative study of parental perspectives. Pediatr. Blood Cancer. 67(6), e28264. https://doi.org/10.1002/pbc.28264 (2020).
Wang, T., Chen, J., Hu, D. & Wang, Y. Qualitative data were analyzed by subject frame method. Chin. Health Resour. 02, 86–88 (2006).
Godin, G. & Shephard, R. J. A simple method to assess exercise behavior in the community. Can. J. Appl. Sport Sci. 10(3), 141–146 (1985).
Amireault, S. & Godin, G. The Godin-Shephard leisure-time physical activity questionnaire: validity evidence supporting its use for classifying healthy adults into active and insufficiently active categories. Percept. Motor Skills. 120(2), 604–622. https://doi.org/10.2466/03.27.PMS.120v19x7 (2015).
Amireault, S., Godin, G., Lacombe, J. & Sabiston, C. M. The use of the Godin-Shephard leisure-time physical activity questionnaire in oncology research: a systematic review. BMC Med. Res. Methodol. 15, 60. https://doi.org/10.1186/s12874-015-0045-7 (2015).
Davison, K. K. Activity-related support from parents, peers, and siblings and adolescents ' physical activity: are there gender differences? J. Phys. Act. Health. 1(4), 363–376. https://doi.org/10.1123/jpah.1.4.363 (2004).
Guo, Q., Wang, X. & Jiang, J. The patterns of physical activity and sedentary behavior in Chinese children and adolescents. China Sport Sci. 37(7), 13. https://doi.org/10.16469/j.css.201707003 (2017).
Plamondon, A., Bouchard, G. & Lachance-Grzela, M. Family dynamics and young adults’ well-being: The mediating role of sibling bullying. J. Interpers. Violence 36(9–10), np5362–np5384. https://doi.org/10.1177/0886260518800313 (2021).
Chen, P. et al. Physical activity and health in Chinese children and adolescents: expert consensus statement (2020). Br. J. Sports Med. 54(22), 1321–1331. https://doi.org/10.1136/bjsports-2020-102261 (2020).
Angeles-Agdeppa, I., Monville-Oro, E., Gonsalves, J. F. & Capanzana, M. V. Integrated school based nutrition programme improved the knowledge of mother and schoolchildren. Matern Child. Nutr. 15(Suppl 3), e12794. https://doi.org/10.1111/mcn.12794 (2019). Suppl 3.
Xu, X. The Relationship between Parents and Children’s Sports Participation: Based on the Model of Knowledge, Attitude and Practice (Beijing Sport University, 2013).
Kim, J. Y. et al. Physical activity levels, exercise preferences, and exercise barriers in Korean children and adolescents after cancer treatment. Support Care Cancer. 30(2), 1787–1796. https://doi.org/10.1007/s00520-021-06588-w (2022).
Yao, C. A. & Rhodes, R. E. Parental correlates in child and adolescent physical activity: a meta-analysis. Int. J. Behav. Nutr. Phys. Act. 12, 10. https://doi.org/10.1186/s12966-015-0163-y (2015).
Rhodes, R. E., Perdew, M. & Malli, S. Correlates of parental support of child and youth physical activity: a systematic review. Int. J. Behav. Med. 27(6), 636–646. https://doi.org/10.1007/s12529-020-09909-1 (2020).
Zheng, J. et al. Individual, interpersonal, and home environmental factors influencing health behaviors among Chinese childhood cancer survivors: a structural equation analysis. Cancer Nurs. https://doi.org/10.1097/ncc.0000000000000991 (2021).
Wiener, L. et al. Impact of caregiving for a child with cancer on parental health behaviors, relationship quality, and spiritual faith: do lone parents fare worse? J. Pediatr. Oncol. Nurs. 33(5), 378–386. https://doi.org/10.1177/1043454215616610 (2016).
Wang, J. W. et al. A qualitative exploration of the unmet psychosocial rehabilitation needs of cancer survivors in China. Psychooncology 25(8), 905–912. https://doi.org/10.1002/pon.4023 (2016).
Islam, M. Z., Farjana, S. & Efa, S. S. Impact of childhood cancer on the family: evidence from Bangladesh. Heliyon 7(2), e06256. https://doi.org/10.1016/j.heliyon.2021.e06256 (2021).
Borrescio-Higa, F. & Valdés, N. The psychosocial burden of families with Childhood Blood Cancer. Int. J. Environ. Res. Public. Health. 19(1). https://doi.org/10.3390/ijerph19010599 (2022).
Guo, A. Research on the current situation of Parents’ Educational concept for Junior High School Students (Northeast Normal University, 2021).
Wong, M. Y. & Chan, S. W. The qualitative experience of Chinese parents with children diagnosed of cancer. J. Clin. Nurs. 15(6), 710–717. https://doi.org/10.1111/j.1365-2702.2006.01297.x (2006).
Schweitzer, R., Griffiths, M. & Yates, P. Parental experience of childhood cancer using interpretative phenomenological analysis. Psychol. Health. 27(6), 704–720. https://doi.org/10.1080/08870446.2011.622379 (2012).
Neel, M. L. M., Stark, A. R. & Maitre, N. L. Parenting style impacts cognitive and behavioural outcomes of former preterm infants: a systematic review. Child. Care Health Dev. 44(4), 507–515. https://doi.org/10.1111/cch.12561 (2018).
Chen, S., Zhang, Y. & Lu, W. A review of the influencing factors of parenting styles. Chin. J. Clin. Psychol. 28(4), 857–860 (2020).
Ernst, M. et al. What’s past is prologue: recalled parenting styles are associated with childhood cancer survivors’ mental health outcomes more than 25 years after diagnosis. Soc. Sci. Med. 252, 112916. https://doi.org/10.1016/j.socscimed.2020.112916 (2020).
Long, K. A. et al. Child-rearing in the context of childhood cancer: perspectives of parents and professionals. Pediatr. Blood Cancer. 61(2), 326–332. https://doi.org/10.1002/pbc.24556 (2014).
Acknowledgements
The authors thank all participants and team members in the hospitals of Children’s Hospital of Zhejiang University and Hangzhou Third Hospital.
Author information
Authors and Affiliations
Contributions
W.H. and W. J. designed the Study concept; Data acquisition: L.D.,Y.J., G.Z., X.J., X.X.,M.J., S.Z., J.L., and L.Y. collect the data; Analysis and interpretation of data: X.F.,Z.J. and L.D. analysesed and interpreted the data; Drafting of the manuscript: X.F. ,L.D.,Z.J. , W.J. and W. H. draft the main manuscrpit text. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This study complied with the principles of the Helsinki Declaration on human research. Written informed consent for participation or signature confirmation was required for this study in order to sure that every patient was willing to participate. No potentially identifiable human images or data is presented in this study.
Consent to participate
All the participants’ parents provided signed informed consent before the surveys were conducted.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xu, F., Lv, D., Zhou, J. et al. Parental influence on Chinese childhood cancer survivors’ physical activity: a mixed methods study. Sci Rep 15, 7998 (2025). https://doi.org/10.1038/s41598-025-87037-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-87037-0
